
Preclinical Evaluation of Bioactive Scaffolds for the Treatment of Mandibular Critical-Sized Bone Defects: A Systematic Review

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
1.1. Role of Scaffolds in BTE
1.2. Properties of an Ideal Scaffold for Bone Regeneration
2. Materials and Methods
2.1. Hypothesis
2.2. Research Question
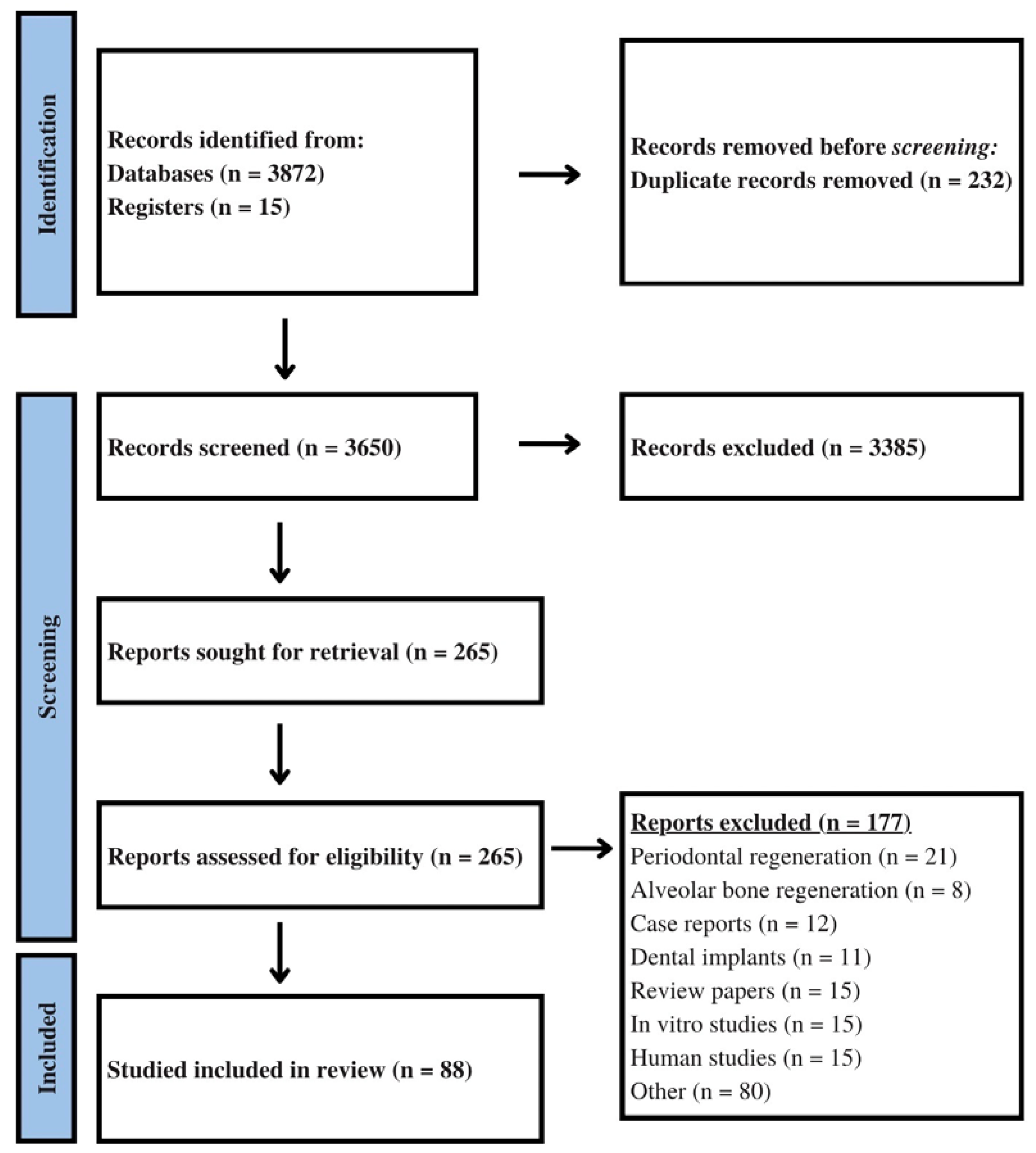
2.3. Search Strategy
2.4. Eligibility Criteria
2.5. Data Extraction
3. Results
3.1. Study Design
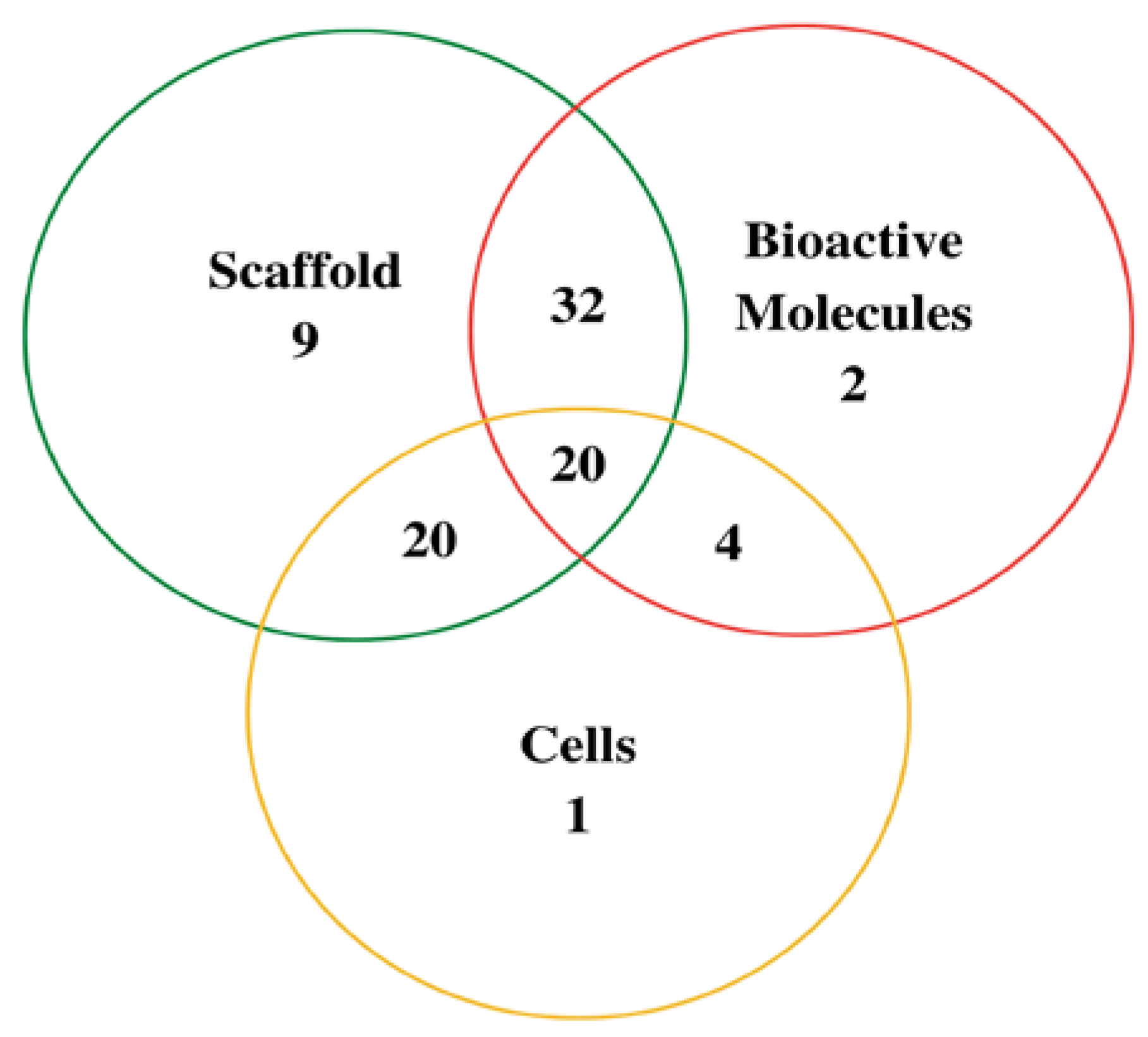
3.2. Scaffolds
3.3. Bioactive Substances
3.4. Cell Therapy
4. Discussion
4.1. Scaffolds
4.2. Bioactive Molecules
4.3. Cell Therapy
4.4. Animal Models
4.5. Study Outcomes
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vujovic, S.; Desnica, J.; Stanisic, D.; Ognjanovic, I.; Stevanovic, M.; Rosic, G. Applications of Biodegradable Magnesium-Based Materials in Reconstructive Oral and Maxillofacial Surgery: A Review. Molecules 2022, 27, 5529. [Google Scholar] [CrossRef]
- Basyuni, S.; Ferro, A.; Santhanam, V.; Birch, M.; McCaskie, A. Systematic scoping review of mandibular bone tissue engineering. Br. J. Oral Maxillofac. Surg. 2020, 58, 632–642. [Google Scholar] [CrossRef]
- Liu, L.; Shi, G.; Cui, Y.; Li, H.; Li, Z.; Zeng, Q.; Guo, Y. Individual construction of freeform-fabricated polycaprolactone scaffolds for osteogenesis. Biomed. Tech. 2017, 62, 467–479. [Google Scholar] [CrossRef]
- Amini, A.R.; Laurencin, C.T.; Nukavarapu, S.P. Bone tissue engineering: Recent advances and challenges. Crit. Rev. Biomed. Eng. 2012, 40, 363–408. [Google Scholar] [CrossRef] [Green Version]
- Oryan, A.; Alidadi, S.; Moshiri, A. Current concerns regarding healing of bone defects. Hard Tissue 2013, 2, 13. [Google Scholar] [CrossRef]
- Jamari, J.; Ammarullah, M.I.; Saad, A.P.M.; Syahrom, A.; Uddin, M.; van der Heide, E.; Basri, H. The Effect of Bottom Profile Dimples on the Femoral Head on Wear in Metal-on-Metal Total Hip Arthroplasty. J. Funct. Biomater. 2021, 12, 38. [Google Scholar] [CrossRef]
- Kretlow, J.D.; Young, S.; Klouda, L.; Wong, M.; Mikos, A.G. Injectable biomaterials for regenerating complex craniofacial tissues. Adv. Mater. 2009, 21, 3368–3393. [Google Scholar] [CrossRef] [Green Version]
- Azevedo, H.S.; Pashkuleva, I. Biomimetic supramolecular designs for the controlled release of growth factors in bone regeneration. Adv. Drug Deliv. Rev. 2015, 94, 63–76. [Google Scholar] [CrossRef] [Green Version]
- Oryan, A.; Kamali, A.; Moshiri, A.; Baghaban Eslaminejad, M. Role of Mesenchymal Stem Cells in Bone Regenerative Medicine: What Is the Evidence? Cells Tissues Organs 2017, 204, 59–83. [Google Scholar] [CrossRef]
- Thrivikraman, G.; Athirasala, A.; Twohig, C.; Boda, S.K.; Bertassoni, L.E. Biomaterials for Craniofacial Bone Regeneration. Dent. Clin. N. Am. 2017, 61, 835–856. [Google Scholar] [CrossRef]
- Putra, R.U.; Basri, H.; Prakoso, A.T.; Chandra, H.; Ammarullah, M.I.; Akbar, I.; Syahrom, A.; Kamarul, T. Level of Activity Changes Increases the Fatigue Life of the Porous Magnesium Scaffold, as Observed in Dynamic Immersion Tests, over Time. Sustainability 2023, 15, 823. [Google Scholar] [CrossRef]
- Stevanovic, M.; Vujovic, S.; Stanisic, D.; Desnica, J.; Ognjanovic, I. The Use of Newly Synthesized Composite Scaffolds for Bone Regeneration—A Review of Literature. Exp. Appl. Biomed. Res. EABR 2022. [Google Scholar] [CrossRef]
- Venkataiah, V.S.; Yahata, Y.; Kitagawa, A.; Inagaki, M.; Kakiuchi, Y.; Nakano, M.; Suzuki, S.; Handa, K.; Saito, M. Clinical Applications of Cell-Scaffold Constructs for Bone Regeneration Therapy. Cells 2021, 10, 2687. [Google Scholar] [CrossRef]
- Valdoz, J.C.; Johnson, B.C.; Jacobs, D.J.; Franks, N.A.; Dodson, E.L.; Sanders, C.; Cribbs, C.G.; Van Ry, P.M. The ECM: To Scaffold, or Not to Scaffold, That Is the Question. Int. J. Mol. Sci. 2021, 22, 12690. [Google Scholar] [CrossRef]
- Velasco, M.A.; Narváez-Tovar, C.A.; Garzón-Alvarado, D.A. Design, materials, and mechanobiology of biodegradable scaffolds for bone tissue engineering. BioMed Res. Int. 2015, 2015, 729076. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Kerns, D.G. Mechanisms of guided bone regeneration: A review. Open Dent. J. 2014, 8, 56–65. [Google Scholar] [CrossRef] [Green Version]
- Nandi, S.K.; Roy, S.; Mukherjee, P.; Kundu, B.; De, D.K.; Basu, D. Orthopaedic applications of bone graft & graft substitutes: A review. Indian J. Med. Res. 2010, 132, 15–30. [Google Scholar]
- Alam, S.; Ueki, K.; Marukawa, K.; Ohara, T.; Hase, T.; Takazakura, D.; Nakagawa, K. Expression of bone morphogenetic protein 2 and fibroblast growth factor 2 during bone regeneration using different implant materials as an onlay bone graft in rabbit mandibles. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2007, 103, 16–26. [Google Scholar] [CrossRef] [Green Version]
- Sheikh, Z.; Hamdan, N.; Ikeda, Y.; Grynpas, M.; Ganss, B.; Glogauer, M. Natural graft tissues and synthetic biomaterials for periodontal and alveolar bone reconstructive applications: A review. Biomater. Res. 2017, 21, 9. [Google Scholar] [CrossRef] [Green Version]
- Elgali, I.; Omar, O.; Dahlin, C.; Thomsen, P. Guided bone regeneration: Materials and biological mechanisms revisited. Eur. J. Oral Sci. 2017, 125, 315–337. [Google Scholar] [CrossRef] [Green Version]
- Boyce, T.; Edwards, J.; Scarborough, N. ALLOGRAFT BONE: The influence of processing on safety and performance. Orthop. Clin. N. Am. 1999, 30, 571–581. [Google Scholar] [CrossRef]
- Zhang, L.; Mu, W.; Chen, S.; Yang, D.; Xu, F.; Wu, Y. The enhancement of osteogenic capacity in a synthetic BMP-2 derived peptide coated mineralized collagen composite in the treatment of the mandibular defects. Biomed. Mater. Eng. 2016, 27, 495–505. [Google Scholar] [CrossRef]
- Guo, J.; Meng, Z.; Chen, G.; Xie, D.; Chen, Y.; Wang, H.; Tang, W.; Liu, L.; Jing, W.; Long, J.; et al. Restoration of critical-size defects in the rabbit mandible using porous nanohydroxyapatite-polyamide scaffolds. Tissue Eng. Part A 2012, 18, 1239–1252. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liu, S.; Fu, Y.; Chang, D.T.; Zhou, Y.H. Mineralised Collagen Scaffolds Loaded with Stromal Cell-derived Factor-1 Improve Mandibular Bone Regeneration. Chin. J. Dent. Res. 2014, 17, 23–29. [Google Scholar] [PubMed]
- Su, J.; Xu, H.; Sun, J.; Gong, X.; Zhao, H. Dual delivery of BMP-2 and bFGF from a new nano-composite scaffold, loaded with vascular stents for large-size mandibular defect regeneration. Int. J. Mol. Sci. 2013, 14, 12714–12728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez-Quintero, J.G.; Durán Riveros, J.Y.; Martínez Valbuena, C.A.; Pedraza Alonso, S.; Munévar, J.C.; Viafara-García, S.M. Critical-sized mandibular defect reconstruction using human dental pulp stem cells in a xenograft model-clinical, radiological, and histological evaluation. Oral Maxillofac. Surg. 2020, 24, 485–493. [Google Scholar] [CrossRef]
- Liu, X.; Zhao, K.; Gong, T.; Song, J.; Bao, C.; Luo, E.; Weng, J.; Zhou, S. Delivery of growth factors using a smart porous nanocomposite scaffold to repair a mandibular bone defect. Biomacromolecules 2014, 15, 1019–1030. [Google Scholar] [CrossRef]
- Li, J.; Li, Y.; Ma, S.; Gao, Y.; Zuo, Y.; Hu, J. Enhancement of bone formation by BMP-7 transduced MSCs on biomimetic nano-hydroxyapatite/polyamide composite scaffolds in repair of mandibular defects. J. Biomed. Mater. Res. A 2010, 95, 973–981. [Google Scholar] [CrossRef]
- Jiang, X.; Gittens, S.A.; Chang, Q.; Zhang, X.; Chen, C.; Zhang, Z. The use of tissue-engineered bone with human bone morphogenetic protein-4-modified bone-marrow stromal cells in repairing mandibular defects in rabbits. Int. J. Oral Maxillofac. Surg. 2006, 35, 1133–1139. [Google Scholar] [CrossRef]
- Zhao, J.; Hu, J.; Wang, S.; Sun, X.; Xia, L.; Zhang, X.; Zhang, Z.; Jiang, X. Combination of beta-TCP and BMP-2 gene-modified bMSCs to heal critical size mandibular defects in rats. Oral Dis. 2010, 16, 46–54. [Google Scholar] [CrossRef]
- Wu, W.; Chen, X.; Mao, T.; Chen, F.; Feng, X. Bone marrow-derived osteoblasts seeded into porous beta-tricalcium phosphate to repair segmental defect in canine’s mandibula. Ulus Travma Acil Cerrahi Derg 2006, 12, 268–276. [Google Scholar] [PubMed]
- Liu, X.; Liu, H.Y.; Lian, X.; Shi, X.L.; Wang, W.; Cui, F.Z.; Zhang, Y. Osteogenesis of mineralized collagen bone graft modified by PLA and calcium sulfate hemihydrate: In vivo study. J. Biomater. Appl. 2013, 28, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wu, X.; Xing, H.; Zhang, G.; Shi, Q.; E, L.; Liu, N.; Yang, T.; Wang, D.; Qi, F.; et al. Porous Nanohydroxyapatite/Collagen Scaffolds Loading Insulin PLGA Particles for Restoration of Critical Size Bone Defect. ACS Appl. Bio. Mater. 2017, 9, 11380–11391. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Lu, C.; Chen, B.; Han, J.; Zhao, Y.; Xiao, Z.; Han, S.; Pan, J.; Dai, J. Restoration of mandibular bone defects with demineralized bone matrix combined with three-dimensional cultured bone marrow-derived mesenchymal stem cells in minipig models. J. Mater. Sci. Mater. Med. 2018, 29, 147. [Google Scholar] [CrossRef]
- Probst, F.A.; Fliefel, R.; Burian, E.; Probst, M.; Eddicks, M.; Cornelsen, M.; Riedl, C.; Seitz, H.; Aszódi, A.; Schieker, M.; et al. Bone regeneration of minipig mandibular defect by adipose derived mesenchymal stem cells seeded tri-calcium phosphate-poly(D,L-lactide-co-glycolide) scaffolds. Sci. Rep. 2020, 10, 2062. [Google Scholar] [CrossRef] [Green Version]
- Stevanovic, M.; Selakovic, D.; Vasovic, M.; Ljujic, B.; Zivanovic, S.; Papic, M.; Zivanovic, M.; Milivojevic, N.; Mijovic, M.; Tabakovic, S.Z.; et al. Comparison of Hydroxyapatite/Poly(lactide-co-glycolide) and Hydroxyapatite/Polyethyleneimine Composite Scaffolds in Bone Regeneration of pigs Mandibular Critical Size Defects: In Vivo Study. Molecules 2022, 27, 1694. [Google Scholar] [CrossRef]
- He, Y.; Zhang, Z.Y.; Zhu, H.G.; Qiu, W.; Jiang, X.; Guo, W. Experimental study on reconstruction of segmental mandible defects using tissue engineered bone combined bone marrow stromal cells with three-dimensional tricalcium phosphate. J. Craniofac Surg. 2007, 18, 800–805. [Google Scholar] [CrossRef]
- Yuan, J.; Cui, L.; Zhang, W.J.; Liu, W.; Cao, Y. Repair of canine mandibular bone defects with bone marrow stromal cells and porous beta-tricalcium phosphate. Biomaterials 2007, 28, 1005–1013. [Google Scholar] [CrossRef]
- Tateno, A.; Asano, M.; Akita, D.; Toriumi, T.; Tsurumachi-Iwasaki, N.; Kazama, T.; Arai, Y.; Matsumoto, T.; Kano, K.; Honda, M. Transplantation of dedifferentiated fat cells combined with a biodegradable type I collagen-recombinant peptide scaffold for critical-size bone defects in rats. J. Oral Sci. 2019, 61, 534–538. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.K.; DeConde, A.S.; Lee, M.; Walthers, C.M.; Sepahdari, A.R.; Elashoff, D.; Grogan, T.; Bezouglaia, O.; Tetradis, S.; St John, M.; et al. Biomimetic scaffolds facilitate healing of critical-sized segmental mandibular defects. Am. J. Otolaryngol. 2015, 36, 1–6. [Google Scholar] [CrossRef]
- Fan, J.; Guo, M.; Im, C.S.; Pi-Anfruns, J.; Cui, Z.K.; Kim, S.; Wu, B.M.; Aghaloo, T.L.; Lee, M. Enhanced Mandibular Bone Repair by Combined Treatment of Bone Morphogenetic Protein 2 and Small-Molecule Phenamil. Tissue Eng. Part A. 2017, 23, 195–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mankani, M.H.; Kuznetsov, S.A.; Wolfe, R.M.; Marshall, G.W.; Robey, P.G. In vivo bone formation by human bone marrow stromal cells: Reconstruction of the mouse calvarium and mandible. Stem. Cells 2006, 24, 2140–2149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tee, B.C.; Desai, K.G.; Kennedy, K.S.; Sonnichsen, B.; Kim, D.G.; Fields, H.W.; Mallery, S.R.; Schwendeman, S.P.; Sun, Z. Reconstructing jaw defects with MSCs and PLGA-encapsulated growth factors. Am. J. Transl. Res. 2016, 8, 2693–2704. [Google Scholar]
- Lopez, C.D.; Diaz-Siso, J.R.; Witek, L.; Bekisz, J.M.; Cronstein, B.N.; Torroni, A.; Flores, R.L.; Rodriguez, E.D.; Coelho, P.G. Three dimensionally printed bioactive ceramic scaffold osseoconduction across critical-sized mandibular defects. J. Surg. Res. 2018, 223, 115–122. [Google Scholar] [CrossRef] [Green Version]
- Herford, A.S.; Lu, M.; Buxton, A.N.; Kim, J.; Henkin, J.; Boyne, P.J.; Caruso, J.M.; Rungcharassaeng, K.; Hong, J. Recombinant human bone morphogenetic protein 2 combined with an osteoconductive bulking agent for mandibular continuity defects in nonhuman primates. J. Oral Maxillofac. Surg. 2012, 70, 703–716. [Google Scholar] [CrossRef]
- Toriumi, D.M.; O’Grady, K.; Horlbeck, D.M.; Desai, D.; Turek, T.J.; Wozney, J. Mandibular reconstruction using bone morphogenetic protein 2: Long-term follow-up in a canine model. Laryngoscope 1999, 109, 1481–1489. [Google Scholar] [CrossRef]
- Witek, L.; Tian, H.; Tovar, N.; Torroni, A.; Neiva, R.; Gil, L.F.; Coelho, P.G. The effect of platelet-rich fibrin exudate addition to porous poly(lactic-co-glycolic acid) scaffold in bone healing: An in vivo study. J. Biomed. Mater. Res. B Appl. Biomater. 2020, 108, 1304–1310. [Google Scholar] [CrossRef]
- Konopnicki, S.; Sharaf, B.; Resnick, C.; Patenaude, A.; Pogal-Sussman, T.; Hwang, K.G.; Abukawa, H.; Troulis, M.J. Tissue-engineered bone with 3-dimensionally printed β-tricalcium phosphate and polycaprolactone scaffolds and early implantation: An in vivo pilot study in a porcine mandible model. J. Oral Maxillofac. Surg. 2015, 73, 1016.e1–1016.e11. [Google Scholar] [CrossRef]
- Fan, J.; Park, H.; Lee, M.K.; Bezouglaia, O.; Fartash, A.; Kim, J.; Aghaloo, T.; Lee, M. Adipose-derived stem cells and BMP-2 delivery in chitosan-based 3D constructs to enhance bone regeneration in a rat mandibular defect model. Tissue Eng. Part A 2014, 20, 2169–2179. [Google Scholar] [CrossRef] [Green Version]
- Das, A.; Fishero, B.A.; Christophel, J.J.; Li, C.J.; Kohli, N.; Lin, Y.; Dighe, A.S.; Cui, Q. Poly(lactic-co-glycolide) polymer constructs cross-linked with human BMP-6 and VEGF protein significantly enhance rat mandible defect repair. Cell Tissue Res. 2016, 364, 125–135. [Google Scholar] [CrossRef]
- DeConde, A.S.; Sidell, D.; Lee, M.; Bezouglaia, O.; Low, K.; Elashoff, D.; Grogan, T.; Tetradis, S.; Aghaloo, T.; St John, M. Bone morphogenetic protein-2-impregnated biomimetic scaffolds successfully induce bone healing in a marginal mandibular defect. Laryngoscope 2013, 123, 1149–1155. [Google Scholar] [CrossRef] [Green Version]
- Arosarena, O.; Collins, W. Comparison of BMP-2 and -4 for rat mandibular bone regeneration at various doses. Orthod. Craniofac. Res. 2005, 8, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Arosarena, O.A.; Collins, W.L. Bone regeneration in the rat mandible with bone morphogenetic protein-2: A comparison of two carriers. Otolaryngol. Head Neck Surg. 2005, 132, 592–597. [Google Scholar] [CrossRef]
- Arosarena, O.A.; Falk, A.; Malmgren, L.; Bookman, L.; Allen, M.J.; Schoonmaker, J.; Tatum, S.; Kellman, R. Defect repair in the rat mandible with bone morphogenic proteins and marrow cells. Arch. Facial Plast. Surg. 2003, 5, 103–108. [Google Scholar] [CrossRef]
- Boyne, P.J.; Salina, S.; Nakamura, A.; Audia, F.; Shabahang, S. Bone regeneration using rhBMP-2 induction in hemimandibulectomy type defects of elderly sub-human primates. Cell Tissue Bank. 2006, 7, 1–10. [Google Scholar] [CrossRef]
- Lohse, N.; Moser, N.; Backhaus, S.; Annen, T.; Epple, M.; Schliephake, H. Continuous delivery of rhBMP2 and rhVEGF165 at a certain ratio enhances bone formation in mandibular defects over the delivery of rhBMP2 alone--An experimental study in rats. J. Control. Release 2015, 220, 201–209. [Google Scholar] [CrossRef]
- Moser, N.; Lohse, N.; Golstein, J.; Kauffmann, P.; Sven, B.; Epple, M.; Schliephake, H. Do we need retarded delivery of bone growth factors in facial bone repair? An experimental study in rats. Eur. Cells Mater. 2017, 34, 162–179. [Google Scholar] [CrossRef]
- Springer, I.N.; Niehoff, P.; Açil, Y.; Marget, M.; Lange, A.; Warnke, P.H.; Pielenz, H.; Roldán, J.C.; Wiltfang, J. BMP-2 and bFGF in an irradiated bone model. J. Craniomaxillofac. Surg. 2008, 36, 210–217. [Google Scholar] [CrossRef]
- Yahia, S.; Khalil, I.A.; El-Sherbiny, I.M. Sandwich-Like Nanofibrous Scaffolds for Bone Tissue Regeneration. ACS Appl. Mater. Interfaces 2019, 11, 28610–28620. [Google Scholar] [CrossRef]
- Schliephake, H.; Weich, H.A.; Dullin, C.; Gruber, R.; Frahse, S. Mandibular bone repair by implantation of rhBMP-2 in a slow release carrier of polylactic acid--an experimental study in rats. Biomaterials 2008, 29, 103–110. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Ries, J.; Gelse, K.; Kloss, F.; von der Mark, K.; Wiltfang, J.; Neukam, F.W.; Schneider, H. Bone regeneration in critical size defects by cell-mediated BMP-2 gene transfer: A comparison of adenoviral vectors and liposomes. Gene Ther. 2003, 10, 1089–1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Streckbein, P.; Jäckel, S.; Malik, C.Y.; Obert, M.; Kähling, C.; Wilbrand, J.F.; Zahner, D.; Heidinger, K.; Kampschulte, M.; Pons-Kühnemann, J.; et al. Reconstruction of critical-size mandibular defects in immunoincompetent rats with human adipose-derived stromal cells. J. Craniomaxillofac. Surg. 2013, 41, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Springer, I.N.; Schildberg, H.; Acil, Y.; Ludwig, K.; Rueger, D.R.; Terheyden, H. Carboxymethylcellulose-stabilized collagenous rhOP-1 device-a novel carrier biomaterial for the repair of mandibular continuity defects. J. Biomed. Mater. Res. Part A 2004, 68, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Schliephake, H.; Knebel, J.W.; Aufderheide, M.; Tauscher, M. Use of cultivated osteoprogenitor cells to increase bone formation in segmental mandibular defects: An experimental pilot study in sheep. Int. J. Oral Maxillofac. Surg. 2001, 30, 531–537. [Google Scholar] [CrossRef]
- Ozaki, M.; Takayama, T.; Yamamoto, T.; Ozawa, Y.; Nagao, M.; Tanabe, N.; Nakajima, A.; Suzuki, N.; Maeno, M.; Yamano, S.; et al. A collagen membrane containing osteogenic protein-1 facilitates bone regeneration in a rat mandibular bone defect. Arch. Oral Biol. 2017, 84, 19–28. [Google Scholar] [CrossRef]
- Marukawa, E.; Asahina, I.; Oda, M.; Seto, I.; Alam, M.; Enomoto, S. Functional reconstruction of the non-human primate mandible using recombinant human bone morphogenetic protein-2. Int. J. Oral Maxillofac. Surg. 2002, 31, 287–295. [Google Scholar] [CrossRef]
- Yamada, Y.; Ueda, M.; Naiki, T.; Takahashi, M.; Hata, K.; Nagasaka, T. Autogenous injectable bone for regeneration with mesenchymal stem cells and platelet-rich plasma: Tissue-engineered bone regeneration. Tissue Eng. 2004, 10, 955–964. [Google Scholar] [CrossRef]
- Seto, I.; Marukawa, E.; Asahina, I. Mandibular reconstruction using a combination graft of rhBMP-2 with bone marrow cells expanded in vitro. Plast. Reconstr. Surg. 2006, 117, 902–908. [Google Scholar] [CrossRef]
- Lopez, C.D.; Diaz-Siso, J.R.; Witek, L.; Bekisz, J.M.; Gil, L.F.; Cronstein, B.N.; Flores, R.L.; Torroni, A.; Rodriguez, E.D.; Coelho, P.G. Dipyridamole Augments Three-Dimensionally Printed Bioactive Ceramic Scaffolds to Regenerate Craniofacial Bone. Plast. Reconstr. Surg. 2019, 143, 1408–1419. [Google Scholar] [CrossRef]
- Seto, I.; Asahina, I.; Oda, M.; Enomoto, S. Reconstruction of the primate mandible with a combination graft of recombinant human bone morphogenetic protein-2 and bone marrow. J. Oral Maxillofac. Surg. 2001, 59, 53–63. [Google Scholar] [CrossRef]
- Alfotawei, R.; Naudi, K.B.; Lappin, D.; Barbenel, J.; Di Silvio, L.; Hunter, K.; McMahon, J.; Ayoub, A. The use of TriCalcium Phosphate (TCP) and stem cells for the regeneration of osteoperiosteal critical-size mandibular bony defects, an in vitro and preclinical study. J. Craniomaxillofac. Surg. 2014, 42, 863–869. [Google Scholar] [CrossRef]
- Abu-Serriah, M.M.; Odell, E.; Lock, C.; Gillar, A.; Ayoub, A.F.; Fleming, R.H. Histological assessment of bioengineered new bone in repairing osteoperiosteal mandibular defects in sheep using recombinant human bone morphogenetic protein-7. Br. J. Oral Maxillofac. Surg. 2004, 42, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Abu-Serriah, M.; Kontaxis, A.; Ayoub, A.; Harrison, J.; Odell, E.; Barbenel, J. Mechanical evaluation of mandibular defects reconstructed using osteogenic protein-1 (rhOP-1) in a sheep model: A critical analysis. Int. J. Oral Maxillofac. Surg. 2005, 34, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Kontaxis, A.; Abu-Serriah, M.; Ayoub, A.F.; Barbenel, J.C. Mechanical testing of recombinant human bone morphogenetic protein-7 regenerated bone in sheep mandibles. Proc. Inst. Mech. Eng. H 2004, 218, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Busuttil Naudi, K.; Ayoub, A.; McMahon, J.; Di Silvio, L.; Lappin, D.; Hunter, K.D.; Barbenel, J. Mandibular reconstruction in the rabbit using beta-tricalcium phosphate (β-TCP) scaffolding and recombinant bone morphogenetic protein 7 (rhBMP-7)—Histological, radiographic and mechanical evaluations. J. Craniomaxillofac. Surg. 2012, 40, e461–e469. [Google Scholar] [CrossRef]
- Deng, N.; Sun, J.; Li, Y.; Chen, L.; Chen, C.; Wu, Y.; Wang, Z.; Li, L. Experimental study of rhBMP-2 chitosan nano-sustained release carrier-loaded PLGA/nHA scaffolds to construct mandibular tissue-engineered bone. Arch. Oral Biol. 2019, 102, 16–25. [Google Scholar] [CrossRef]
- Jin, I.G.; Kim, J.H.; Wu, H.G.; Kim, S.K.; Park, Y.; Hwang, S.J. Effect of bone marrow-derived stem cells and bone morphogenetic protein-2 on treatment of osteoradionecrosis in a rat model. J. Craniomaxillofac. Surg. 2015, 43, 1478–1486. [Google Scholar] [CrossRef]
- Yun, P.Y.; Kim, Y.K.; Jeong, K.I.; Park, J.C.; Choi, Y.J. Influence of bone morphogenetic protein and proportion of hydroxyapatite on new bone formation in biphasic calcium phosphate graft: Two pilot studies in animal bony defect model. J. Craniomaxillofac. Surg. 2014, 42, 1909–1917. [Google Scholar] [CrossRef]
- Kim, J.; Yang, H.J.; Cho, T.H.; Lee, S.E.; Park, Y.D.; Kim, H.M.; Kim, I.S.; Seo, Y.K.; Hwang, S.J.; Kim, S.J. Enhanced regeneration of rabbit mandibular defects through a combined treatment of electrical stimulation and rhBMP-2 application. Med. Biol. Eng. Comput. 2013, 51, 1339–1348. [Google Scholar] [CrossRef]
- Poudel, S.B.; Bhattarai, G.; Kim, J.H.; Kook, S.H.; Seo, Y.K.; Jeon, Y.M.; Lee, J.C. Local delivery of recombinant human FGF7 enhances bone formation in rat mandible defects. J. Bone Miner. Metab. 2017, 35, 485–496. [Google Scholar] [CrossRef]
- Behnia, A.; Haghighat, A.; Talebi, A.; Nourbakhsh, N.; Heidari, F. Transplantation of stem cells from human exfoliated deciduous teeth for bone regeneration in the dog mandibular defect. World J. Stem. Cells 2014, 6, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Khojasteh, A.; Behnia, H.; Hosseini, F.S.; Dehghan, M.M.; Abbasnia, P.; Abbas, F.M. The effect of PCL-TCP scaffold loaded with mesenchymal stem cells on vertical bone augmentation in dog mandible: A preliminary report. J. Biomed. Mater. Res. B Appl. Biomater. 2013, 101, 848–854. [Google Scholar] [CrossRef]
- Gallego, L.; Junquera, L.; García, E.; García, V.; Alvarez-Viejo, M.; Costilla, S.; Fresno, M.F.; Meana, A. Repair of rat mandibular bone defects by alveolar osteoblasts in a novel plasma-derived albumin scaffold. Tissue Eng. Part A 2010, 16, 1179–1187. [Google Scholar] [CrossRef] [Green Version]
- Gallego, L.; Pérez-Basterrechea, M.; García-Consuegra, L.; Álvarez-Viejo, M.; Megías, J.; Novoa, A.; Costilla, S.; Meana, Á.; Junquera, L. Repair of segmental mandibular bone defects in sheep using bone marrow stromal cells and autologous serum scaffold: A pilot study. J. Clin. Periodontol. 2015, 42, 1143–1151. [Google Scholar] [CrossRef]
- Park, J.H.; Jung, S.Y.; Lee, C.K.; Ban, M.J.; Lee, S.J.; Kim, H.Y.; Oh, H.J.; Kim, B.K.; Park, H.S.; Jang, S.H.; et al. A 3D-printed polycaprolactone/β-tricalcium phosphate mandibular prosthesis: A pilot animal study. Laryngoscope 2020, 130, 358–366. [Google Scholar] [CrossRef]
- Li, X.; Song, T.; Chen, X.; Wang, M.; Yang, X.; Xiao, Y.; Zhang, X. Osteoinductivity of Porous Biphasic Calcium Phosphate Ceramic Spheres with Nanocrystalline and Their Efficacy in Guiding Bone Regeneration. ACS Appl. Mater. Interfaces 2019, 11, 3722–3736. [Google Scholar] [CrossRef]
- Issa, J.P.; do Nascimento, C.; Bentley, M.V.; Del Bel, E.A.; Iyomasa, M.M.; Sebald, W.; de Albuquerque, R.F., Jr. Bone repair in rat mandible by rhBMP-2 associated with two carriers. Micron 2008, 39, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Hussein, K.A.; Zakhary, I.E.; Elawady, A.R.; Emam, H.A.; Sharawy, M.; Baban, B.; Akeel, S.; Al-Shabrawey, M.; Elsalanty, M.E. Difference in soft tissue response between immediate and delayed delivery suggests a new mechanism for recombinant human bone morphogenetic protein 2 action in large segmental bone defects. Tissue Eng. Part A 2012, 18, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Ekholm, M.; Hietanen, J.; Tulamo, R.M.; Muhonen, J.; Lindqvist, C.; Kellomäki, M.; Suuronen, R. The copolymer of epsilon-caprolactone-lactide and tricalcium phosphate does not enhance bone growth in mandibular defect of sheep. J. Mater. Sci. Mater. Med. 2006, 17, 139–145. [Google Scholar] [CrossRef]
- Jégoux, F.; Goyenvalle, E.; Cognet, R.; Malard, O.; Moreau, F.; Daculsi, G.; Aguado, E. Mandibular segmental defect regenerated with macroporous biphasic calcium phosphate, collagen membrane, and bone marrow graft in dogs. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 971–978. [Google Scholar] [CrossRef] [Green Version]
- Srouji, S.; Rachmiel, A.; Blumenfeld, I.; Livne, E. Mandibular defect repair by TGF-beta and IGF-1 released from a biodegradable osteoconductive hydrogel. J. Craniomaxillofac. Surg. 2005, 33, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Çakır-Özkan, N.; Eğri, S.; Bekar, E.; Altunkaynak, B.Z.; Kabak, Y.B.; Kıvrak, E.G. The Use of Sequential VEGF- and BMP2-Releasing Biodegradable Scaffolds in Rabbit Mandibular Defects. J. Oral Maxillofac. Surg. 2017, 75, 221.e1–221.e14. [Google Scholar] [CrossRef] [PubMed]
- Carlisle, P.; Guda, T.; Silliman, D.T.; Burdette, A.J.; Talley, A.D.; Alvarez, R.; Tucker, D.; Hale, R.G.; Guelcher, S.A.; BrownBaer, P.R. Localized low-dose rhBMP-2 is effective at promoting bone regeneration in mandibular segmental defects. J. Biomed. Mater. Res. B Appl. Biomater. 2019, 107, 1491–1503. [Google Scholar] [CrossRef] [PubMed]
- Stigler, R.G.; Schimke, M.M.; Bigus, S.; Steinmüller-Nethl, D.; Tillmann, K.; Lepperdinger, G. Pervasion of beta-tricalcium phosphate with nanodiamond particles yields efficient and safe bone replacement material amenable for biofunctionalization and application in large-size osseous defect healing. Nanomed. Nanotechnol. Biol. Med. 2019, 16, 250–257. [Google Scholar] [CrossRef]
- Wang, Y.; Cai, X.; Huang, J.; Zhou, Y.; Jiang, T.; Wang, Y. Bone regeneration in critically sized rat mandible defects through the endochondral pathway using hydroxyapatite-coated 3D-printed Ti6Al4V scaffolds. RSC Adv. 2018, 8, 31745–31754. [Google Scholar] [CrossRef] [Green Version]
- Helal, M.H.; Hendawy, H.D.; Gaber, R.A.; Helal, N.R.; Aboushelib, M.N. Osteogenesis ability of CAD-CAM biodegradable polylactic acid scaffolds for reconstruction of jaw defects. J. Prosthet. Dent. 2019, 121, 118–123. [Google Scholar] [CrossRef]
- Khojasteh, A.; Hosseinpour, S.; Dehghan, M.M.; Mashhadiabbas, F.; Rezai Rad, M.; Ansari, S.; Farzad Mohajeri, S.; Zadeh, H.H. Antibody-Mediated Osseous Regeneration for Bone Tissue Engineering in Canine Segmental Defects. BioMed Res. Int. 2018, 2018, 9508721. [Google Scholar] [CrossRef] [Green Version]
- Nuntanaranont, T.; Promboot, T.; Sutapreyasri, S. Effect of expanded bone marrow-derived osteoprogenitor cells seeded into polycaprolactone/tricalcium phosphate scaffolds in new bone regeneration of rabbit mandibular defects. J. Mater. Sci. Mater. Med. 2018, 29, 24. [Google Scholar] [CrossRef]
- Maglione, M.; Spano, S.; Ruaro, M.E.; Salvador, E.; Zanconati, F.; Tromba, G.; Turco, G. In vivo evaluation of chitosan-glycerol gel scaffolds seeded with stem cells for full-thickness mandibular bone regeneration. J. Oral Sci. 2017, 59, 225–232. [Google Scholar] [CrossRef] [Green Version]
- Song, W.Y.; Liu, G.M.; Li, J.; Luo, Y.G. Bone morphogenetic protein-2 sustained delivery by hydrogels with microspheres repairs rabbit mandibular defects. Tissue Eng. Regen. Med. 2016, 13, 750–761. [Google Scholar] [CrossRef]
- Mao, Y.; Hu, M.; Chen, L.; Chen, X.; Liu, M.; Zhang, M.; Nie, M.; Liu, X. CGF-HLC-I repaired the bone defect repair of the rabbits mandible through tight junction pathway. Front. Bioeng. Biotechnol. 2022, 10, 976499. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Cao, N.; Zhang, Y.; Cao, G.; Hao, C.; Liu, K.; Li, X.; Wang, W. The Ability and Mechanism of nHAC/CGF in Promoting Osteogenesis and Repairing Mandibular Defects. Nanomaterials 2022, 12, 212. [Google Scholar] [CrossRef] [PubMed]
- Cao, S.S.; Li, S.Y.; Geng, Y.M.; Kapat, K.; Liu, S.B.; Perera, F.H.; Li, Q.; Terheyden, H.; Wu, G.; Che, Y.J.; et al. Prefabricated 3D-Printed Tissue-Engineered Bone for Mandibular Reconstruction: A Preclinical Translational Study in Primate. ACS Biomater. Sci. Eng. 2021, 7, 5727–5738. [Google Scholar] [CrossRef]
- Barrientos-Lezcano, F.J.; Redondo-González, L.M.; Alberca-Zeballos, M.; Sánchez-García, A.M.; García-Sancho, J. Mandibular bone regeneration with autologous adipose-derived mesenchymal stem cells and coralline hydroxyapatite: Experimental study in rats. Br. J. Oral Maxillofac. Surg. 2021, 59, 1192–1199. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.Z.; Su, J.S. Restoration of critical defects in the rabbit mandible using osteoblasts and vascular endothelial cells co-cultured with vascular stent-loaded nano-composite scaffolds. J. Mech. Behav. Biomed. Mater. 2021, 124, 104831. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Park, T.H.; Ryu, J.Y.; Kim, D.K.; Oh, E.J.; Kim, H.M.; Shim, J.H.; Yun, W.S.; Huh, J.B.; Moon, S.H.; et al. Osteogenesis of 3D-Printed PCL/TCP/bdECM Scaffold Using Adipose-Derived Stem Cells Aggregates; An Experimental Study in the Canine Mandible. Int. J. Mol. Sci. 2021, 22, 5409. [Google Scholar] [CrossRef]
- Park, S.A.; Lee, H.J.; Kim, S.Y.; Kim, K.S.; Jo, D.W.; Park, S.Y. Three-dimensionally printed polycaprolactone/beta-tricalcium phosphate scaffold was more effective as an rhBMP-2 carrier for new bone formation than polycaprolactone alone. J. Biomed. Mater. Res. A 2021, 109, 840–848. [Google Scholar] [CrossRef]
- Zhang, P.; Hong, Z.; Yu, T.; Chen, X.; Jing, X. In vivo mineralization and osteogenesis of nanocomposite scaffold of poly(lactide-co-glycolide) and hydroxyapatite surface-grafted with poly(L-lactide). Biomaterials 2009, 30, 58–70. [Google Scholar] [CrossRef]
- Terheyden, H.; Warnke, P.; Dunsche, A.; Jepsen, S.; Brenner, W.; Palmie, S.; Toth, C.; Rueger, D.R. Mandibular reconstruction with prefabricated vascularized bone grafts using recombinant human osteogenic protein-1: An experimental study in miniature pigs. Part II: Transplantation. Int. J. Oral Maxillofac. Surg. 2001, 30, 469–478. [Google Scholar] [CrossRef]
- Lynn, A.K.; Yannas, I.V.; Bonfield, W. Antigenicity and immunogenicity of collagen. J. Biomed. Mater. Res. B Appl. Biomater. 2004, 71, 343–354. [Google Scholar] [CrossRef]
- Kim, M.H.; Kim, B.S.; Park, H.; Lee, J.; Park, W.H. Injectable methylcellulose hydrogel containing calcium phosphate nanoparticles for bone regeneration. Int. J. Biol. Macromol. 2018, 109, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Townsend, J.M.; Andrews, B.T.; Feng, Y.; Wang, J.; Nudo, R.J.; Van Kampen, E.; Gehrke, S.H.; Berkland, C.J.; Detamore, M.S. Superior calvarial bone regeneration using pentenoate-functionalized hyaluronic acid hydrogels with devitalized tendon particles. Acta Biomater. 2018, 71, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Zhai, P.; Peng, X. Li, B. Liu, Y.; Sun, H.; Li, X. The application of hyaluronic acid in bone regeneration. Int. J. Biol. Macromol. 2020, 151, 1224–1239. [Google Scholar] [CrossRef] [PubMed]
- Micic, M.; Antonijevic, D.; Milutinovic-Smiljanic, S.; Trisic, D.; Colovic, B.; Kosanovic, D.; Prokic, B.; Vasic, J.; Zivkovic, S.; Milasin, J.; et al. Developing a novel resorptive hydroxyapatite-based bone substitute for over-critical size defect reconstruction: Physicochemical and biological characterization and proof of concept in segmental rabbit’s ulna reconstruction. Biomedizinische Technik. Biomed. Eng. 2020, 65, 491–505. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Zhu, T.; Li, J.; Cui, L.; Zhang, Z.; Zhuang, X.; Ding, J. Poly(lactic-co-glycolic acid)-based composite bone-substitute materials. Bioact. Mater. 2020, 6, 346–360. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.G.; Zeng, Y.T.; Kankala, R.K.; Zhang, S.S.; Chen, A.Z.; Wang, S.B. Characterization and Preliminary Biological Evaluation of 3D-Printed Porous Scaffolds for Engineering Bone Tissues. Materials 2018, 11, 1832. [Google Scholar] [CrossRef] [Green Version]
- Dong, X.P.; Zhang, Y.W.; Pei, Y.J.; Wang, Z.; Zhang, X.X.; Yu, X.L.; Ai, Z.Z.; Mei, Y.X.; Li, J.N. Three-dimensional printing for the accurate orthopedics: Clinical cases analysis. Bio-Des. Manuf. 2022, 3, 122–132. [Google Scholar] [CrossRef]
- Liang, X.; Qi, Y.; Pan, Z.; He, Y.; Liu, X.; Cui, S.; Ding, J. Design and preparation of quasi-spherical salt particles as water-soluble porogens to fabricate hydrophobic porous scaffolds for tissue engineering and tissue regeneration. Mater. Chem. Front. 2018, 8, 1539–1553. [Google Scholar] [CrossRef]
- Lee, H.; Yoo, J.J.; Kang, H.W.; Cho, D.W. Investigation of thermal degradation with extrusion-based dispensing modules for 3D bioprinting technology. Biofabrication 2016, 8, 015011. [Google Scholar] [CrossRef]
- Yu, Y.; Sun, B.; Yi, C.; Mo, X. Stem cell homing-based tissue engineering using bioactive materials. Front. Mater. Sci. 2017, 11, 93–105. [Google Scholar] [CrossRef]
- Batool, F.; Strub, M.; Petit, C.; Bugueno, I.M.; Bornert, F.; Clauss, F.; Huck, O.; Kuchler-Bopp, S.; Benkirane-Jessel, N. Periodontal Tissues, Maxillary Jaw Bone, and Tooth Regeneration Approaches: From Animal Models Analyses to Clinical Applications. Nanomaterials 2018, 8, 337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Ye, X.; Wang, H.; Zhu, M.; Wang, B.; Yan, H. The influence of pH and temperature on the morphology of hydroxyapatite synthesized by hydrothermal method. Ceram. Int. 2003, 29, 629–633. [Google Scholar] [CrossRef]
- Rodríguez-Lugo, V.; Hernández, J.S.; Arellano-Jimenez, M.J.; Hernández-Tejeda, P.H.; Recillas-Gispert, S. Characterization of hydroxyapatite by electron microscopy. Microsc. Microanal. 2005, 11, 516–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jokanovic, V.; Jokanovic, B.; Markovic, D.; Zivojinovic, V.; Pasalic, S.; Izvonar, D.; Plavsic, M. Kinetics and sintering mechanisms of hydro-thermally obtained hydroxyapatite. Mater. Chem. Phys. 2008, 111, 180–185. [Google Scholar] [CrossRef]
- Ungureanu, D.N.; Angelescu, N.; Bacinschi, Z.; Stoian, E.V.; Rizescu, C.Z. Thermal stability of chemically precipitated hydroxyapatite nanopowders. Int. J. Biol. Biomed. Eng. 2011, 5, 57–64. [Google Scholar]
- Bodhak, S.; Bose, S.; Bandyopadhyay, A. Electrically polarized HAp-coated Ti: In vitro bone cell-material interactions. Acta Biomater. 2010, 6, 641–651. [Google Scholar] [CrossRef]
- Zhang, B.G.; Myers, D.E.; Wallace, G.G.; Brandt, M.; Choong, P.F. Bioactive coatings for orthopaedic implants-recent trends in development of implant coatings. Int. J. Mol. Sci. 2014, 15, 11878–11921. [Google Scholar] [CrossRef] [Green Version]
- Fitzpatrick, V.; Martín-Moldes, Z.; Deck, A.; Torres-Sanchez, R.; Valat, A.; Cairns, D.; Li, C.; Kaplan, D.L. Functionalized 3D-printed silk-hydroxyapatite scaffolds for enhanced bone regeneration with innervation and vascularization. Biomaterial. 2021, 276, 120995. [Google Scholar] [CrossRef]
- Jokanović, V.; Čolović, B.; Marković, D.; Petrović, M.; Jokanović, M.; Milosavljević, P.; Sopta, J. In Vivo investigation of ALBO-OS scaffold based on hydroxyapatite and PLGA. J. Nanomater. 2016, 2016, 3948768. [Google Scholar] [CrossRef] [Green Version]
- Furtos, G.; Rivero, G.; Rapuntean, S.; Abraham, G.A. Amoxicillin-loaded electrospun nanocomposite membranes for dental applications. J. Biomed. Mater. Res. B Appl. Biomater. 2017, 105, 966–976. [Google Scholar] [CrossRef]
- Xia, D.; Yang, F.; Zheng, Y.; Liu, Y.; Zhou, Y. Research status of biodegradable metals designed for oral and maxillofacial applications: A review. Bioact. Mater. 2021, 6, 4186–4208. [Google Scholar] [CrossRef] [PubMed]
- Hang, R.; Wang, C.; Yu, Z.; Li, Z.; Xiao, Y. Biodegradable metallic wires in dental and orthopedic applications: A review. Materials 2018, 8, 212. [Google Scholar] [CrossRef] [Green Version]
- Rider, P.; Kačarević, Ž.P.; Elad, A.; Rothamel, D.; Sauer, G.; Bornert, F.; Windisch, P.; Hangyási, D.; Molnar, B.; Hesse, B.; et al. Biodegradation of a Magnesium Alloy Fixation Screw Used in a Guided Bone Regeneration Model in Beagle Dogs. Materials 2022, 15, 4111. [Google Scholar] [CrossRef] [PubMed]
- Muschler, G.F.; Raut, V.P.; Patterson, T.E.; Wenke, J.C.; Hollinger, J.O. The design and use of animal models for translational research in bone tissue engineering and regenerative medicine. Tissue Eng. Part B Rev. 2010, 16, 123–145. [Google Scholar] [CrossRef] [Green Version]
- Boden, S.D.; Grob, D.; Damien, C. Ne-Osteo bone growth factor for posterolateral lumbar spine fusion: Results from a nonhuman primate study and a prospective human clinical pilot study. Spine 2004, 29, 504–514. [Google Scholar] [CrossRef]
- Chanchareonsook, N.; Junker, R.; Jongpaiboonkit, L.; Jansen, J.A. Tissue-engineered mandibular bone reconstruction for continuity defects: A systematic approach to the literature. Tissue Eng. Part B Rev. 2014, 20, 147–162. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.S.; Lee, E.N.; Cho, T.H.; Song, Y.M.; Hwang, S.J.; Oh, J.H.; Park, E.K.; Koo, T.Y.; Seo, Y.K. Promising efficacy of Escherichia coli recombinant human bone morphogenetic protein-2 in collagen sponge for ectopic and orthotopic bone formation and comparison with mammalian cell recombinant human bone morphogenetic protein-2. Tissue Eng. Part A 2011, 17, 337–348. [Google Scholar] [CrossRef]
- Moghadam, H.G.; Urist, M.R.; Sandor, G.K.; Clokie, C.M. Successful mandibular reconstruction using a BMP bioimplant. J. Craniofacial Surg. 2001, 12, 119–128. [Google Scholar] [CrossRef]
- Warnke, P.H.; Springer, I.N.; Wiltfang, J.; Acil, Y.; Eufinger, H.; Wehmöller, M.; Russo, P.A.; Bolte, H.; Sherry, E.; Behrens, E.; et al. Growth and transplantation of a custom vascularised bone graft in a man. Lancet 2004, 364, 766–770. [Google Scholar] [CrossRef]
- Heliotis, M.; Lavery, K.M.; Ripamonti, U.; Tsiridis, E.; di Silvio, L. Transformation of a prefabricated hydroxyapatite/osteogenic protein-1 implant into a vascularised pedicled bone flap in the human chest. Int. J. Oral Maxillofac. Surg. 2006, 35, 265–269. [Google Scholar] [CrossRef]
- Herford, A.S.; Boyne, P.J. Reconstruction of mandibular continuity defects with bone morphogenetic protein-2 (rhBMP-2). J. Oral Maxillofac. Surg. 2008, 66, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Chao, M.; Donovan, T.; Sotelo, C.; Carstens, M.H. In situ osteogenesis of hemimandible with rhBMP-2 in a 9-year-old boy: Osteoinduction via stem cell concentration. J. Craniofac. Surg. 2006, 17, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Clokie, C.M.; Sándor, G.K. Reconstruction of 10 major mandibular defects using bioimplants containing BMP-7. J. Can. Dent. Assoc. 2008, 74, 67–72. [Google Scholar]
- Glied, A.N.; Kraut, R.A. Off-label use of rhBMP-2 for reconstruction of critical-sized mandibular defects. N. Y. State Dent. J. 2010, 76, 32–35. [Google Scholar]
- Herford, A.S.; Cicciù, M. Recombinant human bone morphogenetic protein type 2 jaw reconstruction in patients affected by giant cell tumor. J. Craniofac. Surg. 2010, 21, 1970–1975. [Google Scholar] [CrossRef]
- Scadden, D.T. The stem-cell niche as an entity of action. Nature 2006, 441, 1075–1079. [Google Scholar] [CrossRef]
- Monaco, E.; Bionaz, M.; Hollister, S.J.; Wheeler, M.B. Strategies for regeneration of the bone using porcine adult adipose-derived mesenchymal stem cells. Theriogenology 2011, 75, 1381–1399. [Google Scholar] [CrossRef] [PubMed]
- Sándor, G.K.; Tuovinen, V.J.; Wolff, J.; Patrikoski, M.; Jokinen, J.; Nieminen, E.; Mannerström, B.; Lappalainen, O.P.; Seppänen, R.; Miettinen, S. Adipose stem cell tissue-engineered construct used to treat large anterior mandibular defect: A case report and review of the clinical application of good manufacturing practice-level adipose stem cells for bone regeneration. J. Oral Maxillofac. Surg. 2013, 71, 938–950. [Google Scholar] [CrossRef]
- Aerssens, J.; Boonen, S.; Lowet, G.; Dequeker, J. Interspecies differences in bone composition, density, and quality: Potential implications for in vivo bone research. Endocrinology 1998, 139, 663–670. [Google Scholar] [CrossRef]
- Gilsanz, V.; Roe, T.F.; Gibbens, D.T.; Schulz, E.E.; Carlson, M.E.; Gonzalez, O.; Boechat, M.I. Effect of sex steroids on peak bone density of growing rabbits. Am. J. Physiol. 1988, 255, E416–E421. [Google Scholar] [CrossRef]
- Castañeda, S.; Largo, R.; Calvo, E.; Rodríguez-Salvanés, F.; Marcos, M.E.; Díaz-Curiel, M.; Herrero-Beaumont, G. Bone mineral measurements of subchondral and trabecular bone in healthy and osteoporotic rabbits. Skelet. Radiol. 2006, 35, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Wancket, L.M. Animal Models for Evaluation of Bone Implants and Devices: Comparative Bone Structure and Common Model Uses. Vet. Pathol. 2015, 52, 842–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reitan, K.; Kvam, E. Comparative behavior of human and animal tissue during experimental tooth movement. Angle Orthod. 1971, 41, 1–14. [Google Scholar] [CrossRef]
- Harper, R.A.; Pfeiffer, F.M.; Choma, T.J. The minipig as a potential model for pedicle screw fixation: Morphometry and mechanics. J. Orthop. Surg. Res. 2019, 14, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schorn, L.; Sproll, C.; Ommerborn, M.; Naujoks, C.; Kübler, N.R.; Depprich, R. Vertical bone regeneration using rhBMP-2 and VEGF. Head Face Med. 2017, 13, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jinno, Y.; Jimbo, R.; Lindström, M.; Sawase, T.; Lilin, T.; Becktor, J.P. Vertical Bone Augmentation Using Ring Technique with Three Different Materials in the Sheep Mandible Bone. Int. J. Oral Maxillofac. Implants 2018, 33, 1057–1063. [Google Scholar] [CrossRef] [PubMed]
- Carrel, J.P.; Wiskott, A.; Moussa, M.; Rieder, P.; Scherrer, S.; Durual, S. A 3D printed TCP/HA structure as a new osteoconductive scaffold for vertical bone augmentation. Clin. Oral Implants. Res. 2016, 27, 55–62. [Google Scholar] [CrossRef]
- Triplett, R.G.; Nevins, M.; Marx, R.E.; Spagnoli, D.B.; Oates, T.W.; Moy, P.K.; Boyne, P.J. Pivotal, randomized, parallel evaluation of recombinant human bone morphogenetic protein-2/absorbable collagen sponge and autogenous bone graft for maxillary sinus floor augmentation. J. Oral Maxillofac. Surg. 2009, 67, 1947–1960. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Scaffold Property | Desirable Properties |
|---|---|
| Biocompatibility |
|
| Biodegradability |
|
| Mechanical stability |
|
| Bioactivity |
|
| Architecture |
|
| Surface of the scaffold |
|
| Sterilibility |
|
| Animals | Number of Studies (%) | Critical-Sized Defect (mm) Mean (SD) | Follow Up (Weeks) Mean (SD) | References |
|---|---|---|---|---|
| Rats | 26 (29.5) | 4.76 (0.3) | 10.1 (5.8) | [24,30,39,40,41,49,50,51,52,53,54,56,57,58,60,61,62,65,77,80,83,87,91,95,99,104] |
| Rabbits | 23 (26.1) | 17.2 (5.3) | 12.4 (4.1) | [22,23,25,26,27,28,29,32,33,44,59,69,71,75,76,79,85,98,100,101,102,105,108] |
| Dogs | 15 (17) | 25.3 (7.8) | 27.1 (24.5) | [31,37,38,46,67,78,81,82,86,88,90,96,97,106,107] |
| Sheep | 8 (9.1) | 34.3 (4.6) | 22.1 (16.3) | [47,64,72,73,74,84,89,94] |
| Mini-pigs | 7 (8) | 33.5 (6.9) | 34.6 (12.9) | [34,35,48,63,92,93,109] |
| nHPs * | 6 (6.8) | 29.1 (12.2) | 43.2 (34.5) | [45,55,66,68,70,103] |
| Swine | 2 (2.3) | 24.3 (5.6) | 10.0 (4.4) | [36,43] |
| Mice | 1 (1.1) | 10.0 | 4.0 | [42] |
| Characterization Approach | Number of Studies (%) | References |
|---|---|---|
| Micro-CT | 35 (39.8) | [24,27,30,33,35,39,40,41,43,44,45,47,49,50,51,62,65,69,76,77,78,79,80,83,84,85,86,88,90,93,99,100,101,102,107] |
| Histology | 79 (89.8) | [22,23,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,41,42,43,44,45,46,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,75,76,77,78,79,80,81,82,83,84,85,86,87,90,91,92,94,95,96,97,98,99,100,101,102,103,104,105,106,107] |
| Radiography | 38 (43.2) | [22,23,25,26,28,32,34,35,37,38,39,43,46,48,56,60,61,62,63,65,66,67,68,70,71,75,79,89,91,92,93,94,97,98,102,103,105,106] |
| Immunohistochemistry | 28 (31.8) | [30,35,36,41,46,47,48,49,50,52,57,60,61,64,67,72,73,76,83,86,88,92,93,96,97,101,102,106] |
| RT-PCR 1 (mRNA quantification) | 6 (6.8) | [23,57,80,88,92,106] |
| Fluorescence microscopy | 4 (4.5) | [53,54,72,109] |
| Biomechanical testing | 11 (12.5) | [24,28,37,38,42,63,73,74,92,102,103] |
| SPECT 2 | 1 (1.1) | [109] |
| SEM 3 | 10 (11.3) | [37,38,59,64,82,83,86,90,107,108] |
| CBCT 4 | 4 (4.5) | [36,59,71,96] |
| Scaffold | Number of Studies (%) | References |
|---|---|---|
| Natural polymers | ||
| Hyaluronic-acid-based | 3 (3.4) | [52,53,77] |
| Collagen | 23 (26.1) | [22,24,39,45,52,54,55,63,64,65,68,72,73,74,79,80,81,88,90,97,100,101,102] |
| Chitosan-based | 6 (6.8) | [49,59,76,87,99,100] |
| Synthetic polymers | ||
| PLGA 1 | 15 (17) | [26,33,35,36,40,41,43,46,47,50,51,66,70,103,108] |
| PLA-based | 3 (3.4) | [32,60,96] |
| PDLLA/CaCO3 2 | 2 (2.3) | [56,57] |
| <PEI 3 | 1 (1.1) | [36] |
| PCL 4 | 7 (8) | [27,59,82,85,98,106,107] |
| PTFE membrane 5 | 1 (1.1) | [94] |
| PU 6 | 1 (1.1) | [93] |
| Bioceramics | ||
| βTCP-based 7 | 12 (13.3) | [30,35,43,44,45,69,78,85,86,90,93,107] |
| HAP 8 | 16 (18.2) | [23,26,27,28,36,42,45,52,54,78,86,90,96,101,102,104] |
| Autologous (any tissue) | 3 (3.4) | [34,67,84] |
| Xenogenic graft (any tissue) | 3 (3.4) | [36,83,109] |
| Bioactive Molecules | Number of Studies (%) | References |
|---|---|---|
| BMP-2 | 31 (35.2) | [22,23,27,30,40,45,46,49,51,52,55,56,57,60,61,66,68,70,76,77,78,79,86,87,93,95,97,100,103,107,108] |
| BMP-7 | 5 (5.6) | [28,71,72,74,75] |
| BMP–4 | 1 (1.1) | [29] |
| BMP-2 + BMP-4 | 1 (1.1) | [53] |
| BMP-2 + phenamil | 1 (1.1) | [41] |
| BMP-2 + VEGF | 3 (3.4) | [43,88,92] |
| BMP-6 + VEGF | 1 (1.1) | [50] |
| BMP-2 + FGF | 3 (3.4) | [25,58,105] |
| FGF | 1 (1.1) | [80] |
| TGF1 + IGF-1 | 1 (1.1) | [91] |
| Insulin | 1 (1.1) | [33] |
| L-PRF | 1 (1.1) | [47] |
| rHOP-1 | 4 (4.5) | [63,65,73,109] |
| Dipyridamole | 1 (1.1) | [69] |
| CGF | 2 (2.3) | [101,102] |
| SDF 1α | 1 (1.1) | [24] |
| Cell Therapy | Number of Studies (%) | References |
|---|---|---|
| BMSCs | 22 (25) | [23,25,29,30,31,33,34,37,38,42,43,48,61,68,70,71,77,80,84,95,98,105] |
| DPSCs | 1 (1.1) | [26] |
| ADSCs | 7 (8) | [35,40,49,62,99,104,106] |
| MSCs | 11 (12.5) | [28,41,50,67,75,79,82,85,94,100,101] |
| SHED | 1 (1.1) | [81] |
| DFAT | 1 (1.1) | [39] |
| Osteoblasts/osteocytes | 2 (2.3) | [65,83] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Desnica, J.; Vujovic, S.; Stanisic, D.; Ognjanovic, I.; Jovicic, B.; Stevanovic, M.; Rosic, G. Preclinical Evaluation of Bioactive Scaffolds for the Treatment of Mandibular Critical-Sized Bone Defects: A Systematic Review. Appl. Sci. 2023, 13, 4668. https://doi.org/10.3390/app13084668
Desnica J, Vujovic S, Stanisic D, Ognjanovic I, Jovicic B, Stevanovic M, Rosic G. Preclinical Evaluation of Bioactive Scaffolds for the Treatment of Mandibular Critical-Sized Bone Defects: A Systematic Review. Applied Sciences. 2023; 13(8):4668. https://doi.org/10.3390/app13084668
Chicago/Turabian StyleDesnica, Jana, Sanja Vujovic, Dragana Stanisic, Irena Ognjanovic, Bojan Jovicic, Momir Stevanovic, and Gvozden Rosic. 2023. "Preclinical Evaluation of Bioactive Scaffolds for the Treatment of Mandibular Critical-Sized Bone Defects: A Systematic Review" Applied Sciences 13, no. 8: 4668. https://doi.org/10.3390/app13084668