
The Importance of Material Used in Speech Therapy: Two Case Studies in Minimally Conscious State Patients

 ,
,
Abstract
:1. Introduction
2. The Effect of Autobiographical Material during a Speech Therapy Session. Case Study One
2.1. Method
2.1.1. Patient
2.1.2. Materials
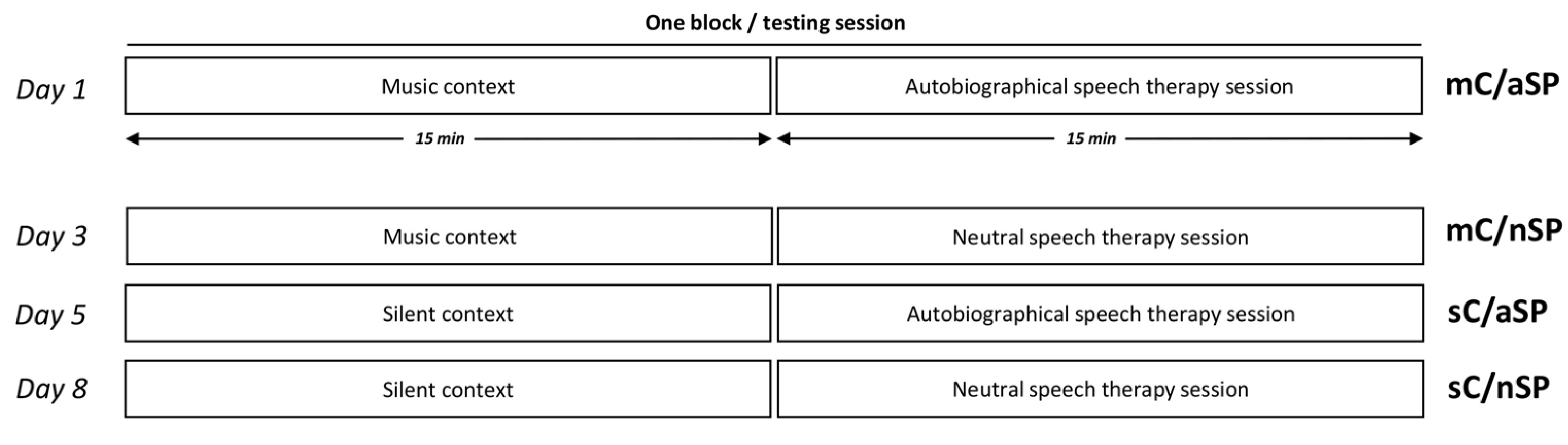
2.1.3. Experimental Protocol
2.1.4. Behavioral Assessment
2.1.5. Data Analysis
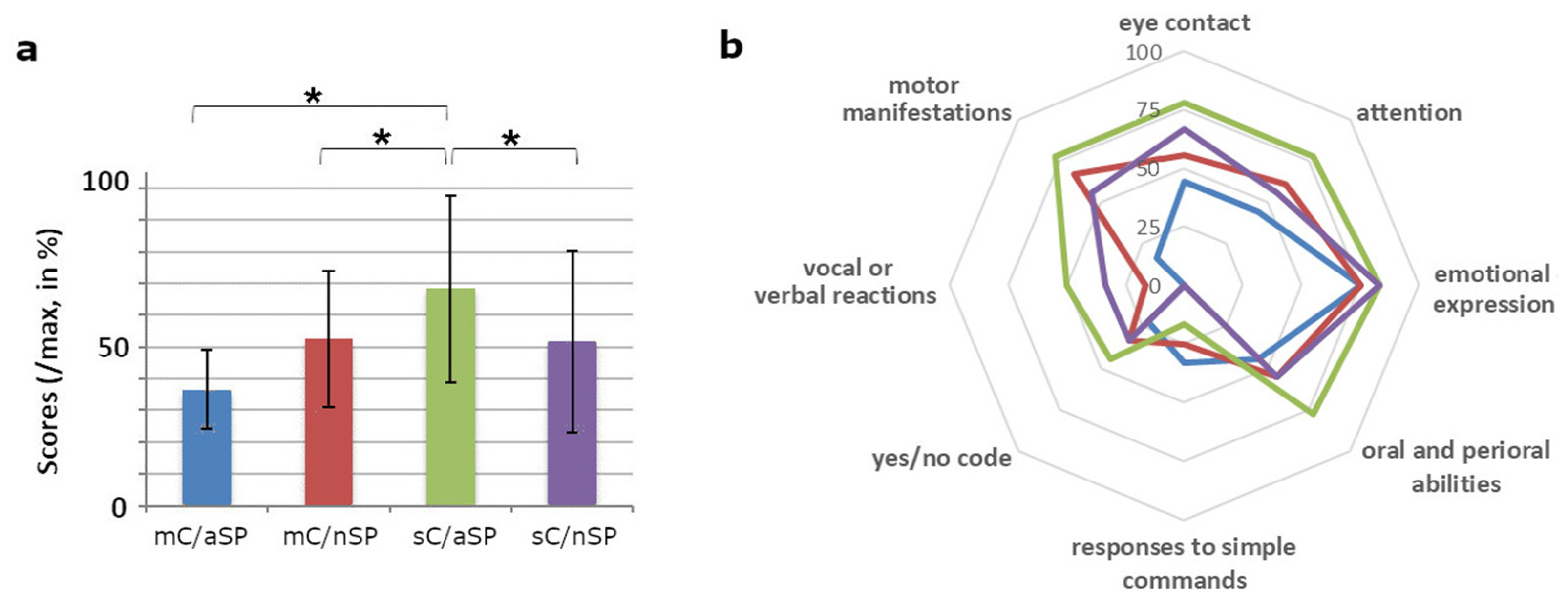
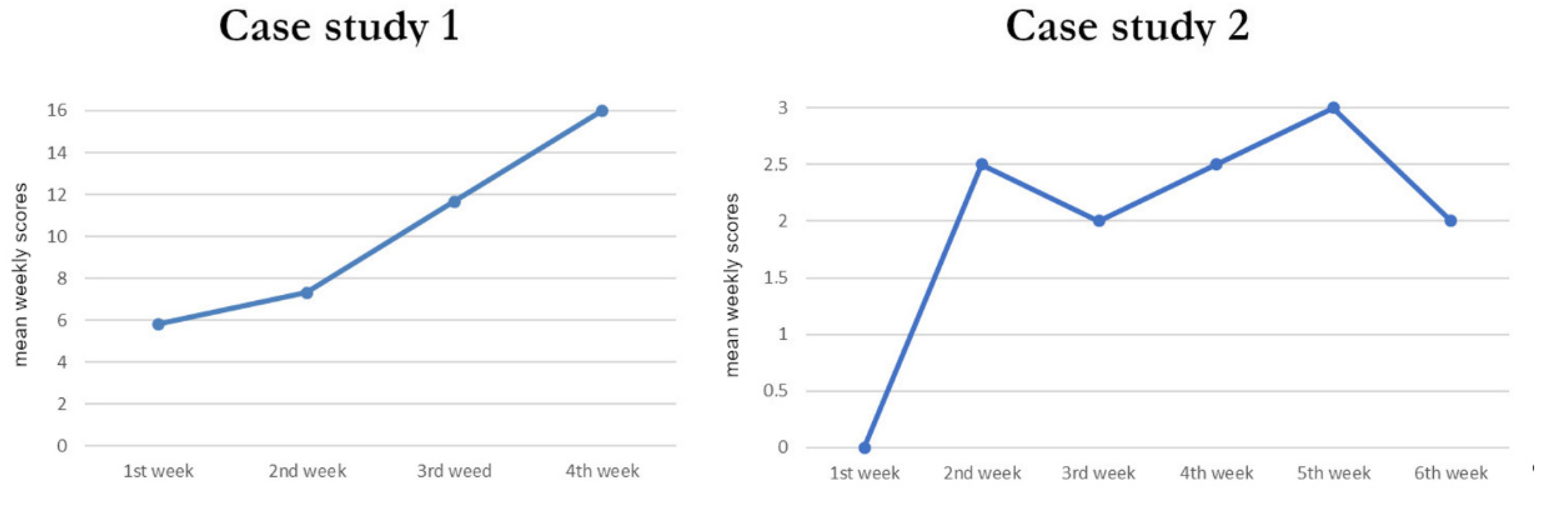
2.2. Results
3. The Effect of Music Tempo on Subsequent Behavioral Assessment. Case Study Two
3.1. Method
3.1.1. Patient
3.1.2. Materials
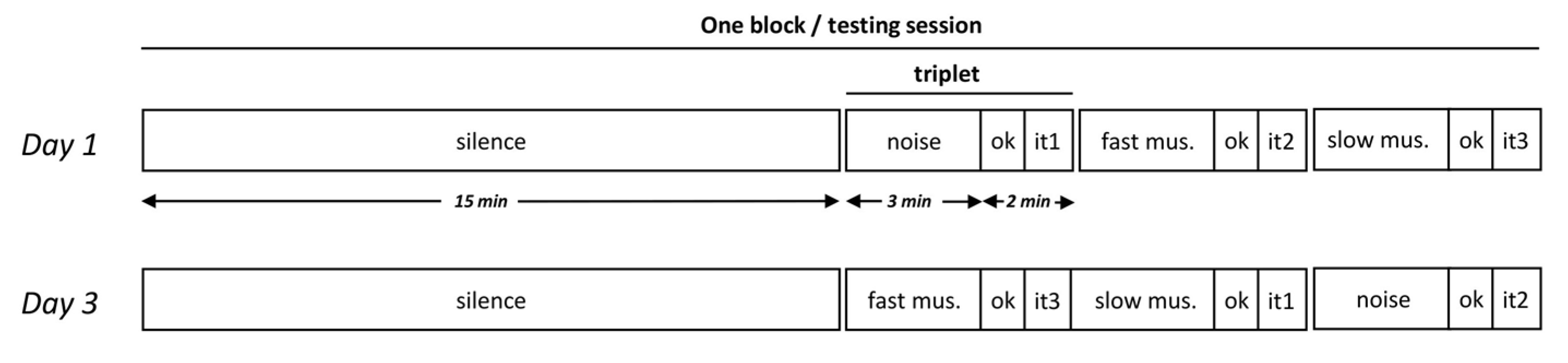
3.1.3. Experimental Protocol
3.1.4. Behavioral Assessment
3.1.5. Data Analysis
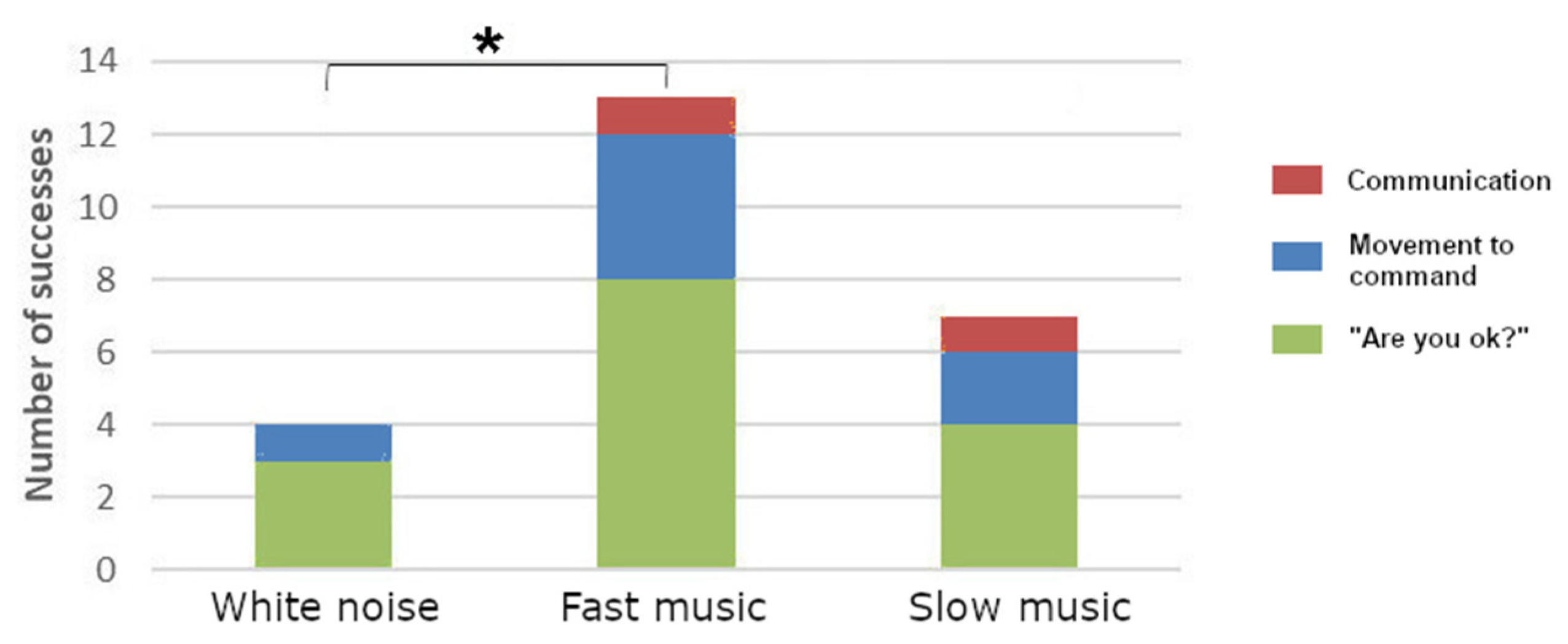
3.2. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scoring/Items | Qualitative Observations | |
|---|---|---|
| PRECURSORS TO COMMUNICATION |
| |
| Score: /8 | ||
| ORAL/PERIORAL |
| |
| Score: /3 | ||
| COMMUNICATION SKILLS |
| Yes/no code: Spontaneous? On solicitation? Reliable? |
| Score: /10 | ||
| OVERALL SCORE: /21 |
- □
- Appeasement/sleepiness
- □
- Agitation
- □
- Opening the eyes when the door is opened
- □
- Opening of the eyes at the beginning of the music
- □
- Orientation of the eyes towards the speakers
- □
- Emotional reactions (smiling, crying, laughing etc.)
- □
- Looking through the door
- □
- Others: …………………………………………………………………..
Appendix B
| Reflex Behaviors | Number of Achievement Observations |
| Chewing | |
| Swallowing | |
| Yawning | |
| Coughing | |
| Non-reflex behaviors | Number of achievement Observations |
| Moving the head | |
| Changing of eyes orientation | |
| Changing in position | |
| Scratching | |
| Touching a part of the body | |
| Acting on an element of the environment (tracheostomy cannula, saturometer, wheelchair, etc.) | |
| Nodding |
References
- Multi-Society Task Force on PVS. Medical aspects of the persistent vegetative state. N. Engl. J. Med. 1994, 330, 1499–1508. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T.; Ashwal, S.; Childs, N.; Cranford, R.; Jennett, B.; Katz, D.I.; Kelly, J.H.; Rosenberg, J.; Whyte, J.; Zafonte, R.D.; et al. The minimally conscious state definition and diagnostic criteria. Neurology 2002, 58, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Bruno, M.-A.; Vanhaudenhuyse, A.; Thibaut, A.; Moonen, G.; Laureys, S. From unresponsive wakefulness to minimally conscious PLUS and functional locked-in syndromes: Recent advances in our understanding of disorders of consciousness. J. Neurol. 2011, 258, 1373–1384. [Google Scholar] [CrossRef] [PubMed]
- Cassol, H.; Aubinet, C.; Thibaut, A.; Wannez, S.; Martial, C.; Martens, G.; Laureys, S. Diagnostic, pronostic et traitements des troubles de la conscience. NPG Neurol.-Psychiatr.-Gériatrie 2018, 18, 47–59. [Google Scholar] [CrossRef] [Green Version]
- General Nomenclature of Speech Therapy Procedures, French Official Journal. 2 July 2019. Available online: https://www.legifrance.gouv.fr/jorf/jo/2019/07/02/0151 (accessed on 16 January 2021).
- Mortensen, J.; Jensen, D.; Kjaersgaard, A. A validation study of the Facial-Oral Tract Therapy Swallowing Assessment of Saliva. Clin. Rehabil. 2016, 30, 410–415. [Google Scholar] [CrossRef]
- Mélotte, E.; Belorgeot, M.; Herr, R.; Simon, J.; Kaux, J.F.; Laureys, S.; Sanz, L.R.; Lagier, A.; Morsomme, D.; Pellas, F.; et al. The Development and Validation of the SWADOC: A Study Protocol for a Multicenter Prospective Cohort Study. Front. Neurol. 2021, 12, 662634. [Google Scholar] [CrossRef]
- Lancioni, G.E.; Bosco, A.; Belardinelli, M.O.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J. An overview of intervention options for promoting adaptive behavior of persons with acquired brain injury and minimally conscious state. Res. Dev. Disabil. 2010, 31, 1121–1134. [Google Scholar] [CrossRef]
- Di Stefano, C.; Cortesi, A.; Masotti, S.; Simoncini, L.; Piperno, R. Increased behavioural responsiveness with complex stimulation in VS and MCS: Preliminary results. Brain Inj. 2012, 26, 1250–1256. [Google Scholar] [CrossRef]
- Meyer, M.J.; Megyesi, J.; Meythaler, J.; Murie-Fernandez, M.; Aubut, J.A.; Foley, N.; Salter, K.; Bayley, M.; Marshall, S.; Teasell, R. Acute management of acquired brain injury Part III: An evidence-based review of interventions used to promote arousal from coma. Brain Inj. 2010, 24, 722–729. [Google Scholar] [CrossRef]
- Woisard, V.; Puech, M. La Réhabilitation de la Déglutition Chez L’adulte, 2nd ed.; De boeck Solal: Marseille, France, 2013. [Google Scholar]
- Perrin, F.; Castro, M.; Tillmann, B.; Luauté, J. Promoting the use of personally relevant stimuli for investigating patients with disorders of consciousness. Front. Psychol. 2015, 6, 1102. [Google Scholar] [CrossRef] [Green Version]
- Bekinschtein, T.; Niklison, J.; Sigman, L.; Manes, F.; Leiguarda, R.; Armony, J.; Owen, A.; Carpintiero, S.; Olmos, L. Emotion processing in the minimally conscious state. J. Neurol. Neurosurg. Psychiatry 2014, 75, 788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharon, H.; Pasternak, Y.; Ben Simon, E.; Gruberger, M.; Giladi, N.; Krimchanski, B.Z.; Hassin, D.; Hendler, T. Emotional Processing of Personally Familiar Faces in the Vegetative State. PLoS ONE 2013, 8, 74711. [Google Scholar]
- Signorino, M.; D’Acunto, S.; Cercaci, S.; Pietropaoli, P.; Angeleri, F. The P300 in traumatic coma: Conditioning of the odd-ball paradigm. J. Psychophysiol. 1997, 11, 59–70. [Google Scholar]
- Perrin, F.; Schnakers, C.; Schabus, M.; Degueldre, C.; Goldman, S.; Brédart, S.; Faymonville, M.-E.; Lamy, M.; Moonen, G.; Luxen, A.; et al. Brain response to one’s own name in vegetative state, minimally conscious state, and locked-in syndrome. Arch. Neurol. 2006, 63, 562–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verger, J.; Ruiz, S.; Tillmann, B.; Ben Romdhane, M.; De Quelen, M.; Castro, M.; Tell, L.; Luauté, J.; Perrin, F. Effets bénéfiques de la musique préférée sur les capacités cognitives des patients en état de conscience minimale. Rev. Neurol. 2014, 170, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Heine, L.; Tillmann, B.; Hauet, M.; Juliat, A.; Dubois, A.; Laureys, S.; Kandel, M.; Plailly, J.; Luauté, J.; Perrin, F. Effects of preference and sensory modality on behavioural reaction in patients with disorders of consciousness. Brain Inj. 2017, 31, 1307–1311. [Google Scholar] [CrossRef]
- Castro, M.; Tillmann, B.; Luauté, J.; Corneyllie, A.; Dailler, F.; André-Obadia, N.; Perrin, F. Boosting cognition with music in patients with disorders of consciousness. Neurorehabilit. Neural Repair 2015, 29, 734–742. [Google Scholar] [CrossRef]
- Altenmüller, E.; McPherson, G.E. Motor Learning and Instrumental Training. In Neurosciences in Music Pedagogy; Gruhn, W., Rauscher, F.H., Eds.; Nova Science: New York, NY, USA, 2007; pp. 121–143. [Google Scholar]
- Moussard, A.; Rochette, F.; Bigand, E. La musique comme outil de stimulation cognitive. L’année Psychol. 2012, 112, 499–542. [Google Scholar] [CrossRef]
- Wan, C.Y.; Schlaug, G. Music making as a tool for promoting brain plasticity across the life span. Neurosci. A Rev. J. Bringing Neurobiol. Neurol. Psychiatry 2010, 16, 566–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altenmüller, E.; Schlaug, G. Apollo’s gift: New aspects of neurologic music therapy. Prog. Brain Res. 2015, 217, 237–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukui, H.; Toyoshima, K. Music facilitate the neurogenesis, regeneration and repair of neurons. Med. Hypotheses 2008, 71, 765–769. [Google Scholar] [CrossRef]
- Grimm, T.; Kreutz, G. Music interventions in disorders of consciousness (DOC)—A systematic review. Brain Inj. 2018, 32, 704–714. [Google Scholar] [CrossRef] [PubMed]
- Magee, W.L. Music therapy with patients in low awareness states: Approaches to assessment and treatment in multidisciplinary care. Neuropsychol. Rehabil. 2005, 15, 522–536. [Google Scholar] [CrossRef] [PubMed]
- Magee, W.L. Music as a diagnostic tool in low awareness states: Considering limbic responses. Brain Inj. 2007, 21, 593–599. [Google Scholar] [CrossRef]
- Baker, F.A. Modifying the melodic intonation therapy program for adults with severe non-fluent aphasia. Music Ther. Perspect. 2000, 18, 110–114. [Google Scholar] [CrossRef]
- Cohen, N.S. The use of superimposed rhythm to decrease the rate of speech in a braindamaged adolescent. J. Music Ther. 1988, 25, 85–93. [Google Scholar] [CrossRef]
- Cohen, N.S. The effect of singing instruction on the speech production of neurologically impaired persons. J. Music Ther. 1992, 29, 87–102. [Google Scholar] [CrossRef]
- Cohen, N.S.; Masse, R. The Application of Singing and Rhythmic Instruction as a Therapeutic Intervention for Persons with Neurogenic Communication Disorders. J. Music Ther. 1993, 30, 81–99. [Google Scholar] [CrossRef]
- Pilon, M.A.; McIntosh, K.W.; Thaut, M.H. Auditory vs. visual speech timing cues as external rate control to enhance verbal intelligibility in mixed spastic-ataxic dysarthric speakers: A pilot study. Brain Inj. 1998, 12, 793–803. [Google Scholar] [CrossRef]
- Heine, L.; Castro, M.; Martial, C.; Tillmann, B.; Laureys, S.; Perrin, F. Exploration of Functional Connectivity During Preferred Music Stimulation in Patients with Disorders of Consciousness. Front. Psychol. 2015, 6, 1704. [Google Scholar] [CrossRef] [PubMed]
- Carrière, M.; Larroque, S.K.; Martial, C.; Bahri, M.A.; Aubinet, C.; Perrin, F.; Laureys, S.; Heine, L. An Echo of Consciousness: Brain Function During Preferred Music. Brain Connect. 2020, 10, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, L.; Porta, C.; Sleight, P. Cardiovascular, cerebrovascular, and respiratory changes induced by different types of music in musicians and non-musicians: The importance of silence. Heart 2006, 92, 445–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez, P.; Danuser, B. Relationships Between Musical Structure and Psychophysiological Measures of Emotion. Emotion 2007, 7, 377–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, K.; Kurita, A.; Takase, B.; Otsuka, T.; Kodani, E.; Kusama, Y.; Atarashi, H.; Mizuno, K. Effects of music therapy on autonomic nervous system activity, incidence of heart failure events, and plasma cytokine and catecholamine levels in elderly patients with cerebrovascular disease and dementia. Int. Heart J. 2009, 50, 95–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacino, J.T.; Kalmar, K.; Whyte, J. The JFK Coma Recovery Scale-Revised: Measurement characteristics and diagnostic utility. Arch. Phys. Med. Rehabil. 2004, 85, 2020–2029. [Google Scholar] [CrossRef] [PubMed]
- Shiel, A.; Horn, S.A.; Wilson, B.A.; Watson, M.J.; Campbell, M.J.; McLellan, D.L. The Wessex Head Injury Matrix (WHIM) main scale: A preliminary report on a scale to assess and monitor patient recovery after severe head injury. Clin. Rehabil. 2000, 14, 408–416. [Google Scholar] [CrossRef]
- Garin, J.; Reina, M. Création et Validation d’une Echelle d’Évaluation de la Communication pour des Patients en Phase d’Éveil de Coma (ECEC). 2013. Available online: http://docnum.univ-lorraine.fr/public/BUMED_MORT_2013_GARIN_JULIE_REINA_MARGOT.pdf (accessed on 16 January 2021).
- Rousseaux, M.; Delacourt, A.; Wyrzykowski, N.; Lefeuvre, M. TLC: Test Lillois de communication. Communication Test; OrthoEdition: Isbergues, France, 2001; 87p. [Google Scholar]
- Soto, D.; Funes, M.I.; Guzmán-García, A.; Warbrick, T.; Rotshtein, P.; Humphreys, G.W. Pleasant music overcomes the loss of awareness in patients with visual neglect. Proc. Natl. Acad. Sci. USA 2009, 106, 6011–6016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalfa, S.; Bella, S.D.; Roy, M.; Peretz, I.; Lupien, S.J. Effects of relaxing music on salivary cortisol level after psychological stress. Ann. N. Y. Acad. Sci. 2003, 999, 374–376. [Google Scholar] [CrossRef]
- Magee, W.L. Music in the diagnosis, treatment and prognosis of people with prolonged disorders of consciousness. Neuropsychol. Rehabil. 2018, 28, 1331–1339. [Google Scholar] [CrossRef]
- Mollakazemi, M.J.; Biswal, D.; Elayi, S.C.; Thyagarajan, S.; Evans, J. Synchronization of Autonomic and Cerebral Rhythms During Listening to Music: Effects of Tempo and Cognition of Songs. Physiol. Res. 2019, 68, 1005–1019. [Google Scholar] [CrossRef]
- Pape, T.L.-B.; Rosenow, J.M.; Steiner, M.; Parrish, T.; Guernon, A.; Harton, B.; Patil, V.; Bhaumik, D.K.; McNamee, S.; Walker, M.; et al. Placebo-controlled trial of familiar auditory sensory training for acute severe traumatic brain injury: A preliminary report. Neurorehabilit. Neural Repair 2015, 29, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Formisano, R.; Vinicola, V.; Penta, F.; Matteis, M.; Brunelli, S.; Weckel, J.W. Active music therapy in the rehabilitation of severe brain injured patients during coma recovery. Ann. Dell’istituto Super. Sanita 2001, 37, 627–630. [Google Scholar]
- Cheng, L.; Cortese, D.; Monti, M.M.; Wang, F.; Riganello, F.; Arcuri, F.; Di, H.; Schnakers, C. Do Sensory Stimulation Programs Have an Impact on Consciousness Recovery? Front. Neurol. 2018, 9, 826. [Google Scholar] [CrossRef] [PubMed] [Green Version]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sautet, A.; Hurtado, L.; Fiveash, A.; Baron, L.; De Quelen, M.; Perrin, F. The Importance of Material Used in Speech Therapy: Two Case Studies in Minimally Conscious State Patients. Brain Sci. 2022, 12, 483. https://doi.org/10.3390/brainsci12040483
Sautet A, Hurtado L, Fiveash A, Baron L, De Quelen M, Perrin F. The Importance of Material Used in Speech Therapy: Two Case Studies in Minimally Conscious State Patients. Brain Sciences. 2022; 12(4):483. https://doi.org/10.3390/brainsci12040483
Chicago/Turabian StyleSautet, Alice, Laura Hurtado, Anna Fiveash, Leslie Baron, Mélaine De Quelen, and Fabien Perrin. 2022. "The Importance of Material Used in Speech Therapy: Two Case Studies in Minimally Conscious State Patients" Brain Sciences 12, no. 4: 483. https://doi.org/10.3390/brainsci12040483