
Magnetic Resonance Imaging Confirmed Olfactory Bulb Reduction in Long COVID-19: Literature Review and Case Series

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
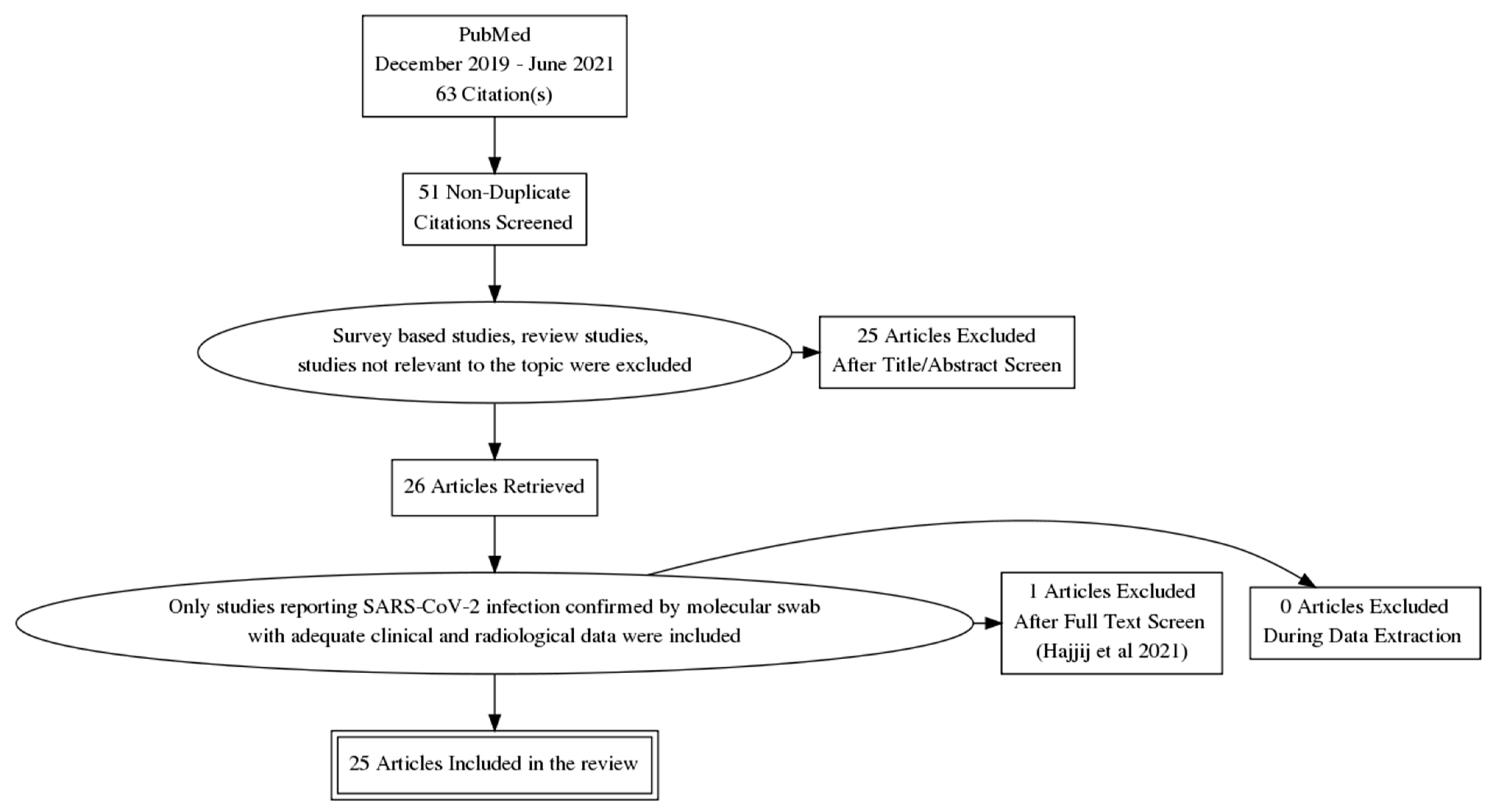
2.1. Literature Review
2.2. Case Series
2.2.1. Patients’ Management
2.2.2. Magnetic Resonance Imaging
3. Results
3.1. Literature Review
3.2. Case Series
3.2.1. Case 1
3.2.2. Case 2
3.2.3. Case 3
3.2.4. Case 4
3.2.5. Case 5
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spinato, G.; Costantini, G.; Fabbris, C.; Menegaldo, A.; Mularoni, F.; Gaudioso, P.; Mantovani, M.; Borsetto, D.; Vijendren, A.; Da Mosto, M.C.; et al. The importance of early detection of ENT symptoms in mild-to-moderate COVID-19. Acta Otorhinolaryngol. Ital. 2021, 41, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Hoang, M.P.; Kanjanaumporn, J.; Aeumjaturapat, S.; Chusakul, S.; Seresirikachorn, K.; Snidvongs, K. Olfactory and gustatory dysfunctions in COVID-19 patients: A systematic review and meta-analysis. Asian Pac. J. Allergy Immunol. 2020, 38, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Ibekwe, T.S.; Fasunla, A.J.; Orimadegun, A. Systematic review and meta-analysis of smell and taste disorders in COVID-19. OTO Open 2020, 4, 4. [Google Scholar] [CrossRef]
- Watson, D.L.B.; Campbell, M.; Hopkins, C.; Smith, B.; Kelly, C.; Deary, V. Altered smell and taste: Anosmia, parosmia and the impact of long COVID-19. PLoS ONE 2021, 16, e0256998. [Google Scholar] [CrossRef]
- Boscolo-Rizzo, P.; Hummel, T.; Hopkins, C.; Dibattista, M.; Menini, A.; Spinato, G.; Fabbris, C.; Emanuelli, E.; D’Alessandro, A.; Marzolino, R.; et al. High prevalence of long-term olfactory, gustatory, and chemesthesis dysfunction in post-COVID-19 patients: A matched case-control study with one-year follow-up using a comprehensive psychophysical evaluation. Rhinol. J. 2021, 59, 517–527. [Google Scholar] [CrossRef]
- Chippa, V.; Aleem, A.; Anjum, F. Post Acute Coronavirus (COVID-19) Syndrome; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK570608/ (accessed on 10 December 2021).
- Keshavarz, P.; Haseli, S.; Yazdanpanah, F.; Bagheri, F.; Raygani, N.; Karimi-Galougahi, M. A systematic review of imaging studies in olfactory dysfunction secondary to COVID-19. Acad. Radiol. 2021, 28, 1530–1540. [Google Scholar] [CrossRef]
- Moonis, G.; Filippi, C.G.; Kirsch, C.F.E.; Mohan, S.; Stein, E.G.; Hirsch, J.A.; Mahajan, A. The spectrum of neuroimaging findings on CT and MRI in adults With COVID-19. Am. J. Roentgenol. 2021, 217, 959–974. [Google Scholar] [CrossRef]
- Oleszkiewicz, A.; Schriever, V.A.; Croy, I.; Hähner, A.; Hummel, T. Updated sniffin’ sticks normative data based on an extended sample of 9139 subjects. Eur. Arch. Otorhinolaryngol. 2019, 276, 719–728. [Google Scholar] [CrossRef] [Green Version]
- Jafari, A.; Lehmann, A.E.; Metson, R. Is olfactory training effective treatment for postinfectious smell loss? Laryngoscope 2021, 131, 1198–1199. [Google Scholar] [CrossRef]
- Kandemirli, S.G.; Altundag, A.; Yildirim, D.; Sanli, D.E.T.; Saatci, O. Olfactory bulb MRI and paranasal sinus CT findings in persistent COVID-19 anosmia. Acad. Radiol. 2021, 28, 28–35. [Google Scholar] [CrossRef]
- Rombaux, P.; Potier, H.; Markessis, E.; Duprez, T.; Hummel, T. Olfactory bulb volume and depth of olfactory sulcus in patients with idiopathic olfactory loss. Eur. Arch. Otorhinolaryngol. 2010, 267, 1551–1556. [Google Scholar] [CrossRef] [PubMed]
- Chetrit, A.; Lechien, J.R.; Ammar, A.; Chekkoury-Idrissi, Y.; Distinguin, L.; Circiu, M.; Saussez, S.; Ballester, M.-C.; Vasse, M.; Berradja, N.; et al. Magnetic resonance imaging of COVID-19 anosmic patients reveals abnormalities of the olfactory bulb: Preliminary prospective study. J. Infect. 2020, 81, 816–846. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Li, X.; Geng, D.; Mei, N.; Wu, P.-Y.; Huang, C.-C.; Jia, T.; Zhao, Y.; Wang, D.; Xiao, A.; et al. Cerebral Micro-Structural Changes in COVID-19 Patients—An MRI-based 3-month follow-up study. EClinicalMedicine 2020, 25, 100484. [Google Scholar] [CrossRef] [PubMed]
- Niesen, M.; Trotta, N.; Noel, A.; Coolen, T.; Fayad, G.; Leurkin-Sterk, G.; Delpierre, I.; Henrard, S.; Sadeghi, N.; Goffard, J.-C.; et al. Structural and metabolic brain abnormalities in COVID-19 patients with sudden loss of smell. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1890–1901. [Google Scholar] [CrossRef] [PubMed]
- Altundag, A.; Yıldırım, D.; Sanli, D.E.T.; Cayonu, M.; Kandemirli, S.G.; Sanli, A.N.; Duz, O.A.; Saatci, O. Olfactory cleft measurements and COVID-19-related anosmia. Otolaryngol. Neck Surg. 2021, 164, 1337–1344. [Google Scholar] [CrossRef]
- Eliezer, M.; Hamel, A.-L.; Houdart, E.; Herman, P.; Housset, J.; Jourdaine, C.; Eloit, C.; Verillaud, B.; Hautefort, C. Loss of smell in patients with COVID-19: MRI data reveal a transient edema of the olfactory clefts. Neurology 2020, 95, e3145–e3152. [Google Scholar] [CrossRef]
- Tsivgoulis, G.; Fragkou, P.C.; Lachanis, S.; Palaiodimou, L.; Lambadiari, V.; Papathanasiou, M.; Sfikakis, P.P.; Voumvourakis, K.I.; Tsiodras, S. Olfactory bulb and mucosa abnormalities in persistent COVID-19-induced anosmia: A magnetic resonance imaging study. Eur. J. Neurol. 2021, 28, 28. [Google Scholar] [CrossRef]
- Aragão, M.; Leal, M.; Filho, O.C.; Fonseca, T.; Valença, M. Anosmia in COVID-19 Associated with Injury to the Olfactory Bulbs Evident on MRI. Am. J. Neuroradiol. 2020, 41, 1703–1706. [Google Scholar] [CrossRef]
- Klironomos, S.; Tzortzakakis, A.; Kits, A.; Öhberg, C.; Kollia, E.; Ahoromazdae, A.; Almqvist, H.; Aspelin, Å.; Martin, H.; Ouellette, R.; et al. Nervous system involvement in coronavirus disease 2019: Results from a retrospective consecutive neuroimaging cohort. Radiology 2020, 297, E324–E334. [Google Scholar] [CrossRef]
- Strauss, S.; Lantos, J.; Heier, L.; Shatzkes, D.; Phillips, C. Olfactory bulb signal abnormality in patients with COVID-19 who present with neurologic symptoms. Am. J. Neuroradiol. 2020, 41, 1882–1887. [Google Scholar] [CrossRef]
- Yousefi-Koma, A.; Haseli, S.; Bakhshayeshkaram, M.; Raad, N.; Karimi-Galougahi, M. Multimodality imaging with PET/CT and MRI reveals hypometabolism in tertiary olfactory cortex in parosmia of COVID-19. Acad. Radiol. 2021, 28, 749–751. [Google Scholar] [CrossRef] [PubMed]
- Li, C.-W.; Syue, L.-S.; Tsai, Y.-S.; Li, M.-C.; Lo, C.-L.; Tsai, C.-S.T.; Chen, P.-L.; Ko, W.-C.; Lee, N.-Y. Anosmia and olfactory tract neuropathy in a case of COVID-19. J. Microbiol. Immunol. Infect. 2021, 54, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Chiu, A.; Fischbein, N.; Wintermark, M.; Zaharchuk, G.; Yun, P.T.; Zeineh, M. COVID-19-induced anosmia associated with olfactory bulb atrophy. Neuroradiology 2021, 63, 147–148. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, D.G.; Hygino da Cruz, L.C., Jr.; Lopes, F.C.R.; Rangel, C.C.; de Araújo Henriques Tessarollo, A.L.; Coelho, K.C.G.; Brandão, R.Z.; Novis, R.A.F.; Novis, S.S.C.; Silveira, R.; et al. Magnetic resonance imaging features of COVID-19-related cranial nerve lesions. J. Neurovirol. 2021, 27, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Galougahi, M.K.; Ghorbani, J.; Bakhshayeshkaram, M.; Naeini, A.S.; Haseli, S. Olfactory bulb magnetic resonance imaging in SARS-CoV-2-induced anosmia: The first report. Acad. Radiol. 2020, 27, 892–893. [Google Scholar] [CrossRef]
- Hatipoglu, N.; Yazici, Z.M.; Palabiyik, F.; Gulustan, F.; Sayin, I. Olfactory bulb magnetic resonance imaging in SARS-CoV-2-induced anosmia in pediatric cases. Int. J. Pediatr. Otorhinolaryngol. 2020, 139, 110469. [Google Scholar] [CrossRef]
- Laurendon, T.; Radulesco, T.; Mugnier, J.; Gérault, M.; Chagnaud, C.; El Ahmadi, A.-A.; Varoquaux, A. Bilateral transient olfactory bulb edema during COVID-19–related anosmia. Neurology 2020, 95, 224–225. [Google Scholar] [CrossRef]
- Politi, L.S.; Salsano, E.; Grimaldi, M. Magnetic resonance imaging alteration of the brain in a patient with coronavirus disease 2019 (COVID-19) and anosmia. JAMA Neurol. 2020, 77, 1028. [Google Scholar] [CrossRef]
- Schönegger, C.M.; Gietl, S.; Heinzle, B.; Freudenschuss, K.; Walder, G. Smell and taste disorders in COVID-19 patients: Objective testing and magnetic resonance imaging in five cases. SN Compr. Clin. Med. 2020, 2, 2535–2539, Epub ahead of print. [Google Scholar] [CrossRef]
- Wang, E.; Ulualp, S.O.; Liu, C.; Veling, M. Sudden anosmia and ageusia in a child: A COVID-19 case report. Otolaryngol. Case Rep. 2021, 18, 100267. [Google Scholar] [CrossRef]
- Zhang, Q.; Shan, K.S.; Abdollahi, S.; Nace, T. Anosmia and ageusia as the only indicators of coronavirus disease 2019 (COVID-19). Cureus 2020, 12, e7918. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.-C.; Tsai, Y.-S.; Syue, L.-S.; Lee, N.-Y.; Li, C.-W. Olfactory bulb atrophy in a case of COVID-19 with hyposmia. Acad. Radiol. 2020, 27, 1649–1650. [Google Scholar] [CrossRef] [PubMed]
- Theodorou, D.J.; Tsaggou, V.; Tsifetaki, N. Anosmia caused by ischaemic olfactory infarction: False alert for COVID-19 infection. QJM Int. J. Med. 2021, 114, 50–51. [Google Scholar] [CrossRef]
- Melegari, G.; Rivi, V.; Zelent, G.; Nasillo, V.; De Santis, E.; Melegari, A.; Bevilacqua, C.; Zoli, M.; Meletti, S.; Barbieri, A. Mild to severe neurological manifestations of COVID-19: Cases reports. Int. J. Environ. Res. Public Health 2021, 18, 3673. [Google Scholar] [CrossRef] [PubMed]
- Ismail, I.I.; Gad, K.A. Absent blood oxygen level-dependent functional magnetic resonance imaging activation of the orbitofrontal cortex in a patient with persistent cacosmia and cacogeusia after COVID-19 infection. JAMA Neurol. 2021, 78, 609. [Google Scholar] [CrossRef] [PubMed]
- Han, P.; Zang, Y.; Akshita, J.; Hummel, T. Magnetic resonance imaging of human olfactory dysfunction. Brain Topogr. 2019, 32, 987–997, Erratum in: Brain Topogr. 2019, 33, 149. [Google Scholar] [CrossRef]
- Mueller, A.; Rodewald, A.; Reden, J.; Gerber, J.; Von Kummer, R.; Hummel, T. Reduced olfactory bulb volume in post-traumatic and post-infectious olfactory dysfunction. NeuroReport 2005, 16, 475–478. [Google Scholar] [CrossRef]
- Yao, L.; Linyin, Y.; Pinto, J.M.; Yuan, X.; Guo, Y.; Liu, Y.; Wei, Y. Olfactory cortex and Olfactory bulb volume alterations in patients with post-infectious Olfactory loss. Brain Imaging Behav. 2018, 12, 1355–1362. [Google Scholar] [CrossRef]
- Griffanti, L.; Raman, B.; Alfaro-Almagro, F.; Filippini, N.; Cassar, M.P.; Sheerin, F.; Okell, T.W.; McConnell, F.A.K.; Chappell, M.A.; Wang, C.; et al. Adapting the UK biobank brain imaging protocol and analysis pipeline for the C-MORE multi-organ study of COVID-19 survivors. Front. Neurol. 2021, 12, 12. [Google Scholar] [CrossRef]
- Douaud, G.; Lee, S.; Alfaro-Almagro, F.; Arthofer, C.; Wang, C.; Lange, F.; Andersson, J.L.; Griffanti, L.; Duff, E.; Jbabdi, S.; et al. Brain imaging before and after COVID-19 in UK Biobank. MedRxiv 2021, 6, 21258690. [Google Scholar] [CrossRef]
- Aiyegbusi, O.L.; Hughes, S.E.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S.; Haroon, S.; Price, G.; Davies, E.H.; Nirantharakumar, K.; et al. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef] [PubMed]
- Hummel, T.; Rissom, K.; Reden, J.; Hähner, A.; Weidenbecher, M.; Hüttenbrink, K.-B. Effects of olfactory training in patients with olfactory loss. Laryngoscope 2009, 119, 496–499. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.T.; Sabha, M.; Damm, M.; Philpott, C.; Oleszkiewicz, A.; Hähner, A.; Hummel, T. Parosmia is associated with relevant olfactory recovery after olfactory training. Laryngoscope 2021, 131, 618–623. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Reference | Design | NoP (NoF) | Age | COVID-19 Classification | Time Symptoms–MRI | OB Size | OB Volume (mm3) | OB Hyperintensity | Other Findings |
|---|---|---|---|---|---|---|---|---|---|
| [11] | Perspective | 23 (14) | 29 | NR | NR | Reduced | R:62; L:60.8 | Yes | OC opacification |
| [13] | Perspective | 23 (14) | 39.0 ± 17.1 | Mild illness | NR | NR | NR | Yes | OC edema |
| [14] | Perspective | 60 (26) | 44.10 ± 16.00 | Mild illness (47 cases) Severe (13 cases) | 90 days | NR | NR | NR | COP altered activity |
| [15] | Perspective | 12 (10) | 42 | NR | 15 days | Asymmetry | NR | No | OC edema; COP altered activity |
| [16] | Case-control | 24 (14) | 39.3 ± 12 | NR | 22 days | Normal | R: 59.76; L: 58.33 | NR | OC reduced volume and inflammation |
| [17] | Case-control | 20 (10) | 34.6 ± 8.8 | NR | 6 days (1st MRI); 30 days (2nd MRI) | Normal | During infection: R: 37.7; L: 40.2 After infection: R: 38.1; L: 38.2 | NR | OC obstruction (1st MRI) |
| [18] | Case-control | 8 (6) | 45.3 | Mild Illness | 70.5 days | Reduced | NR | NR | OC edema |
| [19] | Retrospective | 5 (NR) | NR | NR | NR | NR | NR | Yes | NR |
| [20] | Retrospective | 37 (NR) | NR | NR | NR | NR | NR | Yes | NR |
| [21] | Retrospective | 12 (6) | 58.25 ± 14.85 | NR | <30 days | Normal | NR | Yes | NR |
| [22] | CR | 1 (1) | 28 | NR | 180 days | Normal | NR | No | COP altered activity |
| [23] | CR | 1 (0) | 21 | Mild illness | 28 days | Reduced | NR | Yes | NR |
| [24] | CR | 1 (1) | 19 | Mild illness | 60 days | Reduced | Before infection: R: 49.5; L: 47.46 After infection: R: 29.96; L: 35.51 | NR | NR |
| [25] | CR | 1 (1) | 41 | NR | 14 days | NR | NR | Yes | NR |
| [26] | CR | 1 (0) | 27 | NR | NR days | Normal | NR | No | NR |
| [27] | CR | 3 (1) | 13 | Mild illness (2 cases) Severe (1 case) | <10 days | Normal | NR | No | NR |
| [28] | CR | 1 (0) | 27 | NR | 7 days | Augmented | R:64; L:73 | Yes | OC edema |
| [29] | CR | 1 (1) | 25 | Mild illness | 3 days | NR | NR | Yes | COP altered activity |
| [30] | CR | 5 (5) | NR | NR | <30 days | Normal | NR | No | COP altered activity |
| [31] | CR | 1(0) | 17 | Mild illness | NR | Normal | NR | No | NR |
| [32] | CR | 1(1) | 60 | Asymptomatic | During infection | NR | NR | No | NR |
| [33] | CR | 1(1) | 16 | Mild illness | 38 days | Asymmetry | NR | No | OT hyperintensity |
| [34] | CR | 1(1) | 68 | Mild illness | NR | Normal | NR | No | OT hyperintensity |
| [35] | CR | 2(2) | 31 | Mild illness (1 case) Severe (1 case) | 25 days | Normal | NR | Yes | NR |
| [36] | CR | 1(1) | 25 | Mild illness | 90 days | Normal | NR | No | NR |
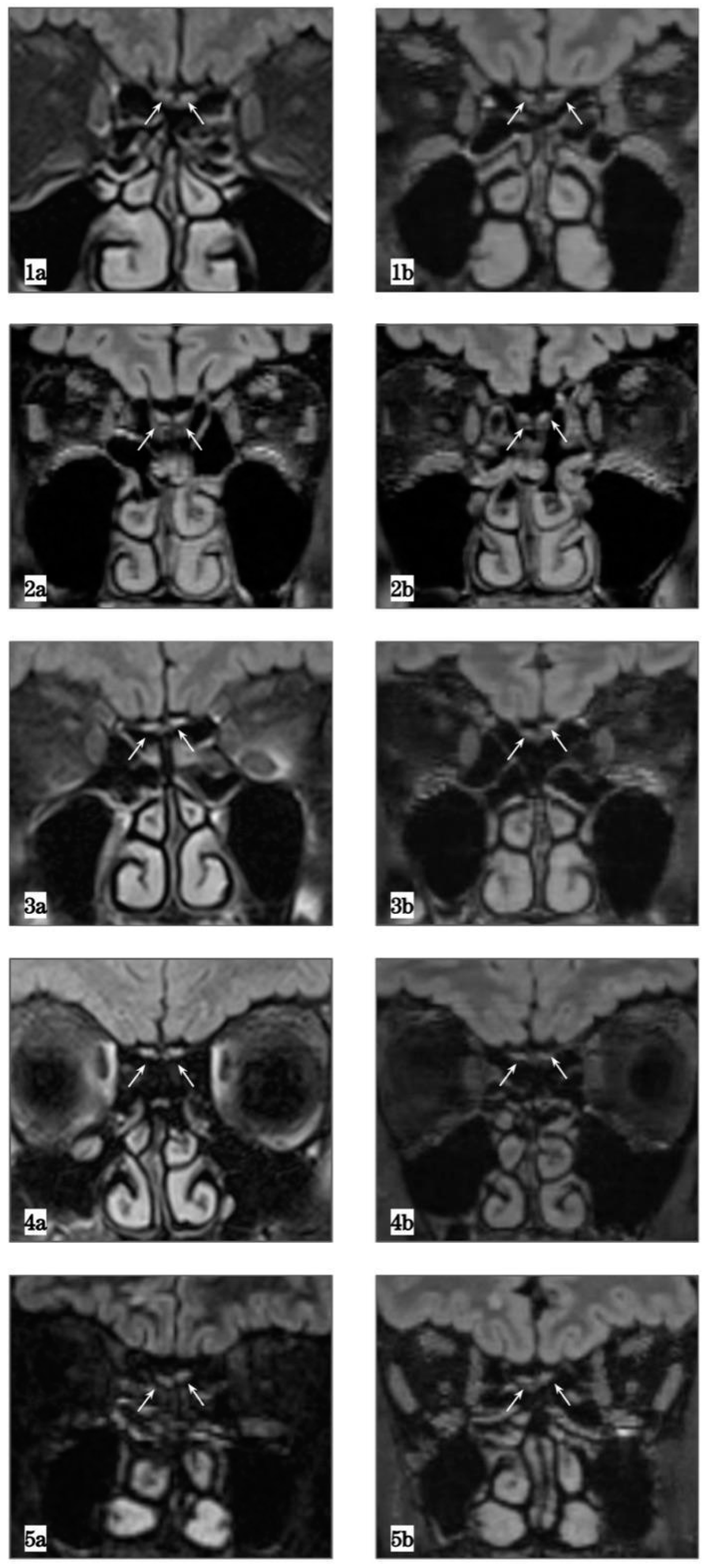
| Case Number | Age, Gender | Sniffin’ Sticks Test | Before COVID-19 Left OBV (mm3) | After COVID-19 Left OBV (mm3) | Before COVID-19 Right OBV (mm3) | After COVID-19 Right OBV (mm3) |
|---|---|---|---|---|---|---|
| Case 1 | 70, M | 23/48 | 86.96 (1a) | 26.07 (1b) | 69.4 (1a) | 26.99 (1b) |
| Case 2 | 70, M | 25/48 | 77.42 (2a) | 37.24 (2b) | 81.36 (2a) | 44.94 (2b) |
| Case 3 | 59, F | 32.5/48 | 75.55 (3a) | 28.33 (3b) | 58.25 (3a) | 19.44 (3b) |
| Case 4 | 23, F | 30.5/48 | 105.44 (4a) | 55.04 (4b) | 116.4 (4a) | 45.93 (4b) |
| Case 5 | 45, M | NA | 40.58 (5a) | 48.3 (5b) | 53.53 (5a) | 66.87 (5b) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frosolini, A.; Parrino, D.; Fabbris, C.; Fantin, F.; Inches, I.; Invitto, S.; Spinato, G.; Filippis, C.D. Magnetic Resonance Imaging Confirmed Olfactory Bulb Reduction in Long COVID-19: Literature Review and Case Series. Brain Sci. 2022, 12, 430. https://doi.org/10.3390/brainsci12040430
Frosolini A, Parrino D, Fabbris C, Fantin F, Inches I, Invitto S, Spinato G, Filippis CD. Magnetic Resonance Imaging Confirmed Olfactory Bulb Reduction in Long COVID-19: Literature Review and Case Series. Brain Sciences. 2022; 12(4):430. https://doi.org/10.3390/brainsci12040430
Chicago/Turabian StyleFrosolini, Andrea, Daniela Parrino, Cristoforo Fabbris, Francesco Fantin, Ingrid Inches, Sara Invitto, Giacomo Spinato, and Cosimo De Filippis. 2022. "Magnetic Resonance Imaging Confirmed Olfactory Bulb Reduction in Long COVID-19: Literature Review and Case Series" Brain Sciences 12, no. 4: 430. https://doi.org/10.3390/brainsci12040430