
Minimizing the Vicious Circle of Pain–Anxiety–Avoidance: The Role of Positive Affect in Endodontic Therapy


Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Procedure
2.3. Measures
- (a)
- Baseline measurements
- i.
- Psychological variables:
- -
- Pain Anticipation: The question ad hoc: ‘How you feel the pain will be during treatment?’ was used to evaluate pain anticipation. This item presented a 10-point Likert-type response scale, ranging from ‘0 = no pain’ to ‘10 = maximum pain’.
- -
- Dental anxiety: The Modified Dental Anxiety Scale (MDAS) in its Spanish validation was used [21]. It is a short and commonly used tool. The MDAS was developed to improve the psychometric characteristics of the previous Dental Anxiety Scale (DAS) [22,23]. It contains 5 items related to dental experiences, with a 5-point Likert (from “not anxious” to “extremely anxious”) scale, obtaining a total score range from 5 to 25. A person is classified as ‘very dentally anxious’ with a score of 19 or higher. In previous studies, Cronbach′s alpha was 0.88 [24]. In our sample, a Cronbach′s alpha of 0.86 was found.
- -
- Positive Affect: The Positive and Negative Affect Scale (PANAS) in its Spanish version was used [25]. Specifically, the positive affect subscale was used to measure positive affect. The PANAS was developed by Watson et al. [26] and was adapted and validated in Spanish by Sandin et al. [27]. It is made up of two independent scales that allow the measurement of positive affect and negative affect. Each of the scales consists of 10 items with a Likert-type response format of 5 points, ranging from ‘1 = not at all’ to ‘5 = extremely’. Specifically, a positive affect is defined as the degree to which people have a tendency to experience positive emotions and engage in a pleasurable way with their environment. Previous research has revealed an exceptional internal consistency (0.90) [28]. Cronbach′s alpha value was 0.85 in our sample.
- ii.
- Clinical variables:
- -
- American Society of Anaesthesiologist’s Physical Status Classification System (ASA-PS) [29]: The ASA-PS was used to categorize the physical health of patients. This classification is a widely graded system used in healthcare-related environments. The rating is composed of six types (I to VI). In this research, only class I (healthy patients), class II (mild systemic disease patients), and class III (severe systemic disease patients) were used. The ASA-PS has been widely used in healthcare fields; however, it should be noted that it has a low inter-rater reliability with a profound dependency on the clinician′s experience [30].
- -
- Medication: This variable included whether the patients had taken medication (or not) for their current dental trouble before starting endodontic treatment. Previous medication became dichotomous variable scores were either 0 (patient hadn′t been taking medication) or 1 (patient had been taking medication). In addition, among the patients who had been taking medication, we registered the type of medication with an item on a response scale ‘1 = anti-inflammatory drugs’, ‘2 = antibiotics’, and ‘3 = antibiotics and anti-inflammatory drugs’.
- -
- The Endodontic Case Difficulty Assessment Form was developed by The American Association of Endodontics (AAE) [31]. The endodontist had to complete this form to identify three influential issues in the treatment: the patient′s considerations, diagnosis and treatment considerations, and additional considerations. For each of these categories, degrees of difficulty of treatment (minimal, moderate, and high) were distributed based on risk factors. The sample was distributed as ‘1 (minimal difficulty) = a case with any complicating factor’, ‘2 (moderate difficulty) = a case with one or more complicating factors’, ‘3 (high difficulty) = exhibiting multiple factors in the “moderate difficulty” category’.
- -
- Pulpal status: Palpation tests, percussion tests, and thermal sensibility tests were used to diagnose pulpal status. The patients were distributed in the following categories: irreversible pulpitis, necrosis, apical periodontitis, and the need for retreatment. Further, in order to assess whether the tooth to be treated showed a radiolucent injury in the bone, preoperative periapical radiography was performed. This was recorded as a dichotomous variable, which was either 1 (the tooth showed a radiolucent apical lesion) or 2 (the tooth did not show a radiolucent apical lesion).
- (b)
- End of treatment
- i.
- Psychological variables:
- -
- Subjective Avoidance: This behavioral indicator was registered using an ad hoc item. One week after Endodontic Therapy was finished, the patients were asked to evaluate the level of avoidance they remembered during treatment, answering: ‘To what extent would you still avoid having root canal treatment?’. A 10-point Likert response format was used for this item (ranging from ‘0 = no avoidance’ to ‘10 = maximum avoidance’).
- ii.
- Clinical variables:
- -
- Number of canals of treated teeth: This was registered as ‘1 = if the tooth had one canal to be treated’, ‘2 = if the tooth had two canals to be treated’, and successively.
2.4. Data Analysis
3. Results
3.1. Descriptive Analyses and Study of Covariates
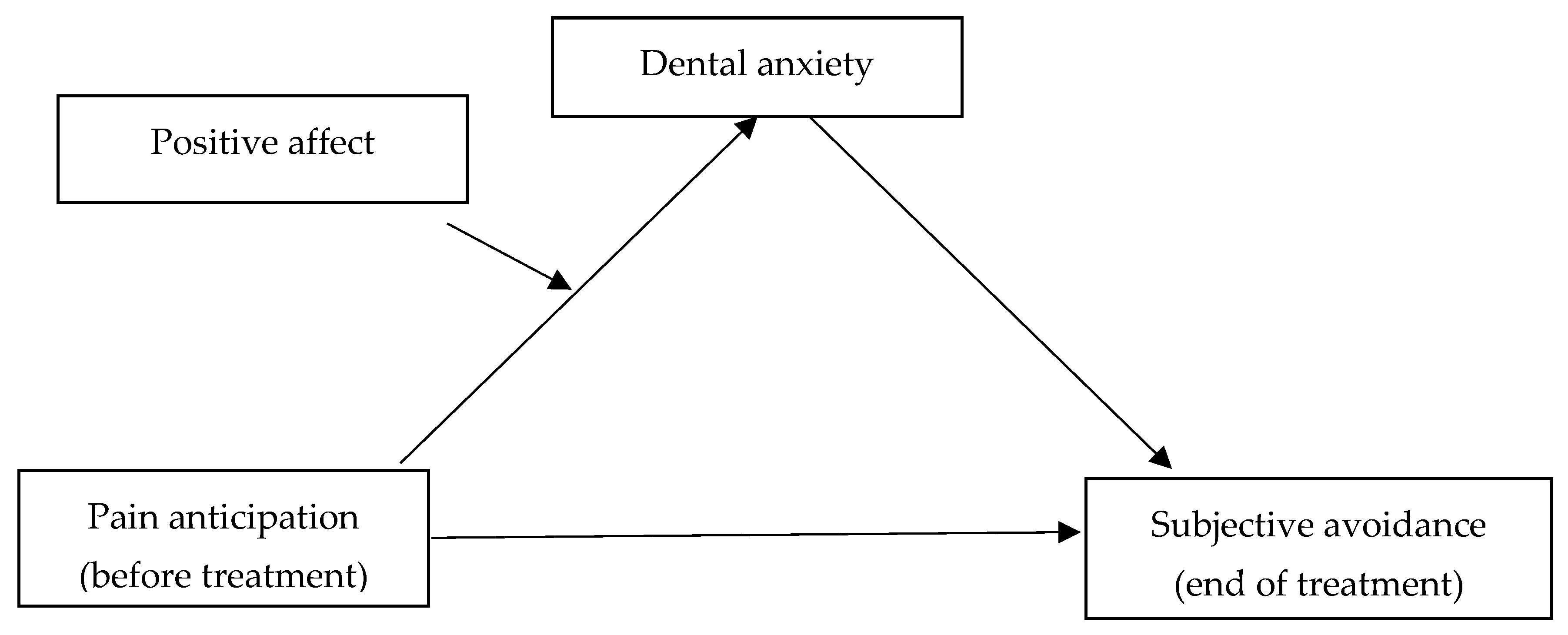
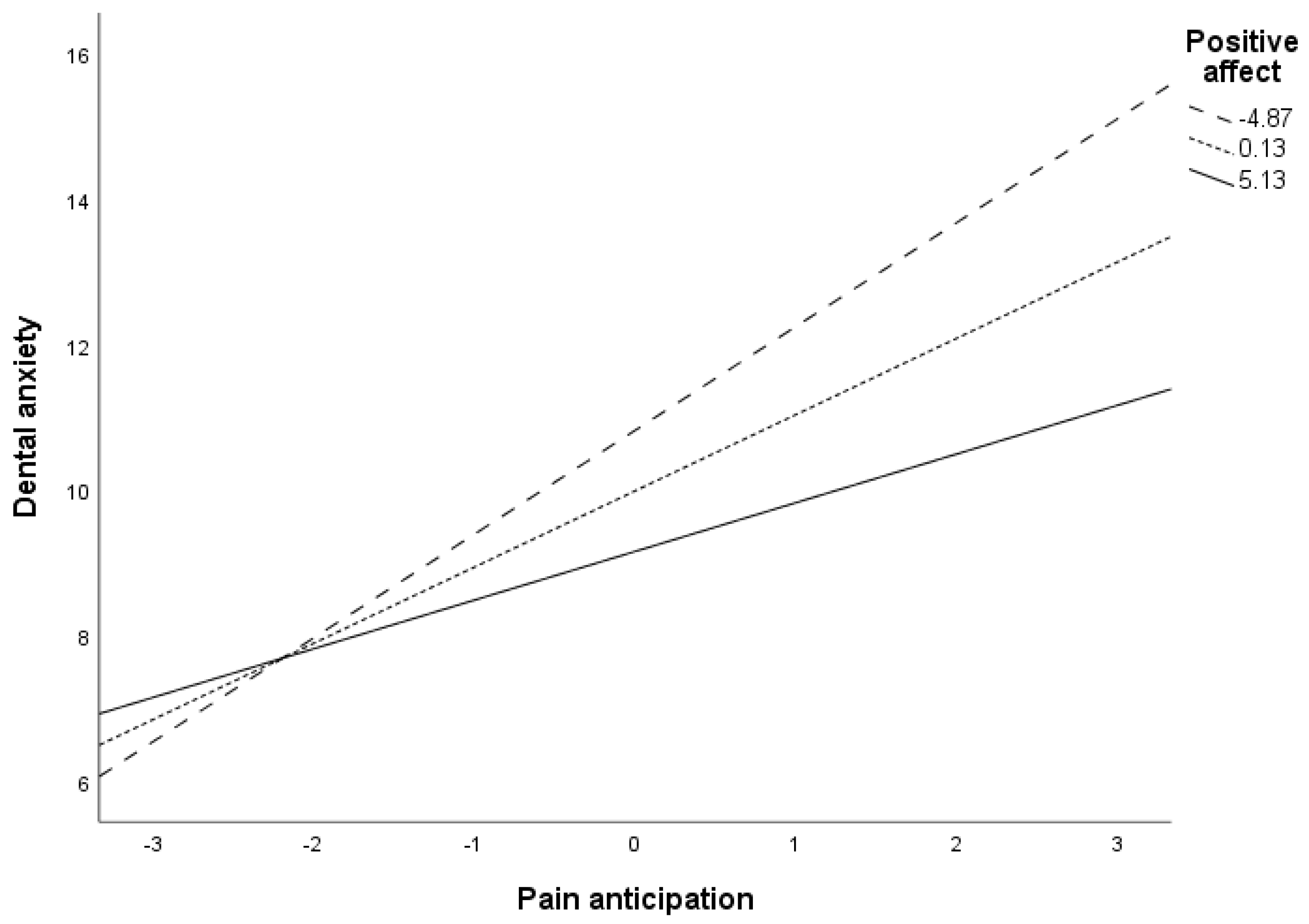
3.2. The Moderation Mediation Model of Pain Anticipation on Subjective Avoidance by Dental Anxiety, at Different Levels of Positive Affect
3.2.1. Previous Analysis: Mediation Role of Dental Anxiety between Pain Anticipation and Subjective Avoidance
3.2.2. The Moderation Mediation Model of Pain Anticipation on Subjective Avoidance by Dental Anxiety at Different Levels of Positive Affect
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thomson, W.M.; Williams, S.M.; Broadbent, J.M.; Poulton, R.; Locker, D. Long-term dental visiting patterns and adult oral health. J. Dent. Res. 2010, 89, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Consejo General de Dentistas de España. Available online: https://www.consejodentistas.es/ (accessed on 19 February 2022).
- European Survey of Health in Spain. Available online: https://www.ine.es/dyngs/INEbase/en/operacion.htm?c=Estadistica_C&cid=1254736176784&menu=resultados&idp=1254735573175 (accessed on 19 February 2022).
- Dou, L.; Vanschaayk, M.M.; Zhang, Y.; Fu, X.; Ji, P.; Yang, D. The prevalence of dental anxiety and its association with pain and other variables among adult patients with irreversible pulpitis. BMC Oral Health 2018, 18, 101. [Google Scholar] [CrossRef] [Green Version]
- Armfield, J.M. Predicting dental avoidance among dentally fearful Australian adults. Eur. J. Oral Sci. 2013, 121, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Strøm, K.; Skaare, A.B.; Willumsen, T. Dental anxiety in 18-year-old Norwegians in 1996 and 2016. Acta Odontol. Scand. 2020, 78, 13–19. [Google Scholar] [CrossRef]
- Berggren, U.; Carlsson, S.G. A psychophysiological therapy for dental fear. Behav. Res. Ther. 1984, 22, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Litt, M.D. A model of pain and anxiety associated with acute stressors: Distress in dental procedures. Behav. Res. Ther. 1996, 34, 459–476. [Google Scholar] [CrossRef]
- Van Wijk, A.J.; Hoogstraten, J. Reducing fear of pain associated with endodontic therapy. Int. Endod. J. 2006, 39, 384–388. [Google Scholar] [CrossRef]
- Lin, C.S.; Niddam, D.M.; Hsu, M.L.; Hsieh, J.C. Pain catastrophizing is associated with dental pain in a stressful context. J. Dent. Res. 2013, 92, 130–135. [Google Scholar] [CrossRef] [Green Version]
- Nermo, H.; Willumsen, T.; Johnsen, J.-A.K. Changes in dental anxiety among 15- to 21-year-olds. A 2-year longitudinal analysis based on the Tromsø study: Fit futures. Community Dent. Oral Epidemiol. 2019, 47, 127–133. [Google Scholar] [CrossRef]
- Armfield, J.M.; Stewart, J.F.; Spencer, J. The vicious cycle of dental fear: Exploring the interplay between oral health, service utilization and dental fear. BMC Oral Health 2007, 7, 1. [Google Scholar] [CrossRef] [Green Version]
- Chandraweera, L.; Goh, K.; Lai-Tong, J.; Newby, J.; Abbott, P. A survey of patients’ perceptions about, and their experiences of, root canal treatment. Aust. Endod. J. 2019, 45, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Bender, I.E. Pulpar pain diagnosis—A review. J. Endod. 2000, 26, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.E.; Carter, G.; George, R. Pathways of fear and anxiety in endodontic patients. Int. Endod. J. 2015, 48, 528–532. [Google Scholar] [CrossRef]
- Perković, I.; Knežević, M.R.; Perić, M.; Krmek, S.J. The level of anxiety and pain perception of endodontic patients. Acta Stomatol. Croat. 2014, 48, 258–267. [Google Scholar] [CrossRef]
- Ibrahim, H.; Lyons, K.M.; Armfield, J.M.; Thomson, W.M. Performance of the Index of Dental Anxiety and Fear in a population-based sample of adults. Aust. Dent. J. 2017, 62, 478–484. [Google Scholar] [CrossRef] [Green Version]
- Jönsson, B.; Holde, G.E.; Baker, S.R. The role of psychosocial factors and treatment need in dental service use and oral health among adults in Norway. Community Dent. Oral Epidemiol. 2020, 48, 215–224. [Google Scholar] [CrossRef] [PubMed]
- McGrath, C. Behavioral Sciences in the Promotion of Oral Health. J. Dent. Res. 2019, 98, 1418–1424. [Google Scholar] [CrossRef]
- European Society of Endodontology. Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [Google Scholar] [CrossRef]
- Coolidge, T.; Chambers, M.A.; Garcia, L.J.; Heaton, L.J.; Coldwell, S.E. Psychometric properties of Spanish-language adult dental fear measures. BMC Oral Health 2008, 8, 15. [Google Scholar] [CrossRef] [Green Version]
- Humphris, G.M.; Morrison, T.; Lindsay, S.J. The Modified Dental Anxiety Scale: Validation and United Kingdom norms. Community Dent. Health 1995, 12, 143–150. [Google Scholar]
- Corah, N.L. Development of a dental anxiety scale. J. Dent. Res. 1969, 48, 596. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Buchanan, H.; Topcu, G. Are dental-related psychological variables important for dental attendance in China? A cross-sectional study. J. Public Health Dent. 2022, 82, 437–444. [Google Scholar] [CrossRef] [PubMed]
- López-Gómez, I.; Hervas, G.; Vazquez, C. Adaptation of the Positive and Negative Affect Schedule (PANAS) in a general Spanish population. Behav. Psychol. 2015, 23, 529–548. [Google Scholar]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Sandín, B.; Chorot, P.; Lostao, L.; Joiner, T.E.; Santed, M.A.; Valiente, R.M. Escalas PANAS de afecto positivo y negativo: Validación factorial y convergencia transcultural. Psicothema 1999, 11, 37–51. [Google Scholar]
- Díaz-García, A.; González-Robles, A.; Mor, S.; Mira, A.; Quero, S.; García-Palacios, A.; Baños, R.M.; Botella, C. Positive and Negative Affect Schedule (PANAS): Psychometric properties of the online Spanish version in a clinical sample with emotional disorders. BMC Psychiatry 2020, 20, 56. [Google Scholar] [CrossRef] [Green Version]
- Saklad, M. Grading of patients for surgical procedures. Anesthesiology 1941, 2, 281–284. [Google Scholar] [CrossRef]
- De Cassani, A.; Boscolo, A.; Tonetti, T.; Ban, I.; Ori, C. Assignment of ASA-physical status relates to anesthesiologists´experience: A survey-based national-study. Korean J. Anesth. 2019, 72, 53–59. [Google Scholar] [CrossRef]
- American Association of Endodontists. Endodontic Case Difficulty Assessment Form and Guidelines. Available online: https://www.aae.org/specialty/wp-content/uploads/sites/2/2022/01/CaseDifficultyAssessmentFormFINAL2022.pdf (accessed on 28 January 2023).
- Hayes, A.F.; Montoya, A.K. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 3rd ed.; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Preacher, K.J.; Rucker, D.D.; Hayes, A.F. Addressing Moderated Mediation Hypotheses: Theory, Methods, and Prescriptions. Multivar. Behav. Res. 2007, 42, 185–227. [Google Scholar] [CrossRef]
- Berggren, U.; Meynert, G. Dental fear and avoidance: Causes, symptoms, and consequences. J. Am. Dent. Assoc. 1984, 109, 247–251. [Google Scholar] [CrossRef]
- Murillo-Benítez, M.; Martín-González, J.; Jiménez-Sánchez, M.C.; Cabanillas-Balsera, D.; Velasco-Ortega, E.; Segura-Egea, J.J. Association between dental anxiety and intraoperative pain during root canal treatment: A cross-sectional study. Int. Endod. J. 2020, 53, 447–454. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Morley, S. The psychological flexibility model: A basis for integration and progress in psychological approaches to chronic pain management. J. Pain 2014, 15, 221–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, W.; McCracken, L.M. Psychological flexibility, acceptance and commitment therapy, and chronic pain. Curr. Opin. Psychol. 2015, 2, 91–96. [Google Scholar] [CrossRef]
- Fisher, S.; Gillanders, D.; Ferreira, N. The experiences of palliative care professionals and their responses to work-related stress: A qualitative study. Br. J. Health Psychol. 2022, 27, 605–622. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Chen, X.; Gong, H.; Wang, W.; Ji, W.; Liang, S. Relationship between paternal adult attachment and adolescent anxiety: The chain-mediating effect of paternal psychological flexibility and father-adolescent attachment. Int. J. Psychol. 2022, 57, 411–419. [Google Scholar] [CrossRef]
- Werner, H.; Young, C.; Hakeberg, M.; Wide, U. A behavioural intervention for young adults with dental caries, using acceptance and commitment therapy (ACT): Treatment manual and case illustration. BMC Oral Health 2020, 20, 233. [Google Scholar] [CrossRef]
- Asimakopoulou, K.; Newton, J.T. The contributions of behaviour change science towards dental public health practice: A new paradigm. Community Dent. Oral Epidemiol. 2015, 43, 2–8. [Google Scholar] [CrossRef] [Green Version]
- Cheng, L.; Zhang, L.; Yue, L.; Ling, J.; Fan, M.; Yang, D.; Huang, Z.; Niu, Y.; Liu, J.; Zhao, J.; et al. Expert consensus on dental caries management. Int. J. Oral Sci. 2022, 14, 17. [Google Scholar] [CrossRef]
- Moore, R. Maximizing Student Clinical Communication Skills in Dental Education-A Narrative Review. Dent. J. 2022, 10, 57. [Google Scholar] [CrossRef]
- Huang, Y.K.; Chen, Y.T.; Chang, Y.C. Initiating narrative medicine into dental education: Opportunity, change, and challenge. J. Formos. Med. Assoc. 2021, 120, 2191–2194. [Google Scholar] [CrossRef]
- Marti, K.C.; Mylonas, A.I.; MacEachern, M.; Gruppen, L. Humanities in Predoctoral Dental Education: A Scoping Review. J. Dent. Educ. 2019, 83, 1174–1198. [Google Scholar] [CrossRef]
- Dockray, S.; Steptoe, A. Positive affect and psychobiological processes. Neurosci. Biobehav. Rev. 2010, 35, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S.I.R.; Rao, D.; Ramachandran, A.; Ashok, B.V.; Baskaradoss, J.K. Neurotic personality trait as a predictor in the prognosis of composite restorations: A 24-month clinical follow up study. Sci. Rep. 2021, 11, 17179. [Google Scholar] [CrossRef] [PubMed]
- Valdes-Stauber, J.; Hummel, K. The relationship between dental anxiety and other kinds of anxiety: A naturalistic, cross-sectional and comparative study. BMC Psychol. 2021, 9, 184. [Google Scholar] [CrossRef] [PubMed]
- Willen, S.S.; Williamson, A.F.; Walsh, C.C.; Hyman, M.; Tootle, W. Rethinking flourishing: Critical insights and qualitative perspectives from the U.S. Midwest. SSM Ment. Health 2022, 2, 100057. [Google Scholar] [CrossRef]
- Baskaradoss, J.K. Relationship between oral health literacy and oral health status. BMC Oral Health 2018, 18, 172. [Google Scholar] [CrossRef]
- Armfield, J.M.; Heaton, L. Management of fear and anxiety in the dental clinic: A review. Aust. Dent. J. 2013, 58, 390–407. [Google Scholar] [CrossRef]
- Bertacco, M.; Soyeux, O.; Durand, R.; Boudrias, P.; Wiseman, L.; Rompré, P.; Raimville, P.; Emami, E.; Gosselin, N. Effect of personalized musical intervention on burden of care in dental implant surgery: A pilot randomized controlled trial. J. Dent. 2022, 120, 104091. [Google Scholar] [CrossRef]
- Sivaramakrishnan, G.; Makki, H.; Aldallal, S.; Alaswad, Z.; Sultan, E.; Ahmed, S.; AlBanna, H.; Alsobaiei, M.; AlSalihi, L. The variables associated with dental anxiety and their management in primary care dental clinics in Bahrain: A cross-sectional study. BMC Oral Health 2022, 22, 137. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Mean (SD) | 2 | 3 | 4 | |
|---|---|---|---|---|
| 1. Pain anticipation | 4.11 (2.40) | 0.581 ** | 0.386 ** | −0.253 * |
| 2. Dental anxiety | 10.29 (4.79) | 0.411 ** | −0.284 ** | |
| 3. Subjective avoidance | 4.75 (3.53) | −0.065 | ||
| 4. Positive affect | 35.72 (5.09) |
| Moderation of Positive Affect on Dental Anxiety | ||||
|---|---|---|---|---|
| VD: Dental Anxiety | B (SE) | t | p | [LLCI-ULCI] |
| VI: Pain anticipation (Pain) | 1.05 (0.179) | 5.88 | <0.001 | [0.70/1.41] |
| M: Positive affect (PA) | −0.17 (0.08) | −1.97 | 0.051 | [−0.33/<0.001] |
| Pain × PA (interaction) | −0.08 (0.03) | −2.17 | 0.032 | [−0.14/−0.006] |
| * previous medication (covariate) | 0.48 (0.94) | 0.512 | 0.609 | [−1.38/2.34] |
| Conditional effects of the predictor (i.e., pain anticipation) at different values of the moderator (PA) | ||||
| −4.87 | 1.42 (0.24) | 5.89 | <0.001 | [0.945/1.91] |
| 0.13 | 1.04 (0.18) | 5.82 | <0.001 | [0.609/1.40] |
| 5.13 | 0.67 (0.26) | 2.58 | 0.011 | [0.154/1.18] |
| Regression of pain anticipation on subjective avoidance through dental anxiety | ||||
| VD: Subjective avoidance | B (SE) | t | p | [LLCI-ULCI] |
| VI: Pain anticipation | 0.33 (0.17) | 1.92 | 0.057 | [−0.01/0.67] |
| Me: Dental anxiety | 0.21 (0.08) | 2.50 | 0.013 | [0.04/0.37] |
| * previous medication (covariate) | −0.09 (0.75) | −0.12 | 0.907 | [−1.58/1.40] |
| Model summary | R2: 0.21 | p < 0.001 | ||
| Indirect effects at values * of PA | ||||
| −4.87 | 0.29 (0.12) | [0.05/0.55] | ||
| 0.13 | 0.21 (0.09) | [0.04/0.42] | ||
| 5.13 | 0.13 (0.09) | [<0.001/0.36] | ||
| Indexes of moderated mediation | −0.02 (0.01) | [−0.04/0.002] | ||
| Effect 1 minus Effect 2. Conditional indirect effects contrast | ||||
| Effect 1 | Effect 2 | contrast | [LLCI/ULCI] | |
| 0.216 0.138 0.138 | 0.294 0.294 0.216 | −0.078 −0.156 −0.078 | [−0.189/0.008] [−0.379/0.016] [−0.189/0.008] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos-Puerta, N.; Peñacoba-Puente, C. Minimizing the Vicious Circle of Pain–Anxiety–Avoidance: The Role of Positive Affect in Endodontic Therapy. Appl. Sci. 2023, 13, 4327. https://doi.org/10.3390/app13074327
Santos-Puerta N, Peñacoba-Puente C. Minimizing the Vicious Circle of Pain–Anxiety–Avoidance: The Role of Positive Affect in Endodontic Therapy. Applied Sciences. 2023; 13(7):4327. https://doi.org/10.3390/app13074327
Chicago/Turabian StyleSantos-Puerta, Noelia, and Cecilia Peñacoba-Puente. 2023. "Minimizing the Vicious Circle of Pain–Anxiety–Avoidance: The Role of Positive Affect in Endodontic Therapy" Applied Sciences 13, no. 7: 4327. https://doi.org/10.3390/app13074327