
Pragmatic Profiles of Adults with Fragile X Syndrome and Williams Syndrome




Abstract
:1. Introduction
1.1. Pragmatic Impairment across Neurodevelopmental Disorders
1.2. Pragmatic Skills in FXS and in WS: Narratives and Conversation
1.3. Pragmatic Skills and Autistic Symptoms in FXS and WS
1.4. Assessment of Pragmatic Impairment
1.5. Objectives
- -
- Maxim of quality (MQL): truthfulness and adjustment to world reality.
- -
- Maxim of relation (MRL): non-related, tangential, and perseverations of topic.
- -
- Maxim of quantity (MQT): redundant, vague, excessive, and reduced utterances.
- -
- Maxim of manner (MMN): repetitions, reformulations, perseverations of form, and alterations of the syntactic order.
- -
- AVI of cooperation: aggregate index of violations of all the maxims.
- -
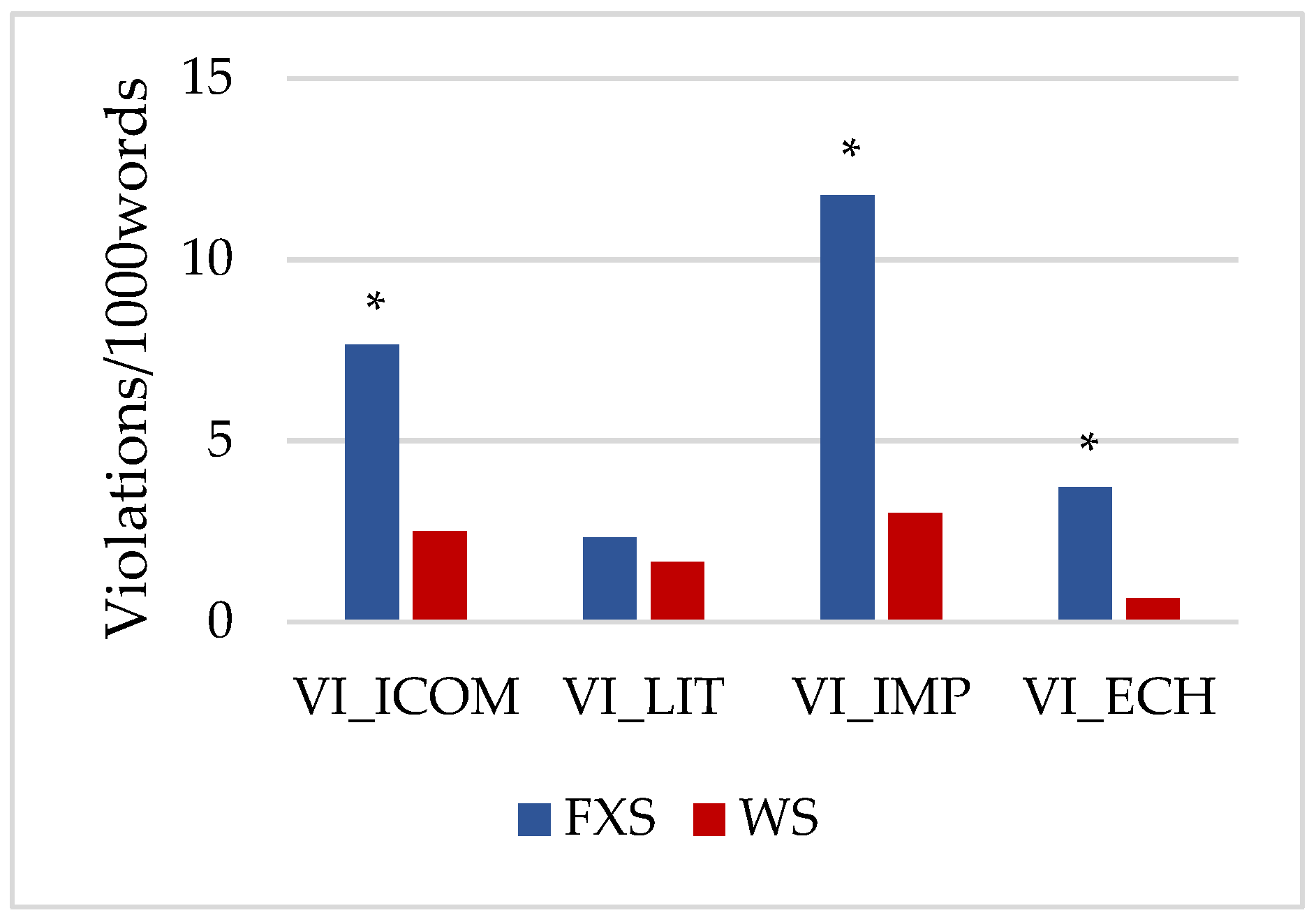
- AVI of conversational response: incomprehension, literal interpretation, impulsivity, and echolalia.
2. Materials and Methods
2.1. Participants
2.2. Instrument
- (a)
- Maxim of Quality (MQL)*INV: and what are you working on here nowadays?*PAR: on nothing.%xepr:$i5:MQL:IMP
- (b)
- Maxim of Relation (MRL)*INV: (that cap) do you know which team it belongs to?*PAR: of basketball.%xepr:$i5:MRL:TNG:ICOM:LIT
- (c)
- Maxim of Quantity (MQT)*INV: why she was called so?*PAR: she was called so.%xepr:$i5:MQT:RUT:ECH
- (d)
- Maxim of Manner (MMN)*INV: what happened to the wolf and the stones?*PAR: and then what else? (.) and then (.) and then something else (.) and then something else (.) and then something else yet (.) and then something else yet about stones.%xepr:$i5:MMN:REP:PER_F
2.3. Procedure
2.4. Data Analysis
3. Results
4. Discussion
4.1. Within-Syndrome Differences in the Profiles of Conversational Cooperation
4.2. Between-Syndrome Differences in the Profiles of Conversational Cooperation
4.3. Differences in the Profiles of Conversational Response
4.4. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Enunciative Pragmatics %xepr Inferences Sublevel $i | ||||
|---|---|---|---|---|
| PREP Item | Main Label | Secondary Label 1 | Secondary Label 2 | Optional Label |
| 5. Cooperative Principle: Maxims $i5 | Maxim of Quality MQL | Question QST | World Reality WOR | Impulsivity IMP Inadequate Comprehension ICOM Literal Language LIT Perseveration PER Echolalia ECH Fabulation FAB Theory of Mind TOM |
| Answer ASW | ||||
| Report RPT | ||||
| Maxim of Quantity MQT | Redundant Utterances RUT | |||
| Vague Utterances VUT | ||||
| Excessive Verbal Production EVP | ||||
| Reduced Verbal Production RVP | Onomatopoeia ONO | |||
| Interjection INT | ||||
| Maxim of Relation MRL | QST | Non-related NRL Tangential TNG Perseveration (of topic) PER | ||
| ASW | ||||
| RPT | ||||
| Maxim of Manner MMN | Repetition REP | |||
| Reformulation REF | ||||
| Perseveration PER | ||||
| Word Order ORD | Addition ADI | |||
| Omission OMI | ||||
| Inversion INV | ||||
| Substitution SST | ||||
| Particularized Implicatures PIM | Flouting MQL PMQL | In/Adequate Comprehension ACOM/ICOM In/Adequate Production ADQ/IDQ | ||
| Flouting MQT PMQT | ||||
| Flouting MRL PMRL | ||||
| Flouting MMN PMMN | ||||
References
- Bellugi, U.; Lichtenberger, L.; Jones, W.; Lai, Z.; George, M.I. The neurocognitive profile of Williams Syndrome: A complex pattern of strengths and weaknesses. J. Cogn. Neurosci. 2000, 12 (Suppl. 1), 7–29. [Google Scholar] [CrossRef]
- Hagerman, R.J.; Berry-Kravis, E.; Hazlett, H.C.; Bailey, D.B.; Moine, H.; Kooy, R.F.; Tassone, F.; Gantois, I.; Sonenberg, N.; Mandel, J.L.; et al. Fragile X syndrome. Nat. Rev. Dis. Primers 2017, 3, 17065. [Google Scholar] [CrossRef]
- Mervis, C.B.; Klein-Tasman, B.P. Williams syndrome: Cognition, personality, and adaptive behavior. Ment. Retard. Dev. Disabil. Res. Rev. 2000, 6, 148–158. [Google Scholar] [CrossRef]
- Royston, R.; Waite, J.; Howlin, P. Williams syndrome: Recent advances in our understanding of cognitive, social and psychological functioning. Curr. Opin. Psychiatry 2019, 32, 60–66. [Google Scholar] [CrossRef] [Green Version]
- Smith, L.E.; Barker, E.T.; Seltzer, M.M.; Abbeduto, L.; Greenberg, J.S. Behavioral phenotype of Fragile X syndrome in adolescence and adulthood. Am. J. Intellect. Dev. Disabil. 2012, 117, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Codina-Sola, M.; Costa-Roger, M.; Pérez-García, D.; Flores, R.; Palacios-Verdú, M.G.; Cusco, I.; Pérez-Jurado, L.A. Genetic factors contributing to autism spectrum disorder in Williams-Beuren syndrome. J. Med. Genet. 2019, 56, 801–808. [Google Scholar] [CrossRef] [Green Version]
- Bartholomay, K.L.; Lee, C.H.; Bruno, J.L.; Lightbody, A.A.; Reiss, A.L. Closing the Gender Gap in Fragile X Syndrome: Review onf Females with Fragile X Syndrome and Preliminary Research Findings. Brain Sci. 2019, 9, 11. [Google Scholar] [CrossRef] [Green Version]
- Pérez-García, D.; Brun-Gasca, C.; Pérez-Jurado, L.A.; Mervis, C.B. Behavioral Profiles of Children with Williams Syndrome from Spain and the United States: Cross-Cultural Similarities and Differences. Am. J. Intellect. Dev. Disabil. 2017, 122, 156–172. [Google Scholar] [CrossRef] [Green Version]
- Abbeduto, L.; Brady, N.; Kover, S.T. Language development and Fragile X syndrome: Profiles, syndrome-specificity, and within-syndrome differences. Ment. Retard. Dev. Disabil. Res. Rev. 2007, 13, 36–46. [Google Scholar] [CrossRef]
- Brock, J. Language abilities in Williams syndrome: A critical review. Dev. Psychopathol. 2007, 19, 97–127. [Google Scholar] [CrossRef] [Green Version]
- Finestack, L.H.; Richmond, E.K.; Abbeduto, L. Language development in individuals with Fragile X syndrome. Top. Lang. Disord. 2009, 29, 133–148. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.M.; Abbeduto, L. Gender differences in repetitive language in Fragile X syndrome. J. Intellect. Disabil. Res. 2007, 51, 387–400. [Google Scholar] [CrossRef]
- Diez-Itza, E.; Miranda, M.; Pérez, V.; Martínez, V. Profiles of Grammatical Morphology in Spanish-Speaking Adolescents with Williams Syndrome and Down. In Atypical Language Development in Romance Languages; Aguilar-Mediavilla, E., Buil-Legaz, L., López-Penadés, R., Sánchez-Azanza, V.A., Adrover-Roig, D., Eds.; John Benjamins: Amsterdam, The Netherlands, 2019; pp. 219–234. [Google Scholar] [CrossRef]
- Belser, R.C.; Sudhalter, V. Conversational characteristics of children with Fragile X syndrome: Repetitive speech. Am. J. Ment. Retard. 2001, 106, 28–38. [Google Scholar] [CrossRef]
- Ng-Cordell, E.; Hanley, M.; Kelly, A.; Riby, D.M. Anxiety in Williams Syndrome: The Role of Social Behaviour, Executive Functions and Change Over Time. J. Autism Dev. Disord. 2018, 48, 796–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Hoyo Soriano, L.; Thurman, A.J.; Abbeduto, L. Specificity: A phenotypic comparison of communication-relevant domains between youth with Down syndrome and Fragile X syndrome. Front. Genet. 2018, 9, 424. [Google Scholar] [CrossRef]
- Rapin, I.; Allen, D. Developmental Language Disorders: Nosologic Considerations. In Neuropsychology of Language, Reading and Spelling; Kirk, U., Ed.; Academic Press: Cambridge, MA, USA, 1983; pp. 155–184. [Google Scholar] [CrossRef]
- Bishop, D.V. Pragmatic language impairment: A correlate of SLI, a distinct subgroup, or part of the autistic continuum? In Speech and Language Impairment in Children: Causes, Characteristics, Intervention and Outcome; Bishop, D.V., Leonard, L.B., Eds.; Psychology Press: Hove, UK, 2000; pp. 701–711. [Google Scholar] [CrossRef]
- Bishop, D.V.; Norbury, C.F. Exploring the borderlands of autistic disorder and specific language impairment: A study using standardised diagnostic instruments. J. Child Psychol. Psychiatry 2002, 43, 917–929. [Google Scholar] [CrossRef]
- Laws, G.; Bishop, D.V. Pragmatic language impairment and social deficits in Williams syndrome: A comparison with Down’s syndrome and specific language impairment. Int. J. Lang. Commun. Disord. 2004, 39, 45–64. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Swineford, L.B.; Thurm, A.; Baird, G.; Wetherby, A.M.; Swedo, S. Social (pragmatic) communication disorder: A research review of this new DSM-5 diagnostic category. J. Neurodev. Disord. 2014, 6, 41. [Google Scholar] [CrossRef] [Green Version]
- Brukner-Wertman, Y.; Laor, N.; Golan, O. Social (pragmatic) communication disorder and its relation to the autism spectrum: Dilemmas arising from the DSM-5 classification. J. Autism Dev. Disord. 2016, 46, 2821–2829. [Google Scholar] [CrossRef]
- Norbury, C.F. Practitioner review: Social (pragmatic) communication disorder conceptualization, evidence and clinical implications. J. Child Psychol. Psychiatry 2014, 55, 204–216. [Google Scholar] [CrossRef] [Green Version]
- Topal, Z.; Demir Samurcu, N.; Taskiran, S.; Tufan, A.E.; Semerci, B. Social communication disorder: A narrative review on current insights. Neuropsychiatr. Dis. Treat. 2018, 14, 2039–2046. [Google Scholar] [CrossRef] [Green Version]
- Abbeduto, L.; McDuffie, A.; Thurman, A.J.; Kover, S.T. Language development in individuals with intellectual and developmental disabilities: From phenotypes to treatments. Int. Rev. Res. Dev. Disabil. 2016, 50, 71–118. [Google Scholar] [CrossRef]
- Del Hoyo Soriano, L.; Thurman, A.J.; Harvey, D.; Kover, S.T.; Abbeduto, L. Expressive language development in adolescents with Down syndrome and Fragile X syndrome: Change over time and the role of family-related factors. J. Neurodev. Disord. 2020, 12, 18. [Google Scholar] [CrossRef]
- Diez-Itza, E.; Martínez, V.; Antón, A. Narrative competence in Spanish-speaking adults with Williams syndrome. Psicothema 2016, 28, 291–297. [Google Scholar] [CrossRef]
- Gonçalves, O.F.; Pinheiro, A.P.; Sampaio, A.; Sousa, N.; Fernández, M.; Henriques, M. The narrative profile in Williams syndrome: There is more to storytelling than just telling a story. Br. J. Dev. Disabil. 2010, 56, 89–109. [Google Scholar] [CrossRef]
- Estigarribia, B.; Martin, G.E.; Roberts, J.E.; Spencer, A.; Gucwa, A.; Sideris, J. Narrative skill in boys with Fragile X syndrome with and without autism spectrum disorder. Appl. Psycholinguist. 2011, 32, 359–388. [Google Scholar] [CrossRef] [Green Version]
- Finestack, L.H.; Palmer, M.; Abbeduto, L. Macrostructural narrative language of adolescents and young adults with Down syndrome or Fragile X syndrome. Am. J. Speech Lang. Pathol. 2012, 21, 29–46. [Google Scholar] [CrossRef] [Green Version]
- Hogan-Brown, A.L.; Losh, M.; Martin, G.E.; Mueffelmann, D.J. An investigation of narrative ability in boys with autism and Fragile X syndrome. Am. J. Intellect. Dev. Disabil. 2013, 118, 77–94. [Google Scholar] [CrossRef] [Green Version]
- Keller-Bell, Y.D.; Abbeduto, L. Narrative development in adolescents and young adults with Fragile X syndrome. Am. J. Ment. Retard. 2007, 112, 289–299. [Google Scholar] [CrossRef]
- Shiro, M.; Diez-Itza, E.; Fernández-Urquiza, M. Evaluative language and component structure of oral narratives in Williams Syndrome. In Atypical Language Development in Romance Languages; Aguilar-Mediavilla, E., Buil-Legaz, L., López-Penadés, R., Sánchez-Azanza, V.A., Adrover-Roig, D., Eds.; John Benjamins: Amsterdam, The Netherlands, 2019; pp. 235–252. [Google Scholar] [CrossRef]
- Reilly, J.; Losh, M.; Bellugi, U.; Wulfeck, B. ‘‘Frog, where are you?” Narratives in children with specific language impairment, early focal brain injury, and Williams syndrome. Brain Lang. 2004, 88, 229–247. [Google Scholar] [CrossRef]
- Van Herwegen, J.; Aznar, A.; Tenenbaum, H. The use of emotions in narratives in Williams syndrome. J. Commun. Disord. 2014, 50, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sudhalter, V.; Cohen, I.L.; Silverman, W.; Wolf-Schein, E.G. Conversational analyses of males with Fragile X, Down syndrome, and autism: Comparison of the emergence of deviant language. Am. J. Ment. Retard. 1990, 94, 431–441. [Google Scholar] [PubMed]
- Sudhalter, V.; Scarborough, H.S.; Cohen, I.L. Syntactic delay and pragmatic deviance in the language of Fragile X males. Am. J. Med. Genet. 1991, 38, 493–497. [Google Scholar] [CrossRef]
- Ferrier, L.J.; Bashir, A.S.; Meryash, D.L.; Johnston, J.; Wolff, P. Conversational skills of individuals with Fragile-X syndrome: A comparison with autism and Down syndrome. Dev. Med. Child Neurol. 1991, 33, 776–788. [Google Scholar] [CrossRef]
- Sudhalter, V.; Belser, R.C. Conversational characteristics of children with Fragile X syndrome: Tangential language. Am. J. Ment. Retard. 2001, 106, 389–400. [Google Scholar] [CrossRef]
- Roberts, J.; Martin, G.E.; Moskowitz, L.; Harris, A.A.; Foreman, J.; Nelson, L. Discourse skills of boys with Fragile X syndrome in comparison to boys with Down syndrome. J. Speech Lang. Hear. Res. 2007, 50, 475–492. [Google Scholar] [CrossRef]
- Kover, S.T.; McDuffie, A.; Abbeduto, L.; Brown, W.T. Effects of sampling context on spontaneous expressive language in males with Fragile X syndrome or Down syndrome. J. Speech Lang. Hear. Res. 2012, 55, 1022–1038. [Google Scholar] [CrossRef]
- Martin, G.E.; Roberts, J.E.; Helm-Estabrooks, N.; Sideris, J.; Vanderbilt, J.; Moskowitz, L. Perseveration in the connected speech of boys with Fragile X syndrome with and without autism spectrum disorder. Am. J. Intellect. Dev. Disabil. 2012, 117, 384–399. [Google Scholar] [CrossRef] [Green Version]
- Reilly, J.; Klima, E.; Bellugi, U. Once more with feeling: Affect and language in atypical populations. Dev. Psychopathol. 1990, 2, 367–391. [Google Scholar] [CrossRef]
- Udwin, O.; Yule, W. Expressive language of children with Williams syndrome. Am. J. Med. Genet. 1990, 37, 108–114. [Google Scholar] [CrossRef]
- Stojanovik, V.; Perkins, M.; Howard, S. Language and conversational abilities in Williams syndrome: How good is good? Int. J. Lang. Commun. Disord. 2001, 36 (Suppl. 1), 234–239. [Google Scholar] [CrossRef]
- Stojanovik, V. Social interaction deficits and conversational inadequacy in Williams syndrome. J. Neurolinguistics 2006, 19, 157–173. [Google Scholar] [CrossRef]
- Fisher, M.H.; Morin, L. Addressing social skills deficits in adults with Williams syndrome. Res. Dev. Disabil. 2017, 71, 77–87. [Google Scholar] [CrossRef]
- Kaufmann, W.E.; Capone, G.; Clarke, M.; Budimirovic, D.B. Autism in genetic intellectual disability: Insights into idiopathic autism. In Autism: Current Theories and Evidence; Zimmerman, A.W., Ed.; The Humana Press Inc.: Totowa, NJ, USA, 2008. [Google Scholar]
- Richards, C.; Jones, C.; Groves, L.; Moss, J.; Oliver, C. Prevalence of autism spectrum disorder phenomenology in genetic disorders: A systematic review and meta-analysis. Lancet Psychiatry 2015, 2, 909–916. [Google Scholar] [CrossRef] [Green Version]
- Harris, S.W.; Hessl, D.; Goodlin-Jones, B.; Ferranti, J.; Bacalman, S.; Barbato, I.; Tassone, F.; Hagerman, P.J.; Herman, H.; Hagerman, R.J. Autism profiles of males with Fragile X syndrome. Am. J. Ment. Retard. 2008, 113, 427–438. [Google Scholar] [CrossRef] [Green Version]
- Abbeduto, L.; Thurman, A.J.; McDuffie, A.; Klusek, J.; Feigles, R.T.; Brown, W.; Harvey, D.J.; Adayev, T.; LaFauci, G.; Dobkins, C.; et al. ASD Comorbidity in Fragile X syndrome: Symptom profile and predictors of symptom severity in adolescent and young adult males. J. Autism Dev. Disord. 2019, 49, 960–977. [Google Scholar] [CrossRef] [PubMed]
- Clifford, S.; Dissanayake, C.; Bui, Q.M.; Huggins, R.; Taylor, A.K.; Loesch, D.Z. Autism spectrum phenotype in males and females with Fragile X full mutation and premutation. J. Autism Dev. Disord. 2007, 37, 738–747. [Google Scholar] [CrossRef]
- Hogan, A.L.; Caravella, K.E.; Ezell, J.; Rague, L.; Hills, K.; Roberts, J.E. Autism spectrum disorder symptoms in infants with Fragile X syndrome: A prospective case series. J. Autism Dev. Disord. 2017, 47, 1628–1644. [Google Scholar] [CrossRef]
- Brock, M.; Hatton, D. Distinguishing features of autism in boys with Fragile X syndrome. J. Intellect. Disabil. Res. 2010, 54, 894–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Losh, M.; Martin, G.E.; Klusek, J.; Hogan-Brown, A.L.; Sideris, J. Social communication and theory of mind in boys with autism and Fragile x syndrome. Front. Psychol. 2012, 3, 266. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Martin, G.E.; Berry-Kravis, E.; Losh, M. A developmental, longitudinal investigation of autism phenotypic profiles in Fragile X syndrome. J. Neurodev. Disord. 2016, 8, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDuffie, A.; Thurman, A.J.; Hagerman, R.J.; Abbeduto, L. Symptoms of autism in males with Fragile X syndrome: A comparison to nonsyndromic ASD using current ADI-R scores. J. Autism Dev. Disord. 2015, 45, 1925–1937. [Google Scholar] [CrossRef] [Green Version]
- Niu, M.; Han, Y.; Dy, A.; Du, J.; Jin, H.; Qin, J.; Zhang, J.; Li, Q.; Hagerman, R.J. Autism symptoms in Fragile X syndrome. J. Child Neurol. 2017, 32, 903–909. [Google Scholar] [CrossRef]
- Klusek, J.; Martin, G.E.; Losh, M. A comparison of pragmatic language in boys with autism and Fragile X syndrome. J. Speech Lang. Hear. Res. 2014, 57, 1692–1707. [Google Scholar] [CrossRef] [PubMed]
- Abbeduto, L.; McDuffie, A.; Thurman, A.J. The Fragile X syndrome–autism comorbidity: What do we really know? Front. Genet. 2014, 5, 355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, S.S.; Lightbody, A.A.; Hirt, M.; Rezvani, A.; Reiss, A.L. Autism in Fragile X syndrome: A category mistake? J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 921–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, W.; Bellugi, U.; Lai, Z.; Chiles, M.; Reilly, J.; Lincoln, A.; Adolphs, R., II. Hypersociability in Williams syndrome. J. Cogn. Neurosci. 2000, 12 (Suppl. 1), 30–46. [Google Scholar] [CrossRef]
- Asada, K.; Itakura, S. Social phenotypes of autism spectrum disorders and Williams syndrome: Similarities and differences. Front. Psychol. 2012, 3, 247. [Google Scholar] [CrossRef] [Green Version]
- Lacroix, A.; Famelart, N.; Guidetti, M. Language and emotional abilities in children with Williams syndrome and children with autism spectrum disorder: Similarities and differences. Pediatric Health Med. Ther. 2016, 7, 89–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philofsky, A.; Fidler, D.J.; Hepburn, S. Pragmatic language profiles of school-age children with autism spectrum disorders and Williams syndrome. Am. J. Speech Lang. Pathol. 2007, 16, 368–380. [Google Scholar] [CrossRef] [Green Version]
- Tordjman, S.; Anderson, G.M.; Botbol, M.; Toutain, A.; Sarda, P.; Carlier, M.; Saugier-Veber, P.; Baumann, C.; Cohen, D.; Lagneaux, C.; et al. Autistic disorder in patients with Williams-Beuren syndrome: A reconsideration of the Williams-Beuren syndrome phenotype. PLoS ONE 2012, 7, e30778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vivanti, G.; Hamner, T.; Lee, N.R. Neurodevelopmental disorders affecting sociability: Recent research advances and future directions in autism spectrum disorder and Williams syndrome. Curr. Neurol. Neurosci. Rep. 2018, 18, 94. [Google Scholar] [CrossRef] [PubMed]
- Hamner, T.; Raitano Lee, N.; Hocking, D.R.; Vivanti, G. Shared and syndrome-specific adaptive difficulties in preschoolers with Williams syndrome and autism spectrum disorder: A cross-syndrome study. J. Intellect. Disabil. Res. 2019, 63, 1305–1311. [Google Scholar] [CrossRef]
- Lacroix, A.; Guidetti, M.; Rogé, B.; Reilly, J. Recognition of emotional and nonemotional facial expressions: A comparison between Williams syndrome and autism. Res. Dev. Disabil. 2009, 30, 976–985. [Google Scholar] [CrossRef]
- Klein-Tasman, B.P.; Phillips, K.D.; Lord, C.; Mervis, C.B.; Gallo, F.J. Overlap with the autism spectrum in young children with Williams syndrome. J. Dev. Behav. Pediatr. 2009, 30, 289–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oberman, L.M.; Kaufmann, W.E. Autism spectrum disorder versus autism spectrum disorders: Terminology, concepts, and clinical practice. Front. Psychiatry 2020, 11, 484. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, L.; Braden, M.; Coan, E.; Welnick, N.; Tanda, T.; Tartaglia, N. Evaluating Social Interactions Using the Autism Screening Instrument for Education Planning-3rd Edition (ASIEP-3): Interaction Assessment in Children and Adults with Fragile X Syndrome. Brain Sci. 2020, 10, 248. [Google Scholar] [CrossRef] [PubMed]
- Kidd, S.A.; Berry-Kravis, E.; Choo, T.H.; Chen, C.; Esler, A.; Hoffmann, A.; Andrews, H.F.; Kaufmann, W.E. Improving the diagnosis of autism spectrum disorder in Fragile X syndrome by adapting the Social Communication Questionnaire and the Social Responsiveness Scale-2. J. Autism Dev. Disord. 2020, 50, 3276–3295. [Google Scholar] [CrossRef]
- Sappok, T.; Brooks, W.; Heinrich, M.; McCarthy, J.; Underwood, L. Cross-cultural validity of the Social Communication Questionnaire for adults with intellectual developmental disorder. J. Autism Dev. Disord. 2017, 47, 393–404. [Google Scholar] [CrossRef] [PubMed]
- Adams, C. Assessment and intervention for children with pragmatic language impairment. In Social Communication Development and Disorders; Hwa-Froelich, D., Ed.; Psychology Press: Hove, UK, 2015; pp. 141–170. [Google Scholar]
- Barokova, M.; Tager-Flusberg, H. Commentary: Measuring language change through natural language samples. J. Autism Dev. Disord. 2018, 50, 2287–2306. [Google Scholar] [CrossRef]
- Abbeduto, L.; Berry-Kravis, E.; Sterling, A.; Sherman, S.; Edgin, J.O.; McDuffie, A.; Hoffmann, A.; Hamilton, D.; Nelson, M.; Aschkenasy, J.; et al. Expressive language sampling as a source of outcome measures for treatment studies in Fragile X syndrome: Feasibility, practice effects, test-retest reliability, and construct validity. J. Neurodev. Disord. 2020, 12, 10. [Google Scholar] [CrossRef] [Green Version]
- Damico, J.S. Clinical discourse analysis: A functional approach to language assessment. In Communication Skills and Classroom Success: Assessment and Therapy Methodologies for Language and Learning Disabled Students; Simon, C.S., Ed.; College-Hill Press: Hove, UK, 1985; pp. 165–204. [Google Scholar]
- Grice, P.H. Logic and Conversation. In Syntax and Semantics 3: Speech Acts; Cole, P., Morgan, J.L., Eds.; Academic Press: Cambridge, MA, USA, 1975; pp. 41–58. [Google Scholar]
- Douglas, J.M.; O’Flaherty, C.A.; Snow, P.C. Measuring perception of communicative ability: The development and evaluation of the La Trobe Communication Questionnaire. Aphasiology 2000, 14, 251–268. [Google Scholar] [CrossRef]
- Surian, L. Are children with autism deaf to Gricean maxims? Cogn. Neuropsychiatry 1996, 1, 55–72. [Google Scholar] [CrossRef]
- Okanda, M.; Asada, K.; Moriguchi, Y.; Itakura, S. Understanding violations of Gricean maxims in preschoolers and adults. Front. Psychol. 2015, 6, 901. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Urquiza, M.; Diez-Itza, E.; Cortiñas, S. PREP-CORP: Sistema de etiquetado pragmático de corpus clínicos de lengua oral. In Investigaciones Actuales en Lingüística. Vol VI; Fernández, M.C., Martí, M., Ruiz, A.M., Eds.; Universidad de Alcalá: Madrid, Spain, 2017; pp. 167–183. [Google Scholar]
- Diez-Itza, E.; Martínez, V.; Pérez, V.; Fernández-Urquiza, M. Explicit Oral Narrative Intervention for Students with Williams Syndrome. Front. Psychol. 2018, 8, 2337. [Google Scholar] [CrossRef]
- Martin, G.E.; Bush, L.; Klusek, J.; Patel, S.; Losh, M. A multimethod analysis of pragmatic skills in children and adolescents with Fragile X syndrome, autism spectrum disorder, and Down syndrome. J. Speech Lang. Hear. Res. 2018, 61, 3023–3037. [Google Scholar] [CrossRef]
- Diez-Itza, E.; Martínez, V.; Miranda, M.; Antón, A.; Ojea, A.I.; Fernández-Urquiza, M.; Pérez, V.; Fernández-Toral, J.; García, I.; Medina, B. “The Syndroling Project”: A Comparative Linguistic Analysis of Typical Development Profiles and Neurodevelopmental Genetic Syndromes (Down, Williams and Fragile X Syndromes). In Proceedings of the IASCL-XII International Congress for the Study of Child Language, Amsterdam, The Netherlands, 14–18 July 2014. [Google Scholar]
- Gallardo, B. Valoración del componente pragmático a partir de datos orales. Rev. Neurol. 2009, 48 (Suppl. 2), S57–S61. [Google Scholar] [CrossRef] [Green Version]
- Abbeduto, L.; Benson, G.; Short, K.; Dolish, J. Effects of sampling context on the expressive language of children and adolescents with mental retardation. Ment. Retard. 1995, 33, 279–288. [Google Scholar]
- MacWhinney, B. The CHILDES Project: Tools for Analyzing Talk, 3rd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2000. [Google Scholar]
- Ellis, P.D. The Essential Guide to Effect Sizes: Statistical Power, Meta-Analysis, and the Interpretation of Research Results; Cambridge University Press: Cambridge, UK, 2010. [Google Scholar] [CrossRef]
- McGrath, R.E.; Meyer, G.J. When effect sizes disagree: The case of r and d. Psychol. Methods. 2006, 11, 386–401. [Google Scholar] [CrossRef] [Green Version]
- Rossi, N.F.; Sampaio, A.; Gonçalves, O.F.; Giacheti, C.M. Analysis of speech fluency in Williams syndrome. Res. Dev. Disabil. 2011, 32, 2957–2962. [Google Scholar] [CrossRef] [Green Version]
- Crawford, H.; Moss, J.; Oliver, C.; Riby, D. Differential effects of anxiety and autism on social scene scanning in males with Fragile X syndrome. J. Neurodev. Disord. 2017, 9, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, L.; Sterling, A.; Barton-Hulsey, A. Gaze avoidance and perseverative language in Fragile X syndrome and autism spectrum disorder: Brief report. Dev. Neurorehabilit. 2018, 21, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Harrop, C.; Dallman, A.R.; Lecavalier, L.; Bodfish, J.W.; Boyd, B.A. Behavioral Inflexibility Across Two Neurogenetic Conditions: Down Syndrome and Fragile X Syndrome. Am. J. Intellect. Dev. Disabil. 2021, 126, 409–420. [Google Scholar] [CrossRef] [PubMed]
- Grant, C.M.; Apperly, I.; Oliver, C. Is theory of mind understanding impaired in males with Fragile X syndrome? J. Abnorm. Child Psychol. 2007, 35, 17–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lacroix, A.; Aguert, M.; Dardier, V.; Stojanovik, V.; Laval, V. Idiom comprehension in French-speaking children and adolescents with Williams’ syndrome. Res. Dev. Disabil. 2010, 31, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Vulchanova, M.; Saldaña, D.; Chahboun, S.; Vulchanov, V. Figurative language processing in atypical populations: The ASD perspective. Front. Hum. Neurosci. 2015, 9, 24. [Google Scholar] [CrossRef] [PubMed]
- Van Den Heuvel, E.; Manders, E.; Swillen, A.; Zink, I. Developmental trajectories of structural and pragmatic language skills in school-aged children with Williams syndrome. J. Intellect. Disabil. Res. 2016, 60, 903–919. [Google Scholar] [CrossRef]
- John, A.E.; Rowe, M.L.; Mervis, C.B. Referential communication skills of children with Williams syndrome: Understanding when messages are not adequate. Am. J. Intellect. Dev. Disabil. 2009, 114, 85–99. [Google Scholar] [CrossRef] [Green Version]
- Chromik, L.C.; Quintin, E.M.; Lepage, J.F.; Hustyi, K.M.; Lightbody, A.A.; Reiss, A.L. The influence of hyperactivity, impulsivity, and attention problems on social functioning in adolescents and young adults with Fragile X syndrome. J. Atten. Disord. 2019, 23, 181–188. [Google Scholar] [CrossRef]
- Crawford, H.; Moss, J.; Stinton, C.; Singla, G.; Oliver, C. Overactivity, impulsivity and repetitive behaviour in males with Fragile X syndrome: Contrasting developmental trajectories in those with and without elevated autism symptoms. J. Intellect. Disabil. Res. 2018, 62, 672–683. [Google Scholar] [CrossRef]
- Parks, K.; Cardy, J.; Woynaroski, T.G.; Sehl, C.G.; Stevenson, R.A. Investigating the Role of Inattention and/or Hyperactivity/impulsivity in Language and Social Functioning Using a Dimensional Approach. J. Commun. Disord. 2021, 89, 106036. [Google Scholar] [CrossRef]
- Roberts, J.E.; Mirrett, P.; Anderson, K.; Burchinal, M.; Neebe, E. Early communication, symbolic behavior, and social profiles of young males with Fragile X syndrome. Am. J. Speech Lang. Pathol. 2002, 11, 295–304. [Google Scholar] [CrossRef]
- Abbeduto, L.; Murphy, M.M.; Cawthon, S.W.; Richmond, E.K.; Weissman, M.D.; Karadottir, S.; O’Brien, A. Receptive language skills of adolescents and young adults with Down or Fragile X syndrome. Am. J. Ment. Retard. 2003, 108, 149–160. [Google Scholar] [CrossRef] [Green Version]
- Price, J.; Roberts, J.; Vandergrift, N.; Martin, G. Language comprehension in boys with Fragile X syndrome and boys with Down syndrome. J. Intellect. Disabil. Res. 2007, 51, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Martin, G.E.; Barstein, J.; Hornickel, J.; Matherly, S.; Durante, G.; Losh, M. Signaling of noncomprehension in communication breakdowns in Fragile X syndrome, Down syndrome, and autism spectrum disorder. J. Commun. Disord. 2017, 65, 22–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul, R.; Dykens, E.; Leckman, J.F.; Watson, M.; Breg, W.R.; Cohen, D.J. A comparison of language characteristics of mentally retarded adults with Fragile X syndrome and those with nonspecific mental retardation and autism. J. Autism Dev. Disord. 1987, 17, 457–468. [Google Scholar] [CrossRef] [PubMed]
- Pruccoli, J.; Spadoni, C.; Orsenigo, A.; Parmeggiani, A. Should Echolalia Be Considered a Phonic Stereotypy? A Narrative Review. Brain Sci. 2021, 11, 862. [Google Scholar] [CrossRef]
- Nelson, S.; McDuffie, A.; Banasik, A.; Tempero Feigles, R.; Thurman, A.J.; Abbeduto, L. Inferential language use by school-aged boys with Fragile X syndrome: Effects of a parent-implemented spoken language intervention. J. Commun. Disord. 2018, 72, 64–76. [Google Scholar] [CrossRef]
- Abbeduto, L.; Klusek, J.; Taylor, J.L.; Abdelnur, N.; Sparapani, N.; Thurman, A.J. Concurrent Associations between Expressive Language Ability and Independence in Adolescents and Adults with Fragile X Syndrome. Brain Sci. 2021, 11, 1179. [Google Scholar] [CrossRef]
- Alfieri, P.; Scibelli, F.; Casula, L.; Piga, S.; Napoli, E.; Valeri, G.; Vicari, S. Cooperative Parent-Mediated Therapy in Children with Fragile X Syndrome and Williams Beuren Syndrome: A Pilot RCT Study of a Transdiagnostic Intervention-Preliminary Data. Brain Sci. 2022, 12, 8. [Google Scholar] [CrossRef]
- Valeri, G.; Casula, L.; Menghini, D.; Amendola, F.A.; Napoli, E.; Pasqualetti, P.; Vicari, S. Cooperative parent-mediated therapy for Italian preschool children with autism spectrum disorder: A randomized controlled trial. Eur. Child Adolesc. Psychiatry 2020, 29, 935–946. [Google Scholar] [CrossRef] [PubMed]
- Stojanovik, V.; Perkins, M.; Howard, S. Linguistic heterogeneity in Williams syndrome. Clin. Linguist. Phon. 2006, 20, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, R.C.; Schmitt, L.; Thurman, A.; Abbeduto, L.; Hong, M.; Pedapati, E.; Dominick, K.; Sweeney, J.; Erickson, C. The relationship between expressive language sampling and clinical measures in Fragile X syndrome and typical development. Brain Sci. 2020, 10, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| FXS-G Mean (SD) | WS-G Mean (SD) | t | p | d | r | |
|---|---|---|---|---|---|---|
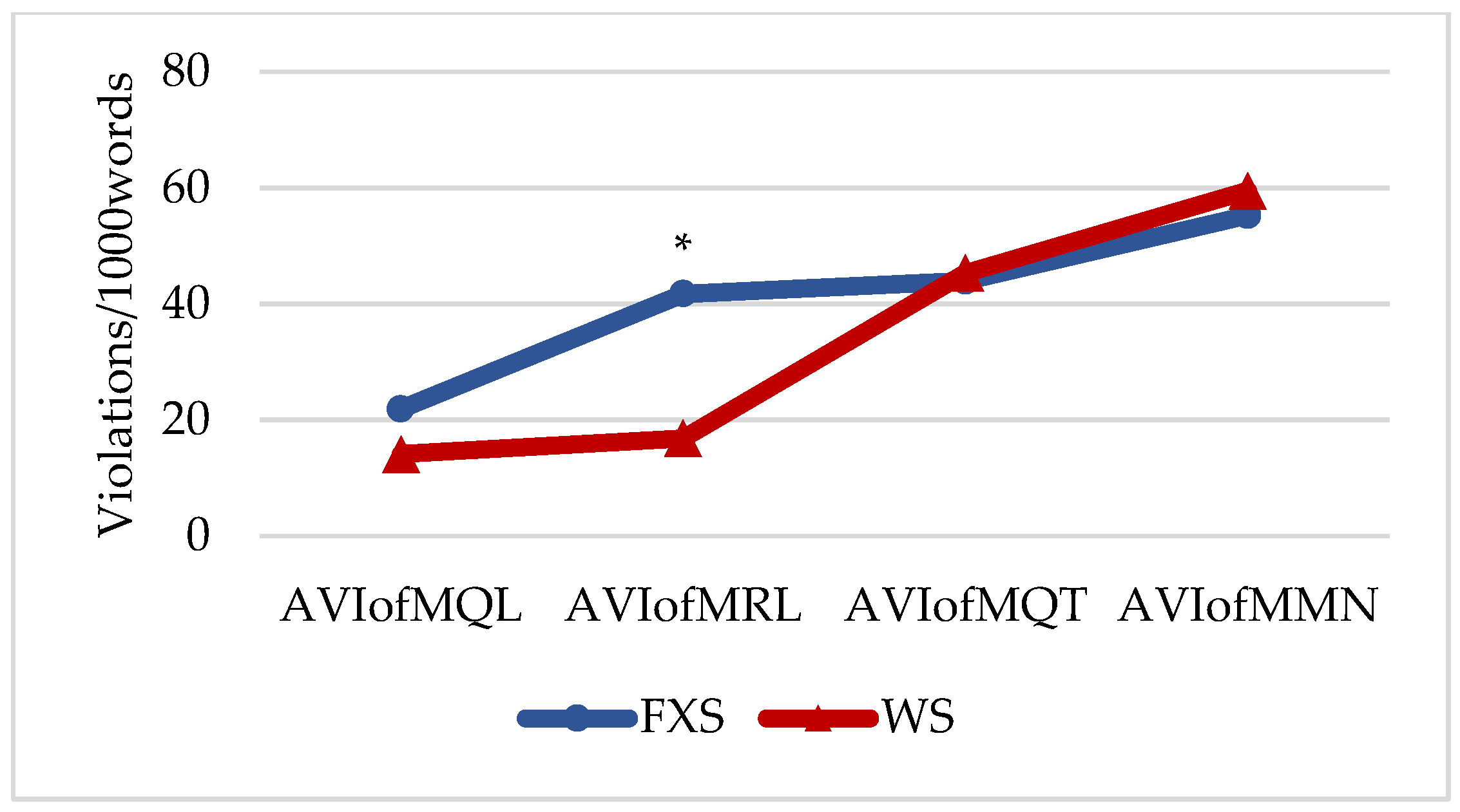
| AVIofMQL | 21.91 (15.52) | 14.16 (6.3) | 1.132 | 0.297 | 0.6543 | 0.3109 |
| AVIofMRL VI_NRL VI_TNG VI_PER_T | 41.75 (20.18) 3.61 (3.73) 15.68 (8.95) 22.46 (11.73) | 16.83 (4.30) 0.66 (0.81) 9.16 (3.19) 7.00 (4.14) | 2.958 1.885 1.678 3.045 | 0.028 * 0.113 0.142 0.022 * | 1.7080 1.0930 0.9768 1.7576 | 0.6494 0.4795 0.4388 0.6601 |
| AVIofMQT VI_RUT VI_VUT VI_EVP VI_RVP | 43.94 (22.25) 8.52 (4.17) 18.53 (12.8) 0.21 (0.33) 16.67 (16.23) | 45.33 (15.92) 6.83 (2.64) 16.66 (5.68) 2.33 (4.80) 19.50 (16.30) | 0.124 0.840 0.327 −1.079 0.301 | 0.904 0.420 0.754 0.306 0.770 | −0.0718 0.6324 0.2175 −0.6231 −0.1875 | −0.0359 0.3015 0.1081 −0.2974 −0.0933 |
| AVIofMMN VI_REP VI_REF VI_PER_F VI_ORD | 55.28 (20.07) 24.84 (12.60) 8.76 (6.79) 14.08 (8.00) 7.59 (4.08) | 59.50 (21.82) 28.0 (18.77) 17.5 (3.93) 4.66 (2.25) 9.33 (4.41) | 0.348 −0.342 −2.725 2.773 −0.707 | 0.735 0.739 0.021 * 0.020 * 0.496 | −0.1950 −0.2614 −1.8973 1.7149 −0.5000 | −0.0970 −0.1296 −0.6882 0.6509 −0.2425 |
| AVIofCOOP | 162.88 (43.92) | 135.16 (24.49) | −1.350 | 0.207 | 0.7753 | 0.3614 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diez-Itza, E.; Viejo, A.; Fernández-Urquiza, M. Pragmatic Profiles of Adults with Fragile X Syndrome and Williams Syndrome. Brain Sci. 2022, 12, 385. https://doi.org/10.3390/brainsci12030385
Diez-Itza E, Viejo A, Fernández-Urquiza M. Pragmatic Profiles of Adults with Fragile X Syndrome and Williams Syndrome. Brain Sciences. 2022; 12(3):385. https://doi.org/10.3390/brainsci12030385
Chicago/Turabian StyleDiez-Itza, Eliseo, Aitana Viejo, and Maite Fernández-Urquiza. 2022. "Pragmatic Profiles of Adults with Fragile X Syndrome and Williams Syndrome" Brain Sciences 12, no. 3: 385. https://doi.org/10.3390/brainsci12030385