
Transcranial Pulsed-Current Stimulation versus Transcranial Direct Current Stimulation in Patients with Disorders of Consciousness: A Pilot, Sham-Controlled Cross-Over Double-Blind Study

 , and
, and
Abstract
: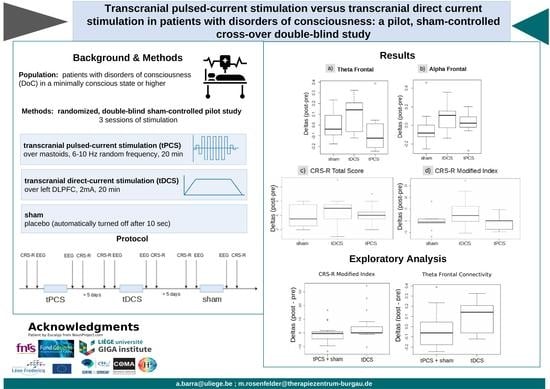
1. Introduction
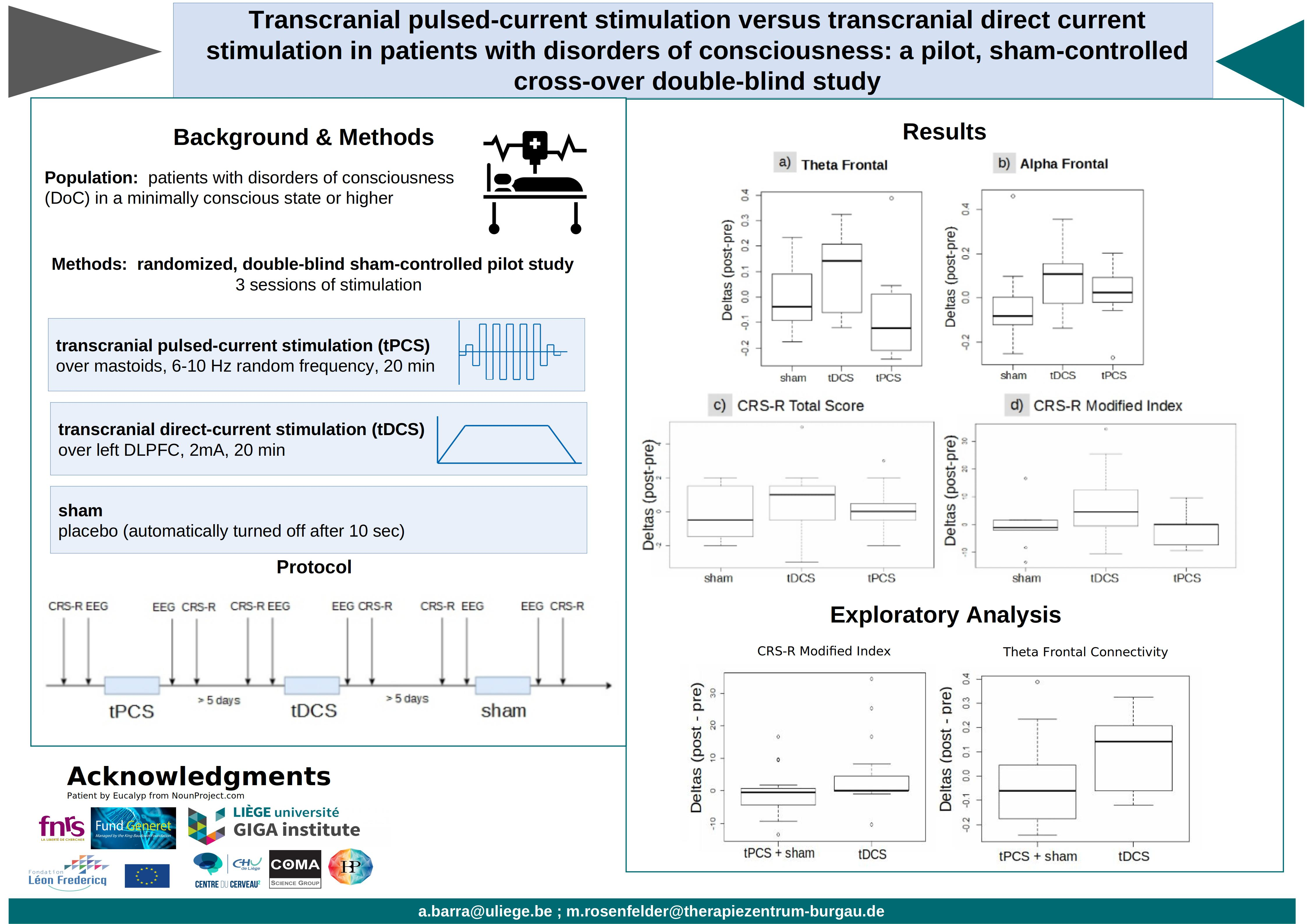
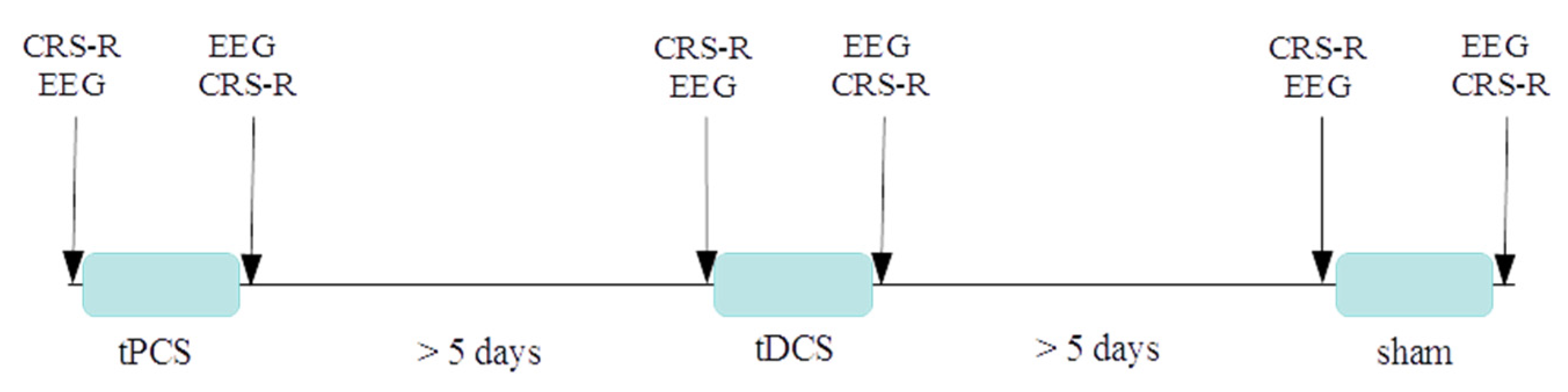
2. Materials and Methods
2.1. Data Analyses
2.2. Statistical Analyses
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jennett, B. The vegetative state. J. Neurol. Neurosurg. Psychiatry 2002, 73, 355–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laureys, S.; Celesia, G.G.; Cohadon, F.; Lavrijsen, J.; León-Carrión, J.; Sannita, W.G.; Sazbon, L.; Schmutzhard, E.; Von Wild, K.R.; Zeman, A.; et al. Unresponsive wakefulness syndrome: A new name for the vegetative state or apallic syndrome. BMC Med. 2010, 8, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacino, J.T.; Ashwal, S.; Childs, N.; Cranford, R.; Jennett, B.; Katz, D.I.; Kelly, J.P.; Rosenberg, J.H.; Whyte, J.; Zafonte, R.D.; et al. The minimally conscious state: Definition and diagnostic criteria. Neurology 2002, 58, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Thibaut, A.; Chennu, S.; Chatelle, C.; Martens, G.; Annen, J.; Cassol, H.; Laureys, S. Theta network centrality correlates with tDCS response in disorders of consciousness. Brain Stimul. 2018, 11, 1407–1409. [Google Scholar] [CrossRef] [Green Version]
- Whyte, J.; Myers, R. Incidence of clinically significant responses to zolpidem among patients with disorders of consciousness: A preliminary placebo controlled trial. Am. J. Phys. Med. Rehabil. 2009, 88, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T.; Whyte, J.; Bagiella, E.; Kalmar, K.; Childs, N.; Khademi, A.; Eifert, B.; Long, D.; Katz, D.; Cho, S.; et al. Placebo-controlled trial of amantadine for severe traumatic brain injury. N. Engl. J. Med. 2012, 366, 819–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunn, H.; Grobelna, A. Neuromodulation technologies for the treatment of Alzheimer disease. Can. J. Health Technol. 2021, 1, 1–19. [Google Scholar] [CrossRef]
- Rahimpour, S.; Gaztanaga, W.; Yadav, A.P.; Chang, S.J.; Krucoff, M.O.; Cajigas, I.; Turner, D.A.; Wang, D.D. Freezing of gait in Parkinson’s disease: Invasive and noninvasive neuromodulation. Neuromodulation Technol. Neural Interface 2020, 24, 829–842. [Google Scholar] [CrossRef]
- Inagawa, T.; Narita, Z.; Sugawara, N.; Maruo, K.; Stickley, A.; Yokoi, Y.; Sumiyoshi, T. A Meta-Analysis of the effect of multisession transcranial direct current stimulation on cognition in dementia and mild cognitive impairment. Clin. EEG Neurosci. 2019, 50, 273–282. [Google Scholar] [CrossRef]
- Lundstrom, B.N.; Wharen, R.E., Jr.; Tatum, W.O. Neuromodulation for epilepsy. Epilepsy 2021, 2021, 431–440. [Google Scholar] [CrossRef]
- Austelle, C.W.; O’Leary, G.H.; Thompson, S.; Gruber, E.; Kahn, A.; Manett, A.J.; Short, B.; Badran, B.W. A comprehensive review of vagus nerve stimulation for depression. Neuromodulation Technol. Neural Interface 2021, 2021. [Google Scholar] [CrossRef]
- Cohen, S.L.; Bikson, M.; Badran, B.W.; George, M.S. A visual and narrative timeline of US FDA milestones for Transcranial Magnetic Stimulation (TMS) devices. Brain Stimul. 2021, 15, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Giordano, J.; Bikson, M.; Kappenman, E.S.; Clark, V.P.; Coslett, H.B.; Hamblin, M.R.; Hamilton, R.; Jankord, R.; Kozumbo, W.J.; McKinley, R.A.; et al. Mechanisms and effects of transcranial direct current stimulation. Dose-Response 2017, 15, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stagg, C.J.; Nitsche, M.A. Physiological basis of transcranial direct current stimulation. Neuroscientist 2011, 17, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Jaberzadeh, S.; Bastani, A.; Zoghi, M. Anodal transcranial pulsed current stimulation: A novel technique to enhance corticospinal excitability. Clin. Neurophysiol. 2014, 125, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Duarte, I.; Gebodh, N.; Schestatsky, P.; Guleyupoglu, B.; Reato, D.; Bikson, M.; Fregni, F. Transcranial electrical stimulation: Transcranial direct current stimulation (tDCS), transcranial alternating current stimulation (tACS), transcranial pulsed current stimulation (tPCS), and transcranial random noise stimulation (tRNS). In The Stimulated Brain; Academic Press: Cambridge, MA, USA, 2014; pp. 35–59. [Google Scholar]
- Thibaut, A.; Bruno, M.-A.; LeDoux, D.; Demertzi, A.; Laureys, S. tDCS in patients with disorders of consciousness: Sham-controlled randomized double-blind study. Neurology 2014, 82, 1112–1118. [Google Scholar] [CrossRef] [PubMed]
- Estraneo, A.; Pascarella, A.; Moretta, P.; Masotta, O.; Fiorenza, S.; Chirico, G.; Crispino, E.; Loreto, V.; Trojano, L. Repeated transcranial direct current stimulation in prolonged disorders of consciousness: A double-blind cross-over study. J. Neurol. Sci. 2017, 375, 464–470. [Google Scholar] [CrossRef]
- Angelakis, E.; Liouta, E.; Andreadis, N.; Korfias, S.; Ktonas, P.; Stranjalis, G.; Sakas, D.E. Transcranial direct current stimulation effects in disorders of consciousness. Arch. Phys. Med. Rehabil. 2014, 95, 283–289. [Google Scholar] [CrossRef]
- Martens, G.; Lejeune, N.; O’Brien, A.T.; Fregni, F.; Martial, C.; Wannez, S.; Laureys, S.; Thibaut, A. Randomized controlled trial of home-based 4-week tDCS in chronic minimally conscious state. Brain Stimul. 2018, 11, 982–990. [Google Scholar] [CrossRef] [Green Version]
- Thibaut, A.; Wannez, S.; Donneau, A.-F.; Chatelle, C.; Gosseries, O.; Bruno, M.-A.; Laureys, S. Controlled clinical trial of repeated prefrontal tDCS in patients with chronic minimally conscious state. Brain Inj. 2017, 31, 466–474. [Google Scholar] [CrossRef]
- Zhang, Y.; Song, W.; Du, J.; Huo, S.; Shan, G.; Li, R. Transcranial direct current stimulation in patients with prolonged disorders of consciousness: Combined behavioral and event-related potential evidence. Front. Neurol. 2017, 8, 620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martens, G.; Fregni, F.; Carrière, M.; Barra, A.; Laureys, S.; Thibaut, A. Single tDCS session of motor cortex in patients with disorders of consciousness: A pilot study. Brain Inj. 2019, 33, 1679–1683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, W.; Wannez, S.; Fregni, F.; Hu, X.; Jing, S.; Martens, G.; He, M.; Di, H.; Laureys, S.; Thibaut, A. Repeated stimulation of the posterior parietal cortex in patients in minimally conscious state: A sham-controlled randomized clinical trial. Brain Stimul. 2017, 10, 718–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martens, G.; Kroupi, E.; Bodien, Y.; Frasso, G.; Annen, J.; Cassol, H.; Barra, A.; Martial, C.; Gosseries, O.; Lejeune, N.; et al. Behavioral and electrophysiological effects of network-based frontoparietal tDCS in patients with severe brain injury: A randomized controlled trial. NeuroImage Clin. 2020, 28, 102426. [Google Scholar] [CrossRef] [PubMed]
- Thibaut, A.; Schiff, N.; Giacino, J.; Laureys, S.; Gosseries, O. Therapeutic interventions in patients with prolonged disorders of consciousness. Lancet Neurol. 2019, 18, 600–614. [Google Scholar] [CrossRef]
- Cavinato, M.; Genna, C.; Formaggio, E.; Gregorio, C.; Storti, S.F.; Manganotti, P.; Casanova, E.; Piperno, R.; Piccione, F. Behavioural and electrophysiological effects of tDCS to prefrontal cortex in patients with disorders of consciousness. Clin. Neurophysiol. 2019, 130, 231–238. [Google Scholar] [CrossRef]
- Carrière, M.; Mortaheb, S.; Raimondo, F.; Annen, J.; Barra, A.; Fossati, M.C.B.; Chatelle, C.; Hermann, B.; Martens, G.; Di Perri, C.; et al. Neurophysiological correlates of a single session of prefrontal tDCS in patients with prolonged disorders of consciousness: A pilot double-blind randomized controlled study. Brain Sci. 2020, 10, 469. [Google Scholar] [CrossRef]
- Jensen, B.R.; Malling, A.S.B.; Schmidt, S.I.; Meyer, M.; Morberg, B.M.; Wermuth, L. Long-term treatment with transcranial pulsed electromagnetic fields improves movement speed and elevates cerebrospinal erythropoietin in Parkinson’s disease. PLoS ONE 2021, 16, e0248800. [Google Scholar] [CrossRef]
- Alon, G.; Yungher, D.A.; Shulman, L.M.; Rogers, M.W. Safety and immediate effect of noninvasive transcranial pulsed current stimulation on gait and balance in Parkinson disease. Neurorehabilit. Neural Repair. 2012, 26, 1089–1095. [Google Scholar] [CrossRef]
- Ruhnau, P.; Rufener, K.S.; Heinze, H.-J.; Zaehle, T. Pulsed transcranial electric brain stimulation enhances speech comprehension. Brain Stimul. 2020, 13, 1402–1411. [Google Scholar] [CrossRef]
- Morales-Quezada, L.; Cosmo, C.; Carvalho, S.; Leite, J.; Castillo-Saavedra, L.; Rozisky, J.R.; Fregni, F. Cognitive effects and autonomic responses to transcranial pulsed current stimulation. Exp. Brain Res. 2014, 233, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Miniussi, C.; Harris, J.; Ruzzoli, M. Modelling non-invasive brain stimulation in cognitive neuroscience. Neurosci. Biobehav. Rev. 2013, 37, 1702–1712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Datta, A.; Dmochowski, J.P.; Guleyupoglu, B.; Bikson, M.; Fregni, F. Cranial electrotherapy stimulation and transcranial pulsed current stimulation: A computer based high-resolution modeling study. NeuroImage 2013, 65, 280–287. [Google Scholar] [CrossRef]
- Saavedra, L.C.; Morales-Quezada, L.; Doruk, D.; Rozinsky, J.; Coutinho, L.; Faria, P.; Perissinotti, I.; Wang, Q.-M.; Fregni, F. QEEG indexed frontal connectivity effects of transcranial pulsed current stimulation (tPCS): A sham-controlled mechanistic trial. Neurosci. Lett. 2014, 577, 61–65. [Google Scholar] [CrossRef]
- Morales-Quezada, L.; Saavedra, L.C.; Rozisky, J.; Hadlington, L.; Fregni, F. Intensity-dependent effects of transcranial pulsed current stimulation on interhemispheric connectivity: A high-resolution qEEG, sham-controlled study. NeuroReport 2014, 25, 1054–1058. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Sustained excitability elevations induced by transcranial DC motor cortex stimulation in humans. Neurology 2001, 57, 1899–1901. [Google Scholar] [CrossRef]
- Giacino, J.T.; Kalmar, K.; Whyte, J. The JFK coma recovery scale-revised: Measurement characteristics and diagnostic utility. Arch. Phys. Med. Rehabil. 2004, 85, 2020–2029. [Google Scholar] [CrossRef]
- Gramfort, A.; Luessi, M.; Larson, E.; Engemann, D.A.; Strohmeier, D.; Brodbeck, C.; Goj, R.; Jas, M.; Brooks, T.; Parkkonen, L.; et al. MEG and EEG data analysis with MNE-Python. Front. Neurosci. 2013, 7, 267. [Google Scholar] [CrossRef] [Green Version]
- Bell, A.J.; Sejnowski, T.J. An information-maximization approach to blind separation and blind deconvolution. Neural Comput. 1995, 7, 1129–1159. [Google Scholar] [CrossRef]
- Schiff, N.D. Recovery of consciousness after brain injury: A mesocircuit hypothesis. Trends Neurosci. 2010, 33, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Edlow, B.L.; Claassen, J.; Schiff, N.D.; Greer, D.M. Recovery from disorders of consciousness: Mechanisms, prognosis and emerging therapies. Nat. Rev. Neurol. 2021, 17, 135–156. [Google Scholar] [CrossRef] [PubMed]
- Chennu, S.; Annen, J.; Wannez, S.; Thibaut, A.; Chatelle, C.; Cassol, H.; Martens, G.; Schnakers, C.; Gosseries, O.; Menon, D.; et al. Brain networks predict metabolism, diagnosis and prognosis at the bedside in disorders of consciousness. Brain 2017, 140, 2120–2132. [Google Scholar] [CrossRef]
- Annen, J.; Filippini, M.M.; Bonin, E.; Cassol, H.; Aubinet, C.; Carrière, M.; Gosseries, O.; Thibaut, A.; Barra, A.; Wolff, A.; et al. Diagnostic accuracy of the CRS-R index in patients with disorders of consciousness. Brain Inj. 2019, 33, 1409–1412. [Google Scholar] [CrossRef] [PubMed]
- Morales-Quezada, L.; Castillo-Saavedra, L.; Cosmo, C.; Doruk, D.; Sharaf, I.; Malavera, A.; Fregni, F. Optimal random frequency range in transcranial pulsed current stimulation indexed by quantitative electroencephalography. NeuroReport 2015, 26, 747–752. [Google Scholar] [CrossRef]
- Dissanayaka, M.T.; Zoghi, M.; Hill, A.T.; Farrell, M.; Egan, G.; Jaberzadeh, S. The effect of transcranial pulsed current stimulation at 4 and 75 Hz on electroencephalography theta and high gamma band power: A pilot study. Brain Connect. 2020, 10, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Castillo-Saavedra, L.; Gebodh, N.; Bikson, M.; Diaz-Cruz, C.; Brandao, R.; Coutinho, L.; Truong, D.; Datta, A.; Shani-Hershkovich, R.; Weiss, M.; et al. Clinically effective treatment of fibromyalgia pain with high-definition transcranial direct current stimulation: Phase II open-label dose optimization. J. Pain 2016, 17, 14–26. [Google Scholar] [CrossRef] [Green Version]
- Hermann, B.; Raimondo, F.; Hirsch, L.; Huang, Y.; Denis-Valente, M.; Pérez, P.; Engemann, D.; Faugeras, F.; Weiss, N.; Demeret, S.; et al. Combined behavioral and electrophysiological evidence for a direct cortical effect of prefrontal tDCS on disorders of consciousness. Sci. Rep. 2020, 10, 1–16. [Google Scholar] [CrossRef]
- Morales-Quezada, L.; Leite, J.; Carvalho, S.; Castillo-Saavedra, L.; Cosmo, C.; Fregni, F. Behavioral effects of transcranial pulsed current stimulation (tPCS): Speed-Accuracy tradeoff in attention switching task. Neurosci. Res. 2016, 109, 48–53. [Google Scholar] [CrossRef]
- Thibaut, A.; Russo, C.; Hurtado-Puerto, A.M.; Morales-Quezada, J.L.; Deitos, A.; Petrozza, J.C.; Freedman, S.; Fregni, F. Effects of transcranial direct current stimulation, transcranial pulsed current stimulation, and their combination on brain oscillations in patients with chronic visceral pain: A pilot crossover randomized controlled study. Front. Neurol. 2017, 8, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Thibaut, A.; Di Perri, C.; Chatelle, C.; Bruno, M.-A.; Bahri, M.A.; Wannez, S.; Piarulli, A.; Bernard, C.; Martial, C.; Heine, L.; et al. Clinical response to tDCS depends on residual brain metabolism and grey matter integrity in patients with minimally conscious state. Brain Stimul. 2015, 8, 1116–1123. [Google Scholar] [CrossRef]
- McDonnell, M.D.; Ward, L.M. The benefits of noise in neural systems: Bridging theory and experiment. Nat. Rev. Neurosci. 2011, 12, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Vasquez, A.C.; Thibaut, A.; Morales-Quezada, L.; Leite, J.; Fregni, F. Patterns of brain oscillations across different electrode montages in transcranial pulsed current stimulation. NeuroReport 2017, 28, 421–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thibaut, A.; Piarulli, A.; Martens, G.; Chatelle, C.; Laureys, S. Effect of multichannel transcranial direct current stimulation to reduce hypertonia in individuals with prolonged disorders of consciousness: A randomized controlled pilot study. Ann. Phys. Rehabil. Med. 2019, 62, 418–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chennu, S.; Bekinschtein, T.A. Arousal modulates auditory attention and awareness: Insights from Sleep, Sedation, and Disorders of consciousness. Front. Psychol. 2012, 3, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gosseries, O.; Vanhaudenhuyse, A.; Bruno, M.-A.; Demertzi, A.; Schnakers, C.; Boly, M.M.; Maudoux, A.; Moonen, G.; Laureys, S. Disorders of consciousness: Coma, vegetative and minimally conscious states. In States of Consciousness; Springer: Berlin/Heidelberg, Germany, 2011; Volume 2011, pp. 29–55. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Age | Sex | Diagnosis | TSI | Etiology | Order of Sessions | Measure | Pre Sham | Post Sham | Pre tDCS | Post tDCS | Pre tPCS | Post tPCS |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ID01 | 71 | F | MCS+ | 12.8 | Stroke | sham tPCS tDCS | CRS-R | 15 | 13 | 10 | 15 | 14 | 14 |
| Modified Index | 49.6 | 47.5 | 3.5 | 64.9 | 55.9 | 49.3 | |||||||
| ID02 | 31 | F | MCS+ | 5 | Anoxic | tDCS tPCS sham | CRS-R | 8 | 10 | 9 | 9 | 9 | 9 |
| Modified Index | 14.9 | 31.5 | 16 | 15.9 | 23.2 | 15.2 | |||||||
| ID03 | 50 | F | MCS− | 4 | Stroke | tPCS tDCS sham | CRS-R | 4 | 2 | 2 | 4 | 7 | 5 |
| Modified Index | 3.4 | 1.37 | 1.37 | 1.3 | 21.1 | 11.8 | |||||||
| ID04 | 63 | M | MCS− | 2.5 | TBI | sham tPCS | CRS-R | 5 | 6 | N/A | N/A | 3 | 3 |
| Modified Index | 19.8 | 6.5 | N/A | N/A | 3.1 | 3.1 | |||||||
| ID05 | 47 | F | MCS− | 3 | Stroke | sham tDCS tPCS | CRS-R | 7 | 5 | 9 | 6 | 7 | 8 |
| Modified Index | 5.8 | 3.8 | 15.2 | 4.8 | 6.9 | 7 | |||||||
| ID06 | 65 | F | MCS+ | 5.8 | Stroke | tPCS sham tDCS | CRS-R | 5 | 4 | 5 | 10 | 4 | 7 |
| Modified Index | 4.5 | 3.5 | 4.5 | 29.8 | 3.4 | 13.1 | |||||||
| ID07 | 60 | F | eMCS | 33 | TBI | tDCS sham tPCS | CRS-R | 14 | 15 | 18 | 19 | 17 | 16 |
| Modified Index | 55.8 | 57.6 | 82 | 90 | 73.6 | 65.2 | |||||||
| ID08 | 34 | M | MCS− | 4.5 | TBI | tPCS tDCS sham | CRS-R | 8 | 10 | 11 | 10 | 10 | 10 |
| Modified Index | 22.2 | 23.6 | 24.6 | 23.6 | 23.6 | 23.6 | |||||||
| ID09 | 51 | F | MCS− | 4 | Stroke | tDCS sham tPCS | CRS-R | 10 | 10 | 9 | 8 | 9 | 11 |
| Modified Index | 23.5 | 23.6 | 22.5 | 21.5 | 23.2 | 32.6 | |||||||
| ID10 | 23 | M | MCS+ | 2 | TBI | sham tPCS tDCS | CRS-R | 13 | 15 | 17 | 18 | 15 | 15 |
| Modified Index | 4.2 | 57 | 66.3 | 74.6 | 49.6 | 49.6 | |||||||
| ID11 | 53 | F | MCS− | 3 | Stroke | sham tDCS tPCS | CRS-R | 7 | 6 | 7 | 8 | 6 | 5 |
| Modified Index | 14.5 | 13.5 | 5.9 | 7 | 6.2 | 4.5 | |||||||
| ID12 | 56 | M | eMCS | 3 | Stroke | tDCS tPCS sham | CRS-R | 20 | 19 | 17 | 18 | 20 | 20 |
| Modified Index | 91.3 | 82.3 | 66.3 | 74.6 | 91.3 | 91.3 |
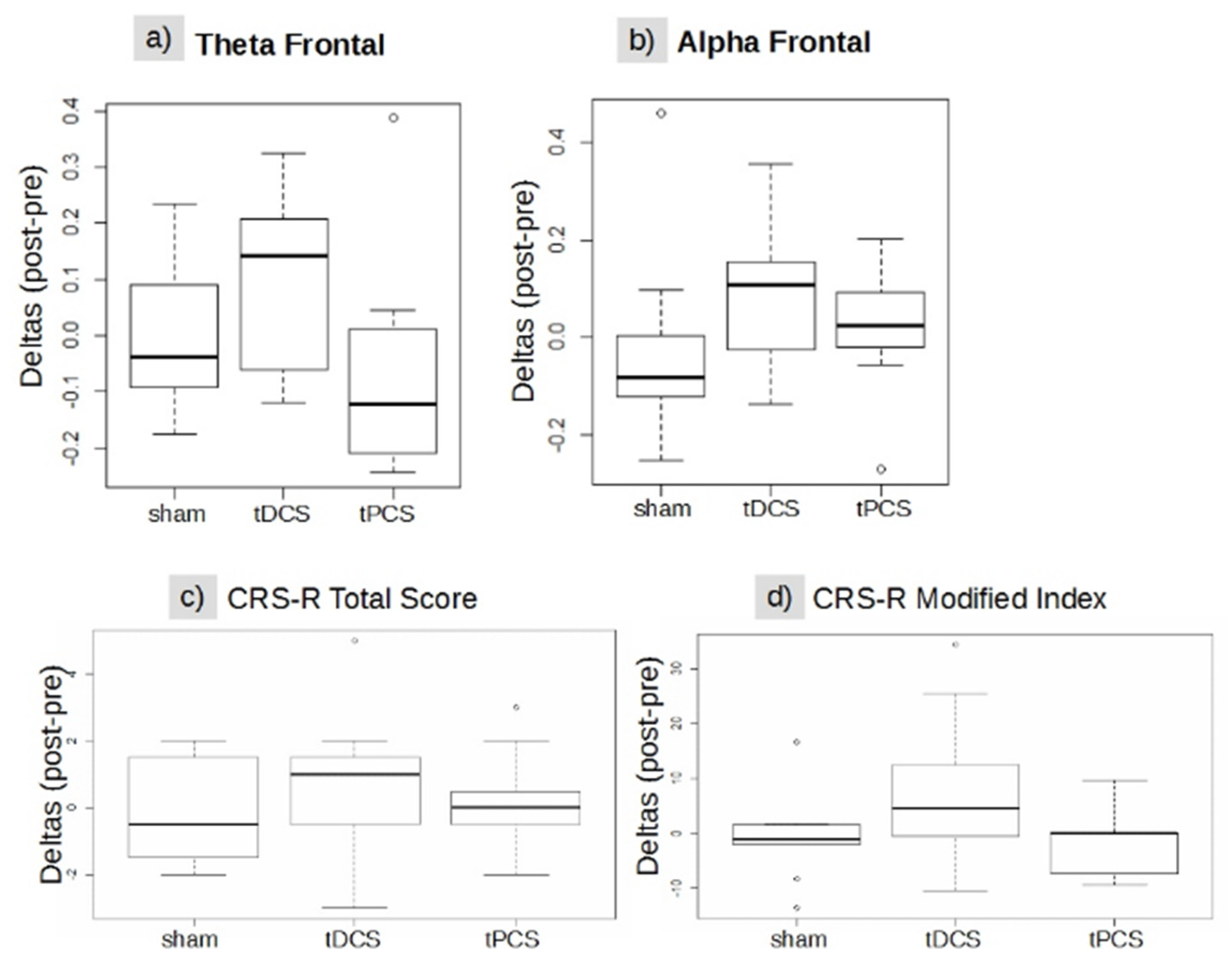
| Sham | tDCS | tPCS | Chi-Squared (p-Value) | |
|---|---|---|---|---|
| Alpha frontal | −0.08 (−0.12; 0.01) | 0.10 (−0.016; 0.15) | 0.02 (−01; 0.09) | 4.90 (0.08) |
| Alpha parietal | 0.000 (−0.02; 0.06) | 0.045 (0.001; 0.12) | 0.011 (−0.04; 0.13) | 0.673 (0.71) |
| Theta frontal | −0.037 (−0.09; 0.09) | 0.142 (−0.05; 0.19) | −0.122 (−0.20; 0.01) | 5.697 (0.05) |
| Theta parietal | −0.12 (−0.20; 0.00) | −0.04 (−0.19; 0.03) | −0.01 (−0.09; 0.00) | 0.08 (0.64) |
| CRS-R total score | −0.5 (−1; 1.25) | 1 (−0.5; 1.5) | 0 (−0.25; 0.25) | 1.47 (0.49) |
| CRS-R modified index | −1.04 (−2.09; 1.47) | 4.52 (−0.26; 10.42) | 0 (−6.93; 0) | 4.11 (0.13) |
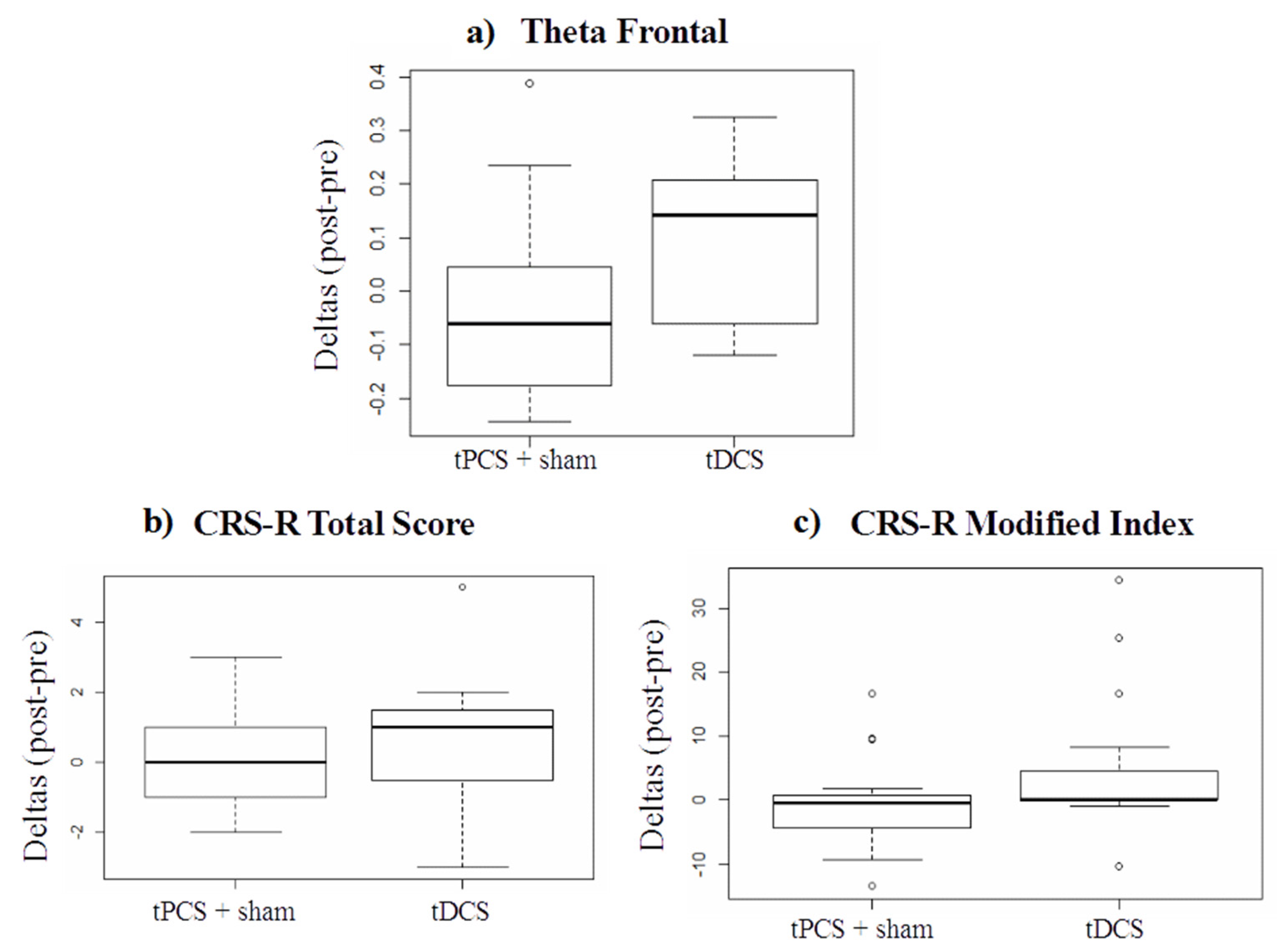
| ([tPCS + sham]) | tDCS | W (p-Value) | |
|---|---|---|---|
| Alpha frontal | −0.00 (−0.10; 0.05) | 0.10 (−0.01; 0.15) | 71 (0.11) |
| Alpha parietal | 0.00 (−0.02; 0.11) | 0.04 (0.00; 0.12) | 96 (0.58) |
| Theta frontal | −0.060 (−0.16; 0.02) | 0.14 (−0.05; 0.20) | 59 (0.04) * |
| Theta parietal | −0.046 (−0.15; 0.00) | −0.03 (−0.19; 0.03) | 104 (0.82) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barra, A.; Rosenfelder, M.; Mortaheb, S.; Carrière, M.; Martens, G.; Bodien, Y.G.; Morales-Quezada, L.; Bender, A.; Laureys, S.; Thibaut, A.; et al. Transcranial Pulsed-Current Stimulation versus Transcranial Direct Current Stimulation in Patients with Disorders of Consciousness: A Pilot, Sham-Controlled Cross-Over Double-Blind Study. Brain Sci. 2022, 12, 429. https://doi.org/10.3390/brainsci12040429
Barra A, Rosenfelder M, Mortaheb S, Carrière M, Martens G, Bodien YG, Morales-Quezada L, Bender A, Laureys S, Thibaut A, et al. Transcranial Pulsed-Current Stimulation versus Transcranial Direct Current Stimulation in Patients with Disorders of Consciousness: A Pilot, Sham-Controlled Cross-Over Double-Blind Study. Brain Sciences. 2022; 12(4):429. https://doi.org/10.3390/brainsci12040429
Chicago/Turabian StyleBarra, Alice, Martin Rosenfelder, Sepehr Mortaheb, Manon Carrière, Geraldine Martens, Yelena G. Bodien, Leon Morales-Quezada, Andreas Bender, Steven Laureys, Aurore Thibaut, and et al. 2022. "Transcranial Pulsed-Current Stimulation versus Transcranial Direct Current Stimulation in Patients with Disorders of Consciousness: A Pilot, Sham-Controlled Cross-Over Double-Blind Study" Brain Sciences 12, no. 4: 429. https://doi.org/10.3390/brainsci12040429