
Acute Effects of Padel Match Play on Circulating Substrates, Metabolites, Energy Balance Enzymes, and Muscle Damage Biomarkers: Sex Differences

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Approach
2.3. Blood Sampling
2.4. Hematological and Biochemical Assessment
2.5. Statistical Analysis
3. Results
3.1. Participant’s Characteristics and Cardiorespiratory Fitness
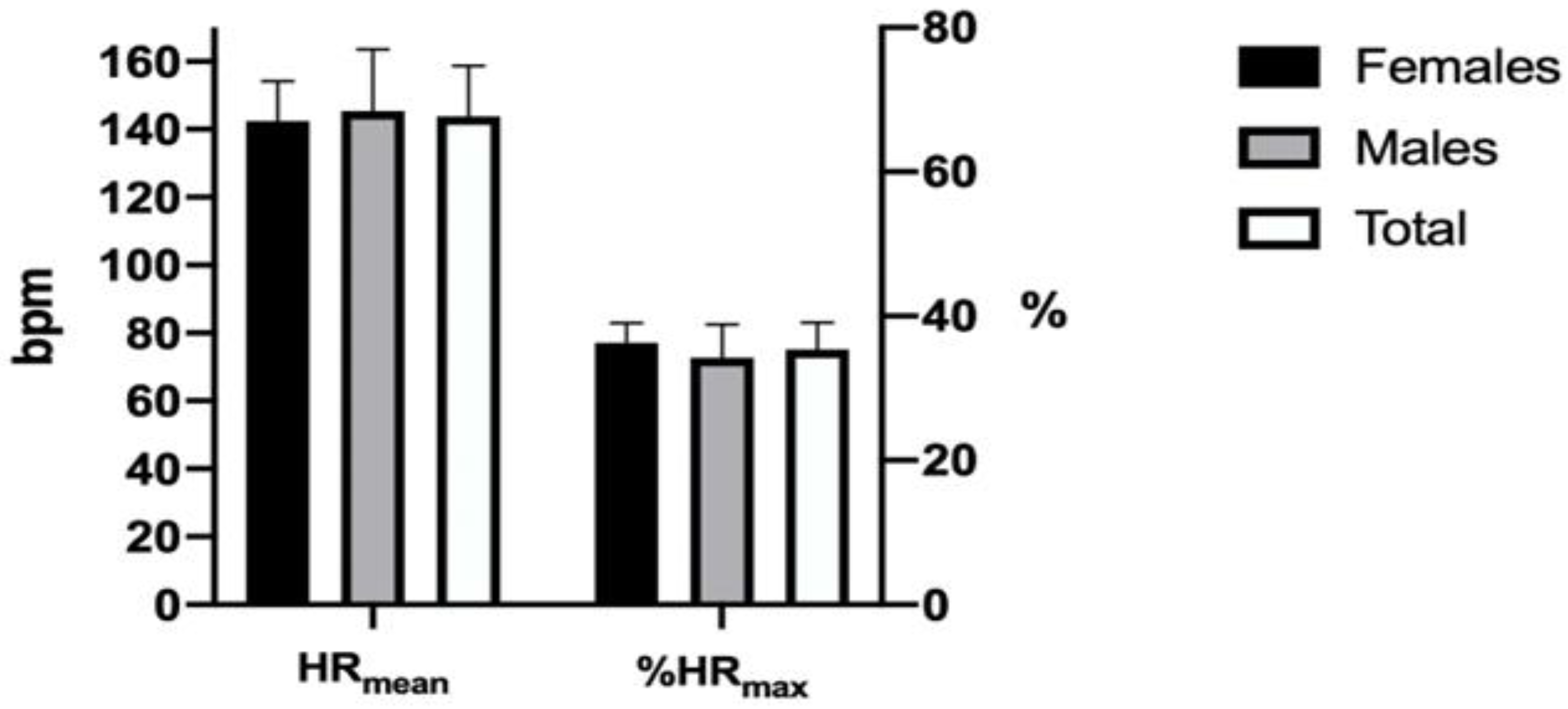
3.2. Characteristics of Simulated Padel Competition
3.3. Biochemical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Padel Federation. Available online: https://www.padelfip.co (accessed on 15 January 2022).
- Carrasco, L.; Romero, S.; Sanudo, B.; de Hoyo, M. Game analysis and energy requirements of paddle tennis competition. Sci. Sports 2011, 26, 338–344. [Google Scholar] [CrossRef]
- García-Giménez, A.; Pradas de la Fuente, F.; Castellar Otín, C.; Carrasco Paez, L. Performance Outcome Measures in Padel: A Scoping Review. Int. J. Environ. Res. Public. Health 2022, 19, 4395. [Google Scholar] [CrossRef]
- Sánchez-Muñoz, C.; Muros, J.J.; Cañas, J.; Courel-Ibáñez, J.; Sánchez-Alcaraz, B.J.; Zabala, M. Anthropometric and physical fitness profiles of world-class male padel players. Int. J. Environ. Res. Public. Health 2020, 17, 508. [Google Scholar] [CrossRef] [PubMed]
- Courel-Ibáñez, J.; Llorca-Miralles, J. Physical fitness in young padel players: A cross-sectional study. Int. J. Environ. Res. Public. Health 2021, 18, 2658. [Google Scholar] [CrossRef] [PubMed]
- Pradas, F.; Sanchez-Pay, A.; Munoz, D.; Sanchez-Alcaraz, B.J. Gender Differences in Physical Fitness Characteristics in Professional Padel Players. Int. J. Environ. Res. Public. Health 2021, 18, 5967. [Google Scholar] [CrossRef] [PubMed]
- Pradas, F.; Cádiz, M.P.; Nestares, M.T.; Martínez-Díaz, I.C.; Carrasco, L. Effects of Padel Competition on Brain Health-Related Myokines. Int. J. Environ. Res. Public. Health 2021, 18, 6042. [Google Scholar] [CrossRef]
- Bartolomé, I.; Córdoba, L.; Crespo, C.; Grijota, F.; Maynar, M.; Muñoz, D. Effects of a paddle match on the urinary excretion of trace minerals in high-level players. Sci. Sport 2016, 31, e131–e137. [Google Scholar] [CrossRef]
- Pradas, F.; Garcia-Gimenez, A.; Toro-Roman, V.; Sanchez-Alcaraz, B.J.; Ochiana, N.; Castellar, C. Effect of a Padel Match on Biochemical and Haematological Parameters in Professional Players with Regard to Gender-Related Differences. Sustainability 2020, 12, 8633. [Google Scholar] [CrossRef]
- Pradas, F.; García-Giménez, A.; Toro-Román, V.; Ochiana, N.; Castellar, C. Gender differences in neuromuscular, haematological, and urinary responses during padel matches. Int. J. Environ. Res. Public. Health 2021, 18, 11859. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010. [Google Scholar]
- Forest, J.C.; Burtis, C.A. Development of Reference Methods and Reference Materials by the IFCC: An Overview. EJIFCC 2001, 13, 71–72. [Google Scholar]
- Dill, D.B.; Costill, D.L. Calculation of percentage changes in volumes of blood, plasma, and red cells in dehydration. J. Appl. Physiol. 1974, 37, 247–248. [Google Scholar] [CrossRef]
- Matomäki, P.; Kainulainen, H.; Kyröläinen, H. Corrected whole blood biomarkers–the equation of Dill and Costill revisited. Physiol. Rep. 2018, 6, e13749. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Earlbaum Associates: Hillsdale, MI, USA, 1988. [Google Scholar]
- Amieba, C.; Salinero Martín, J.J. Overview of paddle competition and its physiological demands. AGON Int. J. Sport Sci. 2013, 3, 60–67. [Google Scholar]
- Priego, J.I.; Melis, J.O.; Llana-Belloch, S.; Pérezsoriano, P.; García, J.C.G.; Almenara, M.S. Padel: A Quantitative study of the shots and movements in the high-performance. J. Hum. Sport. Exerc. 2013, 8, 925–931. [Google Scholar] [CrossRef]
- Castillo-Rodriguez, A.; Alvero-Cruz, J.R.; Hernandez-Mendo, A.; Fernandez-Garcia, J.C.; Castillo-Rodríguez, A.; Alvero-Cruz, J.R. Physical and physiological responses in Paddle Tennis competition. Int. J. Perform. Anal. Sport. 2014, 14, 524–534. [Google Scholar] [CrossRef]
- Courel-Ibanez, J.; Sánchez-Alcaraz, B.J.; Muñoz, D. Exploring Game Dynamics in Padel: Implications for Assessment and Training. J. Strength. Cond. Res. 2019, 33, 1971–1977. [Google Scholar] [CrossRef] [PubMed]
- García-Benítez, S.; Courel-Ibáñez, J.; Pérez-Bilbao, T.; Felipe, J.L.; Courel-Ibáñez, J. Game Responses During Young Padel Match Play: Age and Sex Comparisons. J. Strength. Cond. Res. 2018, 32, 1144–1149. [Google Scholar] [CrossRef] [PubMed]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint Position Statement. Diabetes Care 2010, 33, 60–67. [Google Scholar]
- Marliss, E.B.; Vranic, M. Intense exercise has unique effects on both insulin release and its roles in glucoregulation: Implications for diabetes. Diabetes 2002, 51 (Suppl. S1), 271–283. [Google Scholar] [CrossRef]
- Peter Adams, O. The impact of brief high-intensity exercise on blood glucose levels. Diabetes Metab. Syndr. Obes. 2013, 6, 113–122. [Google Scholar] [CrossRef]
- Bodell, N.; Gillum, T. 90 Minutes of Moderate-Intensity Exercise does not Attenuate Postprandial Triglycerides in Older Adults. Int. J. Exerc. Sci. 2016, 9, 677–684. [Google Scholar]
- Kelly, R.S.; Kelly, M.P.; Kelly, P. Metabolomics, physical activity, exercise and health: A review of the current evidence. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165936. [Google Scholar] [CrossRef]
- Calles-Escandon, J.; Cunningham, J.J.; Snyder, P.; Jacob, R.; Huszar, G.; Loke, J.; Felig, P. Influence of exercise on urea, creatinine, and 3-methylhistidine excretion in normal human subjects. Am. J. Physiol. 1984, 246 Pt 1, E334–E338. [Google Scholar] [CrossRef] [PubMed]
- Banfi, G.; Del Fabbro, M.; Lippi, G. Serum creatinine concentration and creatinine-based estimation of glomerular filtration rate in athletes. Sport. Med. 2009, 39, 331–337. [Google Scholar] [CrossRef]
- Welsh, R.; Warburton, D.E.R.; Haykowksy, M.J. Hematological response to the half ironman triathlon [abstract]. Med. Sci. Sports Exerc. 1999, 31, s63. [Google Scholar] [CrossRef]
- Banfi, G.; Colombini, A.; Lombardi, G.; Lubkowska, A. Metabolic Markers in Sports Medicine. In Advances in Clinical Chemistry, 1st ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2012; Volume 56, pp. 1–54. [Google Scholar]
- McKune, A.; Semple, S.J.; Peters-Futre, E.M. Acute exercise-induced muscle injury. Biol. Sport. 2012, 29, 3–10. [Google Scholar] [CrossRef]
- Brancaccio, P.; Limongelli, F.M.; Maffulli, N. Monitoring of serum enzymes in sport. Br. J. Sports Med. 2006, 40, 96–97. [Google Scholar] [CrossRef]
- Sorichter, S.; Mair, J.; Koller, A.; Pelsers, M.M.; Puschendorf, B.; Glatz, J.F.C. Early assesment of exercise induced skeletal muscle injury using plasma fatty acid binding protein. Br. J. Sports Med. 1998, 32, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Pelsers, M.M.; Chapelle, J.P.; Knapen, M.; Vermeer, C.; Muijtjens, A.M.; Hermes, W.T.; Glatz, J.F. Influence of age and sex and day-to-day and within-day biological variation on plasma concentrations of fatty acid-binding protein and myoglobin in healthy subjects. Clin. Chem. 1999, 45, 441–443. [Google Scholar]
- Ishimura, S.; Furuhashi, M.; Watanabe, Y.; Hoshina, K.; Fuseya, T.; Mita, T.; Okazaki, Y.; Koyama, M.; Tanaka, M.; Akasaka, H.; et al. Circulating levels of fatty acid-binding protein family and metabolic phenotype in the general population. PLoS ONE 2013, 8, 2–8. [Google Scholar] [CrossRef]
- Oosthuyse, T.; Bosch, A.N. The Effect of the Menstrual Cycle on Exercise Metabolism. Sports Med. 2010, 40, 207–227. [Google Scholar] [CrossRef] [PubMed]
- Lavoie, J.M.; Dionne, N.; Helie, R.; Brisson, G.R. Menstrual cycle phase dissociation of blood glucose homeostasis during exercise. J. Appl. Physiol. 1987, 62, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Romero-Parra, N.; Cupeiro, R.; Alfaro-Magallanes, V.M.; Rael, B.; Rubio-Arias, J.Á.; Peinado, A.B.; Benito, P.J. Exercise-induced muscle damage during the menstrual cycle: A systematic review and meta-analysis. J. Strength. Cond. Res. 2021, 35, 549–561. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Females | Males | Total | Sig. (CI = 95%) | Effect Size (d) | |
|---|---|---|---|---|---|
| Age (years) | 29.0 ± 3.8 | 25.2 ± 7.9 | 27.3 ± 6.2 | p = 0.169 | 0.61 |
| Height (cm) | 167.1 ± 5.6 | 176.6 ± 2.4 | 171.4 ± 6.5 | p < 0.001 | 2.20 |
| Weight (kg) | 60.7 ± 4.5 | 77.0 ± 6.5 | 68.0 ± 9.9 | p < 0.001 | 2.91 |
| BMI (kg/m2) | 21.7 ± 1.0 | 24.6 ± 1.8 | 23.0 ± 2.0 | p < 0.001 | 1.99 |
| Body fat (%) | 20.2 ± 2.1 | 13.3 ± 5.4 | 17.1 ± 5.2 | p = 0.001 | 1.68 |
| Muscle mass (%) | 37.1 ± 2.9 | 43.8 ± 1.8 | 40.1 ± 4.2 | p < 0.001 | 2.77 |
| VO2max (L/min) | 2.89 ± 0.39 | 4.41 ± 0.53 | 3.57 ± 0.89 | p < 0.001 | 3.27 |
| HRmax (bpm) | 186.3 ± 7.8 | 188.3 ± 11.3 | 187.2 ± 9.3 | p = 0.636 | 0.21 |
| Biomarkers | Female Players | Females Intragroup Contrast | Male Players | Males Intragroup Contrast | Total Players | Total Intergroup Contrast | Sex Intergroup Contrast |
|---|---|---|---|---|---|---|---|
BG pre BG post | 89.15 ± 11.93 (81.94–96.36) 98.23 ± 16.99 (87.96–108.49) | a p = 0.118 d = 0.84 | 92.78 ± 11.04 (84.29–101.27) 92.78 ± 13.40 (82.47–103.08) | a p = 1 d = 0 | 90.64 ± 11.45 (85.56–95.71) 96.00 ± 15.52 (89.12–102.88) | a p = 0.161 d = 0.39 | a p = 0.527 d = 0.31 a p = 0.431 d = 0.36 |
TGs pre TGs post | 96.07 ± 61.93 (58.65–133.50) 82.23 ± 62.70 (44.34–120.12) | b p = 0.116 d = 0.22 | 117.33 ± 73.339 (60.96–173.70) 107.89 ± 75.39 (49.94–165.84) | b p = 0.553 d = 0.13 | 104.77 ± 65.99 (75.51–134.03) 92.73 ± 67.66 (62.72–122.73) | c p = 0.94 d = 0.18 | c p = 0.401 d = 0.31 c p = 0.395 d = 0.37 |
Cr pre Cr post | 0.78 ± 0.08 (0.73–0.83) 0.88 ± 0.12 (0.81–0.95) | a p < 0.001 d = 0.98 | 1.06 ± 0.12 (0.97–1.16) 1.21 ± 0.11 (1.12–1.29) | a p < 0.001 d = 1.30 | 0.90 ± 0.17 (0.82–0.97) 1.01 ± 0.20 (0.92–1.10) | a p < 0.001 d = 0.59 | a p < 0.001 d = 2.74 a p < 0.001 d = 2.87 |
Urea pre Urea post | 34.70 ± 8.04 (29.83–39.55) 39.00 ± 9.42 (33.31–44.69) | a p < 0.001 d = 0.49 | 40.33 ± 8.38 (33.89–46.77) 45.89 ± 8.58 (39.29–52.48) | a p < 0.001 d = 0.65 | 37.00 ± 8.47 (33.24–40.76) 41.82 ± 9.52 (37.59–46.04) | a p < 0.001 d = 0.53 | a p = 0.112 d = 0.68 a p = 0.123 d = 0.76 |
LDL pre LDL post | 29.54 ± 16.79 (19.39–39.68) 30.54 ± 17.29 (20.09–40.99) | b p = 0.033 d = 0.06 | 22.11 ± 10.03 (14.40–29.82) 20.44 ± 9.49 (13.15–27.74) | b p = 0.040 d = 0.17 | 26.50 ± 14.61 (20.02–32.98) 26.41 ± 15.20 (19.67–33.15) | c p = 0.003 d = 0 | c p = 0.269 d = 0.54 c p = 0.128 d = 0.72 |
| CK pre CK post | 115.54 ± 62.93 (77.51–153.56) 147.23 ± 97.88 (88.08–206.38) | b p = 0.001 d = 0.38 | 262.89 ± 189.02 (117.59–408.18) 308.22 ± 187.12 (164.39–452.06) | b p = 0.008 d = 0.24 | 175.82 ± 146.19 (110.99–240.64) 213.09 ± 159.30 (142.46–283.72) | c p < 0.001 d = 0.24 | c p = 0.012 d = 1.04 c p = 0.016 d = 1.08 |
LDH pre LDH post | 170.38 ± 25.28 (155.11–185.66) 182.69 ± 20.92 (170.05–195.33) | a p = 0.008 d = 0.53 | 231.22 ± 30.44 (207.83–254.62) 249.67 ± 38.75 (219.87–279.46) | a p = 0.066 d = 0.53 | 195.27 ± 40.69 (177.23–213.31) 210.09 ± 44.25 (190.47–229.71) | a p = 0.002 d = 0.35 | a p < 0.001 d = 2.17 a p < 0.001 d = 2.15 |
FABP-3 pre FABP-3 post | 1667.69 ± 597.78 (1306.45–2028.93) 3218.73 ± 1921.99 (2062.71–4374.74) | b p = 0.004 d = 1.09 | 1945.57 ± 590.78 (1491.45–2399.69) 3848.12 ± 890.16 (3163.88–4532.36) | b p < 0.001 d = 2.52 | 1781.37 ± 597.26 (1516.56–2046.18) 3476.21 ± 1579.04 (2776.10–4176.31) | c p < 0.001 d = 1.42 | c p = 0.389 d = 0.47 c p = 0.376 d = 0.42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pradas de la Fuente, F.; Cádiz, M.P.; Moreno-Azze, A.; Martínez-Díaz, I.C.; Carrasco, L. Acute Effects of Padel Match Play on Circulating Substrates, Metabolites, Energy Balance Enzymes, and Muscle Damage Biomarkers: Sex Differences. Appl. Sci. 2023, 13, 13281. https://doi.org/10.3390/app132413281
Pradas de la Fuente F, Cádiz MP, Moreno-Azze A, Martínez-Díaz IC, Carrasco L. Acute Effects of Padel Match Play on Circulating Substrates, Metabolites, Energy Balance Enzymes, and Muscle Damage Biomarkers: Sex Differences. Applied Sciences. 2023; 13(24):13281. https://doi.org/10.3390/app132413281
Chicago/Turabian StylePradas de la Fuente, Francisco, María Pía Cádiz, Alejandro Moreno-Azze, Inmaculada C. Martínez-Díaz, and Luis Carrasco. 2023. "Acute Effects of Padel Match Play on Circulating Substrates, Metabolites, Energy Balance Enzymes, and Muscle Damage Biomarkers: Sex Differences" Applied Sciences 13, no. 24: 13281. https://doi.org/10.3390/app132413281