Tonic Cold Pain Detection Using Choi–Williams Time-Frequency Distribution Analysis of EEG Signals: A Feasibility Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
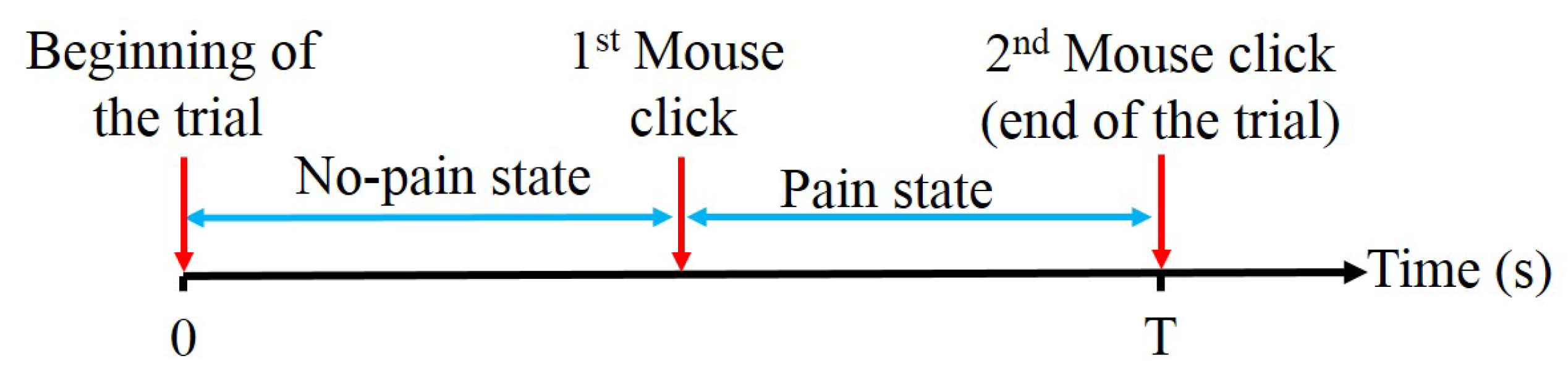
2.2. Experimental Protocol
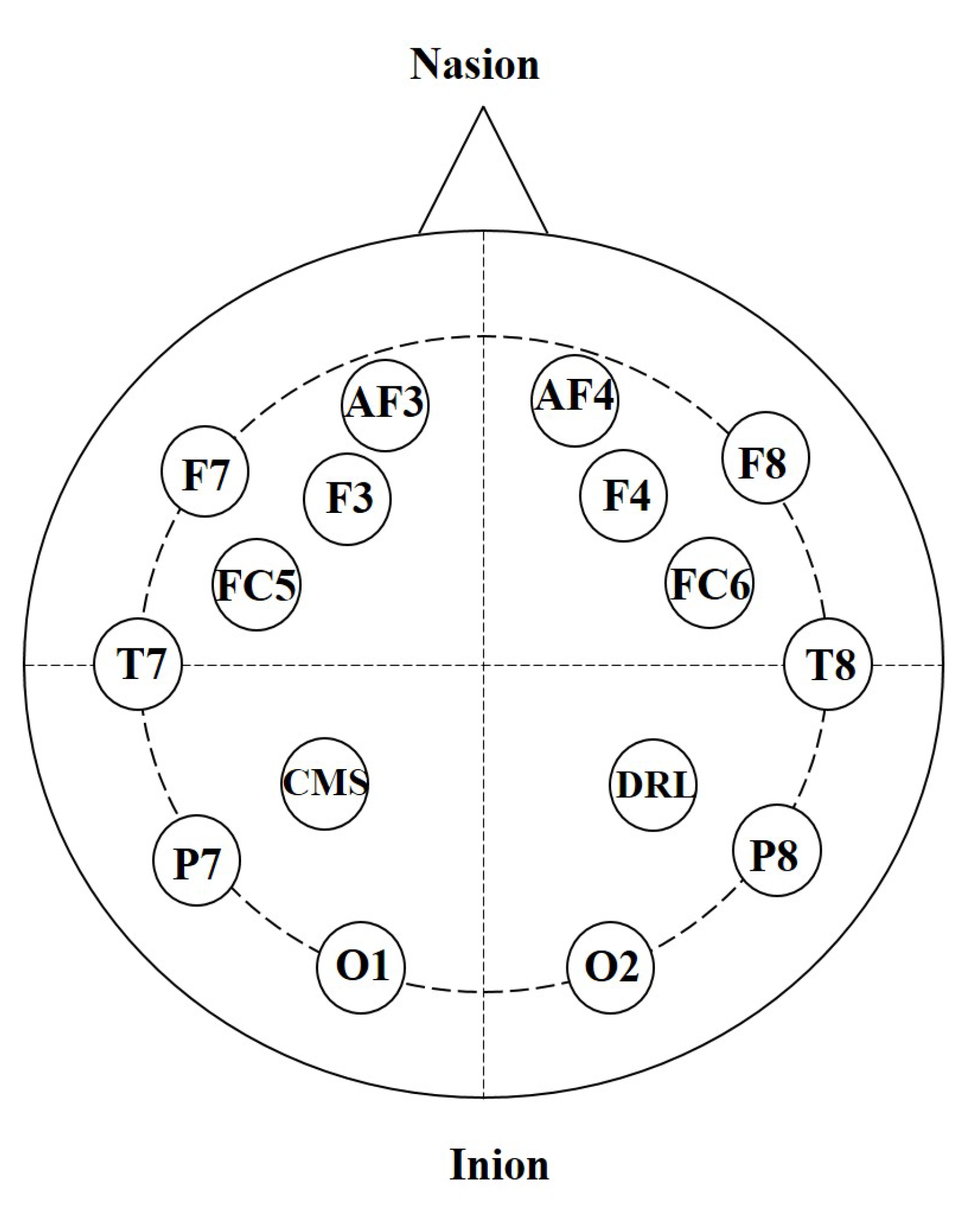
2.3. Data Acquisition and Preprocessing
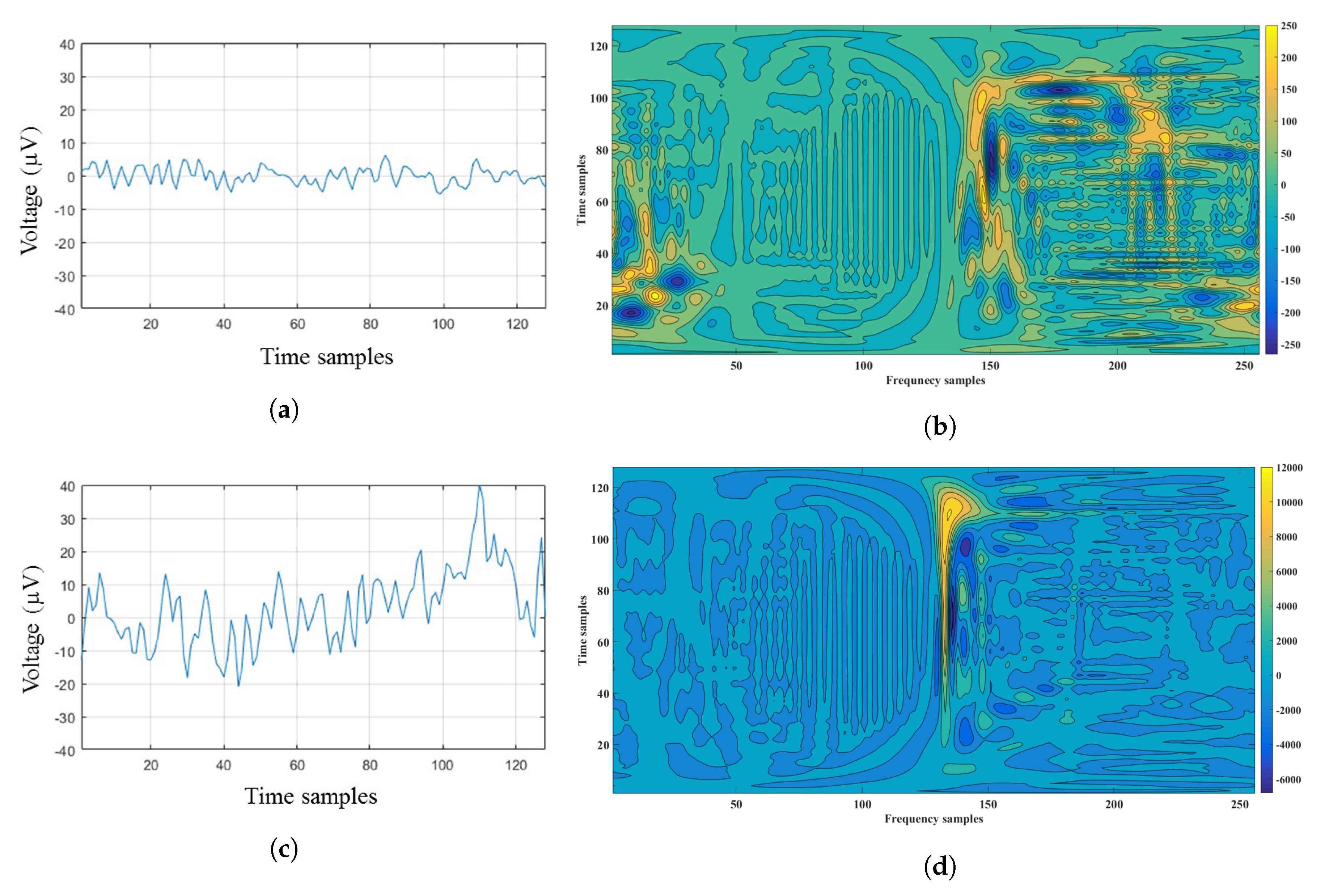
2.4. Time-Frequency Analysis of the EEG Signals
2.5. Feature Extraction
2.6. Classification
2.7. Performance Evaluation
3. Experimental Results and Discussion
3.1. Results of the Channel-Based Evaluation Procedure
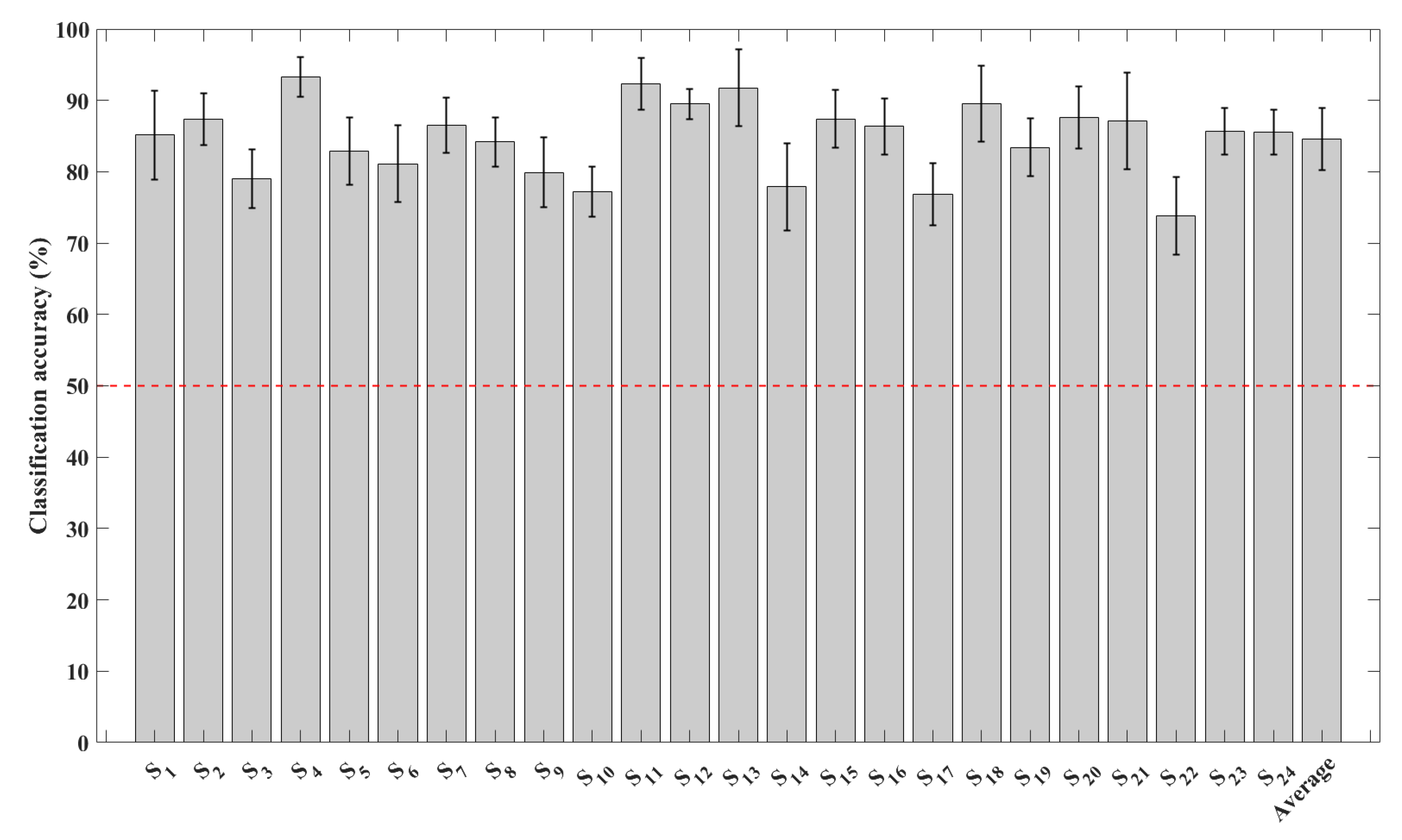
3.1.1. Results Obtained Using All the EEG Channels
3.1.2. Results of the Channel Reduction Procedure
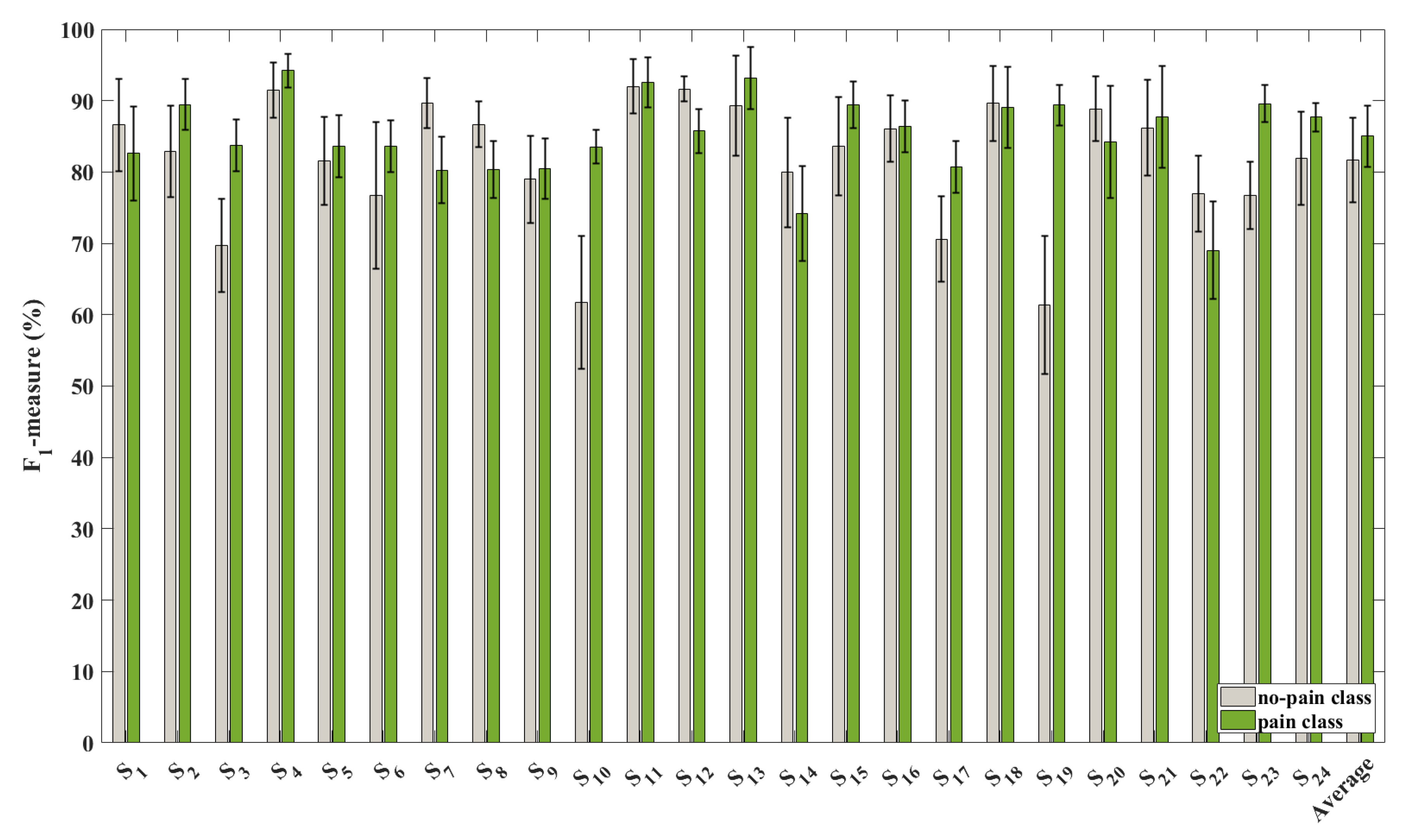
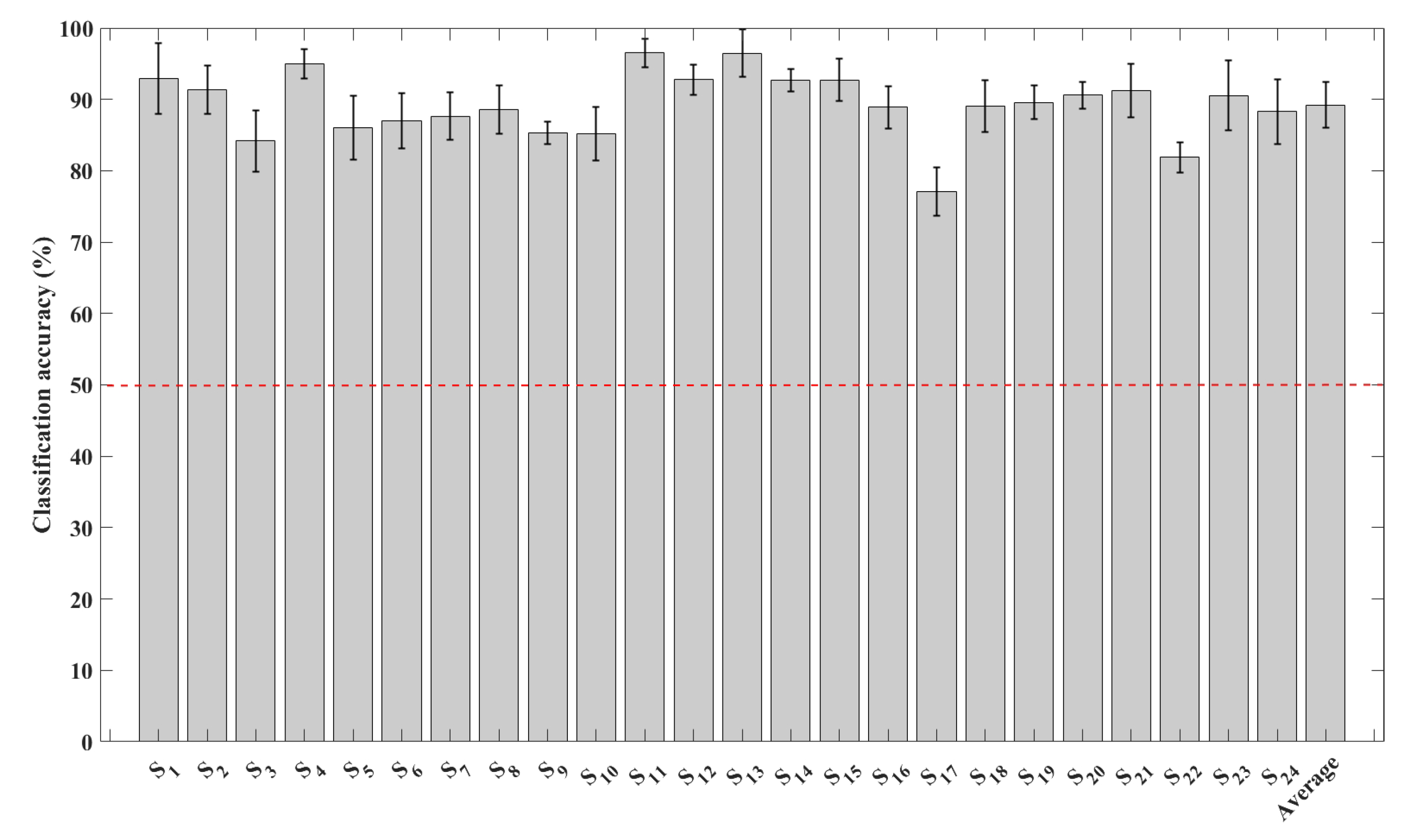
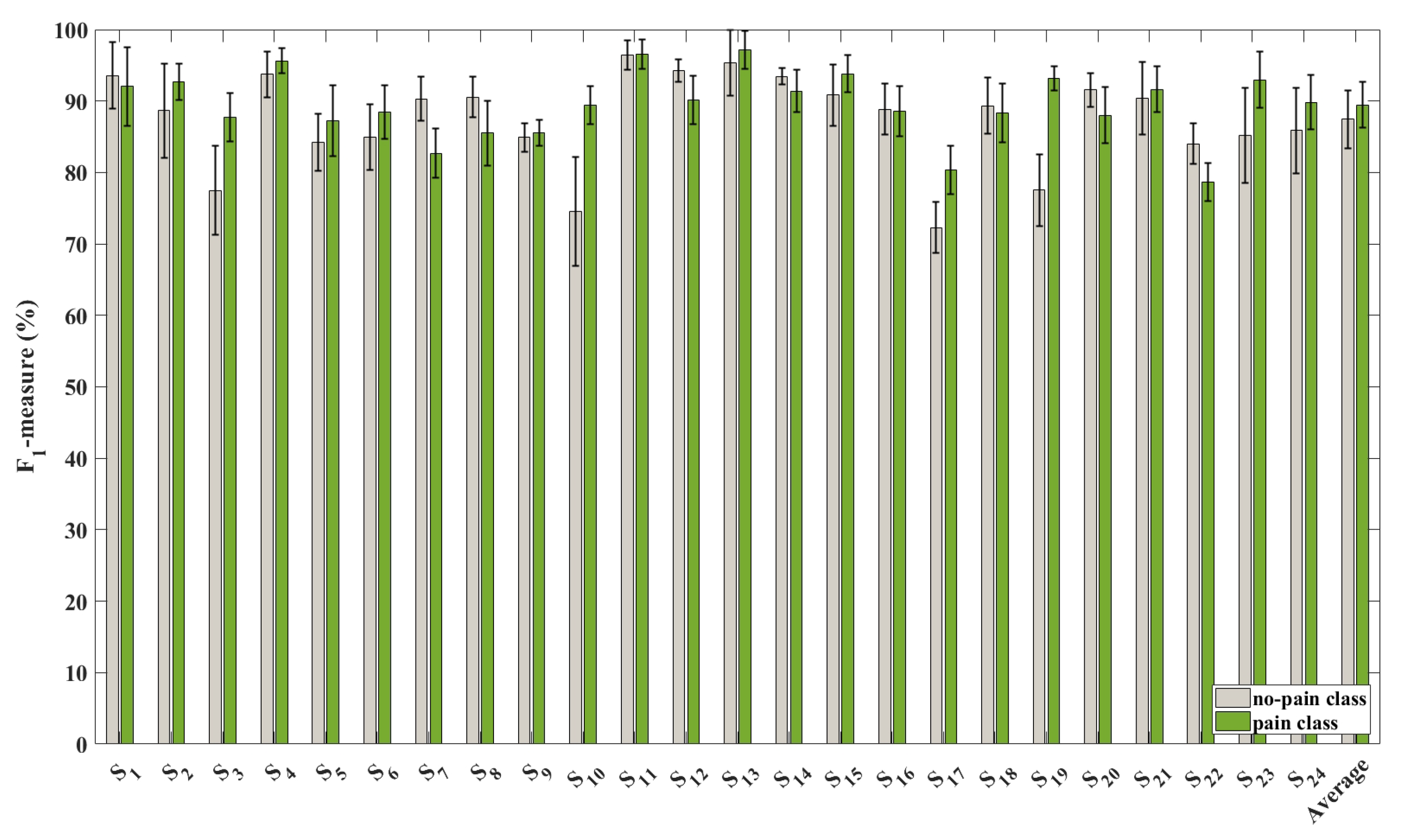
3.2. Results of the Feature-Based Evaluation Procedure
3.3. Comparison with Other Approaches
3.4. Limitations and Future Work
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Herr, K.; Coyne, P.J.; McCaffery, M.; Manworren, R.; Merkel, S. Pain assessment in the patient unable to self-report: Position statement with clinical practice recommendations. Pain Manag. Nurs. 2011, 12, 230–250. [Google Scholar] [CrossRef] [PubMed]
- Lamothe, M.; Roy, J.S.; Bouffard, J.; Gagné, M.; Bouyer, L.J.; Mercier, C. Effect of tonic pain on motor acquisition and retention while learning to reach in a force field. PLoS ONE 2014, 9, e99159. [Google Scholar] [CrossRef] [PubMed]
- Sinke, C.; Schmidt, K.; Forkmann, K.; Bingel, U. Phasic and tonic pain differentially impact the interruptive function of pain. PLoS ONE 2015, 10, e0118363. [Google Scholar] [CrossRef] [PubMed]
- Nicolas-Alonso, L.F.; Gomez-Gil, J. Brain computer interfaces, a review. Sensors 2012, 12, 1211–1279. [Google Scholar] [CrossRef] [PubMed]
- Alazrai, R.; Alwanni, H.; Baslan, Y.; Alnuman, N.; Daoud, M.I. EEG-Based Brain-Computer Interface for Decoding Motor Imagery Tasks within the Same Hand Using Choi–Williams Time-Frequency Distribution. Sensors 2017, 17, 1937. [Google Scholar] [CrossRef] [PubMed]
- Alazrai, R.; Alwanni, H.; Daoud, M.I. EEG-based BCI system for decoding finger movements within the same hand. Neurosci. Lett. 2019, 698, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Nir, R.R.; Sinai, A.; Raz, E.; Sprecher, E.; Yarnitsky, D. Pain assessment by continuous EEG: Association between subjective perception of tonic pain and peak frequency of alpha oscillations during stimulation and at rest. Brain Res. 2010, 1344, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Panavaranan, P.; Wongsawat, Y. EEG-based pain estimation via fuzzy logic and polynomial kernel support vector machine. In Proceedings of the 6th IEEE Biomedical Engineering International Conference, Amphur Muang, Thailand, 23–25 October 2013; pp. 1–4. [Google Scholar]
- Shao, S.; Shen, K.; Yu, K.; Wilder-Smith, E.P.; Li, X. Frequency-domain EEG source analysis for acute tonic cold pain perception. Clin. Neurophysiol. 2012, 123, 2042–2049. [Google Scholar] [CrossRef] [PubMed]
- Vatankhah, M.; Toliyat, A. Pain Level Measurement Using Discrete Wavelet Transform. Int. J. Eng. Technol. 2016, 8, 380–384. [Google Scholar] [CrossRef] [Green Version]
- Akansu, A.N.; Haddad, P.A.; Haddad, R.A.; Haddad, P.R. Multiresolution Signal Decomposition: Transforms, Subbands, and Wavelets; Academic Press: Cambridge, MA, USA, 2001. [Google Scholar]
- Mallat, S. A Wavelet Tour of Signal Processing: The Sparse Way; Academic Press: Cambridge, MA, USA, 2008. [Google Scholar]
- Hadjileontiadis, L.J. EEG-Based Tonic Cold Pain Characterization Using Wavelet Higher Order Spectral Features. IEEE Trans. Biomed. Eng. 2015, 62, 1981–1991. [Google Scholar] [CrossRef] [PubMed]
- Alazrai, R.; Aburub, S.; Fallouh, F.; Daoud, M.I. EEG-based BCI system for classifying motor imagery tasks of the same hand using empirical mode decomposition. In Proceedings of the 10th IEEE International Conference on Electrical and Electronics Engineering (ELECO), Bursa, Turkey, 30 November–2 December 2017; pp. 615–619. [Google Scholar]
- Toole, J.M.O. Discrete Quadratic Time-Frequency Distributions: Definition, Computation, and a Newborn Electroencephalogram Application. Ph.D. Thesis, School of Medicine, The University of Queensland, Brisbane, Australia, 2009. [Google Scholar]
- Boashash, B. Time-fRequency Signal Analysis and Processing: A Comprehensive Reference; Academic Press: Cambridge, MA, USA, 2015. [Google Scholar]
- Boashash, B.; Azemi, G.; O’Toole, J.M. Time-Frequency Processing of Nonstationary Signals: Advanced TFD Design to Aid Diagnosis with Highlights from Medical Applications. IEEE Signal Process. Mag. 2013, 30, 108–119. [Google Scholar] [CrossRef]
- Boashash, B.; Ouelha, S. Automatic signal abnormality detection using time-frequency features and machine learning: A newborn EEG seizure case study. Knowl.-Based Syst. 2016, 106, 38–50. [Google Scholar] [CrossRef]
- Dowman, R.; Rissacher, D.; Schuckers, S. EEG indices of tonic pain-related activity in the somatosensory cortices. Clin. Neurophysiol. 2008, 119, 1201–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Herrero, G.; De Clercq, W.; Anwar, H.; Kara, O.; Egiazarian, K.; Van Huffel, S.; Van Paesschen, W. Automatic removal of ocular artifacts in the EEG without an EOG reference channel. In Proceedings of the IEEE 7th Nordic Signal Processing Symposium, Rejkjavik, Iceland, 7–9 June 2006; pp. 130–133. [Google Scholar]
- Alazrai, R.; Homoud, R.; Alwanni, H.; Daoud, M.I. EEG-Based Emotion Recognition Using Quadratic Time-Frequency Distribution. Sensors 2018, 18, 2739. [Google Scholar] [CrossRef] [PubMed]
- Castiglioni, P. Choi–Williams Distribution. In Encyclopedia of Biostatistics; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2005. [Google Scholar]
- Alazrai, R.; Momani, M.; Khudair, H.A.; Daoud, M.I. EEG-based tonic cold pain recognition system using wavelet transform. Neural Comput. Appl. 2017. [Google Scholar] [CrossRef]
- Choi, H.I.; Williams, W.J. Improved time-frequency representation of multicomponent signals using exponential kernels. IEEE Trans. Acoust. Speech Signal Process. 1989, 37, 862–871. [Google Scholar] [CrossRef]
- Hahn, S.L. Hilbert Transforms in Signal Processing; Artech House Boston: Norwood, MA, USA, 1996; Volume 2. [Google Scholar]
- Swami, A.; Mendel, J.; Nikias, C. Higher-Order Spectra Analysis (HOSA) Toolbox. Version 2.0. 2000. Available online: http://www.mathworks.com/matlabcentral/fileexchange/3013 (accessed on 30 June 2019).
- Chang, C.C.; Lin, C.J. LIBSVM: A library for support vector machines. ACM Trans. Intell. Syst. Technol. 2011, 2, 27. [Google Scholar] [CrossRef]
- Hsu, C.W.; Chang, C.C.; Lin, C.J. A Practical Guide to Support Vector Classification; Technical Report; Department of Computer Science, National Taiwan University: Taipei, Taiwan, 2003. [Google Scholar]
- Al-Timemy, A.H.; Bugmann, G.; Escudero, J.; Outram, N. Classification of Finger Movements for the Dexterous Hand Prosthesis Control With Surface Electromyography. IEEE J. Biomed. Health Inform. 2013, 17, 608–618. [Google Scholar] [CrossRef] [PubMed]
- Goge, A.; Chan, A. Investigating Classification Parameters for Continuous Myoelectrically Controlled Prostheses; Canadian Medical and Biological Engineering Society: Ottawa, ON, Canada, 2005; Volume 28. [Google Scholar]
- Li, G.; Schultz, A.E.; Kuiken, T.A. Quantifying Pattern Recognition—Based Myoelectric Control of Multifunctional Transradial Prostheses. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 185–192. [Google Scholar] [PubMed]
- Li, G.; Kuiken, T.A. EMG pattern recognition control of multifunctional prostheses by transradial amputees. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 6914–6917. [Google Scholar]
- Han, J.; Pei, J.; Kamber, M. Data Mining: Concepts and Techniques; Elsevier: Amsterdam, The Netherlands, 2011. [Google Scholar]
- Van den Broek, S.P.; Reinders, F.; Donderwinkel, M.; Peters, M. Volume conduction effects in EEG and MEG. Electroencephalogr. Clin. Neurophysiol. 1998, 106, 522–534. [Google Scholar] [CrossRef]
- Liao, K.; Xiao, R.; Gonzalez, J.; Ding, L. Decoding individual finger movements from one hand using human EEG signals. PLoS ONE 2014, 9, e85192. [Google Scholar] [CrossRef] [PubMed]
- Aftanas, L.; Reva, N.; Varlamov, A.; Pavlov, S.; Makhnev, V. Analysis of evoked EEG synchronization and desynchronization in conditions of emotional activation in humans: Temporal and topographic characteristics. Neurosci. Behav. Physiol. 2004, 34, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, Z.; Frounchi, J.; Amiri, M. Wavelet-based emotion recognition system using EEG signal. Neural Comput. Appl. 2017, 28, 1985–1990. [Google Scholar] [CrossRef]
- Penfield, W.; Rasmussen, T.; Erickson, T. The Cerebral Cortex of Man, a Clinical Study of Localization of Function. Am. J. Phys. Med. Rehabil. 1954, 33, 126. [Google Scholar]
- Borckardt, J.J.; Romagnuolo, J.; Reeves, S.T.; Madan, A.; Frohman, H.; Beam, W.; George, M.S. Feasibility, safety, and effectiveness of transcranial direct current stimulation for decreasing post-ERCP pain: A randomized, sham-controlled, pilot study. Gastrointest. Endosc. 2011, 73, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Morabito, F.C.; Campolo, M.; Mammone, N.; Versaci, M.; Franceschetti, S.; Tagliavini, F.; Sofia, V.; Fatuzzo, D.; Gambardella, A.; Labate, A.; et al. Deep learning representation from electroencephalography of early-stage Creutzfeldt-Jakob disease and features for differentiation from rapidly progressive dementia. Int. J. Neural Syst. 2017, 27, 1650039. [Google Scholar] [CrossRef] [PubMed]
- Alazrai, R.; Abuhijleh, M.; Alwanni, H.; Daoud, M.I. A Deep Learning Framework for Decoding Motor Imagery Tasks of the Same Hand using EEG Signals. IEEE Access 2019, 7, 109612–109627. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time-Frequency Feature | Mathematical Expression of the Time-Frequency Feature |
|---|---|
| The mean of the CWD () | |
| The variance of the CWD () | |
| The skewness of the CWD () | |
| The kurtosis of the CWD () | |
| Sum of the logarithmic amplitudes of the CWD () | |
| Median absolute deviation of the CWD () | |
| Root mean square value of the CWD () | |
| interquartile range of the CWD () | |
| The flatness of the CWD () | |
| The flux of the CWD () | |
| The normalized Renyi entropy of the CWD () | |
| The energy concentration of the CWD () |
| Iterations of the Channel Reduction Procedure | Eliminated EEG Channel | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Average classification accuracy(%) | Iteration 1 | 83.76 | 83.53 | 83.69 | 83.82 | 84.08 | 83.59 | 83.89 | 83.78 | 84.11 | 84.15 | 83.93 | 84.23 | 83.59 | 84.33 |
| Iteration 2 | 83.19 | 82.98 | 82.96 | 83.55 | 83.29 | 83.27 | 83.42 | 82.82 | 83.24 | 83.20 | 83.75 | 83.60 | 83.76 | ||
| Iteration 3 | 81.83 | 82.18 | 82.13 | 82.43 | 82.52 | 82.40 | 82.11 | 82.07 | 82.40 | 82.61 | 82.55 | 82.63 | |||
| Iteration 4 | 81.60 | 81.62 | 81.13 | 82.38 | 81.98 | 81.92 | 81.99 | 82.04 | 81.98 | 82.30 | 82.57 | ||||
| Iteration 5 | 80.81 | 81.22 | 80.88 | 81.30 | 81.37 | 81.32 | 81.51 | 81.44 | 81.59 | 81.72 | |||||
| Iteration 6 | 80.54 | 80.37 | 79.11 | 80.43 | 80.68 | 80.68 | 80.57 | 80.84 | 81.08 | ||||||
| Iteration 7 | 78.98 | 79.63 | 78.26 | 79.71 | 79.66 | 79.64 | 79.75 | 79.98 | |||||||
| Iteration 8 | 77.58 | 78.27 | 77.75 | 78.26 | 78.10 | 78.24 | 78.72 | ||||||||
| Iteration 9 | 75.70 | 76.27 | 76.29 | 76.31 | 76.46 | 76.96 | |||||||||
| Iteration 10 | 74.20 | 74.86 | 74.29 | 74.75 | 75.34 | ||||||||||
| Iteration 11 | 71.41 | 71.69 | 72.06 | 72.23 | |||||||||||
| Iteration 12 | 68.32 | 69.20 | 71.01 | ||||||||||||
| Iteration 13 | 65.08 | 65.90 | |||||||||||||
| Iteration 14 | 65.90 | ||||||||||||||
| Iterations of the Feature Reduction Procedure | Eliminated Time-Frequency Feature | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Average classification accuracy(%) | Iteration 1 | 84.36 | 82.21 | 84.41 | 84.53 | 84.54 | 85.05 | 84.61 | 84.68 | 83.59 | 85.67 | 85.39 | 86.63 |
| Iteration 2 | 86.04 | 84.45 | 86.22 | 86.23 | 86.44 | 86.73 | 86.23 | 86.45 | 85.93 | 87.35 | 87.68 | ||
| Iteration 3 | 87.24 | 85.79 | 87.25 | 87.44 | 87.63 | 87.95 | 87.45 | 87.61 | 86.62 | 88.62 | |||
| Iteration 4 | 88.49 | 87.05 | 88.55 | 88.69 | 88.64 | 88.04 | 88.66 | 88.71 | 88.81 | ||||
| Iteration 5 | 87.87 | 83.98 | 87.94 | 88.31 | 88.25 | 88.29 | 88.25 | 88.39 | |||||
| Iteration 6 | 88.25 | 84.65 | 87.94 | 88.31 | 88.25 | 88.29 | 88.39 | ||||||
| Iteration 7 | 87.91 | 84.25 | 87.73 | 88.3 | 88.26 | 88.5 | |||||||
| Iteration 8 | 88.47 | 86.37 | 88.62 | 88.72 | 88.88 | ||||||||
| Iteration 9 | 88.85 | 86.66 | 88.73 | 89.24 | |||||||||
| Iteration 10 | 88.51 | 86.83 | 89.02 | ||||||||||
| Iteration 11 | 87.01 | 87.06 | |||||||||||
| Iteration 12 | 87.06 | ||||||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alazrai, R.; AL-Rawi, S.; Alwanni, H.; Daoud, M.I. Tonic Cold Pain Detection Using Choi–Williams Time-Frequency Distribution Analysis of EEG Signals: A Feasibility Study. Appl. Sci. 2019, 9, 3433. https://doi.org/10.3390/app9163433
Alazrai R, AL-Rawi S, Alwanni H, Daoud MI. Tonic Cold Pain Detection Using Choi–Williams Time-Frequency Distribution Analysis of EEG Signals: A Feasibility Study. Applied Sciences. 2019; 9(16):3433. https://doi.org/10.3390/app9163433
Chicago/Turabian StyleAlazrai, Rami, Saifaldeen AL-Rawi, Hisham Alwanni, and Mohammad I. Daoud. 2019. "Tonic Cold Pain Detection Using Choi–Williams Time-Frequency Distribution Analysis of EEG Signals: A Feasibility Study" Applied Sciences 9, no. 16: 3433. https://doi.org/10.3390/app9163433