
Particulate Matter 2.5 Level Modulates Brachial Artery Flow-Mediated Dilation Response to Aerobic Exercise in Healthy Young Men


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
2.3. Body Composition
2.4. Maximal Cardiopulmonary Exercise Test
2.5. Blood Pressure and Brachial Artery Flow-Mediated Dilation
2.6. PM2.5 Concentration
2.7. Statistical Analyses
3. Results
3.1. Subject Characteristics and PM2.5 Concentrations
3.2. Responses to Treadmill Running in HPM2.5 and LPM2.5 Conditions
3.2.1. Blood Pressure
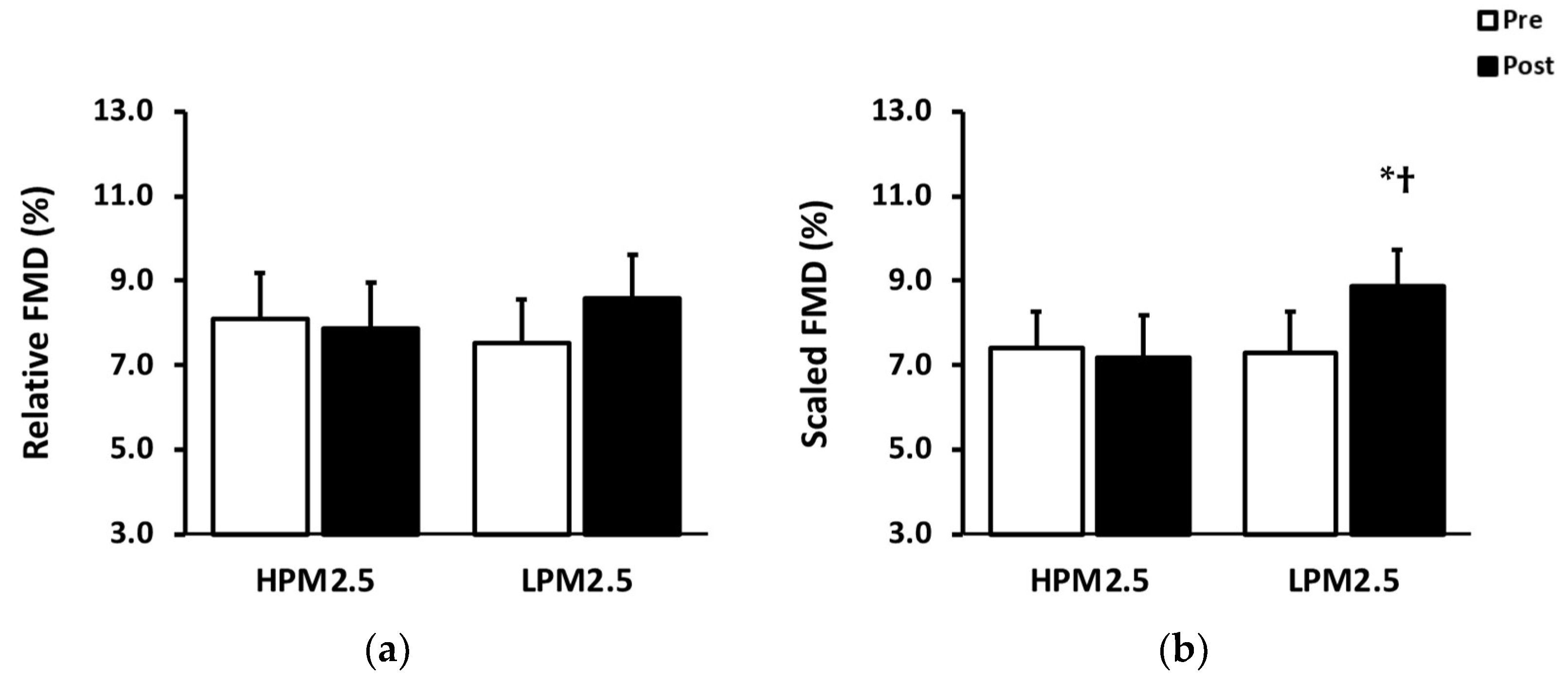
3.2.2. Brachial Artery Flow-Mediated Dilation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alexeeff, S.E.; Liao, N.S.; Liu, X.; Van Den Eeden, S.K.; Sidney, S. Long-Term PM2.5 Exposure and Risks of Ischemic Heart Disease and Stroke Events: Review and Meta-Analysis. J. Am. Heart Assoc. 2021, 10, e016890. [Google Scholar] [CrossRef] [PubMed]
- Hayes, R.B.; Lim, C.; Zhang, Y.; Cromar, K.; Shao, Y.; Reynolds, H.R.; Silverman, D.T.; Jones, R.R.; Park, Y.; Jerrett, M.; et al. PM2.5 air pollution and cause-specific cardiovascular disease mortality. Int. J. Epidemiol. 2020, 49, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Kim, O.J.; Lee, S.H.; Kang, S.H.; Kim, S.Y. Incident cardiovascular disease and particulate matter air pollution in South Korea using a population-based and nationwide cohort of 0.2 million adults. Environ. Health Glob. 2020, 19, 113. [Google Scholar] [CrossRef]
- Miller, M.R.; Newby, D.E. Air pollution and cardiovascular disease: Car sick. Cardiovasc. Res. 2020, 116, 279–294. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A., 3rd; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.Y.; Mancini, G.B.; Kuramoto, L.; Schulzer, M.; Frohlich, J.; Ignaszewski, A. The prognostic importance of endothelial dysfunction and carotid atheroma burden in patients with coronary artery disease. J. Am. Coll Cardiol. 2003, 42, 1037–1043. [Google Scholar] [CrossRef]
- Gokce, N.; Keaney, J.F., Jr.; Hunter, L.M.; Watkins, M.T.; Menzoian, J.O.; Vita, J.A. Risk stratification for postoperative cardiovascular events via noninvasive assessment of endothelial function: A prospective study. Circulation 2002, 105, 1567–1572. [Google Scholar] [CrossRef]
- Luscher, T.F.; Barton, M. Biology of the endothelium. Clin. Cardiol. 1997, 20, II-3–II-10. [Google Scholar] [CrossRef]
- Early, K.S.; Stewart, A.; Johannsen, N.; Lavie, C.J.; Thomas, J.R.; Welsch, M. The Effects of Exercise Training on Brachial Artery Flow-Mediated Dilation: A Meta-analysis. J. Cardiopulm. Rehabil. Prev. 2017, 37, 77–89. [Google Scholar] [CrossRef]
- Kapilevich, L.V.; Kologrivova, V.V.; Zakharova, A.N.; Mourot, L. Post-exercise Endothelium-Dependent Vasodilation Is Dependent on Training Status. Front. Physiol. 2020, 11, 348. [Google Scholar] [CrossRef]
- Siasos, G.; Athanasiou, D.; Terzis, G.; Stasinaki, A.; Oikonomou, E.; Tsitkanou, S.; Kolokytha, T.; Spengos, K.; Papavassiliou, A.G.; Tousoulis, D. Acute effects of different types of aerobic exercise on endothelial function and arterial stiffness. Eur. J. Prev. Cardiol. 2016, 23, 1565–1572. [Google Scholar] [CrossRef] [PubMed]
- Becquemin, M.H.; Swift, D.L.; Bouchikhi, A.; Roy, M.; Teillac, A. Particle deposition and resistance in the noses of adults and children. Eur. Respir. J. 1991, 4, 694–702. [Google Scholar] [CrossRef]
- Daigle, C.C.; Chalupa, D.C.; Gibb, F.R.; Morrow, P.E.; Oberdorster, G.; Utell, M.J.; Frampton, M.W. Ultrafine particle deposition in humans during rest and exercise. Inhal. Toxicol. 2003, 15, 539–552. [Google Scholar] [CrossRef]
- McCafferty, W.B.; Horvath, S. Air Pollution and Athletic Performance; Charles C Thomas Publisher Ltd.: Springfield, IL, USA, 1981. [Google Scholar]
- Cole, C.A.; Carlsten, C.; Koehle, M.; Brauer, M. Particulate matter exposure and health impacts of urban cyclists: A randomized crossover study. Environ. Health 2018, 17, 78. [Google Scholar] [CrossRef] [PubMed]
- Giles, L.V.; Tebbutt, S.J.; Carlsten, C.; Koehle, M.S. The effect of low and high-intensity cycling in diesel exhaust on flow-mediated dilation, circulating NOx, endothelin-1 and blood pressure. PLoS ONE 2018, 13, e0192419. [Google Scholar] [CrossRef] [PubMed]
- Weichenthal, S.; Hatzopoulou, M.; Goldberg, M.S. Exposure to traffic-related air pollution during physical activity and acute changes in blood pressure, autonomic and micro-vascular function in women: A cross-over study. Part Fibre Toxicol. 2014, 11, 70. [Google Scholar] [CrossRef]
- Peretz, A.; Sullivan, J.H.; Leotta, D.F.; Trenga, C.A.; Sands, F.N.; Allen, J.; Carlsten, C.; Wilkinson, C.W.; Gill, E.A.; Kaufman, J.D. Diesel exhaust inhalation elicits acute vasoconstriction in vivo. Environ. Health Perspect. 2008, 116, 937–942. [Google Scholar] [CrossRef]
- Krebs, B.; Burney, J.; Zivin, J.G.; Neidell, M. Using Crowd-Sourced Data to Assess the Temporal and Spatial Relationship between Indoor and Outdoor Particulate Matter. Environ. Sci. Technol. 2021, 55, 6107–6115. [Google Scholar] [CrossRef]
- Thijssen, D.H.J.; Bruno, R.M.; van Mil, A.; Holder, S.M.; Faita, F.; Greyling, A.; Zock, P.L.; Taddei, S.; Deanfield, J.E.; Luscher, T.; et al. Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur. Heart J. 2019, 40, 2534–2547. [Google Scholar] [CrossRef]
- Stefani, L.; Mascherini, G.; Galanti, G. Aerobic threshold for exercise prescription. Int. J. Clin. Med. 2010, 1, 6–9. [Google Scholar] [CrossRef]
- Atkinson, G.; Batterham, A.M. Allometric scaling of diameter change in the original flow-mediated dilation protocol. Atherosclerosis 2013, 226, 425–427. [Google Scholar] [CrossRef]
- Barath, S.; Mills, N.L.; Lundback, M.; Tornqvist, H.; Lucking, A.J.; Langrish, J.P.; Soderberg, S.; Boman, C.; Westerholm, R.; Londahl, J.; et al. Impaired vascular function after exposure to diesel exhaust generated at urban transient running conditions. Part Fibre Toxicol. 2010, 7, 19. [Google Scholar] [CrossRef] [PubMed]
- Tornqvist, H.; Mills, N.L.; Gonzalez, M.; Miller, M.R.; Robinson, S.D.; Megson, I.L.; Macnee, W.; Donaldson, K.; Soderberg, S.; Newby, D.E.; et al. Persistent endothelial dysfunction in humans after diesel exhaust inhalation. Am. J. Respir. Crit. Care Med. 2007, 176, 395–400. [Google Scholar] [CrossRef]
- Johnson, B.D.; Padilla, J.; Wallace, J.P. The exercise dose affects oxidative stress and brachial artery flow-mediated dilation in trained men. Eur. J. Appl. Physiol. 2012, 112, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Tinken, T.M.; Thijssen, D.H.J.; Hopkins, N.; Black, M.A.; Dawson, E.A.; Minson, C.T.; Newcomer, S.C.; Laughlin, M.H.; Cable, N.T.; Green, D.J. Impact of Shear Rate Modulation on Vascular Function in Humans. Hypertension 2009, 54, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Rundell, K.W.; Hoffman, J.R.; Caviston, R.; Bulbulian, R.; Hollenbach, A.M. Inhalation of ultrafine and fine particulate matter disrupts systemic vascular function. Inhal. Toxicol. 2007, 19, 133–140. [Google Scholar] [CrossRef]
- Li, Z.W.; Hyseni, X.; Carter, J.D.; Soukup, J.M.; Dailey, L.A.; Huang, Y.C.T. Pollutant particles enhanced H2O2 production from NAD(P)H oxidase and mitochondria in human pulmonary artery endothelial cells. Am. J. Physiol.-Cell Physiol. 2006, 291, C357–C365. [Google Scholar] [CrossRef]
- Wauters, A.; Dreyfuss, C.; Pochet, S.; Hendrick, P.; Berkenboom, G.; van de Borne, P.; Argacha, J.F. Acute Exposure to Diesel Exhaust Impairs Nitric Oxide-Mediated Endothelial Vasomotor Function by Increasing Endothelial Oxidative Stress. Hypertension 2013, 62, 352–358. [Google Scholar] [CrossRef]
- Ohara, Y.; Peterson, T.E.; Harrison, D.G. Hypercholesterolemia Increases Endothelial Superoxide Anion Production. J. Clin. Investig. 1993, 91, 2546–2551. [Google Scholar] [CrossRef]
- Rundell, K.W.; Steigerwald, M.D.; Fisk, M.Z. Montelukast prevents vascular endothelial dysfunction from internal combustion exhaust inhalation during exercise. Inhal. Toxicol. 2010, 22, 754–759. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S. Getting Sympathetic About Air Pollution Exposure. J. Am. Heart Assoc. 2021, 10, e021675. [Google Scholar] [CrossRef] [PubMed]
- Hijmering, M.L.; Stroes, E.S.G.; Olijhoek, J.; Hutten, B.A.; Blankestijn, P.J.; Rabelink, T.J. Sympathetic activation markedly reduces endothelium-dependent, flow-mediated vasodilation. J. Am. Coll. Cardiol. 2002, 39, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Brook, J.R.; Urch, B.; Vincent, R.; Rajagopalan, S.; Silverman, F. Inhalation of fine particulate air pollution and ozone causes acute arterial vasoconstriction in healthy adults. Circulation 2002, 105, 1534–1536. [Google Scholar] [CrossRef] [PubMed]
- Thomson, E.; Goegan, P.; Kumarathasan, P.; Vincent, R. Air pollutants increase gene expression of the vasoconstrictor endothelin-1 in the lungs. BBA Mol. Basis Dis. 2004, 1689, 75–82. [Google Scholar] [CrossRef]
- Black, M.A.; Cable, N.T.; Thijssen, D.H.J.; Green, D.J. Importance of measuring the time course of flow-mediated dilatation in humans. Hypertension 2008, 51, 203–210. [Google Scholar] [CrossRef]
- Fernandes, I.A.; Sales, A.R.K.; Rocha, N.G.; Silva, B.M.; Vianna, L.C.; da Nobrega, A.C.L. Preserved flow-mediated dilation but delayed time-to-peak diameter in individuals with metabolic syndrome. Clin. Physiol. Funct. I 2014, 34, 270–276. [Google Scholar] [CrossRef]
- Irace, C.; Tschakovsky, M.E.; Carallo, C.; Cortese, C.; Gnasso, A. Endothelial dysfunction or dysfunctions? Identification of three different FMD responses in males with type 2 diabetes. Atherosclerosis 2008, 200, 439–445. [Google Scholar] [CrossRef]
- Irace, C.; Carallo, C.; Loprete, A.; Tripolino, C.; Scavelli, F.; Gnasso, A. Delayed flow-mediated vasodilation and carotid atherosclerosis. Eur. J. Clin. Invest. 2013, 43, 49–55. [Google Scholar] [CrossRef]
- Zanoli, L.; Lentini, P.; Granata, A.; Gaudio, A.; Fatuzzo, P.; Serafino, L.; Rastelli, S.; Fiore, V.; D’Anca, A.; Santo Signorelli, S.; et al. A systematic review of arterial stiffness, wave reflection and air pollution. Mol. Med. Rep. 2017, 15, 3425–3429. [Google Scholar] [CrossRef]
- Tripolino, C.; Gnasso, A.; Carallo, C.; Scavelli, F.B.; Irace, C. Difference in carotid artery elasticity in subjects with different brachial artery kinetic of vasodilatation. J. Hum. Hypertens. 2016, 30, 493–497. [Google Scholar] [CrossRef]
- Ballard, K.D.; Timsina, R.; Timmerman, K.L. Influence of time of day and intermittent aerobic exercise on vascular endothelial function and plasma endothelin-1 in healthy adults. Chronobiol. Int. 2021, 38, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Weitzberg, E.; Ahlborg, G.; Lundberg, J.M. Differences in Vascular Effects and Removal of Endothelin-1 in Human Lung, Brain, and Skeletal-Muscle. Clin. Physiol. 1993, 13, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Franklin, B.A.; Brook, R.; Pope, C.A. Air Pollution and Cardiovascular Disease. Curr. Prob. Cardiol. 2015, 40, 207–238. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| HPM2.5 | LPM2.5 | |
|---|---|---|
| Age, years | 24.6 ± 0.4 | |
| Height, cm | 177.4 ± 1.5 | |
| Body weight, kg | 77.9 ± 1.6 | 77.5 ± 1.8 |
| BMI, kg/m2 | 24.8 ± 0.6 | 24.7 ± 0.7 |
| Outdoor PM2.5 concentration, μg/m3 | 150.9 ± 27.1 * | 17.6 ± 4.7 |
| Indoor PM2.5 concentration, μg/m3 | 59.0 ± 2.1 * | 7.8 ± 1.0 |
| HPM2.5 | LPM2.5 | p-Value | |||||
|---|---|---|---|---|---|---|---|
| pre | Post | pre | Post | C | T | C × T | |
| SBP, mmHg | 114.2 ± 2.0 | 120.3 ± 2.3 | 116.0 ± 2.3 | 119.7 ± 2.4 | 0.47 | <0.001 | 0.22 |
| DBP, mmHg | 70.3 ± 2.6 | 73.6 ± 2.6 | 69.8 ± 3.0 | 73.0 ± 2.7 | 0.66 | <0.001 | >0.99 |
| PP, mmHg | 43.9 ± 1.5 | 46.8 ± 1.5 | 46.2 ± 1.3 | 46.7 ± 2.0 | 0.49 | 0.07 | 0.26 |
| HR, bpm | 59.3 ± 2.4 | 76.9 ± 1.9 | 60.3 ± 2.8 | 76.1 ± 2.8 | 0.94 | <0.001 | 0.39 |
| HPM2.5 | LPM2.5 | p-Value | |||||
|---|---|---|---|---|---|---|---|
| pre | Post | pre | Post | C | T | C × T | |
| Baseline diameter, mm | 3.68 ± 0.11 #,† | 3.78 ± 0.10 * | 3.76 ± 0.11 | 3.74 ± 0.11 | 0.51 | <0.01 | <0.01 |
| Peak diameter, mm | 3.97 ± 0.11 † | 4.07 ± 0.10 | 4.04 ± 0.10 | 4.06 ± 0.12 | 0.42 | 0.03 | 0.15 |
| Absolute FMD, mm | 0.29 ± 0.04 | 0.29 ±0.04 | 0.28 ± 0.03 | 0.32 ± 0.03 | 0.86 | 0.40 | 0.16 |
| FMD/SRAUC, 10−3 % s | 0.14 ± 0.02 | 0.11 ± 0.01 | 0.12 ± 0.01 | 0.15 ± 0.02 | 0.37 | 0.23 | 0.35 |
| SRAUC, 103 s−1 | 54.13 ± 5.14 | 63.88 ± 3.83 | 64.75 ± 7.11 | 65.74 ± 7.95 | 0.33 | 0.26 | 0.22 |
| TTP, s | 58.8 ± 1.0 † | 57.4 ± 3.2 | 52.1 ± 2.8 | 55.3 ± 3.5 | 0.18 | 0.76 | 0.31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-S.; Lee, D.G.; Hwang, M.-H. Particulate Matter 2.5 Level Modulates Brachial Artery Flow-Mediated Dilation Response to Aerobic Exercise in Healthy Young Men. Appl. Sci. 2023, 13, 4936. https://doi.org/10.3390/app13084936
Kim J-S, Lee DG, Hwang M-H. Particulate Matter 2.5 Level Modulates Brachial Artery Flow-Mediated Dilation Response to Aerobic Exercise in Healthy Young Men. Applied Sciences. 2023; 13(8):4936. https://doi.org/10.3390/app13084936
Chicago/Turabian StyleKim, Jin-Su, Do Gyun Lee, and Moon-Hyon Hwang. 2023. "Particulate Matter 2.5 Level Modulates Brachial Artery Flow-Mediated Dilation Response to Aerobic Exercise in Healthy Young Men" Applied Sciences 13, no. 8: 4936. https://doi.org/10.3390/app13084936