
Does Olfactory Dysfunction Correlate with Disease Progression in Parkinson’s Disease? A Systematic Review of the Current Literature

 ,
,  , ,
, ,
Abstract
:1. Introduction
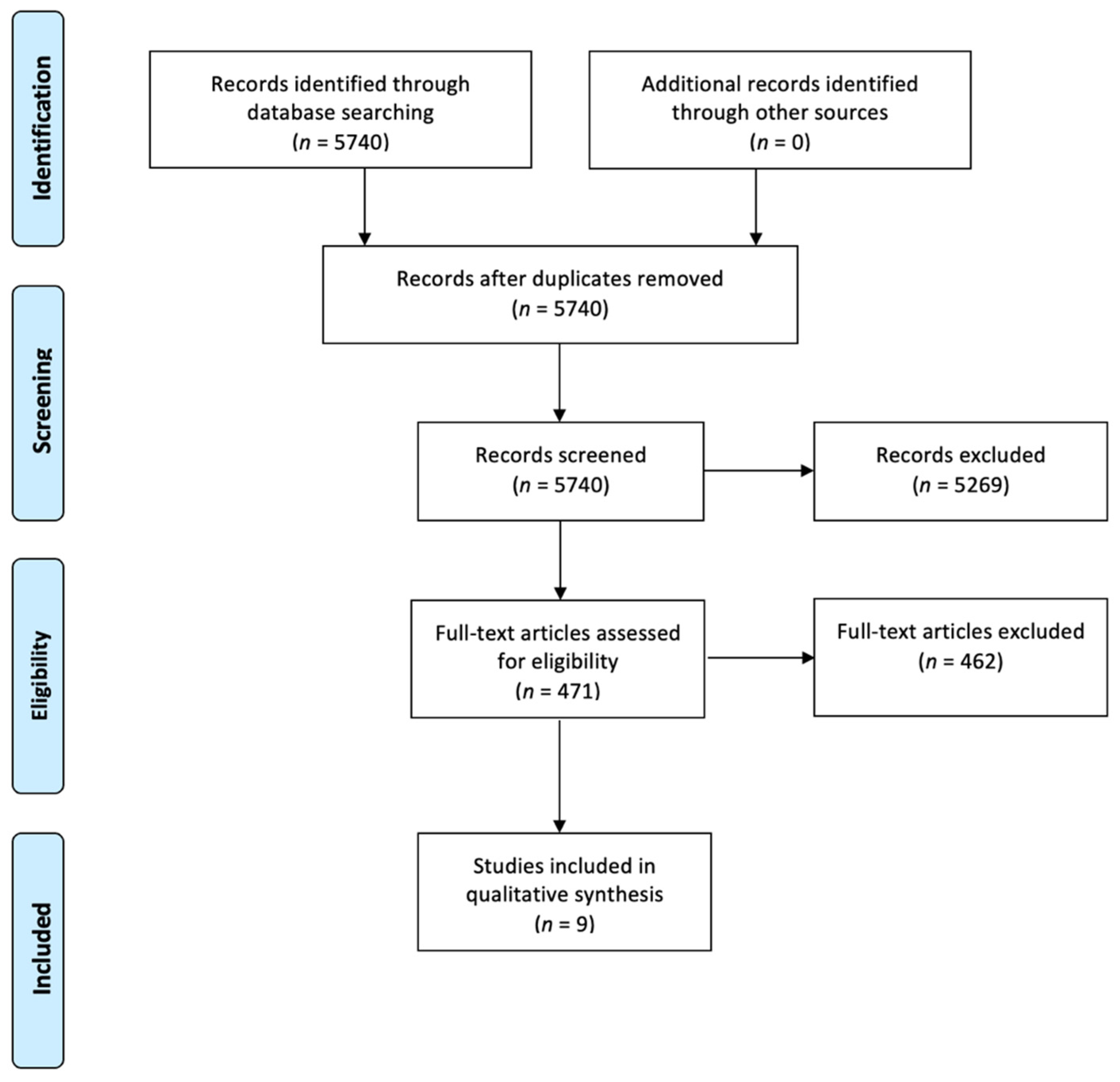
2. Methods
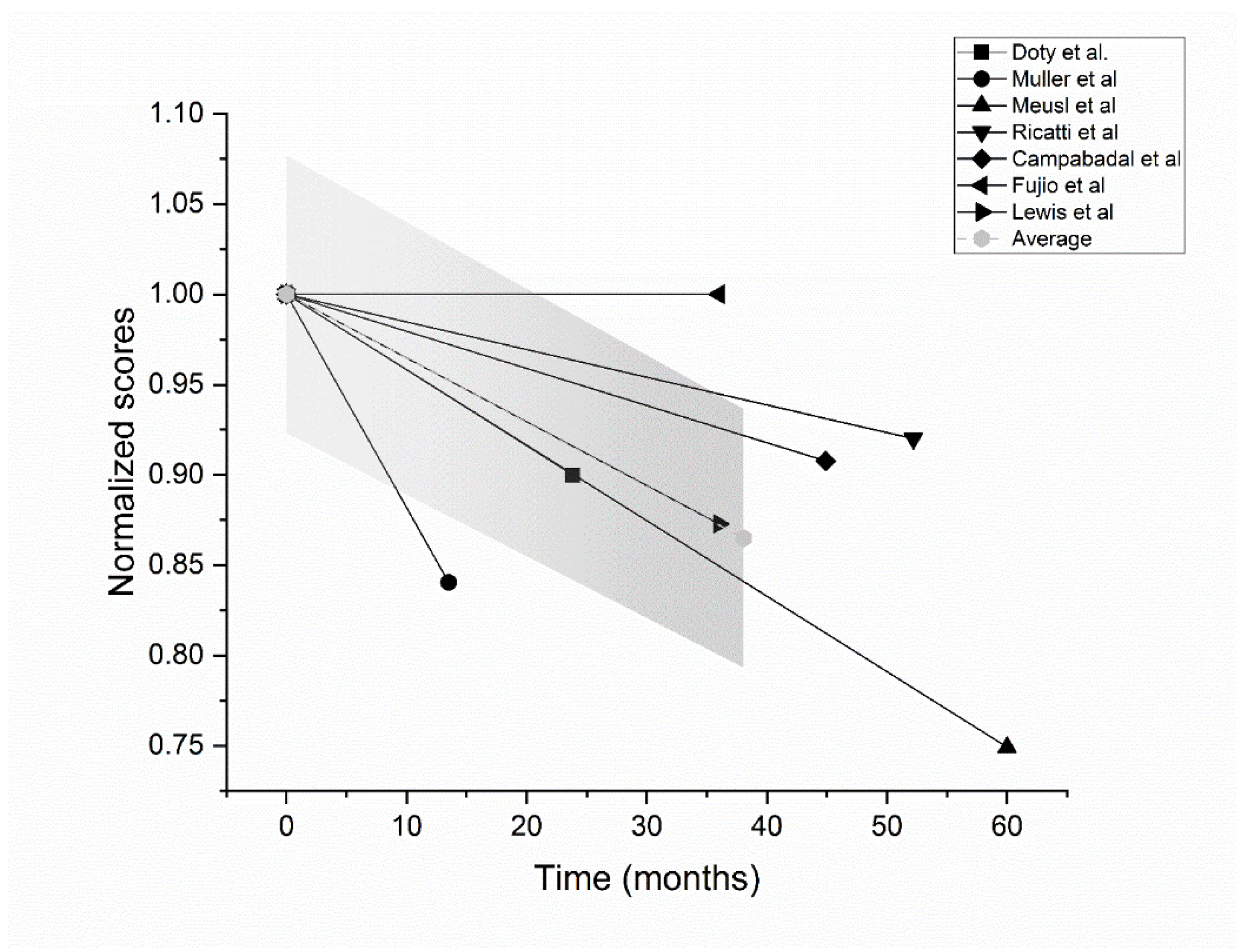
3. Results
4. Discussion
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Attems, J.; Walker, L.; Jellinger, K.A. Olfaction and Aging: A Mini-Review. Gerontology 2015, 61, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Doty, R.L.; Kamath, V. The Influences of Age on Olfaction: A Review. Front Psychol. 2014, 5, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ercoli, T.; Masala, C.; Pinna, I.; Orofino, G.; Solla, P.; Rocchi, L.; Defazio, G. Qualitative smell/taste disorders as sequelae of acute COVID-19. Neurol. Sci. 2021, 42, 4921–4926. [Google Scholar] [CrossRef] [PubMed]
- Solla, P.; Masala, C.; Liscia, A.; Piras, R.; Ercoli, T.; Fadda, L.; Hummel, T.; Haenher, A.; DeFazio, G. Sex-related differences in olfactory function and evaluation of possible confounding factors among patients with Parkinson’s disease. J. Neurol. 2019, 267, 57–63. [Google Scholar] [CrossRef]
- Doty, R.L. Olfaction in Parkinson’s disease and related disorders. Neurobiol. Dis. 2012, 46, 527–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belvisi, D.; Pellicciari, R.; Fabbrini, A.; Costanzo, M.; Pietracupa, S.; De Lucia, M.; Modugno, N.; Magrinelli, F.; Dallocchio, C.; Ercoli, T.; et al. Risk factors of Parkinson disease. Neurology 2020, 95, e2500–e2508. [Google Scholar] [CrossRef]
- Solla, P.; Masala, C.; Pinna, I.; Ercoli, T.; Loy, F.; Orofino, G.; Fadda, L.; Defazio, G. Frequency and Determinants of Olfactory Hallucinations in Parkinson’s Disease Patients. Brain Sci. 2021, 11, 841. [Google Scholar] [CrossRef]
- Marek, M.; Linnepe, S.; Klein, C.; Hummel, T.; Paus, S. High prevalence of olfactory dysfunction in cervical dystonia. Park. Relat. Disord. 2018, 53, 33–36. [Google Scholar] [CrossRef]
- Tinazzi, M.; Erro, R.; Mascia, M.M.; Esposito, M.; Ercoli, T.; Ferrazzano, G.; Di Biasio, F.; Pellicciari, B.; Eleopra, R.; Bono, F.; et al. Demographic and clinical determinants of neck pain in idiopathic cervical dystonia. J. Neural. Transm. 2020, 127, 1435–1439. [Google Scholar] [CrossRef]
- Murphy, C. Olfactory and other sensory impairments in Alzheimer disease. Nat. Rev. Neurol. 2019, 15, 11–24. [Google Scholar] [CrossRef]
- Yoo, H.S.; Jeon, S.; Chung, S.J.; Yun, M.; Lee, P.H.; Sohn, Y.H.; Evans, A.C.; Ye, B.S. Olfactory dysfunction in Alzheimer’s disease– and Lewy body–related cognitive impairment. Alzheimer’s Dement 2018, 14, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.S.; Sewell, L. Olfactory dysfunction in pure autonomic failure: Implications for the pathogenesis of Lewy body diseases. Park. Relat. Disord. 2009, 15, 516–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Defazio, G.; Ercoli, T.; Erro, R.; Pellicciari, R.; Mascia, M.M.; Fabbrini, G.; Albanese, A.; Lalli, S.; Eleopra, R.; Barone, P.; et al. Idiopathic Non-task-Specific Upper Limb Dystonia, a Neglected Form of Dystonia. Mov. Disord. 2020, 35, 2038–2045. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.S.; Chung, S.J.; Lee, Y.H.; Ye, B.S.; Sohn, Y.H.; Lee, P.H. Association between Olfactory Deficit and Motor and Cognitive Function in Parkinson’s Disease. J. Mov. Disord. 2020, 13, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Cavaco, S.; Gonçalves, A.; Mendes, A.; Vila-Chã, N.; Moreira, I.; Fernandes, J.; Teixeira-Pinto, A.; Lima, A.B. Abnormal Olfaction in Parkinson’s Disease Is Related to Faster Disease Progression. Behav. Neurol. 2015, 2015, 976589. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Tredici, K.; Del, R.U.; de Vos, R.A.; Jansen Steur, E.N.H.; Braak, E. Staging of Brain Pathology Related to Sporadic Parkinson’s Disease. Neurobiol. Aging 2003, 24, 197–211. [Google Scholar] [CrossRef]
- Hawkes, C.H.; Del Tredici, K.; Braak, H. A timeline for Parkinson’s disease. Park. Relat. Disord. 2010, 16, 79–84. [Google Scholar] [CrossRef]
- Lee, E.-Y.; Eslinger, P.J.; Du, G.; Kong, L.; Lewis, M.M.; Huang, X. Olfactory-Related Cortical Atrophy is Associated with Olfactory Dysfunction in Parkinson’s Disease. Mov. Disord. 2014, 29, 1205–1208. [Google Scholar] [CrossRef] [Green Version]
- Wattendorf, E.; Welge-Lüssen, A.; Fiedler, K.; Bilecen, D.; Wolfensberger, M.; Fuhr, P.; Hummel, T.; Westermann, B. Olfactory Impairment Predicts Brain Atrophy in Parkinson’s Disease. J. Neurosci. 2009, 29, 15410–15413. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.; Yu, C.; Fan, F.; Zhang, K.; Zhu, C.; Wu, T.; Li, K.; Chan, P. Correlation between Progressive Changes in Piriform Cortex and Olfactory Performance in Early Parkinson’s Disease. Eur. Neurol. 2011, 66, 98–105. [Google Scholar] [CrossRef]
- Marek, K.; Jennings, D.; Lasch, S.; Siderowf, A.; Tanner, C.; Simuni, T.; Coffey, C.; Kieburtz, K.; Flagg, E.; Chowdhury, S.; et al. The Parkinson Progression Marker Initiative (PPMI). Prog. Neurobiol. 2011, 95, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Defazio, G. The natural history of treated PD in an incident, community-based cohort: Does the future begin? J. Neurol. Neurosurg. Psychiatry 2011, 82, 1065. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, A.; Reichmann, H.; Livermore, A.; Hummel, T. Olfactory function in idiopathic Parkinson’s disease (IPD): Results from cross-sectional studies in IPD patients and long-term follow-up of de-novo IPD patients. J. Neural Transm. 2002, 109, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Herting, B.; Schulze, S.; Reichmann, H.; Haehner, A.; Hummel, T. A longitudinal study of olfactory function in patients with idiopathic Parkinson’s disease. J. Neurol. 2008, 255, 367–370. [Google Scholar] [CrossRef]
- Meusel, T.; Westermann, B.; Fuhr, P.; Hummel, T.; Welge-Lüssen, A. The course of olfactory deficits in patients with Parkinson’s disease—A study based on psychophysical and electrophysiological measures. Neurosci. Lett. 2010, 486, 166–170. [Google Scholar] [CrossRef]
- Ricatti, M.J.; Ottaviani, S.; Boschi, F.; Fasano, A.; Tinazzi, M.; Cecchini, M.P. A prospective evaluation of taste in Parkinson’s disease. J. Neural Transm. 2017, 124, 347–352. [Google Scholar] [CrossRef]
- Domellöf, M.E.; Lundin, K.-F.; Edström, M.; Forsgren, L. Olfactory dysfunction and dementia in newly diagnosed patients with Parkinson’s disease. Park. Relat. Disord. 2017, 38, 41–47. [Google Scholar] [CrossRef]
- Fujio, H.; Inokuchi, G.; Kuroki, S.; Tatehara, S.; Katsunuma, S.; Kowa, H.; Nibu, K.-I. Three-year prospective study on olfaction of patients with Parkinson’s disease. Auris Nasus Larynx 2020, 47, 899–904. [Google Scholar] [CrossRef]
- Campabadal, A.; Uribe, C.; Segura, B.; Baggio, H.C.; Abos, A.; Garcia-Diaz, A.I.; Marti, M.J.; Valldeoriola, F.; Compta, Y.; Bargallo, N.; et al. Brain correlates of progressive olfactory loss in Parkinson’s disease. Park. Relat. Disord. 2017, 41, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Lewis, M.M.; Harkins, E.; Lee, E.-Y.; Stetter, C.; Snyder, B.; Corson, T.; Du, G.; Kong, L.; Huang, X. Clinical Progression of Parkinson’s Disease: Insights from the NINDS Common Data Elements. J. Park. Dis. 2020, 10, 1075–1085. [Google Scholar] [CrossRef] [PubMed]
- Doty, R.L.; Deems, D.A.; Stellar, S. Olfactory dysfunction in parkinsonism: A general deficit unrelated to neurologic signs, disease stage, or disease duration. Neurology 1988, 38, 1237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansari, K.; Johnson, A. Olfactory function in patients with Parkinson’s disease. J. Chronic Dis. 1975, 28, 493–497. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Solla, P.; Masala, C.; Ercoli, T.; Orofino, G.; Loy, F.; Pinna, I.; Fadda, L.; Defazio, G. Olfactory Impairment in Parkinson’s Disease Patients with Tremor Dominant Subtype Compared to Those with Akinetic Rigid Dominant Subtype: A Pilot Study. Brain Sci. 2022, 12, 196. [Google Scholar] [CrossRef] [PubMed]
- Alster, P.; Madetko, N.; Koziorowski, D.; Friedman, A. Microglial Activation and Inflammation as a Factor in the Pathogenesis of Progressive Supranuclear Palsy (PSP). Front. Neurosci. 2020, 14, 1–7. [Google Scholar] [CrossRef]
- Torabi, A.; Mohammadbagheri, E.; Akbari Dilmaghani, N.; Bayat, A.-H.; Fathi, M.; Vakili, K.; Alizadeh, R.; Rezaeimirghaed, O.; Hajiesmaeili, M.; Ramezani, M.; et al. Proinflammatory Cytokines in the Olfactory Mucosa Result in COVID-19 Induced Anosmia. ACS Chem. Neurosci. 2020, 11, 1909–1913. [Google Scholar] [CrossRef]
- Merello, M.; Bhatia, K.P.; Obeso, J.A. SARS-CoV-2 and the risk of Parkinson’s disease: Facts and fantasy. Lancet Neurol. 2021, 20, 94–95. [Google Scholar] [CrossRef]
- Ercoli, T.; Lutzoni, L.; Orofino, G.; Muroni, A.; Defazio, G. Functional neurological disorder after COVID-19 vaccination. Neurol. Sci. 2021, 42, 3989–3990. [Google Scholar] [CrossRef]
- Hajjij, A.; Benslima, N.; Aasfara, J.; Bensouda, H.; Mahi, M.; Benariba, F. MRI of the Olfactory Tract in a Case of Post-COVID-19 Persistent Anosmia. Integr. J. Med Sci. 2021, 8, 406. [Google Scholar] [CrossRef]
- Makhoul, K.; Jankovic, J. Parkinson’s disease after COVID-19. J. Neurol. Sci. 2021, 422, 117331. [Google Scholar] [CrossRef] [PubMed]
- Tissingh, G.; Berendse, H.W.; Bergmans, P.; Dewaard, R.; Drukarch, B.; Stoof, J.C.; Wolters, E.C. Loss of olfaction in de novo and treated Parkinson’s disease: Possible implications for early diagnosis. Mov. Disord. 2001, 16, 41–46. [Google Scholar] [CrossRef]
- McKinnon, J.; Evidente, V.; Driver-Dunckley, E.; Premkumar, A.; Hentz, J.; Shill, H.; Sabbagh, M.; Caviness, J.; Connor, N.; Adler, C. Olfaction in the Elderly: A Cross-Sectional Analysis Comparing Parkinson’s Disease with Controls and Other Disorders. Int. J. Neurosci. 2010, 120, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Sorokowska, A.; Schriever, V.A.; Gudziol, V.; Hummel, C.; Hähner, A.; Iannilli, E.; Sinding, C.; Aziz, M.; Seo, H.S.; Negoias, S.; et al. Changes of olfactory abilities in relation to age: Odor identification in more than 1400 people aged 4 to 80 years. Eur. Arch. Oto-Rhino-Laryngol. 2014, 272, 1937–1944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, R.; Zhao, Y.; He, Y.; Zhou, Y.; Yang, J.; Zhou, X.; Zhu, L.; Zhou, X.; Liu, Z.; Xu, Q.; et al. Olfactory Dysfunction Predicts Disease Progression in Parkinson’s Disease: A Longitudinal Study. Front. Neurosci. 2020, 14, 1264. [Google Scholar] [CrossRef]
- Baba, T.; Kikuchi, A.; Hirayama, K.; Nishio, Y.; Hosokai, Y.; Kanno, S.; Hasegawa, T.; Sugeno, N.; Konno, M.; Suzuki, K.; et al. Severe olfactory dysfunction is a prodromal symptom of dementia associated with Parkinson’s disease: A 3 year longitudinal study. Brain 2012, 135, 161–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fullard, M.E.; Tran, B.; Xie, S.X.; Toledo, J.B.; Scordia, C.; Linder, C.; Purri, R.; Weintraub, D.; Duda, J.E.; Chahine, L.M.; et al. Olfactory impairment predicts cognitive decline in early Parkinson’s disease. Park. Relat. Disord. 2016, 25, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Masala, C.; Solla, P.; Liscia, A.; DeFazio, G.; Saba, L.; Cannas, A.; Cavazzana, A.; Hummel, T.; Haehner, A. Correlation among olfactory function, motors’ symptoms, cognitive impairment, apathy, and fatigue in patients with Parkinson’s disease. J. Neurol. 2018, 265, 1764–1771. [Google Scholar] [CrossRef]
- Politis, M.; Wu, K.; Molloy, S.; Bain, P.G.; Chaudhuri, K.R.; Piccini, P. Parkinson’s disease symptoms: The patient’s perspective. Mov. Disord. 2010, 25, 1646–1651. [Google Scholar] [CrossRef]
- Hurt, C.S.; Landau, S.; Burn, D.J.; Hindle, J.V.; Samuel, M.; Wilson, K.; Brown, R.G.; PROMS-PD Study Group. Cognition, coping, and outcome in Parkinson’s disease. Int. Psychogeriatr. 2012, 24, 1656–1663. [Google Scholar] [CrossRef]
- Opara, J.A.; Brola, W.; Leonardi, M.; Błaszczyk, B. Quality of Life in Parkinson’s Disease. J. Med. Life 2012, 5, 375–381. [Google Scholar] [PubMed]
- Cecchini, M.P.; Federico, A.; Zanini, A.; Mantovani, E.; Masala, C.; Tinazzi, M.; Tamburin, S. Olfaction and taste in Parkinson’s disease: The association with mild cognitive impairment and the single cognitive domain dysfunction. J. Neural Transm. 2019, 126, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Defazio, G.; Fabbrini, G.; Erro, R.; Albanese, A.; Barone, P.; Zibetti, M.; Esposito, M.; Pellicciari, R.; Avanzino, L.; Bono, F.; et al. Does Acute Peripheral Trauma Contribute to Idiopathic Adult-Onset Dystonia? Parkinsonism Relat. Disord. 2020, 71, 40–43. [Google Scholar] [CrossRef]
- Dagostino, S.; Ercoli, T.; Gigante, A.F.; Pellicciari, R.; Fadda, L.; Defazio, G. Sensory trick in upper limb dystonia. Park. Relat. Disord. 2019, 63, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Uecker, F.C.; Olze, H.; Kunte, H.; Gerz, C.; Göktas, O.; Harms, L.; Schmidt, F.A. Longitudinal Testing of Olfactory and Gustatory Function in Patients with Multiple Sclerosis. PLoS ONE 2017, 12, e0170492. [Google Scholar] [CrossRef] [Green Version]
- Lucassen, E.B.; Turel, A.; Knehans, A.; Huang, X.; Eslinger, P. Olfactory dysfunction in Multiple Sclerosis: A scoping review of the literature. Mult. Scler. Relat. Disord. 2015, 6, 1–9. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Ref | Authors | Sample Size | Sex | Control Size | Olfactory Test | Follow-up | Clinical Features Tested |
|---|---|---|---|---|---|---|---|
| [32] | Doty et al., 1988 | PD n = 81 Re-tested PD n = 24 | 46 M 35 F 14 M 10 F | Matched HC form a computer-based registry and n = 25 patients with AD | UPSIT | Mean 23.8 ± 8.7 months (range 5–36 months) | -Age -Disease duration -H&Y -Antiparkinsonian drugs -PIT |
| [24] | Muller et al., 2002 | PD n = 5 (de-novo) | 4 M 1 F | No control cohort | SST (Extended, TDI) | Mean 13.5 months (range 5–19 months) | -Age -UPDRS |
| [25] | Herting et al., 2008 | PD n = 27 | 22 M 5 F | No control cohort | SST (Extended, TDI) | Mean 4.4 years (range 3–6 years) | -Age -Disease duration -UPDRS III -H&Y -Clinical subtypes -Age at onset |
| [26] | Meusel et al., 2010 | PD n = 19 | 14 M 5 F | No control cohort | SST (Extended, TDI) | 5 years | -Age -Disease duration -UPDRS -H&Y -BDI -MMSE |
| [27] | Ricatti et al., 2016 | PD n = 26 | 16 M 10 F | No control cohort | SST (16-stick version) | 4.35 ± 0.49 years (range 3.5–5.6 years) | -H&Y -Taste (WMT, TST) |
| [24] | Campabadal et al., 2017 | PD n = 25 | 14 M 11 F | HC n = 24 | UPSIT | 44.9 ± 5.7 months (PD) 45.9 ± 3.5 months (HC) | -Disease duration -UPDRS III -H&Y -LEDD -SPC |
| [28] | Domellof et al., 2017 | Baseline n = 125 1 year n = 113 3 years n = 92 5 years n = 77 8 years n = 27 | 75 M 50 F | No control cohort | B-SIT | 5 years 1 year 3 years 5 years 8 years | -Age -Disease duration -UPDRS I II III IV -H&Y -PD subtypes -MMSE -MADRS |
| [29] | Fujio et al., 2019 | PD n = 56 Complete follow-up PD n = 42 | 27 M 29 F 26 M 16 F | No control cohort | OE | 3 years | -MMSE |
| [31] | Lewis et al., 2020 | PD n = 125: (31 E early, 39 M middle, 55 L late stage) 1 y visit: n = 101 2 y visit: n = 90 3 y visit n = 80 | 69 M 56 F | Data available upon request to the authors | UPSIT | 1 year 2 years 3 years | -Age -Education -Disease duration -UPDRS I, II, III, IV -H&Y -LEDD -MoCA -HDRS -PDQ-39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ercoli, T.; Masala, C.; Cadeddu, G.; Mascia, M.M.; Orofino, G.; Gigante, A.F.; Solla, P.; Defazio, G.; Rocchi, L. Does Olfactory Dysfunction Correlate with Disease Progression in Parkinson’s Disease? A Systematic Review of the Current Literature. Brain Sci. 2022, 12, 513. https://doi.org/10.3390/brainsci12050513
Ercoli T, Masala C, Cadeddu G, Mascia MM, Orofino G, Gigante AF, Solla P, Defazio G, Rocchi L. Does Olfactory Dysfunction Correlate with Disease Progression in Parkinson’s Disease? A Systematic Review of the Current Literature. Brain Sciences. 2022; 12(5):513. https://doi.org/10.3390/brainsci12050513
Chicago/Turabian StyleErcoli, Tommaso, Carla Masala, Gianluca Cadeddu, Marcello Mario Mascia, Gianni Orofino, Angelo Fabio Gigante, Paolo Solla, Giovanni Defazio, and Lorenzo Rocchi. 2022. "Does Olfactory Dysfunction Correlate with Disease Progression in Parkinson’s Disease? A Systematic Review of the Current Literature" Brain Sciences 12, no. 5: 513. https://doi.org/10.3390/brainsci12050513