Estimation of Work of Breathing from Respiratory Muscle Activity In Spontaneous Ventilation: A Pilot Study



Abstract
:1. Introduction
2. Materials and Methods
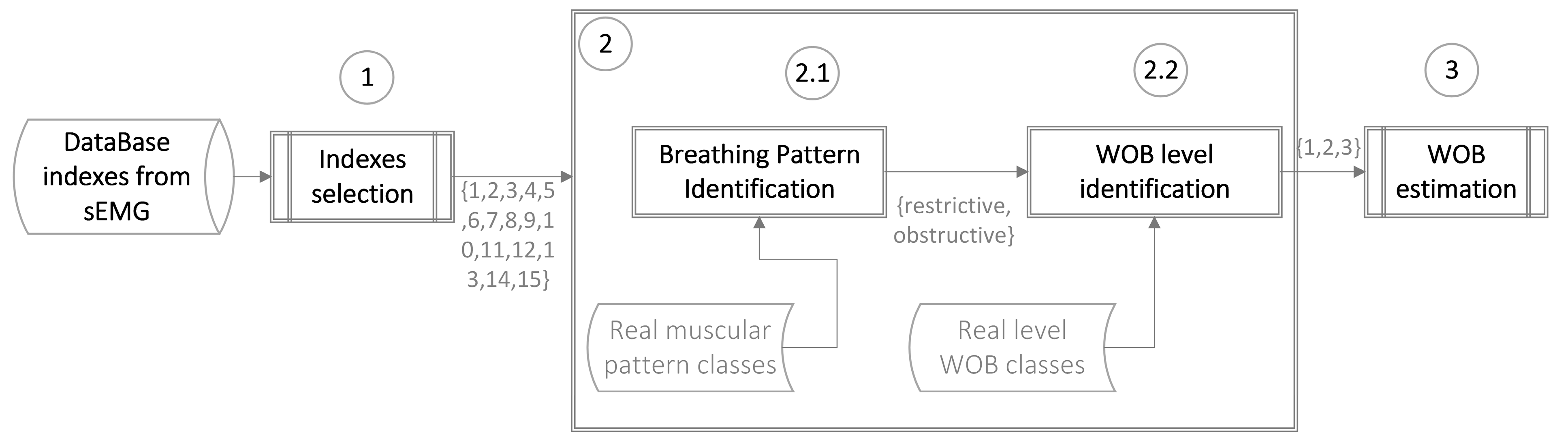
2.1. Experimental Design
2.2. Subjects
2.3. Measurements and Signal Acquisition
2.3.1. Respiratory and Surface Electromyography Signals
2.3.2. Respiratory Mechanics
2.4. Data Analysis
2.4.1. Indexes from Surface Electromyography of Respiratory Muscles
Time Domain Indexes
Frequency Domain Indexes
2.4.2. Work of Breathing Estimation
- Calculus of correlation coefficients of n-indexes with the response variable Y.
- Sort the n-indexes from highest to lowest correlation coefficient X = [x1, x2…..xn].
- Add index xi to the P vector.
- Calculus of regression and partial Fj-values between response variable Y and P, where j is the index in the P vector.
- Selection of the lowest Fj-value and comparison between this and the F-value at α = 0.05 in the F-distribution.
- If the Fj-value is higher than the F-value at α = 0.05, i is incremented by one, the index Pj is removed from the P vector.
- Steps 3–6 are repeated until the last index enters the P vector.
- Accuracy: number of samples correctly classified/number of total samples
- Specificity: number correctly classified as normal WOB/number of total normal WOB.
- Sensitivity (Group 2 only): number correctly classified as medium WOB/number of total medium WOB.
- Sensitivity (Group 3 only): number correctly classified as elevated WOB/number of total elevated WOB.
- Sensitivity (Group 2 and Group 3): number correctly classified as high WOB/number of total high WOB.
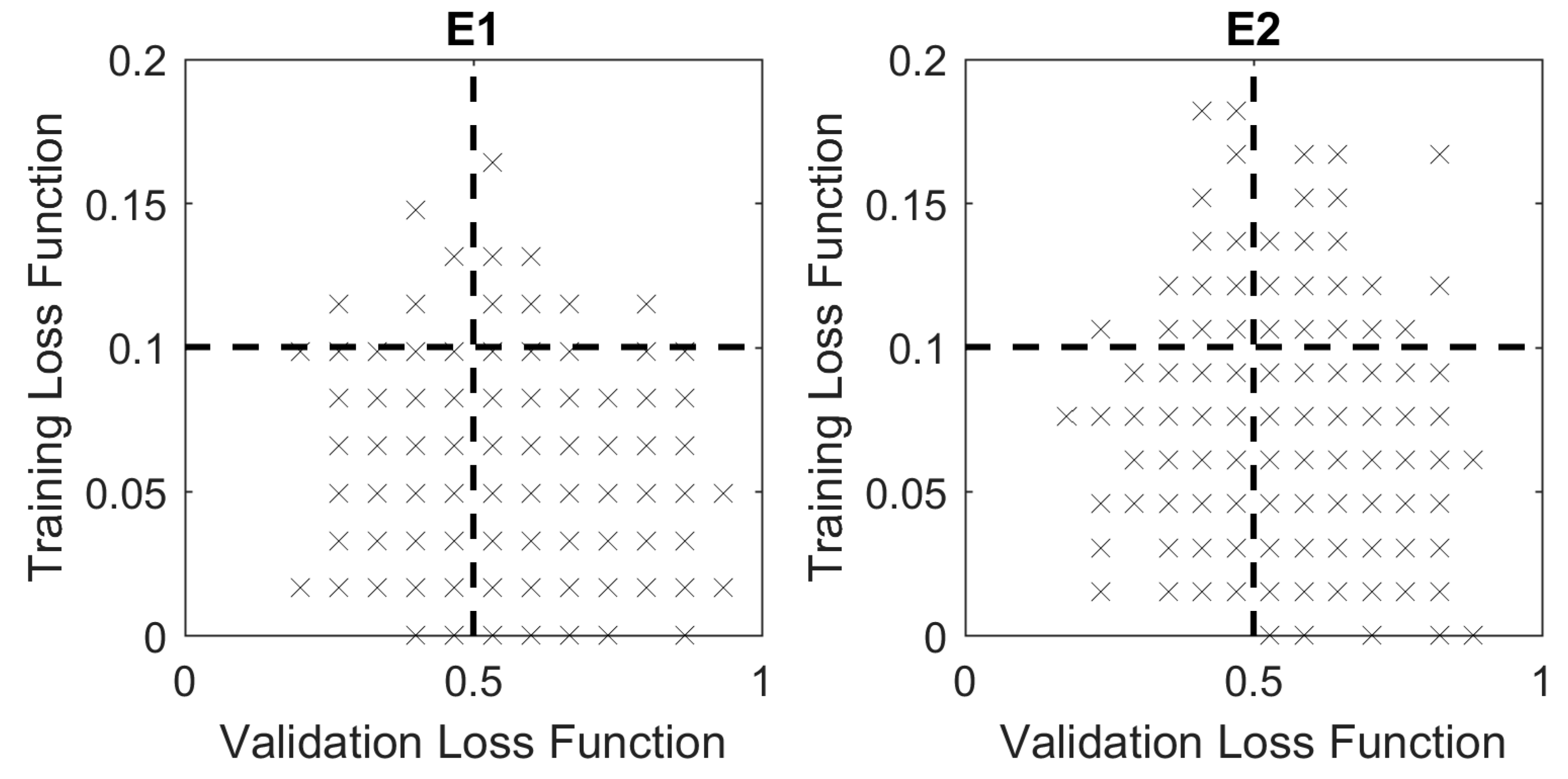
Optimization of Model Parameters
2.5. Statistical Analysis
3. Results
3.1. Ventilatory Pattern Classification
3.2. WOB Level Classification
3.3. WOB Estimation
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Grinnan, D.C.; Truwit, J.D. Clinical review: Respiratory mechanics in spontaneous and assisted ventilation. Crit. Care 2005, 9, 472–484. [Google Scholar] [CrossRef] [Green Version]
- Brochard, L.; Martin, G.S.; Blanch, L.; Pelosi, P.; Belda, F.J.; Jubran, A.; Gattinoni, L.; Mancebo, J.; Ranieri, V.M.; Richard, J.C.M.; et al. Clinical review: Respiratory monitoring in the ICU—A consensus of 16. Crit. Care 2012, 16, 219. [Google Scholar] [CrossRef] [PubMed]
- Tulaimat, A.; Patel, A.; Wisniewski, M.; Gueret, R. The validity and reliability of the clinical assessment of increased work of breathing in acutely ill patients. J. Crit. Care 2016, 34, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Aboussouan, L. Respiratory Failure and the Need for Ventilatory Support. In Egan’s Fundamentals of Respiratory Care, 11th ed.; Kacmarek, R., Stoller, J., Heuer, A., Eds.; Elsevier: St. Louis, MO, USA, 2017; pp. 971–986. [Google Scholar]
- Piraino, T. Monitoring the Patient in the Intensive Care Unit. In Egan’s Fundamentals of Respiratory Care, 11th ed.; Kacmarek, R., Stoller, J., Heuer, A., Eds.; Elsevier: St. Louis, MO, USA, 2017; pp. 1154–1189. [Google Scholar]
- Sharp, J.T.; Henry, J.P.; Sweany, S.K.; Meadows, W.R.; Pietras, R.J. The Total Work of Breathing in Normal and Obese Men. J. Clin. Investig. 1964, 43, 728–739. [Google Scholar] [CrossRef]
- Diehl, J.L.; Mercat, A.; Guérot, E.; Aïssa, F.; Teboul, J.L.; Richard, C.; Labrousse, J. Helium/oxygen mixture reduces the work of breathing at the end of the weaning process in patients with severe chronic obstructive pulmonary disease. Crit. Care Med. 2003, 31, 1415–1420. [Google Scholar] [CrossRef]
- Kirton, O.C.; DeHaven, C.B.; Morgan, J.P.; Windsor, J.; Civetta, J.M. Elevated imposed work of breathing masquerading as ventilator weaning intolerance. Chest 1995, 108, 1021–1025. [Google Scholar] [CrossRef] [PubMed]
- Umbrello, M.; Formenti, P.; Longhi, D.; Galimberti, A.; Piva, I.; Pezzi, A.; Mistraletti, G.; Marini, J.J.; Iapichino, G. Diaphragm ultrasound as indicator of respiratory effort in critically ill patients undergoing assisted mechanical ventilation: A pilot clinical study. Crit. Care 2015, 19, 161. [Google Scholar] [CrossRef]
- Khirani, S.; Polese, G.; Aliverti, A.; Appendini, L.; Nucci, G.; Pedotti, A.; Colledan, M.; Lucianetti, A.; Baconnier, P.; Rossi, A. On-line monitoring of lung mechanics during spontaneous breathing: A physiological study. Respir. Med. 2010, 104, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Banner, M.J.; Tams, C.G.; Euliano, N.R.; Stephan, P.J.; Leavitt, T.J.; Martin, A.D.; Al-Rawas, N.; Gabrielli, A. Real time noninvasive estimation of work of breathing using facemask leak-corrected tidal volume during noninvasive pressure support: Validation study. J. Clin. Monit. Comput. 2016, 30, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Chiti, L.; Hug, F.; Demoule, A.; Similowski, T. Surface electromyogram of inspiratory muscles: A possible routine monitoring tool in the intensive care unit. Br. J. Anaesth. 2011, 106, 913–914. [Google Scholar] [CrossRef]
- Schmidt, M.; Banzett, R.B.; Raux, M.; Morélot-Panzini, C.; Dangers, L.; Similowski, T.; Demoule, A. Unrecognized suffering in the ICU: Addressing dyspnea in mechanically ventilated patients. Intensive Care Med. 2014, 40, 1–10. [Google Scholar] [CrossRef]
- Schmidt, M.; Kindler, F.; Gottfried, S.B.; Raux, M.; Hug, F.; Similowski, T.; Demoule, A. Dyspnea and surface inspiratory electromyograms in mechanically ventilated patients. Intensive Care Med. 2013, 39, 1368–1376. [Google Scholar] [CrossRef]
- Salazar, M.B.; Hernandez, A.M.; Mananas, M.A. Assessment of mechanically ventilated patients intoxicated with organophosphates by a novel surface electromyographic index. J. Crit. Care 2017, 41, 260–267. [Google Scholar] [CrossRef]
- Salazar, M.B.; Hernandez, A.M.; Mananas, M.A.; Zuluaga, A.F. Potential clinical application of surface electromyography as indicator of neuromuscular recovery during weaning tests after organophosphate poisoning. Rev. Bras. Ter. Intensiv. 2017, 29, 253–258. [Google Scholar] [Green Version]
- Munoz, I.C.; Hernandez, A.M.; Alonso, J.F.; Mananas, M.Á.; Atehortúa, L.H. Assessment of weaning indexes based on diaphragm activity in mechanically ventilated subjects after cardiovascular surgery. A pilot study. Rev. Bras. Ter. Intensiv. 2017, 29, 213–221. [Google Scholar] [Green Version]
- Chowdhury, R.; Reaz, M.; Ali, M.; Bakar, A.; Chellappan, K.; Chang, T. Surface Electromyography Signal Processing and Classification Techniques. Sensors 2013, 13, 12431–12466. [Google Scholar] [CrossRef] [Green Version]
- Perchiazzi, G.; Rylander, C.; Pellegrini, M.; Larsson, A. Monitoring of total positive end-expiratory pressure during mechanical ventilation by artificial neural networks. J. Clin. Monit. Comput. 2017, 31, 551–559. [Google Scholar] [CrossRef]
- Banner, M.J.; Euliano, N.R.; Brennan, V.; Peters, C.; Layon, A.J.; Gabrielli, A. Power of breathing determined noninvasively with use of an artificial neural network in patients with respiratory failure. Crit. Care Med. 2006, 34, 1052–1059. [Google Scholar] [CrossRef]
- Hernández, A.M.; Salazar, M.B.; Muñoz, I.C. Efecto del incremento del PEEP en la actividad muscular respiratoria en sujetos sanos bajo ventilación espontánea. IATREIA 2016, 29, 280–291. [Google Scholar]
- Muñoz, I.C.; Urrego, D.A.; Vallejo, A.F.; Hernández, A.M. Device for simulation of restrictive pathologies in healthy subjects with non-invasive mechanical ventilation. Rev. Fac. Ing. Univ. Antioq. 2018, 1, 19–26. [Google Scholar] [CrossRef]
- Stănescu, D.C.; Nemery, B.; Veriter, C.; Maréchal, C. Pattern of breathing and ventilatory response to CO2 in subjects practicing hatha-yoga. J. Appl. Physiol. 1981, 51, 1625–1629. [Google Scholar] [CrossRef]
- Chakraborti, S.; Gibbons, J.D. Nonparametric Statistical Inference, 4th ed.; Marcel Dekker, Inc.: New York, NY, USA, 2003. [Google Scholar]
- Hernández, A.M. Sistema de Control. Respiratorio Ante Estímulos y Patologías. Análisis, Modelado y Simulación, 1st ed.; Publicia: Saarbrücken, Germany, 2007. [Google Scholar]
- Alonso, J.F.; Mañanas, M.A.; Rojas, M.; Bruce, E.N. Coordination of respiratory muscles assessed by means of nonlinear forecasting of demodulated myographic signals. J. Electromyogr. Kinesiol. 2011, 21, 1064–1073. [Google Scholar] [CrossRef] [Green Version]
- Chien, M.Y.; Wu, Y.T.; Chang, Y.J. Assessment of diaphragm and external intercostals fatigue from surface EMG using cervical magnetic stimulation. Sensors 2008, 8, 2174–2187. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, I.C.; Hernández, A.M. Noninvasive approach to estimate ventilatory mechanics in spontaneous breathing with different PEEP and pressure support values: Validation with mechanical simulation. In Proceedings of the VII Latin American Congress on Biomedical Engineering CLAIB 2016, Bucaramanga, Santander, Colombia, 26–28 October 2016; pp. 241–244. [Google Scholar]
- Munoz, I.C.; Hernández, A.M. Cambios en la mecánica ventilatoria debidos a variaciones de la PEEP y la presión soporte: Estudio en sujetos sanos bajo ventilación mecánica no invasiva. Rev. Fac. Med. 2017, 65, 321–328. [Google Scholar] [CrossRef]
- Becher, T.; Schädler, D.; Rostalski, P.; Zick, G. Determination of respiratory system compliance during pressure support ventilation by small variations of pressure support. J. Clin. Monit. Comput. 2018, 32, 741–751. [Google Scholar] [CrossRef]
- De Luca, C.J.; Donald, G.L.; Kuznetsov, M.; Roy, S.H. Filtering the surface EMG signal: Movement artifact and baseline noise contamination. J. Biomech. 2010, 43, 1573–1579. [Google Scholar] [CrossRef]
- Merletti, R.; Parker, P.A. Electromyography: Physiology, Engineering, and Non-Invasive Applications; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2004. [Google Scholar]
- Haykin, S.S. Adaptive Filter Theory, 5th ed.; Pearson Education: Upper Saddle River, NJ, USA, 2014. [Google Scholar]
- Camacho, A.; Hernandez, A.M.; Londono, Z.; Serna, L.Y.; Mananas, M.A. A synchronization system for the analysis of biomedical signals recorded with different devices from mechanically ventilated patients. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), San Diego, CA, USA, 28 August–1 September 2012; pp. 1944–1947. [Google Scholar]
- Draper, N.R.; Smith, H. Selecting the “Best” Regression Equation. In Applied Regression Analysis, 3rd ed.; Draper, N.R., Smith, H., Eds.; John Wiley & Sons, Inc.: New York, NY, USA, 1998; pp. 335–336. [Google Scholar]
- Tourassi, G.D.; Frederick, E.D.; Markey, M.K.; Floyd, C.E. Application of the mutual information criterion for feature selection in computer-aided diagnosis. Med. Phys. 2001, 28, 2394–2402. [Google Scholar] [CrossRef]
- Hwang, W. Data Mining in Ergonomics. In International Encyclopedia of Ergonomics and Human Factors, 2nd ed.; Karwowski, W., Ed.; Taylor & Francis Group: Louisville, KY, USA, 2006; pp. 3077–3081. [Google Scholar]
- Polikar, R. Ensemble based systems in decision making. IEEE Circuits Syst. Mag. 2006, 6, 21–45. [Google Scholar] [CrossRef]
- Subasi, A.; Yilmaz, M.; Ozcalik, H.R. Classification of EMG signals using wavelet neural network. J. Neurosci. Methods 2006, 156, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Guler, H.; Kilic, U. The development of a novel knowledge-based weaning algorithm using pulmonary parameters: A simulation study. Med. Biol. Eng. Comput. 2017, 56, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Vicario, F.; Albanese, A.; Wang, D.; Karamolegkos, N.; Chbat, N.W. Constrained optimization for noninvasive estimation of work of breathing. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milano, Italy, 25–29 August 2015; pp. 5327–5330. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Index | Time Domain | Index | Frequency Domain |
|---|---|---|---|
| MaxAmpj | Maximum amplitude of the sEMG signal of muscle j: Dia, Int or Strn | Fcj | The central frequency of power spectral density of sEMG signal of muscle j |
| Rj-k | Pearson correlation between pairs of amplitudes of sEMG signals of the muscles j and k | RHLj | The ratio between high and low frequencies of power spectral density of sEMG signal of muscle j |
| Cj-k | Spectral coherence between pairs of sEMG signals of the muscles j and k |
| Respiratory Muscular Pattern | |||
|---|---|---|---|
| Classifier Algorithm | Configuration | Validation | |
| LDA | Gamma = 0 Delta = 0 Discriminant type: linear Indexes: logarithmic transformed | K-fold 20% | |
| SVM | Box Constraint = 962.47 Kernel Scale = 8.4 Kernel Function: Gaussian Indexes: Standardized | K-fold 20% | |
| KNN | Distance: Euclidean Number of Neighbors: 2 Indexes: Standardized | K-fold 20% | |
| WOB LEVEL | |||
| Classifier Algorithm | Experiment 1 | Experiment 2 | Validation |
| Configuration | Configuration | ||
| LDA | Gamma = 0.49 Delta = 0.06 Discriminant type: linear Indexes: logarithmic transformed | K-fold 20% | |
| SVM | Box Constraint = 1 Kernel Scale = 1 Kernel Function: Gaussian Indexes: Standardized | Box Constraint = 0.7416 Kernel Scale = 110.77 Kernel Function: Gaussian Indexes: Standardized | K-fold 20% |
| KNN | Distance: Euclidean Number of Neighbors: 2 Indexes: Standardized | K-fold 20% | |
| META-CLASSIFIER KNN | Distance: Euclidean Number of Neighbors: 2 Indexes: Standardized | K-fold 20% | |
| NN | Training function: Levenberg-Marquardt hidden layer: 1 hidden layer sizes: 10 input layer sizes: 4 output layer sizes: 3 Indexes: Standardized | K-fold 20% | |
| Index | Experiment | P-Value | |
|---|---|---|---|
| Restrictive (E1) | Obstructive (E2) | ||
| CDia-Int | 0.67 [0.64–0.73] | 0.75 [0.72–0.80] | <0.01 |
| CDia-Strn | 0.72 [0.70–0.76] | 0.65 [0.62–0.70] | <0.01 |
| FCStrn (Hz) | 77.84 [68.24–86.71] | 62.37 [58.46–67.88] | <0.01 |
| RHLStrn | 169.76 [107.71–229.17] | 92.07 [55.00–131.52] | <0.01 |
| Parameter/Index | Restrictive (E1) | P-Value | ||||
|---|---|---|---|---|---|---|
| G1 | G2 | G3 | G1- G2 | G1- G3 | G2- G3 | |
| WOBr (J/L) | 0.61 ± 0.13 | 1.02 ± 0.14 | 1.52 ± 0.13 | <0.05 | <0.05 | <0.05 |
| MaxAmpDia (mV) | 0.024 [0.022–0.030] | 0.032 [0.022–0.049] | 0.054 [0.040–0.068] | * | <0.05 | <0.05 |
| MaxAmpInt (mV) | 0.020 [0.016–0.027] | 0.032 [0.020–0.043] | 0.034 [0.020–0.049] | <0.05 | <0.05 | * |
| MaxAmpStrn (mV) | 0.018 [0.010–0.024] | 0.021 [0.014–0.036] | 0.021 [0.017–0.041] | * | * | * |
| CDia-Int | 0.66 [0.62–0.68] | 0.67 [0.65–0.75] | 0.71 [0.67–0.83] | * | <0.05 | * |
| α1 | 0.55 ± 10-5 | 1.07 ± 0.04 | 1.55 ± 10–5 | - | - | - |
| α2 | 0.45 ± 10-5 | 0.93 ± 0.04 | 1.45 ± 10–5 | - | - | - |
| Obstructive (E2) | ||||||
| WOBr (J/L) | 0.63 ± 0.12 | 1.03 ± 0.14 | 1.51 ± 0.12 | <0.05 | <0.05 | <0.05 |
| MaxAmpDia (mV) | 0.028 [0.021–0.038] | 0.031 [0.023–0.047] | 0.050 [0.038–0.083] | * | <0.05 | <0.05 |
| MaxAmpInt (mV) | 0.016 [0.010–0.029] | 0.019 [0.013–0.036] | 0.023 [0.015–0.045] | * | * | * |
| MaxAmpStrn (mV) | 0.016 [0.010–0.023] | 0.017 [0.013–0.022] | 0.030 [0.019–0.048] | * | <0.05 | <0.05 |
| CDia-Int | 0.79 [0.75–0.84] | 0.75 [0.72–0.78] | 0.73 [0.69–0.75] | <0.05 | <0.05 | * |
| α1 | 0.55 ± 10–5 | 1.05 ± 10–5 | 1.55 ± 10–5 | - | - | - |
| α2 | 0.45 ± 10–5 | 0.95 ± 10–5 | 1.45 ± 10–5 | - | - | - |
| Algorithm | Accuracy (%) | Specificity (%) | Sensitivity (%) (Group 2) | Sensitivity (%) (Group 3) | ||||
|---|---|---|---|---|---|---|---|---|
| E1 | E2 | E1 | E2 | E1 | E2 | E1 | E2 | |
| LDA | 56.58 | 55.42 | 57.69 | 17.39 | 63.89 | 75.56 | 35.71 | 53.33 |
| SVM | 47.37 | 56.63 | 0 | 0 | 100 | 100 | 0 | 0 |
| KNN | 39.47 | 54.22 | 34.62 | 52.17 | 41.67 | 64.44 | 42.86 | 26.67 |
| STACKING (LDA-SVM-KNN) | 35.53 | 46.99 | 53.85 | 17.39 | 25.00 | 77.78 | 21.43 | 0 |
| STACKING (LDA-KNN-KNN) | 40.79 | 48.19 | 42.31 | 17.39 | 44.44 | 75.56 | 28.57 | 13.33 |
| STACKING (SVM-KNN-KNN) | 47.37 | 37.35 | 42.31 | 65.22 | 66.67 | 24.44 | 7.14 | 33.33 |
| STACKING (LDA-SVM-KNN-KNN) | 50.00 | 43.37 | 34.62 | 34.78 | 66.67 | 62.22 | 35.71 | 0 |
| NN | 80.00 [93.42] | 82.35 [91.57] | 92.31 | 82.61 | 91.67 | 100 | 100 | 80 |
| Real Values | |||||
|---|---|---|---|---|---|
| Group 1 | Group 2 | Group 3 | Total | ||
| Predicted Values | Group 1 | 41 | 4 | 0 | 45 |
| Group 2 | 5 | 73 | 3 | 81 | |
| Group 3 | 3 | 4 | 26 | 33 | |
| Total | 49 | 81 | 29 | 159 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz, I.C.; Hernández, A.M.; Mañanas, M.Á. Estimation of Work of Breathing from Respiratory Muscle Activity In Spontaneous Ventilation: A Pilot Study. Appl. Sci. 2019, 9, 2007. https://doi.org/10.3390/app9102007
Muñoz IC, Hernández AM, Mañanas MÁ. Estimation of Work of Breathing from Respiratory Muscle Activity In Spontaneous Ventilation: A Pilot Study. Applied Sciences. 2019; 9(10):2007. https://doi.org/10.3390/app9102007
Chicago/Turabian StyleMuñoz, Isabel Cristina, Alher Mauricio Hernández, and Miguel Ángel Mañanas. 2019. "Estimation of Work of Breathing from Respiratory Muscle Activity In Spontaneous Ventilation: A Pilot Study" Applied Sciences 9, no. 10: 2007. https://doi.org/10.3390/app9102007