

Machine-Learning-Based-Approaches for Sleep Stage Classification Utilising a Combination of Physiological Signals: A Systematic Review

Abstract
:1. Introduction
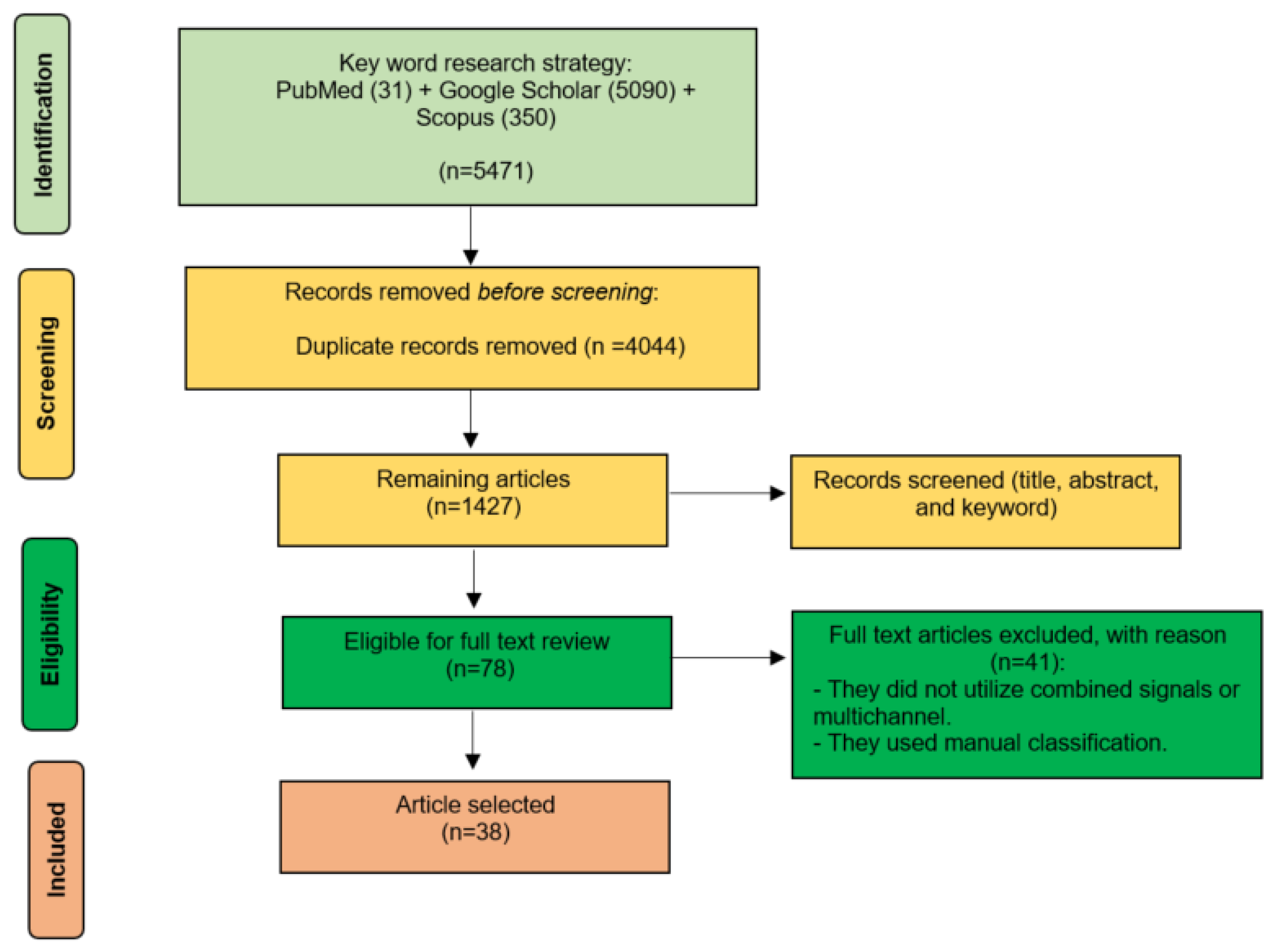
2. Methodology of Selection Papers
2.1. Data Sources
2.2. Data Extraction
2.3. Data Analyses
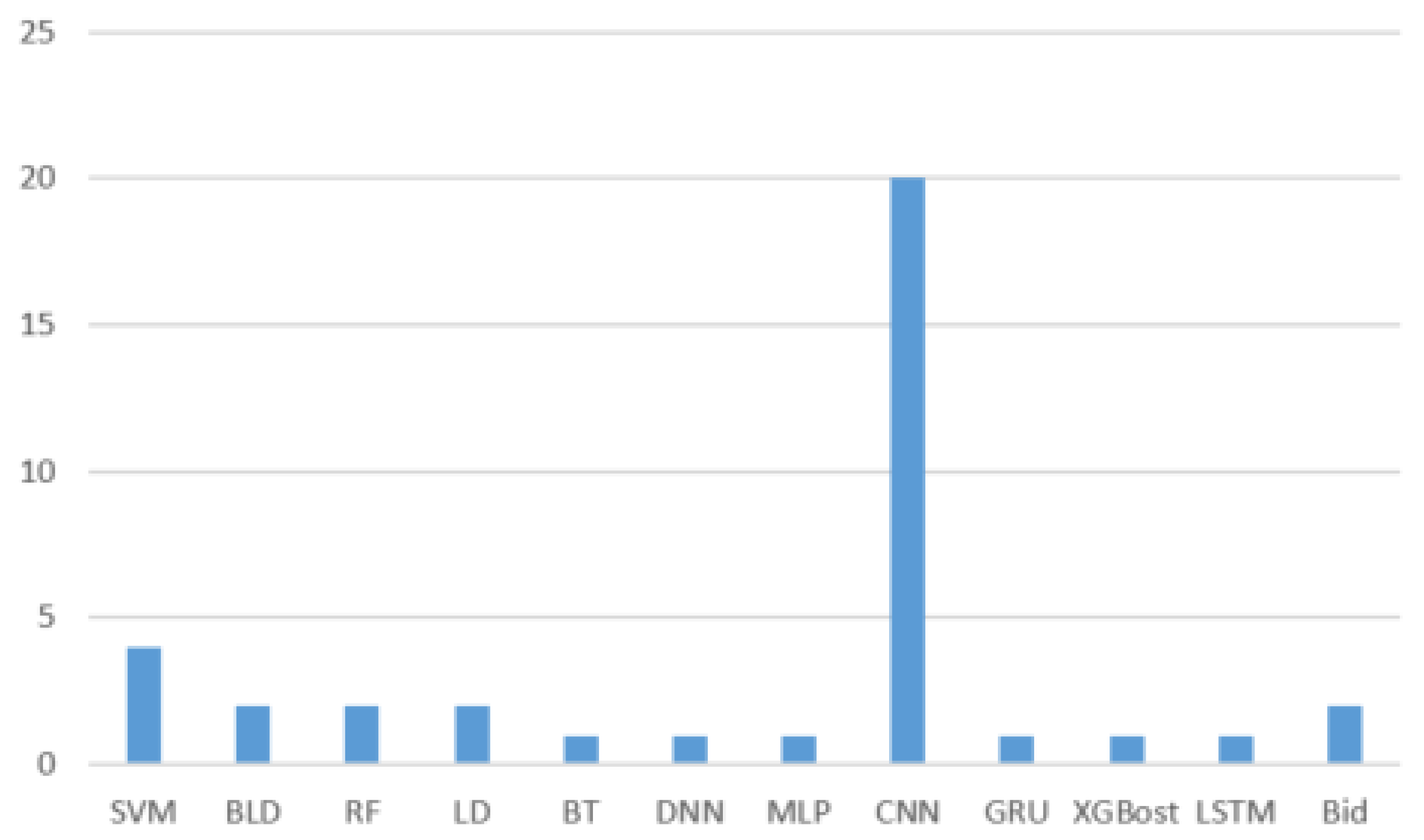
2.4. Results
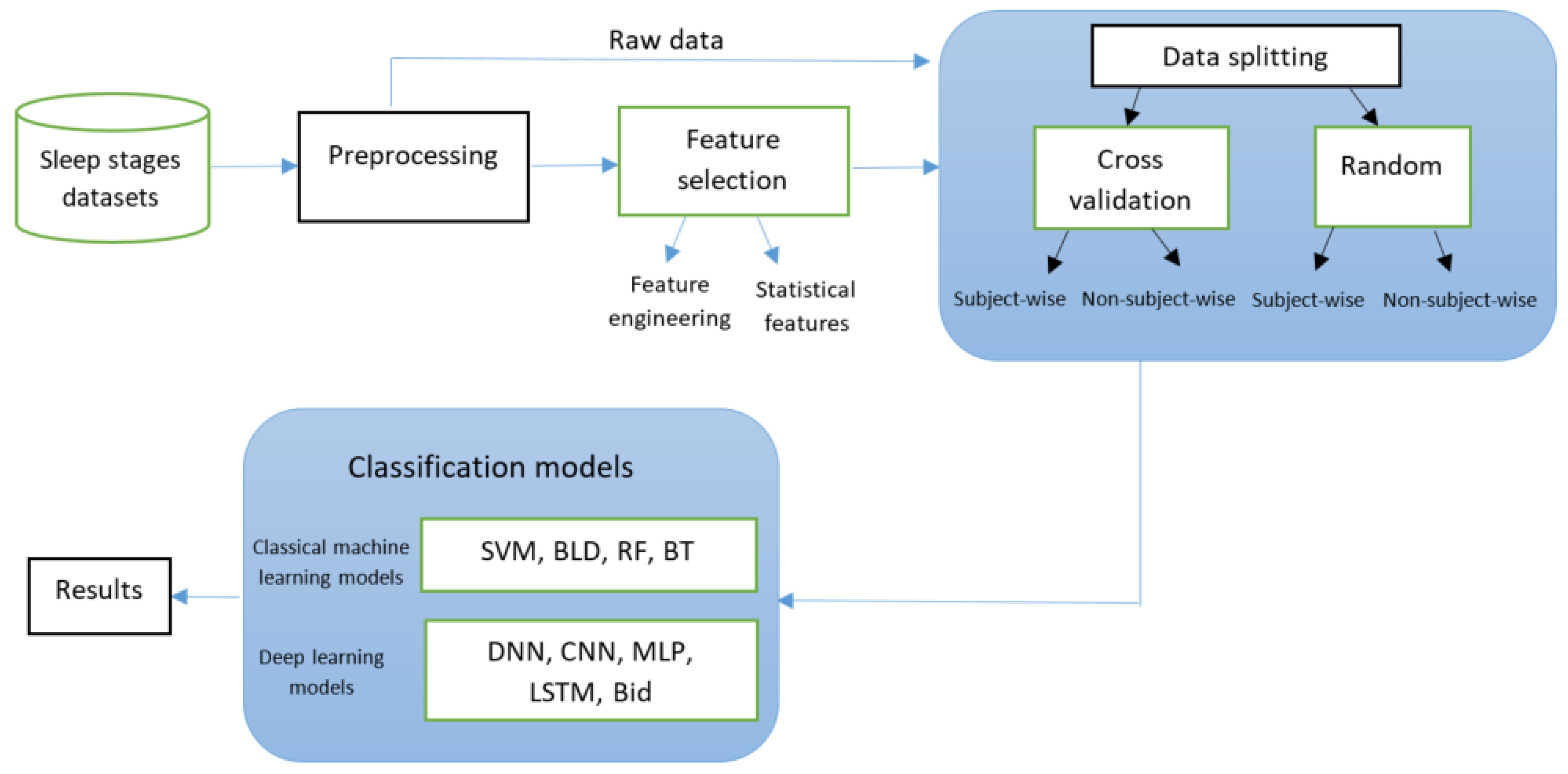
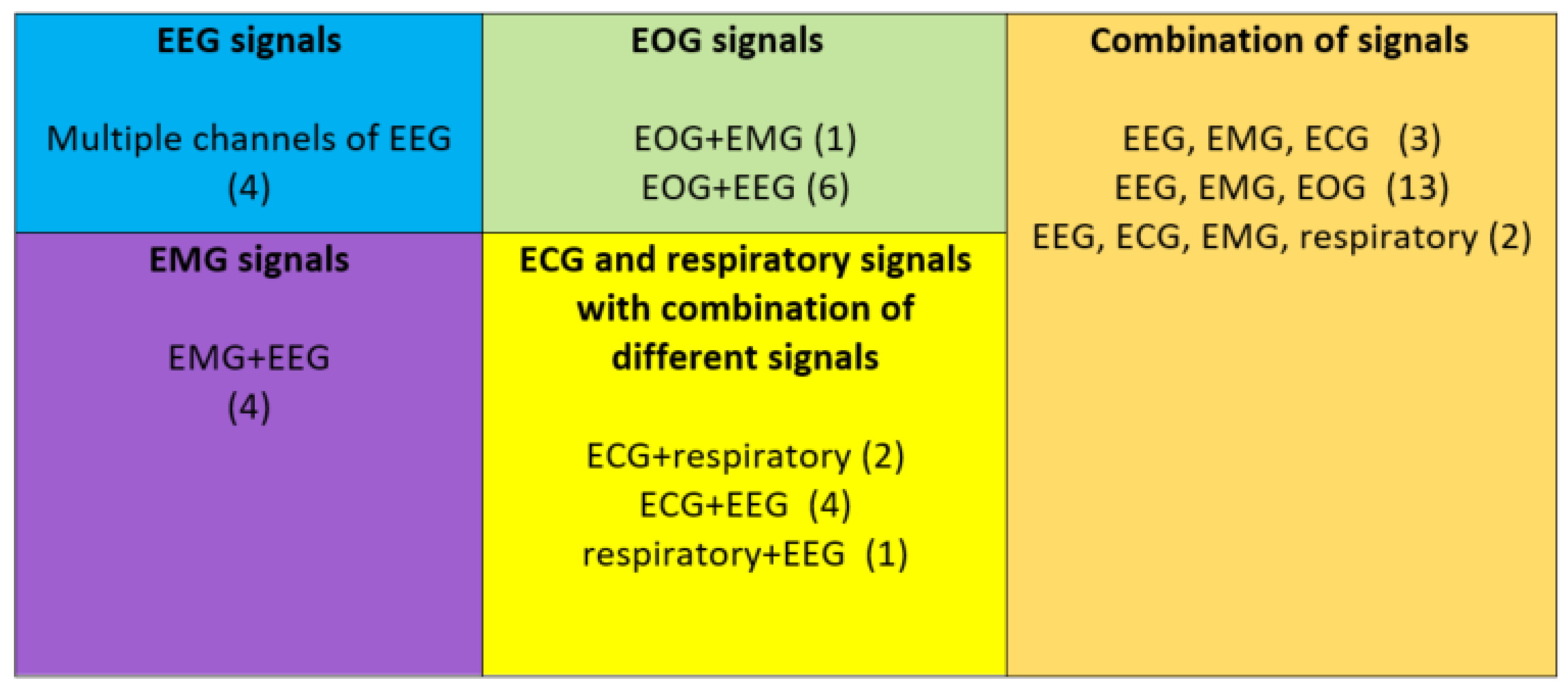
3. Conceptual Framework for the Classification of Sleep Stages
4. Literature Review
4.1. Electroencephalogram (EEG)
4.2. Electromyogram (EMG)
4.3. Electrooculogram (EOG)
4.4. Electrocardiogram (ECG) and Respiratory
4.5. Combination of Signals

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S.No | Author/Year | Dataset | Number of Samples/Recordings | Signals | Number of Channels | Input | Classification | Number of Classes | Accuracy | Kappa | Splitting Strategy |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Esteevez et al., 2002 [104] | Private | 11 recordings | EOG, EMG, EEG | - | FFT | Fuzzy rule | 5 | - | - | - |
| 2 | Estrada et al., 2006 [71] | Private | 10 recordings | EOG, EMG | 2 | FFT | Fuzzy rule | 5 | - | - | - |
| 3 | Akin et al., 2008 [65] | Private | 30 recordings | EEG, EMG | 2 | WT | DNN | 3 | - | 98.00 | 50% training + 50% testing |
| 4 | Yu et al., 2012 [86] | Private | 4 recordings | EEG, ECG | 2 | FFT | SVM | 5 | 99.00 | - | - |
| 5 | Long et al., 2014 [82] | Private | 115 recordings | ECG, respiratory | - | Statistic features | LD | 2 | 95.00 | 59.00 | - |
| 6 | Willemen et al., 2014 [88] | Private | 35,124 samples | EEG, EMG, respiratory | - | WT | SVM | 5 | 69.00 | 69.50 | - |
| 7 | Helland et al., 2015 [89] | Private | 10 recordings | EEG, ECG, respiratory | 3 | Statistic features | BLD | 3 | 80.00 | ||
| 8 | Fonseca et al., 2015 [83] | Private | - | ECG, respiratory | 2 | Statistical features | BLD | 3 | 80.00 | 49.00 | - |
| 9 | Kim et al., 2018 [66] | Sleep-edf | 5 recordings | EEG, EMG | 2 | TD | SVM | 5 | 93.80 | 94.00 | 10-fold |
| 10 | Takatani et al., 2018 [90] | Private | 431 recordings | EEG, ECG, EMG | - | RR+FFT | LD | 5 | 80.00 | - | - |
| 11 | Cui et al., 2018 [93] | ISRUC-Sleep | 106 recordings | EEG, EOG, EMG | 5 | Fine-grained | 2D-CNN | 5 | 90.12 | 81.00 | 10-fold subject-wise |
| 12 | Tripathy et al., 2018 [85] | MIT-BIH | 18 recordings | EEG, ECG | 2 | Statistic features | DNN | 5 | 73.70 | - | 10-fold subject-wise |
| 13 | Yuan et al., 2018 [98] | UCD | 25 recordings | EEG, ECG, EMG | - | Raw data | 1D-CNN 2D-CNN | 5 | 73.00 | - | - |
| STFT | 74.22 | - | |||||||||
| 14 | Bisawal et al., 2018 [91] | Private | 10,000 samples | EEG, EMG, ECG | 6 | FFT | 1D-CNN+ Bi-LSTM | 5 | 87.50 | 80.50 | Train 90%, testing 10% subject-wise |
| 15 | Zhang et al., 2018 [94] | SHHS | 5804 recordings | EEG, EMG, EOG | 5 | TD+FFT | 2D-CNN | 5 | 86.00 | 82.00 | Train 90%, testing 10% subject-wise |
| 16 | Chambon et al., 2018 [95] | MASS | 62 recordings | EEG, EOG, EMG | 11 | Raw data | 2D-CNN | 5 | 79.00 | 70.00 | 5-fold subject-wise |
| 17 | Phan et al., 2019 [74] | MASS | 200 recordings | EEG, EOG | 2 | FFT | 2D-CNN | 5 | 87.10 | 81.50 | 20-fold subject-wise |
| 18 | Yildirim et al., 2019 [72] | Sleep-edf | 15,188 samples | EEG, EOG | 2 | Raw data | 1D-CNN | 3 5 | 94.64 91.22 | - | Training 70%, validation 15%, testing 15% non-subject-wise |
| Sleep-edfx | 127,512 samples | 2 | 3 5 | 94.34 90.98 | |||||||
| 19 | Blanco et al., 2019 [59] | Sleep-edfx | 20 recordings | EEG | 2 | Raw data | 1D-CNN | 5 | 92.60 | 84.00 | 20-fold subject-wise |
| 20 | Phan et al., 2019 [105] | Sleep-edf | 20 recordings | EEG, EMG, EOG | 2 | FFT | 2D-CNN | 5 | 82.30 | 75.00 | Training 19 subjects, validation 4 subjects, testing 4 subjects |
| MASS | 200 recordings | 82.50 | 75.00 | 20-fold cross-validation | |||||||
| 21 | Satapathy et al., 2020 [60] | ISRUC-Sleep Subgroup 1 | 6000 samples | EEG | 2 | Raw data | 1D-CNN | 5 | 97.22 | - | Training 70%, testing 30% |
| ISRUC-Sleep Subgroup 2 | 95.06 | - | |||||||||
| 22 | Tautan et al., 2020 [64] | PhysioNet Challenge | 994 recordings | EEG, ECG | 2 | Statistic features+FFT | RF | 5 | 72.52 | - | 10-fold subject-wise |
| EEG, EMG | 88.65 | - | |||||||||
| EEG, respiratory | 93.72 | - | |||||||||
| EEG, ECG | 2 | Statistic features+FFT | MLP | 5 | 60.28 | - | |||||
| EEG, EMG | 66.70 | - | |||||||||
| EEG, respiratory | 52.27 | - | |||||||||
| 23 | Sokolovsky et al., 2020 [73] | Sleep-edfx | 20 recordings | EEG, EOG | 3 | Raw data | 1D-CNN | 5 | 81.00 | - | 10-fold subject-wise |
| 24 | Xu et al., 2020 [96] | Sleep-edf | 37,628 samples | EEG, EMG, EOG | 4 | Raw data | 1D-CNN | 5 | 85.40 | 78.90 | 5-fold subject-wise |
| Sleep-edfx | 213,695 samples | 81.60 | 74.70 | ||||||||
| 25 | Delimayanti et al., 2020 [61] | Sleep-edfx | 127,663 samples | EEG | 2 | FFT | SVM | 3 | 94.14 | - | 10-fold |
| 5 | 91.37 | - | |||||||||
| 26 | Casal et al., 2021 [84] | SHHS | 5000 recordings | ECG, respiratory | 2 | Raw data | GRU | 2 | 90.13 | 74.00 | Training 50%, validation 25%, testing 25% subject-wise |
| 27 | Zhao et al., 2021 [87] | MIT-BIH | 10,127 samples | EEG, ECG | 2 | Raw data | 1D-CNN | 2 | 98.84 | - | 10 fold |
| 28 | Sharma et al., 2022 [97] | SHHS visit 1 | 5,861,304 samples | EEG, EOG, EMG | 5 | WT | BT | 3 5 | 95.05 94.79 | 83.80 | Training 90%, testing 10% |
| SHHS visit 2 | 3,037,838 samples | 3 5 | 95.44 95.20 | 86.00 | |||||||
| 29 | Satapathy et al., 2022 [99] | ISRUC-Sleep Subgroup 1 | 3750 samples | EEG, EOG, EMG | 3 | Raw data | 1D-CNN | 3 5 | 98.61 89.46 | - | Training 70%, testing 30% |
| ISRUC-Sleep Subgroup 2 | 3750 samples | 3 5 | 98.78 98.46 | ||||||||
| 30 | Satapathy et al., 2022 [100] | ISRUC-Sleep Subgroup 1 | 3750 samples | EEG, EOG, EMG | 3 | Statistic features | RF | 5 | 98.52 | - | Training 70%, testing 30% |
| ISRUC-Sleep Subgroup 3 | 3750 samples | 5 | 98.46 | ||||||||
| 31 | Pie et al., 2022 [102] | SHHS visit 1 | 717,883 samples | EEG, EMG, EOG | 4 | Raw data | 1D-CNN | 5 | 83.15 | 89.00 | Training 50%, validation 20%, testing 30% |
| 32 | Sekkal et al., 2022 [75] | Sleep-edfx | 21,265 samples | EEG, EOG | 3 | Statistic features | SVM | 5 | 89.10 | 82.00 | Training 80%, testing 15% |
| 33 | Almutairi et al., 2023 [67] | Sleep-edfx | 72,000 samples | EEG, EMG | 3 | Raw data | 1D-CNN + LSTM | 3 | 95.46 | 90.12 | |
| EEG, EOG | 3 | 95.65 | 89.70 | ||||||||
| EEG, EMG, EOG | 4 | Raw data | 1D-CNN + LSTM | 3 5 | 96.36 96.57 | 93.40 83.05 | Training 70%, validation 15%, testing 15%, non-subject-wise | ||||
| ISRUC-Sleep Subgroup 1 | 56,515 samples | EEG, EMG, EOG | 5 | 3 5 | 94.90 93.96 | 90.34 77.31 | |||||
| 34 | Choi et al., 2023 [92] | SHHS | 9736 recordings | ECG, EMG, EEG | 3 | Statistic features | XGBoost | 5 | 85.00 | - | 10-fold non-subject-wise |
| 35 | Dequidt et al., 2023 [62] | MASS | 62 recordings | EEG | 8 | FFT | VGG-16 | 5 | 82.96 | 80.90 | 31-fold subject-wise |
| 36 | Toma et al., 2023 [101] | Sleep-edf | 20 recordings | EEG, EMG, EOG | 4 | Raw data | 1D-CNN + Bi-LSTM | 5 | 91.44 | 89.00 | Training 85%, testing 15% non-subject-wise |
| 37 | Toma et al., 2023 [76] | Sleep-edf | 20 recordings | EEG, EOG | 3 | Raw data | 1D-CNN + RNN | 5 | 90.30 | 86.86 | Training 85%, testing 15% non-subject-wise |
| 38 | Huang et al., 2023 [103] | Sleep-edfx | 20 recordings | EEG, EOG, EMG | 3 | Raw data | 1D-CNN + attention | 5 | 90.30 | 86.86 | - |
5. Gaps in Literature
5.1. Testing of Multiple Datasets
5.2. Splitting Strategy
5.3. Computational Complexity
5.4. Imbalanced Dataset
5.5. Scarcity of Studies Using a Combination of Signals for Sleep Stage Classification
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Laposky, A.D.; Bass, J.; Kohsaka, A.; Turek, F.W. Sleep and circadian rhythms: Key components in the regulation of energy metabolism. FEBS Lett. 2008, 582, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.W.; Duffy, J.F. Sleep, sleep disorders, and sexual dysfunction. World J. Men Health 2019, 37, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M. Epidemiological overview of sleep disorders in the general population. Sleep Med. Res. 2011, 2, 1–9. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Smirne, S. Prevalence and consequences of insomnia disorders in the general population of Italy. Sleep Med. 2002, 3, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Fietze, I.; Laharnar, N.; Bargiotas, P.; Basoglu, O.K.; Dogas, Z.; Drummond, M.; Fanfulla, F.; Gislason, T.; Gouveris, H.; Grote, L.; et al. Management of obstructive sleep apnea in Europe–A 10-year follow-up. Sleep Med. 2022, 97, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Sotres-Alvarez, D.; Gallo, L.C.; Ramos, A.R.; Aviles-Santa, L.; Perreira, K.M.; Isasi, C.R.; Zee, P.C.; Savin, K.L.; Schneiderman, N.; et al. Associations of sleep-disordered breathing and insomnia with incident hypertension and diabetes. The Hispanic community health study/study of Latinos. Am. J. Respir. Crit. Care Med. 2021, 203, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Streatfeild, J.; Smith, J.; Mansfield, D.; Pezzullo, L.; Hillman, D. The social and economic cost of sleep disorders. Sleep 2021, 44, zsab132. [Google Scholar] [CrossRef]
- Pennings, N.; Golden, L.; Yashi, K.; Tondt, J.; Bays, H.E. Sleep-disordered breathing, sleep apnea, and other obesity-related sleep disorders: An Obesity Medicine Association (OMA) Clinical Practice Statement (CPS) 2022. Obes. Pillars 2022, 4, 100043. [Google Scholar] [CrossRef]
- Yan, B.; Yang, J.; Zhao, B.; Fan, Y.; Wang, W.; Ma, X. Objective sleep efficiency predicts cardiovascular disease in a community population: The sleep heart health study. J. Am. Heart Assoc. 2021, 10, e016201. [Google Scholar] [CrossRef]
- Silber, M.H.; Ancoli-Israel, S.; Bonnet, M.H.; Chokroverty, S.; Grigg-Damberger, M.M.; Hirshkowitz, M.; Kapen, S.; Keenan, S.A.; Kryger, M.H.; Penzel, T.; et al. The visual scoring of sleep in adults. J. Clin. Sleep Med. 2007, 3, 121–131. [Google Scholar] [CrossRef]
- Obal, F., Jr.; Krueger, J.M. Biochemical regulation of non-rapid-eye-movement sleep. Front.-Biosci.-Landmark 2003, 8, 520–550. [Google Scholar]
- Somers, V.K.; Dyken, M.E.; Mark, A.L.; Abboud, F.M. Sympathetic-nerve activity during sleep in normal subjects. N. Engl. J. Med. 1993, 328, 303–307. [Google Scholar] [CrossRef]
- Penzel, T.; Kantelhardt, J.W.; Lo, C.C.; Voigt, K.; Vogelmeier, C. Dynamics of heart rate and sleep stages in normals and patients with sleep apnea. Neuropsychopharmacology 2003, 28, S48–S53. [Google Scholar] [CrossRef] [PubMed]
- Bloch, K.E. Polysomnography: A systematic review. Technol. Health Care 1997, 5, 285–305. [Google Scholar] [CrossRef] [PubMed]
- Coronel, C.; Wiesmeyr, C.; Garn, H.; Kohn, B.; Wimmer, M.; Mandl, M.; Glos, M.; Penzel, T.; Klösch, G.; Stefanic-Kejik, A.; et al. Detection of respiratory events by respiratory effort and oxygen desaturation. J. Med. Biol. Eng. 2020, 40, 517–525. [Google Scholar] [CrossRef]
- Campbell, I.G. EEG recording and analysis for sleep research. Curr. Protoc. Neurosci. 2009, 49, 10–12. [Google Scholar] [CrossRef] [PubMed]
- Kesper, K.; Canisius, S.; Penzel, T.; Ploch, T.; Cassel, W. ECG signal analysis for the assessment of sleep-disordered breathing and sleep pattern. Med. Biol. Eng. Comput. 2012, 50, 135–144. [Google Scholar] [CrossRef]
- Jammes, B.; Sharabty, H.; Esteve, D. Automatic EOG analysis: A first step toward automatic drowsiness scoring during wake-sleep transitions. Somnologie-Schlafforschung Schlafmed. 2008, 12, 227–232. [Google Scholar] [CrossRef]
- Shokrollahi, M.; Krishnan, S. Sleep EMG analysis using sparse signal representation and classification. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 3480–3483. [Google Scholar]
- Steriade, M.M.; McCarley, R.W. Brainstem Control of Wakefulness and Sleep; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Collop, N.A. Scoring variability between polysomnography technologists in different sleep laboratories. Sleep Med. 2002, 3, 43–47. [Google Scholar] [CrossRef]
- Zhou, X.Y.; Guo, Y.; Shen, M.; Yang, G.Z. Application of artificial intelligence in surgery. Front. Med. 2020, 14, 417–430. [Google Scholar] [CrossRef] [PubMed]
- Albaqami, H.; Hassan, G.M.; Datta, A. Wavelet-Based Multi-Class Seizure Type Classification System. Appl. Sci. 2022, 12, 5702. [Google Scholar] [CrossRef]
- Aboalayon, K.A.I.; Faezipour, M.; Almuhammadi, W.S.; Moslehpour, S. Sleep stage classification using EEG signal analysis: A comprehensive survey and new investigation. Entropy 2016, 18, 272. [Google Scholar] [CrossRef]
- Zhang, Y.; Weng, Y.; Lund, J. Applications of explainable artificial intelligence in diagnosis and surgery. Diagnostics 2022, 12, 237. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Ronzhina, M.; Janoušek, O.; Kolářová, J.; Nováková, M.; Honzík, P.; Provazník, I. Sleep scoring using artificial neural networks. Sleep Med. Rev. 2012, 16, 251–263. [Google Scholar] [CrossRef] [PubMed]
- Movahedi, F.; Coyle, J.L.; Sejdić, E. Deep belief networks for electroencephalography: A review of recent contributions and future outlooks. IEEE J. Biomed. Health Inform. 2017, 22, 642–652. [Google Scholar] [CrossRef]
- Loh, H.W.; Ooi, C.P.; Vicnesh, J.; Oh, S.L.; Faust, O.; Gertych, A.; Acharya, U.R. Automated detection of sleep stages using deep learning techniques: A systematic review of the last decade (2010–2020). Appl. Sci. 2020, 10, 8963. [Google Scholar] [CrossRef]
- Mishra, S.; Birok, R. Literature review: Sleep stage classification based on EEG signals using artificial intelligence technique. Recent Trends Commun. Electron. 2021, 10, 241–244. [Google Scholar]
- Faust, O.; Razaghi, H.; Barika, R.; Ciaccio, E.J.; Acharya, U.R. A review of automated sleep stage scoring based on physiological signals for the new millennia. Comput. Methods Programs Biomed. 2019, 176, 81–91. [Google Scholar] [CrossRef]
- Fiorillo, L.; Puiatti, A.; Papandrea, M.; Ratti, P.L.; Favaro, P.; Roth, C.; Bargiotas, P.; Bassetti, C.L.; Faraci, F.D. Automated sleep scoring: A review of the latest approaches. Sleep Med. Rev. 2019, 48, 101204. [Google Scholar] [CrossRef] [PubMed]
- Dixon-Woods, M.; Bonas, S.; Booth, A.; Jones, D.R.; Miller, T.; Sutton, A.J.; Shaw, R.L.; Smith, J.A.; Young, B. How can systematic reviews incorporate qualitative research? A critical perspective. Qual. Res. 2006, 6, 27–44. [Google Scholar] [CrossRef]
- Kemp, B.; Zwinderman, A.H.; Tuk, B.; Kamphuisen, H.A.; Oberye, J.J. Analysis of a sleep-dependent neuronal feedback loop: The slow-wave microcontinuity of the EEG. IEEE Trans. Biomed. Eng. 2000, 47, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Kemp, B.; Zwinderman, A.; Tuk, B.; Kamphuisen, H.; Oberyé, J. Sleep-EDF Database Expanded. Available online: https://www.physionet.org (accessed on 17 July 2018).
- O’reilly, C.; Gosselin, N.; Carrier, J.; Nielsen, T. Montreal Archive of Sleep Studies: An open-access resource for instrument benchmarking and exploratory research. J. Sleep Res. 2014, 23, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Ichimaru, Y.; Moody, G. Development of the polysomnographic database on CD-ROM. Psychiatry Clin. Neurosci. 1999, 53, 175–177. [Google Scholar] [CrossRef] [PubMed]
- Khalighi, S.; Sousa, T.; Santos, J.M.; Nunes, U. ISRUC-Sleep: A comprehensive public dataset for sleep researchers. Comput. Methods Programs Biomed. 2016, 124, 180–192. [Google Scholar] [CrossRef] [PubMed]
- Quan, S.F.; Howard, B.V.; Iber, C.; Kiley, J.P.; Nieto, F.J.; O’Connor, G.T.; Rapoport, D.M.; Redline, S.; Robbins, J.; Samet, J.M.; et al. The sleep heart health study: Design, rationale, and methods. Sleep 1997, 20, 1077–1085. [Google Scholar]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef]
- Ghassemi, M.M.; Moody, B.E.; Lehman, L.W.H.; Song, C.; Li, Q.; Sun, H.; Mark, R.G.; Westover, M.B.; Clifford, G.D. You snooze, you win: The physionet/computing in cardiology challenge 2018. In Proceedings of the 2018 Computing in Cardiology Conference (CinC), Maastricht, The Netherlands, 23–26 September 2018; Volume 45, pp. 1–4. [Google Scholar]
- Redfern, M.S.; Hughes, R.E.; Chaffin, D.B. High-pass filtering to remove electrocardiographic interference from torso EMG recordings. Clin. Biomech. 1993, 8, 44–48. [Google Scholar] [CrossRef]
- Mohamad, I.B.; Usman, D. Standardization and its effects on K-means clustering algorithm. Res. J. Appl. Sci. Eng. Technol. 2013, 6, 3299–3303. [Google Scholar] [CrossRef]
- Karthik, G.V.S.; Fathima, S.Y.; Rahman, M.Z.U.; Ahamed, S.R.; Lay-Ekuakille, A. Efficient signal conditioning techniques for brain activity in remote health monitoring network. IEEE Sensors J. 2013, 13, 3276–3283. [Google Scholar] [CrossRef]
- Nussbaumer, H.J. Fast convolution algorithms. In Fast Fourier Transform and Convolution Algorithms; Springer: Berlin/Heidelberg, Germany, 1982; pp. 32–79. [Google Scholar]
- Sundararajan, D. Discrete Wavelet Transform: A Signal Processing Approach; John Wiley & Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Phan, H.; Andreotti, F.; Cooray, N.; Chén, O.Y.; De Vos, M. DNN filter bank improves 1-max pooling CNN for single-channel EEG automatic sleep stage classification. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 453–456. [Google Scholar]
- Pan, J.; Tompkins, W.J. A real-time QRS detection algorithm. IEEE Trans. Biomed. Eng. 1985, 3, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Koles, Z.; Lind, J.; Soong, A. Spatio-temporal decomposition of the EEG: A general approach to the isolation and localization of sources. Electroencephalogr. Clin. Neurophysiol. 1995, 95, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Chandrashekar, G.; Sahin, F. A survey on feature selection methods. Comput. Electr. Eng. 2014, 40, 16–28. [Google Scholar] [CrossRef]
- Yunita, A.; Santoso, H.B.; Hasibuan, Z.A. Deep Learning for Predicting Students’ Academic Performance. In Proceedings of the 2019 Fourth International Conference on Informatics and Computing (ICIC), Semarang, Indonesia, 16–17 October 2019; pp. 1–6. [Google Scholar]
- Yadav, S.; Shukla, S. Analysis of k-fold cross-validation over hold-out validation on colossal datasets for quality classification. In Proceedings of the 2016 IEEE 6th International Conference on Advanced Computing (IACC), Bhimavaram, Andhra Pradesh, India, 27–28 February 2016; pp. 78–83. [Google Scholar]
- Morley, A.; Hill, L.; Kaditis, A. 10–20 System EEG Placement; European Respiratory Society: Lausanne, Switzerland, 2016; p. 34. [Google Scholar]
- Lee, M.; Song, C.B.; Shin, G.H.; Lee, S.W. Possible effect of binaural beat combined with autonomous sensory meridian response for inducing sleep. Front. Hum. Neurosci. 2019, 13, 425. [Google Scholar] [CrossRef] [PubMed]
- Lechat, B.; Hansen, K.; Catcheside, P.; Zajamsek, B. Beyond K-complex binary scoring during sleep: Probabilistic classification using deep learning. Sleep 2020, 43, zsaa077. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Molina, G.; Tsoneva, T.; Jasko, J.; Steele, B.; Aquino, A.; Baher, K.; Pastoor, S.; Pfundtner, S.; Ostrowski, L.; Miller, B.; et al. Closed-loop system to enhance slow-wave activity. J. Neural Eng. 2018, 15, 066018. [Google Scholar] [CrossRef]
- Nir, Y.; Massimini, M.; Boly, M.; Tononi, G. Sleep and consciousness. In Neuroimaging of Consciousness; Springer: Berlin/Heidelberg, Germany, 2013; pp. 133–182. [Google Scholar]
- Fernandez-Blanco, E.; Rivero, D.; Pazos, A. Convolutional neural networks for sleep stage scoring on a two-channel EEG signal. Soft Comput. 2020, 24, 4067–4079. [Google Scholar] [CrossRef]
- Satapathy, S.K.; Loganathan, D.; Narayanan, P.; Sharathkumar, S. Convolutional neural network for classification of multiple sleep stages from dual-channel EEG signals. In Proceedings of the 2020 IEEE 4th Conference on Information & Communication Technology (CICT), Chennai, India, 3–5 December 2020; pp. 1–16. [Google Scholar]
- Delimayanti, M.K.; Laya, M.; Faisal, M.R.; Naryanto, R.F.; Satou, K. The Effect of Feature Selection on Automatic Sleep Stage Classification Based On Multichannel EEG Signals. In Proceedings of the 2021 IEEE 5th International Conference on Information Technology, Information Systems and Electrical Engineering (ICITISEE), Purwokerto, Indonesia, 24–25 November 2021; pp. 272–276. [Google Scholar]
- Dequidt, P.; Seraphim, M.; Lechervy, A.; Gaez, I.I.; Brun, L.; Etard, O. Automatic Sleep Stage Classification on EEG Signals Using Time-Frequency Representation. In Proceedings of the International Conference on Artificial Intelligence in Medicine, Portoroz, Slovenia, 12–15 June 2023; Springer: Berlin/Heidelberg, Germany, 2023; pp. 250–259. [Google Scholar]
- Levendowski, D.J.; Louis, E.K.S.; Strambi, L.F.; Galbiati, A.; Westbrook, P.; Berka, C. Comparison of EMG power during sleep from the submental and frontalis muscles. Nat. Sci. Sleep 2018, 10, 431. [Google Scholar] [CrossRef]
- Tăutan, A.M.; Rossi, A.C.; de Francisco, R.; Ionescu, B. Automatic sleep stage detection: A study on the influence of various PSG input signals. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 5330–5334. [Google Scholar]
- Akin, M.; Kurt, M.B.; Sezgin, N.; Bayram, M. Estimating vigilance level by using EEG and EMG signals. Neural Comput. Appl. 2008, 17, 227–236. [Google Scholar] [CrossRef]
- Kim, H.; Choi, S. Automatic sleep stage classification using eeg and emg signal. In Proceedings of the 2018 Tenth International Conference on Ubiquitous and Future Networks (ICUFN), Prague, Czech Republic, 3–6 July 2018; pp. 207–212. [Google Scholar]
- Almutairi, H.; Hassan, G.M.; Datta, A. Classification of sleep stages from EEG, EOG and EMG signals by SSNet. arXiv 2023, arXiv:2307.05373. [Google Scholar]
- Banerjee, A.; Pal, M.; Tibarewala, D.; Konar, A. Electrooculogram based blink detection to limit the risk of eye dystonia. In Proceedings of the 2015 Eighth International Conference on Advances in Pattern Recognition (ICAPR), Kolkata, India, 4–7 January 2015; pp. 1–6. [Google Scholar]
- Banerjee, A.; Pal, M.; Datta, S.; Tibarewala, D.; Konar, A. Eye movement sequence analysis using electrooculogram to assist autistic children. Biomed. Signal Process. Control. 2014, 14, 134–140. [Google Scholar] [CrossRef]
- Leclair-Visonneau, L.; Oudiette, D.; Gaymard, B.; Leu-Semenescu, S.; Arnulf, I. Do the eyes scan dream images during rapid eye movement sleep? Evidence from the rapid eye movement sleep behaviour disorder model. Brain 2010, 133, 1737–1746. [Google Scholar] [CrossRef] [PubMed]
- Estrada, E.; Nazeran, H.; Barragan, J.; Burk, J.R.; Lucas, E.A.; Behbehani, K. EOG and EMG: Two important switches in automatic sleep stage classification. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 2458–2461. [Google Scholar]
- Yildirim, O.; Baloglu, U.B.; Acharya, U.R. A deep learning model for automated sleep stages classification using PSG signals. Int. J. Environ. Res. Public Health 2019, 16, 599. [Google Scholar] [CrossRef]
- Sokolovsky, M.; Guerrero, F.; Paisarnsrisomsuk, S.; Ruiz, C.; Alvarez, S.A. Deep learning for automated feature discovery and classification of sleep stages. IEEE/ACM Trans. Comput. Biol. Bioinform. 2019, 17, 1835–1845. [Google Scholar] [CrossRef] [PubMed]
- Phan, H.; Andreotti, F.; Cooray, N.; Chén, O.Y.; De Vos, M. SeqSleepNet: End-to-end hierarchical recurrent neural network for sequence-to-sequence automatic sleep staging. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Sekkal, R.N.; Bereksi-Reguig, F.; Ruiz-Fernandez, D.; Dib, N.; Sekkal, S. Automatic sleep stage classification: From classical machine learning methods to deep learning. Biomed. Signal Process. Control. 2022, 77, 103751. [Google Scholar] [CrossRef]
- Toma, T.I.; Choi, S. An End-to-End Convolutional Recurrent Neural Network with Multi-Source Data Fusion for Sleep Stage Classification. In Proceedings of the 2023 International Conference on Artificial Intelligence in Information and Communication (ICAIIC), Bali, Indonesia, 20–23 February 2023; pp. 564–569. [Google Scholar]
- Kaplan, V.; Zhang, J.; Russi, E.; Bloch, K. Detection of inspiratory flow limitation during sleep by computer assisted respiratory inductive plethysmography. Eur. Respir. J. 2000, 15, 570–578. [Google Scholar] [CrossRef]
- Seena, V.; Yomas, J. A review on feature extraction and denoising of ECG signal using wavelet transform. In Proceedings of the 2014 2nd International Conference on Devices, Circuits and Systems (ICDCS), Coimbatore, India, 6–8 March 2014; pp. 1–6. [Google Scholar]
- Silva, C.V.; Philominraj, A.; del Río, C. A DSP Practical Application: Working on ECG Signal. In Applications of Digital Signal Processing; IntechOpen: London, UK, 2011. [Google Scholar]
- Snyder, F.; Hobson, J.A.; Morrison, D.F.; Goldfrank, F. Changes in respiration, heart rate, and systolic blood pressure in human sleep. J. Appl. Physiol. 1964, 19, 417–422. [Google Scholar] [CrossRef]
- Gaiduk, M.; Rodríguez, J.J.P.; Seepold, R.; Madrid, N.M.; Penzel, T.; Glos, M.; Ortega, J.A. Estimation of sleep stages analyzing respiratory and movement signals. IEEE J. Biomed. Health Inform. 2021, 26, 505–514. [Google Scholar] [CrossRef]
- Long, X.; Fonseca, P.; Foussier, J.; Haakma, R.; Aarts, R.M. Sleep and wake classification with actigraphy and respiratory effort using dynamic warping. IEEE J. Biomed. Health Inform. 2013, 18, 1272–1284. [Google Scholar] [CrossRef]
- Fonseca, P.; Long, X.; Radha, M.; Haakma, R.; Aarts, R.M.; Rolink, J. Sleep stage classification with ECG and respiratory effort. Physiol. Meas. 2015, 36, 2027. [Google Scholar] [CrossRef] [PubMed]
- Casal, R.; Di Persia, L.E.; Schlotthauer, G. Classifying sleep–wake stages through recurrent neural networks using pulse oximetry signals. Biomed. Signal Process. Control. 2021, 63, 102195. [Google Scholar] [CrossRef]
- Tripathy, R.; Acharya, U.R. Use of features from RR-time series and EEG signals for automated classification of sleep stages in deep neural network framework. Biocybern. Biomed. Eng. 2018, 38, 890–902. [Google Scholar] [CrossRef]
- Yu, S.; Chen, X.; Wang, B.; Wang, X. Automatic sleep stage classification based on ECG and EEG features for day time short nap evaluation. In Proceedings of the 10th World Congress on Intelligent Control and Automation, Beijing, China, 6–8 July 2012; pp. 4974–4977. [Google Scholar]
- Zhao, R.; Xia, Y.; Wang, Q. Dual-modal and multi-scale deep neural networks for sleep staging using EEG and ECG signals. Biomed. Signal Process. Control. 2021, 66, 102455. [Google Scholar] [CrossRef]
- Willemen, T.; Van Deun, D.; Verhaert, V.; Vandekerckhove, M.; Exadaktylos, V.; Verbraecken, J.; Van Huffel, S.; Haex, B.; Vander Sloten, J. An evaluation of cardiorespiratory and movement features with respect to sleep-stage classification. IEEE J. Biomed. Health Inform. 2013, 18, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Helland, V.F.; Gapelyuk, A.; Suhrbier, A.; Riedl, M.; Penzel, T.; Kurths, J.; Wessel, N. Investigation of an automatic sleep stage classification by means of multiscorer hypnogram. Methods Inf. Med. 2010, 49, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Takatani, T.; Takahashi, Y.; Yoshida, R.; Imai, R.; Uchiike, T.; Yamazaki, M.; Shima, M.; Nishikubo, T.; Ikada, Y.; Fujimoto, S. Relationship between frequency spectrum of heart rate variability and autonomic nervous activities during sleep in newborns. Brain Dev. 2018, 40, 165–171. [Google Scholar] [CrossRef]
- Biswal, S.; Sun, H.; Goparaju, B.; Westover, M.B.; Sun, J.; Bianchi, M.T. Expert-level sleep scoring with deep neural networks. J. Am. Med. Inform. Assoc. 2018, 25, 1643–1650. [Google Scholar] [CrossRef]
- Choi, J.; Kwon, S.; Park, S.; Han, S. Validation of the influence of biosignals on performance of machine learning algorithms for sleep stage classification. Digit. Health 2023, 9, 20552076231163783. [Google Scholar] [CrossRef]
- Cui, Z.; Zheng, X.; Shao, X.; Cui, L. Automatic sleep stage classification based on convolutional neural network and fine-grained segments. Complexity 2018, 2018, 9248410. [Google Scholar] [CrossRef]
- Zhang, L.; Fabbri, D.; Upender, R.; Kent, D. Automated sleep stage scoring of the Sleep Heart Health Study using deep neural networks. Sleep 2019, 42, zsz159. [Google Scholar] [CrossRef] [PubMed]
- Chambon, S.; Galtier, M.N.; Arnal, P.J.; Wainrib, G.; Gramfort, A. A deep learning architecture for temporal sleep stage classification using multivariate and multimodal time series. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 758–769. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Wang, X.; Zhangt, X.; Bin, G.; Jia, Z.; Chen, K. Computation-Efficient Multi-Model Deep Neural Network for Sleep Stage Classification. In Proceedings of the 2020 Asia Service Sciences and Software Engineering Conference, Nagoya, Japan, 13–15 May 2020; pp. 1–8. [Google Scholar]
- Sharma, M.; Yadav, A.; Tiwari, J.; Karabatak, M.; Yildirim, O.; Acharya, U.R. An Automated Wavelet-Based Sleep Scoring Model Using EEG, EMG, and EOG Signals with More Than 8000 Subjects. Int. J. Environ. Res. Public Health 2022, 19, 7176. [Google Scholar] [CrossRef]
- Yuan, Y.; Jia, K.; Ma, F.; Xun, G.; Wang, Y.; Su, L.; Zhang, A. A hybrid self-attention deep learning framework for multivariate sleep stage classification. BMC Bioinform. 2019, 20, 586. [Google Scholar] [CrossRef] [PubMed]
- Satapathy, S.K.; Loganathan, D. Automated classification of multi-class sleep stages classification using polysomnography signals: A nine-layer 1D-convolution neural network approach. Multimed. Tools Appl. 2023, 82, 8049–8091. [Google Scholar] [CrossRef]
- Satapathy, S.K.; Loganathan, D. Multimodal multiclass machine learning model for automated sleep staging based on time series data. SN Comput. Sci. 2022, 3, 276. [Google Scholar] [CrossRef]
- Toma, T.I.; Choi, S. An End-to-End Multi-Channel Convolutional Bi-LSTM Network for Automatic Sleep Stage Detection. Sensors 2023, 23, 4950. [Google Scholar] [CrossRef]
- Pei, W.; Li, Y.; Siuly, S.; Wen, P. A hybrid deep learning scheme for multi-channel sleep stage classification. Comput. Mater. Contin. 2022, 71, 889–905. [Google Scholar]
- Huang, X.; Shirahama, K.; Irshad, M.T.; Nisar, M.A.; Piet, A.; Grzegorzek, M. Sleep Stage Classification in Children Using Self-Attention and Gaussian Noise Data Augmentation. Sensors 2023, 23, 3446. [Google Scholar] [CrossRef]
- Estévez, P.; Held, C.; Holzmann, C.; Perez, C.; Pérez, J.; Heiss, J.; Garrido, M.; Peirano, P. Polysomnographic pattern recognition for automated classification of sleep-waking states in infants. Med. Biol. Eng. Comput. 2002, 40, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Phan, H.; Andreotti, F.; Cooray, N.; Chén, O.Y.; De Vos, M. Joint classification and prediction CNN framework for automatic sleep stage classification. IEEE Trans. Biomed. Eng. 2018, 66, 1285–1296. [Google Scholar] [CrossRef] [PubMed]
- Özdemir, A.; Yavuz, U.; Dael, F.A. Performance evaluation of different classification techniques using different datasets. Int. J. Electr. Comput. Eng. 2019, 9, 3584–3590. [Google Scholar] [CrossRef]
- Laber, E.S.; Pereira, F.d.A.M. Splitting criteria for classification problems with multi-valued attributes and large number of classes. Pattern Recognit. Lett. 2018, 111, 58–63. [Google Scholar] [CrossRef]
- Tougui, I.; Jilbab, A.; El Mhamdi, J. Impact of the choice of cross-validation techniques on the results of machine learning-based diagnostic applications. Healthc. Inform. Res. 2021, 27, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Shinde, P.P.; Shah, S. A review of machine learning and deep learning applications. In Proceedings of the 2018 Fourth International Conference on Computing Communication Control and Automation (ICCUBEA), Pune, India, 16–18 August 2018; pp. 1–6. [Google Scholar]
- Utomo, O.K.; Surantha, N.; Isa, S.M.; Soewito, B. Automatic sleep stage classification using weighted ELM and PSO on imbalanced data from single lead ECG. Procedia Comput. Sci. 2019, 157, 321–328. [Google Scholar] [CrossRef]
- Page, A.; Turner, J.; Mohsenin, T.; Oates, T. Comparing raw data and feature extraction for seizure detection with deep learning methods. In Proceedings of the Twenty-Seventh International Flairs Conference, Pensacola Beach, FL, USA, 21–23 May 2014. [Google Scholar]
- Jain, A.; Zongker, D. Feature selection: Evaluation, application, and small sample performance. IEEE Trans. Pattern Anal. Mach. Intell. 1997, 19, 153–158. [Google Scholar] [CrossRef]
- Ahmed, H.O.A.; Nandi, A.K. Vibration Image Representations for Fault Diagnosis of Rotating Machines: A Review. Machines 2022, 10, 1113. [Google Scholar] [CrossRef]









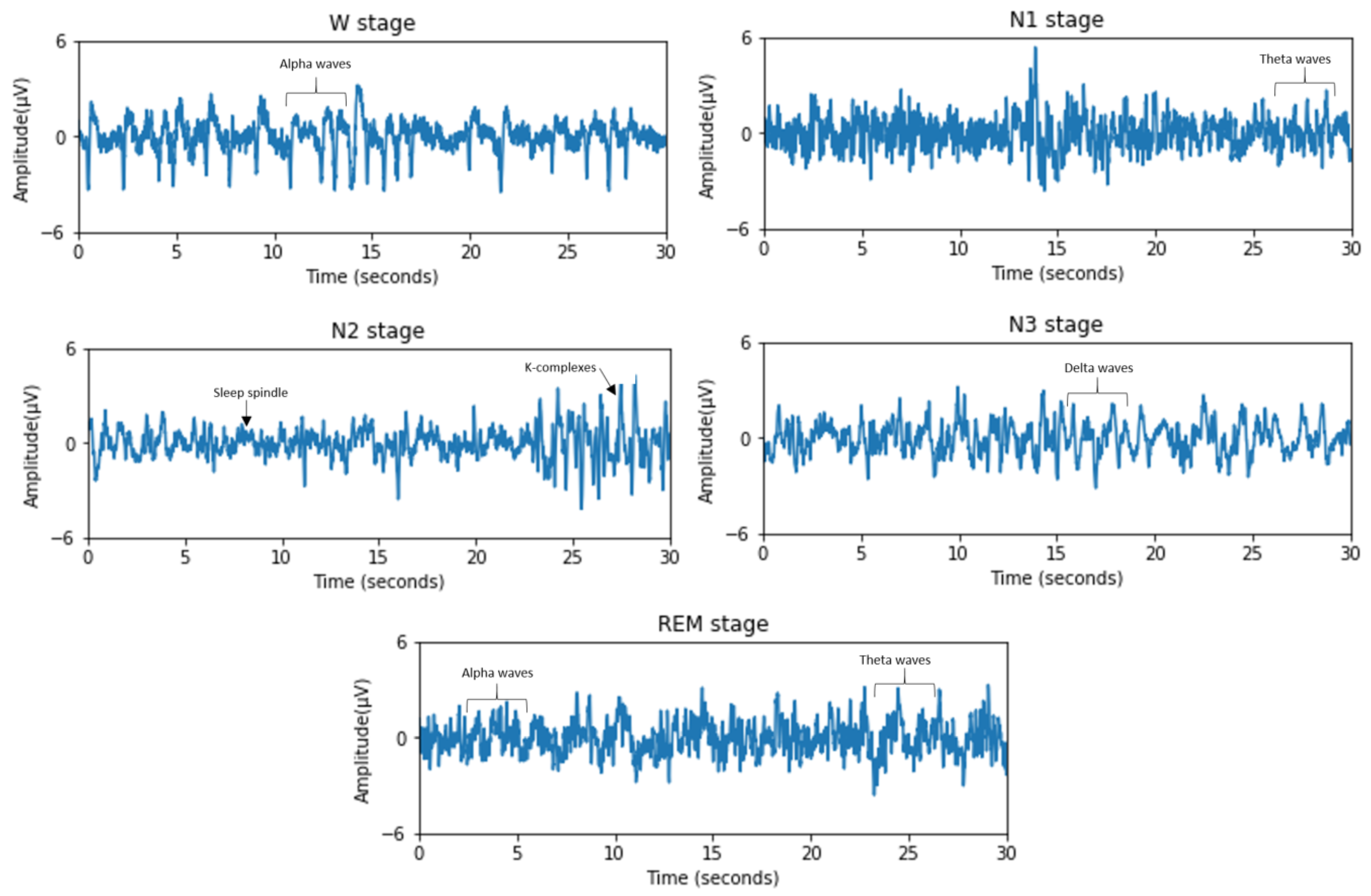
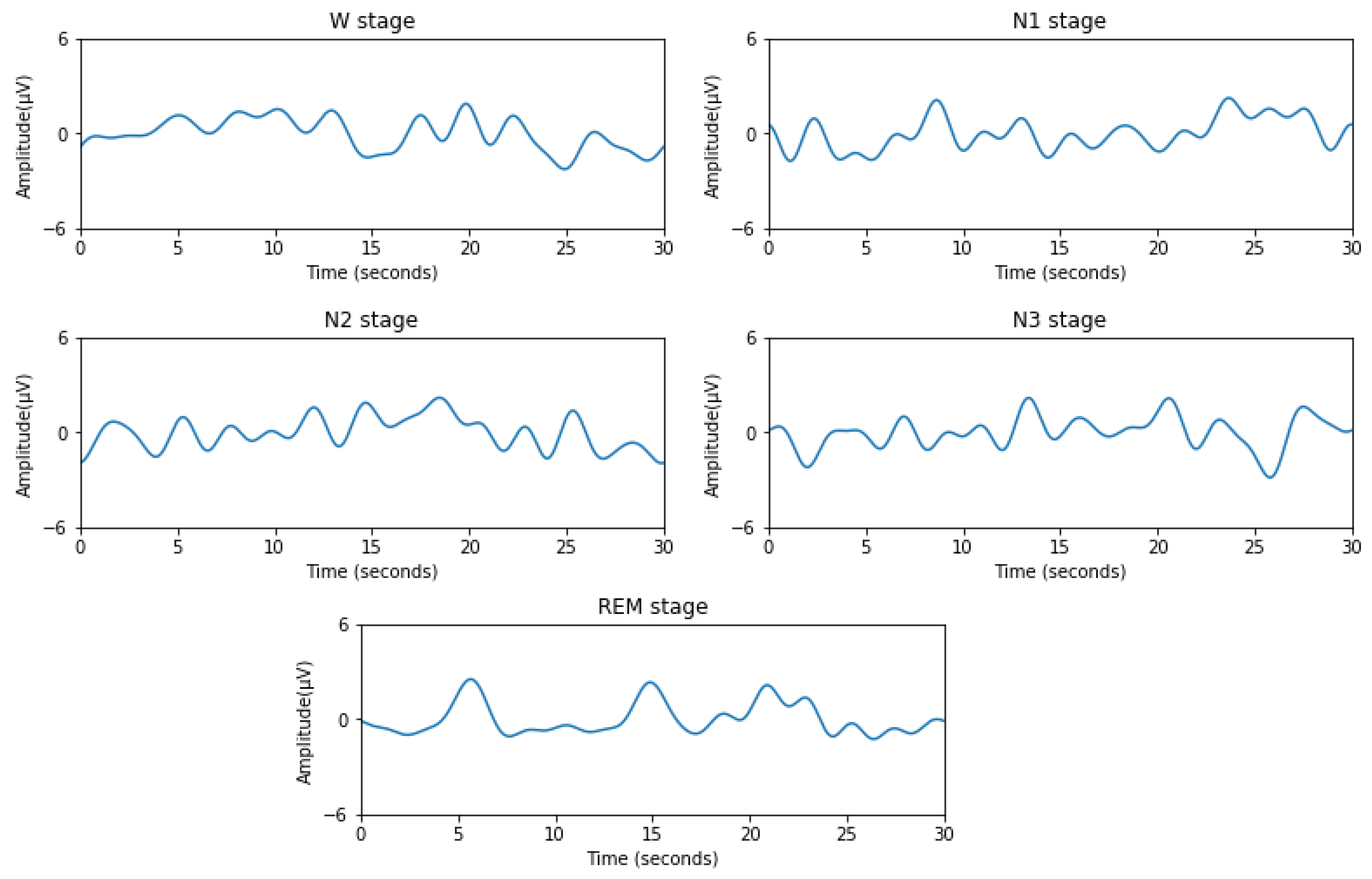
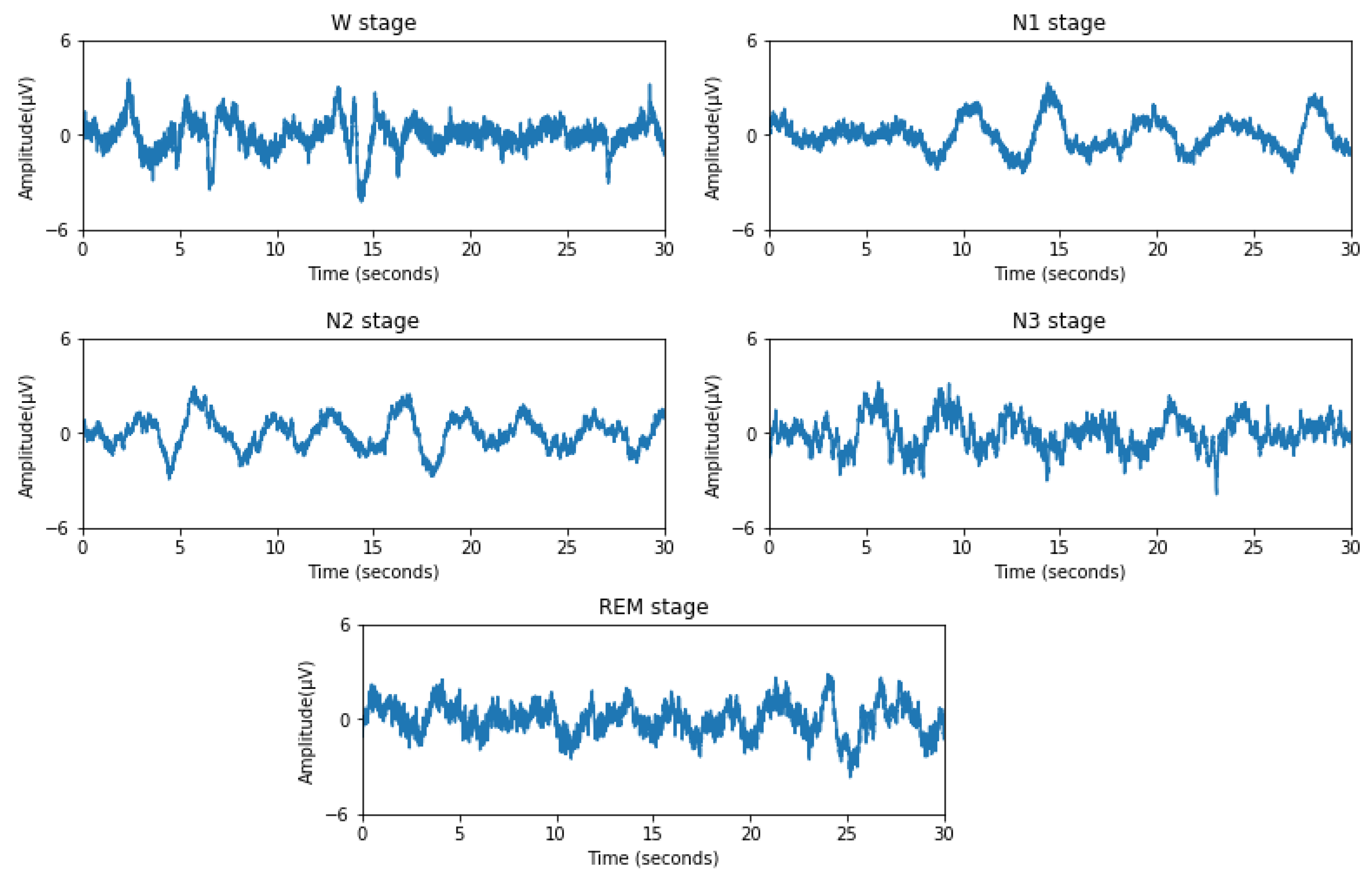
| Sleep Stage | Characteristic Frequency |
|---|---|
| W | Alpha (8–12 Hz) |
| N1 | Theta (4–8 Hz) |
| N2 | Spindle and K-complexes (12–15 Hz) |
| N3 | Delta (0.5–4 Hz) |
| REM | Alpha (8–12 Hz) Theta (4–8 Hz) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almutairi, H.; Hassan, G.M.; Datta, A. Machine-Learning-Based-Approaches for Sleep Stage Classification Utilising a Combination of Physiological Signals: A Systematic Review. Appl. Sci. 2023, 13, 13280. https://doi.org/10.3390/app132413280
Almutairi H, Hassan GM, Datta A. Machine-Learning-Based-Approaches for Sleep Stage Classification Utilising a Combination of Physiological Signals: A Systematic Review. Applied Sciences. 2023; 13(24):13280. https://doi.org/10.3390/app132413280
Chicago/Turabian StyleAlmutairi, Haifa, Ghulam Mubashar Hassan, and Amitava Datta. 2023. "Machine-Learning-Based-Approaches for Sleep Stage Classification Utilising a Combination of Physiological Signals: A Systematic Review" Applied Sciences 13, no. 24: 13280. https://doi.org/10.3390/app132413280