
Internet-Based Video Program to Promote Physical Activity, Health, and Well-Being of Brazilian Older Adults during the COVID-19 Pandemic
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
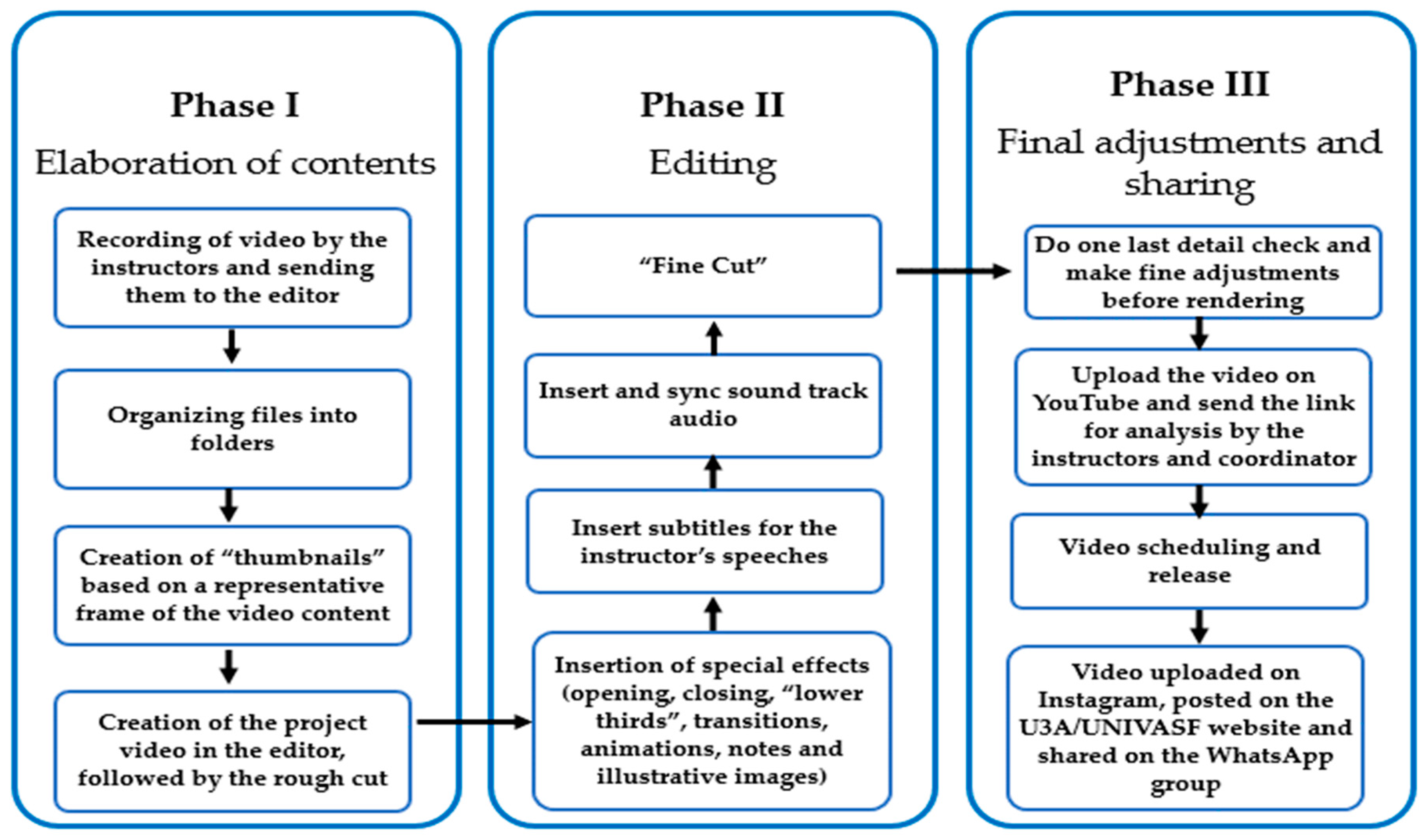
2.3. System Development
2.3.1. Video Planning
2.3.2. Video Recording and Editing
2.3.3. Video Sharing on the YouTube Platform
2.3.4. Video Sharing on Instagram
2.4. Evaluation of the Program “U3A in Motion”
Analysis of the Interviews
3. Results
3.1. Physical Exercises
3.2. Psychosocial Dynamics
3.3. Interviews
3.3.1. Discovery of the Program
3.3.2. Difficulties with the Video Methodology
3.3.3. Satisfaction with the Program “U3A in Motion”
3.3.4. Suggestions to Improve Future Videos
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- IBGE-Brazilian Institute of Geography and Statistics. IBGE Releases Estimate of the Population of Municipalities for 2020. Available online: https://agenciadenoticias.ibge.gov.br/agencia-sala-de-imprensa/2013-agencia-de-noticias/releases/28668-ibge-divulga-estimativa-da-populacao-dos-municipios-para-2020#:~:text=OIBGEdivulgahojeas,77%25emrelaçãoa2019 (accessed on 10 March 2023).
- Brazil Ministry of Health Coronavirus Dashboard. Available online: https://covid.saude.gov.br/ (accessed on 10 February 2023).
- Goethals, L.; Barth, N.; Guyot, J.; Hupin, D.; Celarier, T.; Bongue, B. Impact of Home Quarantine on Physical Activity Among Older Adults Living at Home During the COVID-19 Pandemic: Qualitative Interview Study. JMIR Aging 2020, 3, e19007. [Google Scholar] [CrossRef] [PubMed]
- Lebrasseur, A.; Fortin-Bédard, N.; Lettre, J.; Raymond, E.; Bussières, E.-L.; Lapierre, N.; Faieta, J.; Vincent, C.; Duchesne, L.; Ouellet, M.-C.; et al. Impact of the COVID-19 Pandemic on Older Adults: Rapid Review. JMIR Aging 2021, 4, e26474. [Google Scholar] [CrossRef] [PubMed]
- De Maio Nascimento, M.; da Silva Neto, H.R.; de Fátima Carreira Moreira Padovez, R.; Neves, V.R. Impacts of Social Isolation on the Physical and Mental Health of Older Adults During Quarantine: A Systematic Review. Clin. Gerontol. 2022, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Harridge, S.D.R.; Lazarus, N.R. Physical Activity, Aging, and Physiological Function. Physiology 2017, 32, 152–161. [Google Scholar] [CrossRef] [Green Version]
- García-Esquinas, E.; Ortolá, R.; Gine-Vázquez, I.; Carnicero, J.A.; Mañas, A.; Lara, E.; Alvarez-Bustos, A.; Vicente-Rodriguez, G.; Sotos-Prieto, M.; Olaya, B.; et al. Changes in Health Behaviors, Mental and Physical Health among Older Adults under Severe Lockdown Restrictions during the COVID-19 Pandemic in Spain. Int. J. Environ. Res. Public Health 2021, 18, 7067. [Google Scholar] [CrossRef]
- Makizako, H.; Nakai, Y.; Shiratsuchi, D.; Akanuma, T.; Yokoyama, K.; Matsuzaki-Kihara, Y.; Yoshida, H. Perceived declining physical and cognitive fitness during the COVID-19 state of emergency among community-dwelling Japanese old-old adults. Geriatr. Gerontol. Int. 2021, 21, 364–369. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A. Precision shielding for COVID-19: Metrics of assessment and feasibility of deployment. BMJ Glob. Health 2021, 6, e004614. [Google Scholar] [CrossRef]
- Bailey, L.; Ward, M.; DiCosimo, A.; Baunta, S.; Cunningham, C.; Romero-Ortuno, R.; Kenny, R.A.; Purcell, R.; Lannon, R.; McCarroll, K.; et al. Physical and mental health of older people while cocooning during the COVID-19 pandemic. QJM Int. J. Med. 2021, 114, 648–653. [Google Scholar] [CrossRef]
- Richardson, D.L.; Duncan, M.J.; Clarke, N.D.; Myers, T.D.; Tallis, J. The influence of COVID-19 measures in the United Kingdom on physical activity levels, perceived physical function and mood in older adults: A survey-based observational study. J. Sports Sci. 2021, 39, 887–899. [Google Scholar] [CrossRef]
- Gustavsson, J.; Beckman, L. Compliance to Recommendations and Mental Health Consequences among Elderly in Sweden during the Initial Phase of the COVID-19 Pandemic—A Cross Sectional Online Survey. Int. J. Environ. Res. Public Health 2020, 17, 5380. [Google Scholar] [CrossRef] [PubMed]
- Emerson, K.G. Coping with being cooped up: Social distancing during COVID-19 among 60+ in the United States. Rev. Panam. Salud Pública 2020, 44, 1. [Google Scholar] [CrossRef] [PubMed]
- Mishra, R.; Park, C.; York, M.K.; Kunik, M.E.; Wung, S.-F.; Naik, A.D.; Najafi, B. Decrease in Mobility during the COVID-19 Pandemic and Its Association with Increase in Depression among Older Adults: A Longitudinal Remote Mobility Monitoring Using a Wearable Sensor. Sensors 2021, 21, 3090. [Google Scholar] [CrossRef] [PubMed]
- Lage, A.; Carrapatoso, S.; de Queiroz Neto, E.S.; Gomes, S.; Soares-Miranda, L.; Bohn, L. Associations Between Depressive Symptoms and Physical Activity Intensity in an Older Adult Population During COVID-19 Lockdown. Front. Psychol. 2021, 12, 1680. [Google Scholar] [CrossRef]
- Wong, F.H.C.; Liu, T.; Leung, D.K.Y.; Zhang, A.Y.; Au, W.S.H.; Kwok, W.W.; Shum, A.K.Y.; Wong, G.H.Y.; Lum, T.Y.-S. Consuming Information Related to COVID-19 on Social Media Among Older Adults and Its Association With Anxiety, Social Trust in Information, and COVID-Safe Behaviors: Cross-sectional Telephone Survey. J. Med. Internet Res. 2021, 23, e26570. [Google Scholar] [CrossRef] [PubMed]
- Masaeli, N.; Farhadi, H. Prevalence of Internet-based addictive behaviors during COVID-19 pandemic: A systematic review. J. Addict. Dis. 2021, 39, 468–488. [Google Scholar] [CrossRef]
- Chen, Y.-R.R.; Schulz, P.J. The Effect of Information Communication Technology Interventions on Reducing Social Isolation in the Elderly: A Systematic Review. J. Med. Internet Res. 2016, 18, e18. [Google Scholar] [CrossRef]
- Di Giacomo, D.; Ranieri, J.; D’Amico, M.; Guerra, F.; Passafiume, D. Psychological Barriers to Digital Living in Older Adults: Computer Anxiety as Predictive Mechanism for Technophobia. Behav. Sci. 2019, 9, 96. [Google Scholar] [CrossRef] [Green Version]
- Xi, W.; Zhang, X.; Ayalon, L. When less intergenerational closeness helps: The influence of intergenerational physical proximity and technology attributes on technophobia among older adults. Comput. Human Behav. 2022, 131, 107234. [Google Scholar] [CrossRef]
- Nascimento, M.M. COVID-19: U3A students’ report on the impacts of social isolation on physical and mental health and access to information about the virus during the pandemic. Educ. Gerontol. 2020, 46, 499–511. [Google Scholar] [CrossRef]
- Duque, M.; Peres-Neto, L. Can older people stop sharing? An ethnographic study on fake news and active aging in Brazil. Online Media Glob. Commun. 2022, 1, 580–599. [Google Scholar] [CrossRef]
- Sixsmith, A.; Horst, B.R.; Simeonov, D.; Mihailidis, A. Older People’s Use of Digital Technology During the COVID-19 Pandemic. Bull. Sci. Technol. Soc. 2022, 42, 19–24. [Google Scholar] [CrossRef]
- Haase, K.R.; Cosco, T.; Kervin, L.; Riadi, I.; O’Connell, M.E. Older Adults’ Experiences With Using Technology for Socialization During the COVID-19 Pandemic: Cross-sectional Survey Study. JMIR Aging 2021, 4, e28010. [Google Scholar] [CrossRef]
- Drazich, B.F.; Li, Q.; Perrin, N.A.; Szanton, S.L.; Lee, J.W.; Huang, C.-M.; Carlson, M.C.; Samuel, L.J.; Regier, N.G.; Rebok, G.W.; et al. The relationship between older adults’ technology use, in-person engagement, and pandemic-related mental health. Aging Ment. Health 2023, 27, 156–165. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Stay Physically Active during Self-Quarantine. Available online: https://quarantrain.org/2020/03/18/who-stay-physically-active-during-self-quarantine/ (accessed on 28 February 2023).
- Joseph, R.P.; Durant, N.H.; Benitez, T.J.; Pekmezi, D.W. Internet-Based Physical Activity Interventions. Am. J. Lifestyle Med. 2014, 8, 42–67. [Google Scholar] [CrossRef] [Green Version]
- Kooij, L.; Groen, W.G.; van Harten, W.H. The Effectiveness of Information Technology-Supported Shared Care for Patients With Chronic Disease: A Systematic Review. J. Med. Internet Res. 2017, 19, e221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vegting, I.L.; Schrijver, E.J.M.; Otten, R.H.J.; Nanayakkara, P.W.B. Internet programs targeting multiple lifestyle interventions in primary and secondary care are not superior to usual care alone in improving cardiovascular risk profile: A systematic review. Eur. J. Intern. Med. 2014, 25, 73–81. [Google Scholar] [CrossRef]
- Bennett, G.G.; Herring, S.J.; Puleo, E.; Stein, E.K.; Emmons, K.M.; Gillman, M.W. Web-based Weight Loss in Primary Care: A Randomized Controlled Trial. Obesity 2010, 18, 308–313. [Google Scholar] [CrossRef]
- Dwyer, M.J.; Pasini, M.; De Dominicis, S.; Righi, E. Physical activity: Benefits and challenges during the COVID-19 pandemic. Scand. J. Med. Sci. Sports 2020, 30, 1291–1294. [Google Scholar] [CrossRef]
- Bagherian, S.; Ghahfarrokhi, M.M.; Banitalebi, E. Effect of the COVID-19 Pandemic on Interest in Home-Based Exercise: An Application of Digital Epidemiology. Int. J. Epidemiol. Res. 2021, 8, 47–53. [Google Scholar] [CrossRef]
- Gould, C.E.; Hantke, N.C. Promoting Technology and Virtual Visits to Improve Older Adult Mental Health in the Face of COVID-19. Am. J. Geriatr. Psychiatry 2020, 28, 889–890. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization (WHO): Geneva, Switzerland, 2020; ISBN 9781134470006.
- Sasaki, S.; Sato, A.; Tanabe, Y.; Matsuoka, S.; Adachi, A.; Kayano, T.; Yamazaki, H.; Matsuno, Y.; Miyake, A.; Watanabe, T. Associations between Socioeconomic Status, Social Participation, and Physical Activity in Older People during the COVID-19 Pandemic: A Cross-Sectional Study in a Northern Japanese City. Int. J. Environ. Res. Public Health 2021, 18, 1477. [Google Scholar] [CrossRef] [PubMed]
- Saraiva, M.D.; Apolinario, D.; Tavares, C.D.E.A.M.; Aliberti, M.J.R. Mobilility and Quality of Life During the COVID-19 Pandemic. J. Nutr. Health Aging 2020, 25, 440–447. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Muff, A.; Meschiany, G.; Lev-Ari, S. Adequacy of Web-Based Activities as a Substitute for In-Person Activities for Older Persons During the COVID-19 Pandemic: Survey Study. J. Med. Internet Res. 2021, 23, e25848. [Google Scholar] [CrossRef] [PubMed]
- Benvenuto, D.; Giovanetti, M.; Ciccozzi, A.; Spoto, S.; Angeletti, S.; Ciccozzi, M. The 2019-new coronavirus epidemic: Evidence for virus evolution. J. Med. Virol. 2020, 92, 455–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piret, J.; Boivin, G. Pandemics Throughout History. Front. Microbiol. 2021, 11, 631736. [Google Scholar] [CrossRef]
- Morgan, O.W.; Abdelmalik, P.; Perez-Gutierrez, E.; Fall, I.S.; Kato, M.; Hamblion, E.; Matsui, T.; Nabeth, P.; Pebody, R.; Pukkila, J.; et al. How better pandemic and epidemic intelligence will prepare the world for future threats. Nat. Med. 2022, 28, 1526–1528. [Google Scholar] [CrossRef]
- De Melo, G.C.; Duprat, I.P.; de Araújo, K.C.G.M.; Fischer, F.M.; Neto, R.A.D.A. Prediction of cumulative rate of COVID-19 deaths in Brazil: A modeling study. Rev. Bras. Epidemiol. 2020, 23, 1–11. [Google Scholar]
- Da Cruz, R.R.; Beltrame, V.; Dallacosta, F.M. Aging and vulnerability: An analysis of 1062 elderly persons. Rev. Bras. Geriatr. Gerontol. 2019, 22. [Google Scholar] [CrossRef]
- Souza, M.L.D.A.; Marques, T.V.; de Amorim, M.M.P. Vulnerability and incidence of covid-19 in Northeastregion of brazil through of the cluster analysis. Hygeia Rev. Bras. Geogr. Médica Saúde 2020, 16, 232–248. [Google Scholar]
- Aung, M.N.; Yuasa, M.; Koyanagi, Y.; Aung, T.N.N.; Moolphate, S.; Matsumoto, H.; Yoshioka, T. Sustainable health promotion for the seniors during COVID-19 outbreak: A lesson from Tokyo. J. Infect. Dev. Ctries. 2020, 14, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Aspers, P.; Corte, U. What is Qualitative in Qualitative Research. Qual. Sociol. 2019, 42, 139–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahman, M.S. The Advantages and Disadvantages of Using Qualitative and Quantitative Approaches and Methods in Language “Testing and Assessment” Research: A Literature Review. J. Educ. Learn. 2016, 6, 102. [Google Scholar] [CrossRef]
- Nascimento, M.; Juchem, L.; Maduro, L. Active Living Program: Sports and leisure in health promotion and quality of life of seniors in Petrolina and Juazeiro, Brazil. Rev. Bras. Ativ. Física Saúde 2016, 21, 593–599. [Google Scholar] [CrossRef] [Green Version]
- Tauben, D.J.; Langford, D.J.; Sturgeon, J.A.; Rundell, S.D.; Towle, C.; Bockman, C.; Nicholas, M. Optimizing telehealth pain care after COVID-19. Pain 2020, 161, 2437–2445. [Google Scholar] [CrossRef]
- Vandelanotte, C.; Müller, A.M.; Short, C.E.; Hingle, M.; Nathan, N.; Williams, S.L.; Lopez, M.L.; Parekh, S.; Maher, C.A. Past, Present, and Future of eHealth and mHealth Research to Improve Physical Activity and Dietary Behaviors. J. Nutr. Educ. Behav. 2016, 48, 219–228.e1. [Google Scholar] [CrossRef]
- Herbert, M.S.; Afari, N.; Liu, L.; Heppner, P.; Rutledge, T.; Williams, K.; Eraly, S.; VanBuskirk, K.; Nguyen, C.; Bondi, M.; et al. Telehealth Versus In-Person Acceptance and Commitment Therapy for Chronic Pain: A Randomized Noninferiority Trial. J. Pain 2017, 18, 200–211. [Google Scholar] [CrossRef]
- Nascimento, M.M.; Giannouli, E. Active aging through the University of the Third Age: The Brazilian model. Educ. Gerontol. 2019, 45, 11–21. [Google Scholar] [CrossRef]
- Rodriguez, A.; Smith, J. Phenomenology as a healthcare research method. Evid. Based Nurs. 2018, 21, 96–98. [Google Scholar] [CrossRef] [Green Version]
- Cilesiz, S. A phenomenological approach to experiences with technology: Current state, promise, and future directions for research. Educ. Technol. Res. Dev. 2011, 59, 487–510. [Google Scholar] [CrossRef]
- Gallagher, K.; Porock, D. The Use of Interviews in Q Methodology. Nurs. Res. 2010, 59, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Hammami, A.; Harrabi, B.; Mohr, M.; Krustrup, P. Physical activity and coronavirus disease 2019 (COVID-19): Specific recommendations for home-based physical training. Manag. Sport Leis. 2022, 27, 26–31. [Google Scholar] [CrossRef]
- Polero, P.; Rebollo-Seco, C.; Adsuar, J.C.; Pérez-Gómez, J.; Rojo-Ramos, J.; Manzano-Redondo, F.; Garcia-Gordillo, M.Á.; Carlos-Vivas, J. Physical Activity Recommendations during COVID-19: Narrative Review. Int. J. Environ. Res. Public Health 2020, 18, 65. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.J.; Lou, J.Q.; Ownby, R.L.; Caballero, J. A systematic review of eHealth interventions to improve health literacy. Health Inform. J. 2016, 22, 81–98. [Google Scholar] [CrossRef] [Green Version]
- Milne-Ives, M.; Lam, C.; De Cock, C.; Van Velthoven, M.H.; Meinert, E. Mobile Apps for Health Behavior Change in Physical Activity, Diet, Drug and Alcohol Use, and Mental Health: Systematic Review. JMIR mHealth uHealth 2020, 8, e17046. [Google Scholar] [CrossRef]
- Marchant, G.; Bonaiuto, F.; Bonaiuto, M.; Descas, E.G. Exercise and Physical Activity eHealth in COVID-19 Pandemic: A Cross-Sectional Study of Effects on Motivations, Behavior Change Mechanisms, and Behavior. Front. Psychol. 2021, 12, 618362. [Google Scholar] [CrossRef]
- Constantinou, D.; Torres, G.; Neophytou, N.; Fourie, P.; Buntting, X.; Gradidge, P. ‘I’m doing it for myself’: Using a smartphone-based exercise service during the COVID-19 lockdown in the Faculty of Health Sciences, University of the Witwatersrand, South Africa. South Afr. J. Sport. Med. 2021, 33, 1–6. [Google Scholar] [CrossRef]
- Sachser, C.; Olaru, G.; Pfeiffer, E.; Brähler, E.; Clemens, V.; Rassenhofer, M.; Witt, A.; Fegert, J.M. The immediate impact of lockdown measures on mental health and couples’ relationships during the COVID-19 pandemic—Results of a representative population survey in Germany. Soc. Sci. Med. 2021, 278, 113954. [Google Scholar] [CrossRef]
- Lahariya, C. ‘Ayushman Bharat’ Program and Universal Health Coverage in India. Indian Pediatr. 2018, 55, 495–506. [Google Scholar] [CrossRef]
- Lahariya, C. Health & Wellness Centers to Strengthen Primary Health Care in India: Concept, Progress and Ways Forward. Indian J. Pediatr. 2020, 87, 916–929. [Google Scholar] [CrossRef]
- Bitton, A.; Fifield, J.; Ratcliffe, H.; Karlage, A.; Wang, H.; Veillard, J.H.; Schwarz, D.; Hirschhorn, L.R. Primary healthcare system performance in low-income and middle-income countries: A scoping review of the evidence from 2010 to 2017. BMJ Glob. Health 2019, 4, e001551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vande Maele, N.; Xu, K.; Soucat, A.; Fleisher, L.; Aranguren, M.; Wang, H. Measuring primary healthcare expenditure in low-income and lower middle-income countries. BMJ Glob. Health 2019, 4, e001497. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Focus | Video Number | Variations | Recommended Frequency |
|---|---|---|---|
| Strength | 3–4, 7–11, 14, 16, 20, 23–25, 31, 32, 34, 44, 50–53, 56 |
| 3 times/day |
| Aerobic resistance | 35–36, 49, 61 |
| 3 times/day |
| Core stabilization and posture | 27, 41, 43, 55, 60 |
| 3 times/day |
| Mobility exercises | 6, 15, 26, 28–29, 33, 42, 45–46, 54, 57, 62 |
| 3 times/day |
| Gait and balance | 22, 37–38 |
| 3 times/day |
| Dual-task | 39–40, 63–66 |
| 3 times/day |
| Flexibility/stretching | 1, 5, 12, 17–19, 21, 30, 47–48, 59 |
| 3 times/day |
| Relaxation/meditation | 2, 12 |
| 3 times/day |
| Themes | Methodological Procedures |
|---|---|
| 1. Introduction | Presentation of intentions and importance of psychosocial activities during the period of isolation and social detachment |
| 2. Memory processes | Simple approach on cognitive performance and possible impacts of pandemic for these functions, as well as suggestions for activities to exercise cognitive processes |
| 3. Remember children’s time games | Tasks to activate long-term memory and motivate participants |
| 4. Plant cultivation | Stimulus to work with gardening, increasing the levels of physical activity in a relaxed way |
| 5. Crafts | Stimulates to perform manual work and occupy the time in a productive and joyful way |
| 6. List names of old friends and colleagues from U3A | Tasks to exercise long-term medium memory |
| 7. Draw what comes to mind | Tasks to stimulate creativity and pleasure |
| 8. Think about and remember happy moments of life | Tasks to stimulate memory and alleviate possible feelings of anxiety |
| 9. Full attention and meditation | Tasks to relax and calm down |
| 10. Tourism: Think of names of places you have already visited | Dynamics to travel through thought |
| 11. Reading books, magazines, poetry | Task for relaxing, having fun, and expanding knowledge |
| 12. Talk about emotions | Task to communicate with someone and talk/listen to everyday emotions |
| 13. Write a letter to someone special | Task to communicate with someone through writing |
| 14. Cognitive Games | Stimulus tasks of cognitive functions |
| 15. Integrational activities with family children | Suggestions for activities to perform with younger families |
| 16. Storytelling | Suggestion of activity to perform with a family member |
| 17. Music of each generation | Task to relax and remember moments of the past through songs |
| 18. Review photographs | Task to remember moments of the past |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Maio Nascimento, M.; Araújo, J.V.S.; da Cruz Neto, P.C.; Rios, P.M.B.; Silva, C.N.; Ihle, A. Internet-Based Video Program to Promote Physical Activity, Health, and Well-Being of Brazilian Older Adults during the COVID-19 Pandemic. Appl. Sci. 2023, 13, 4326. https://doi.org/10.3390/app13074326
de Maio Nascimento M, Araújo JVS, da Cruz Neto PC, Rios PMB, Silva CN, Ihle A. Internet-Based Video Program to Promote Physical Activity, Health, and Well-Being of Brazilian Older Adults during the COVID-19 Pandemic. Applied Sciences. 2023; 13(7):4326. https://doi.org/10.3390/app13074326
Chicago/Turabian Stylede Maio Nascimento, Marcelo, João Victor Silva Araújo, Pedro Cecílio da Cruz Neto, Pâmala Morais Bagano Rios, Carolina Nascimento Silva, and Andreas Ihle. 2023. "Internet-Based Video Program to Promote Physical Activity, Health, and Well-Being of Brazilian Older Adults during the COVID-19 Pandemic" Applied Sciences 13, no. 7: 4326. https://doi.org/10.3390/app13074326