1. Introduction
Mandibular laterodeviation is a condition in which the mandible and maxilla of a patient are not perfectly aligned, presenting a lateral deviation. There are two main methods for treating mandibular laterodeviation: non-surgical treatment (fixed and removable orthodontic appliances) and surgical treatment (orthopedic surgery and orthognathic surgery) [
1]. On the basis of the etiology, they can be divided into structural or functional, and the latter is distinguished from the former both because they recognize different causes of origin and for the lack of lesions or structural alterations; the jaw, in case of precontact, to find the occlusal boarding, rising from the resting position, moves laterally to avoid the occlusal interference by establishing an avoidance reflex and modifying its starting position [
2]. Functional lateral deviation can be the effect of a cross or a scissor bite due to the reduction of the transverse diameter of the palate, but could also be due to a neuromuscular asymmetry because of birth trauma associated with muscular torticollis and/or ocular defects [
3,
4,
5,
6,
7]. The traditional diagnosis of functional lateral deviation is based on a clinical evaluation and dental casts, supported by an instrumental analysis through X-rays in the postero–anterior projection; however, these diagnostic techniques do not provide any information about the neuromuscular system [
8,
9].
Among the parameters used for orthodontic diagnostic evaluation, the vertical dimension of occlusion, the antero–posterior and latero–lateral reciprocal relationship of the dental arches are of fundamental clinical importance. Variations in the spatial relationship between the upper and lower arches, compared to ideal standards, are relevant factors in the design of the orthodontic treatment plan [
10]
Typically, orthodontic treatment of a functional lateral deviation consists of therapy with different devices that align the jaw.
Often, orthodontic treatment, despite possible immediate aesthetic success, determines a constrained occlusal position that could determine long-term stability problems; occlusion does not require neuromuscular adaptation, but rather, orthodontic treatment must adapt to the neuromuscular system and not vice versa [
11,
12].
One of the possible hypotheses regarding the instability of orthodontic results could be that the neuromuscular balance was not taken into account during the diagnosis and treatment of laterodeviations. Thus, orthodontic treatment could achieve an aesthetic result at the expense of neuromuscular balance. This could lead to instability of the result in the medium and long term. In general terms, it could be suggested that orthodontic therapy should achieve an occlusion that does not require neuromuscular adaptation and that the therapy itself should adapt to the neuromuscular system.
Several years ago, some authors stressed the importance of the mandibular rest position and its reproducibility as a diagnostic reference [
13,
14].
According to this idea, the mandibular rest position is largely determined by the spatial position in which the occlusal contact occurs. Therefore, the mandibular rest position is usually ”adapted” by the neuromuscular system, which will keep the mandible in a position appropriate for stomatognathic functions. A recent literature review indicates that there is strong clinical evidence that Rest Mandible Position (RMP), Rest Vertical Dimension (RVD), and the Interocclusal Dimension (IOD) are to be found within a three-dimensional spatial “range” largely determined by the active adaptation of the neuromuscular system [
15].
This adaptation is extensive, but in specific cases, probably associated with other not necessarily occlusal components, dimensional variations may go beyond the limits of muscular compensation and induce occlusal instability and/or acute and chronic suffering [
16,
17].
The basic idea of these observations is that starting from a relaxed neuromuscular resting position of the mandible, it is possible, by comparing it with the habitual occlusion, to assess the three-dimensional occlusal space in which the contact between the jaws should take place without an adaptation effort of the stomatognathic musculature.
The use of dental ULFTENS is among the techniques used to achieve muscle relaxation and a resting position of the jaw. Dental ULFTENS belongs to the category of TENS that involves, in a general sense, the cutaneous stimulation of nerve branches located more proximally to the electrode application site. The mechanism of action of such stimulation has been extensively studied and demonstrated and involves, depending on the frequency of delivery, the intervention of different response modulation centers. Stimulation with frequencies below 20 Hz is referred to as low-frequency TENS, and below 4 Hz is referred to as ultra-low-frequency TENS, also called “acupuncture-like” in some cases [
18,
19]. In the case of low and ultra-low-frequency TENS, a central mechanism of action mediated by the prefrontal cortex and the ventrolateral PAG has been suggested. This action involves, among others, an endorphinic activity at the PAG level, a peripheral response characterized by modulation of central pain pathways, and a reduction in muscle tone together with a lowering of sympathetic tone [
20]. Transcutaneous electrical nerve stimulation and conditioned pain modulation influence the perception of pain in humans [
21].
Dental ULFTENS consists of transcutaneous electrical stimulation with an electrostimulation of the V and VII pairs of cranial nerves. It is performed through the application of electrodes bilaterally at the level of the area anterior to the tragus. The stimulation frequency is of the order of 0.66, which is why it belongs to the ultra-low category, and the amplitude of this stimulation is such that it evokes a minimal passive upward movement of the jaw. This is determined by the direct action of the impulse that reaches deep into the mandibular branch of the trigeminal, through the coronoid incisura, exciting its motor fibers and causing peripherally in a dromic way a contraction of the elevator muscles of the mandible. In this way, it would act according to a central mechanism as mentioned above and associate an automatic peripheral muscular upward movement of the mandible. Dental ULFTENS has been shown to be able to reduce the myoelectric activity of the masseter and anterior temporalis muscles in a resting position [
22]. This technique of muscle stimulation and relaxation has already been used to evaluate sagittal relationships in an orthodontic population characterized as Class II division I with mandible dentoalveolar retrusion and allows for visualizing an unusual trend of growth. The work suggested that different orthodontic diagnoses can be hypothesized through ULFTENS depending on the individual subject’s characteristic neuromuscular vector [
1], in particular, through sensory amplitude stimulation, which is less uncomfortable for young patients [
23]. It is therefore possible to hypothesize treatments aimed at the neuromuscular structure of the individual independently of the classical malocclusion pattern based on clinical, model, and radiogram observations. At this present time, there are no observations regarding the effects on the lateral plane of acutely administered ULFTENS in orthodontically aged subjects characterized by functional laterodeviation. It is conceivable that, as with the effects of ULFTENS in the sagittal plane, responses can be observed that are guided by the neuromuscular vector of the individual subject, irrespective of the type or direction of laterodeviation classified statically by clinical observation, plaster models, and radiograms.
The primary objective of TENS is to decondition and relax the muscles of the jaw and face in order to identify and establish the mandibular rest position with stomatognathic muscles relaxed. The aim of this study is the evaluation of changes in the occlusal position of the jaw after the relaxation procedure operated through the use of ULFTENS (ultra-low-frequency transcutaneous electric nervous stimulation) in children with diagnosed functional mandibular lateral deviation.
2. Material and Methods
This study was carried out according to the principles of the Helsinki Declaration. The University Ethics Committee approved the following project (16137/2016). Initially, in this study, 130 subjects between the ages of 8 and 13 were visited by the same operator at the dental clinic of the University of L’Aquila.
The inclusion criteria were as follows:
Deviated chin from midsagittal plane (considering a plane drawn perpendicular to the bipupillary line and the commissural line);
Misalignment between the upper and lower frenulum;
Asymmetries between the upper and lower interincisal lines and between the molar and canine classes;
Deviation of the median line in maximum intercuspidation, and in a resting position;
Deviation of the jaw during mouth opening;
Noises and “tenderness” of the temporomandibular joint,
No orthodontic treatment performed prior to the visit;
Deviation of the midline of the anterior teeth > 1.5 mm with open mouth alignment.
The exclusion criteria were as follows:
Absence of written informed consent from parents/legal guardians;
Presence of systemic diseases;
Presence of epilepsy and/or pacemaker;
Presence of skeletal asymmetry;
Presence of posterior or lateral cross bite;
Absence of congenital torticollis at birth;
Presence of metabolic problems, or systemic or infectious diseases of the mother in the gestational period and drug or medication intake;
Absence of dystocic delivery or preceded by the use of vasosuprine or oxytocin, and absence of traumatic practices during delivery (e.g., forceps) or breech delivery;
Absence of major trauma to the face, skull, and neck during childhood that required medical intervention.
In the end, 60 patients were enrolled in this study (mean age 10.1 ± 0.81), and the protocol used was the one described below.
2.1. Experimental Protocol
Neuromuscular recording was performed on 60 patients. First, alginate impressions of the upper and lower arches were taken and accurate dental casts were made for each patient. The midline asymmetry was measured in relation to the upper and lower incisal midline. Secondly, the discrepancy of the midline with respect to the upper and lower interincisal lines was evaluated. For each plaster model then, reference points were highlighted: a line that goes from the interincisal point of the maxilla up to the mandible, and a line on the right and left molar side on the horizontal plane.
Later TENS was applied to relax the musculature and thus determine the rest position of the mandible, which was then measured and recorded.
TENS was administered using an electro-stimulator specifically designed for dentistry called Myomonitor J5 (J5, Myotronics, Kent, WA, USA,
https://www.myotronics.com/j5, accessed on 4 December 2023).
The electrical pulse delivered has a frequency of 0.66 Hz, which is why this type of stimulation is also called ULF (ultra-low frequency) TENS. The duration of the impulse is less than 500 μs, and the amplitude is such that it does not evoke the upward movement of the mandible during the preparation phase (5 min) prior to recording the cranial jaw relationship. This amplitude of stimulation, defined as sensory amplitude, has been shown to be sufficient in inducing a reduction in the surface emg values of the anterior temporal and masseter muscles comparable to that obtained with motor amplitude ULFTENS, which requires a greater amplitude of stimulation and, therefore, more discomfort for the recipient. Stimulation is transferred to the subject by means of three electrodes, one positioned posteriorly on the neck (below the hairline, on the midline) and the other two anterior to the tragus, one on the right and the other on the left. The electrode on the back of the neck is the positive end of the stimulating circuit, while the negative end is split into the two anterior electrodes to allow symmetrical and simultaneous stimulation (
Figure 1).
The stimulation protocol involves 5 min of sensory amplitude stimulation, then the person is asked to open the mouth and a previously prepared occlusal registration material is injected onto the occlusal surfaces with a disposable syringe without needle. In our case, this is a dental resin (Sapphire™ Acrylic Peripheral Impression Material, Keystone Industries, Gibbstown, NJ, USA,
https://dental.keystoneindustries.com/product/sapphire-acrylic-peripheral-impression-material/, accessed on 7 December 2023).
The patient is asked to close the mouth and gently pull the lips together without manipulating the jaw or the face. One waits a minute for the jaw to return to the rest position obtained with ULFTENS and increases the amplitude of the impulse until a slight automatic upward movement of the jaw towards the upper jaw is obtained. This movement determines the impression of the teeth of the upper jaw in the resin placed on the occlusal surface. When the resin has a plastic consistency (approx. 1 min) it is removed from the mouth and placed on the plaster models awaiting its complete hardening.
At this point, the child is discharged. When hardening is complete, the models are mounted on the Galetti articulator(Sevtis-Fisat s.r.l. Plastic Technology, Tianjin, China). In
Figure 2, there is shown a patient who does not change her position after TENS [
1,
24].
With dental casts mounted in the articulator in the myocentric position with the interposed print, the change from the occlusal position was evaluated considering the initial reference lines; it was then calculated in millimeters and analyzed by a digital caliper. All measurements were performed twice, and the examiner’s error was examined using the formula s(i) = √Σd2/2n. The intra observer methodological error s(i) was calculated from duplicated recordings. S denotes the variance of the total sample of 60.
2.2. Statistical Analysis
The Stata package was used to perform a paired t-test for independent samples comparing mean and variance shifts of the midline, right molar side, and left molar side. Differences with a value of p < 0.05 were regarded as significant. A correlative tendency was analyzed with Pearson’s correlation coefficient (r). A value of r equal to or greater than 0.65 was considered a positive correlation. Two sample proportion tests were carried out on movement direction comparing left or right shifts on the midline, with those on the right and left molar sides. Differences with a value of p < 0.05 were regarded as positively correlated. One sample proportion test was performed on each measurement (midline, right molar side, left molar side) considering 0.5 (50%) as the probability of left or right shift.
3. Results
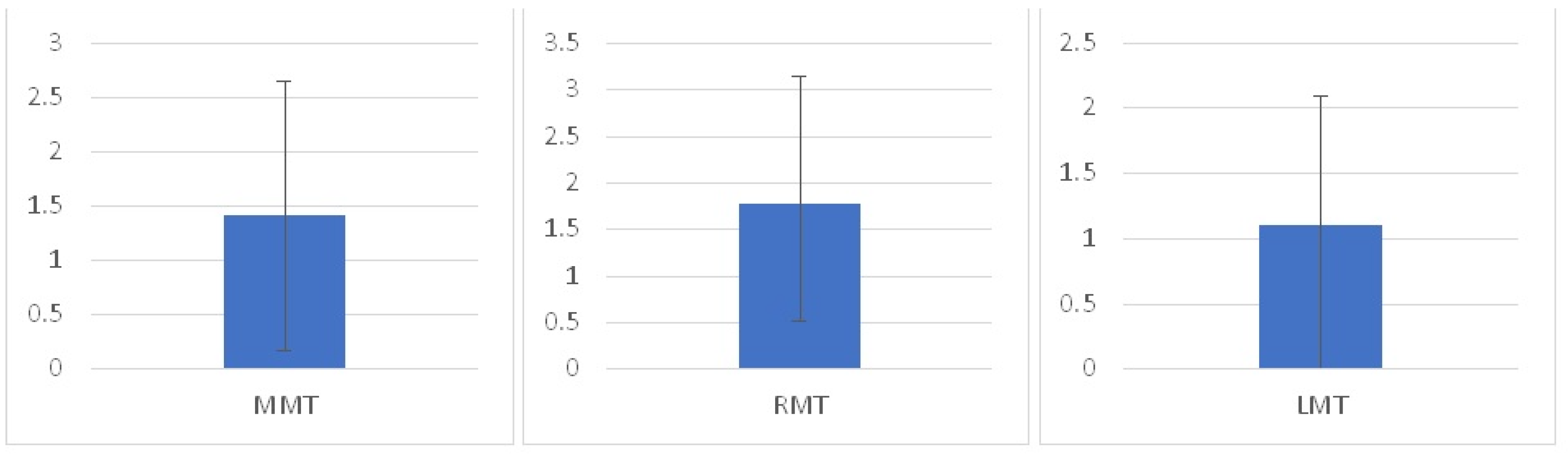
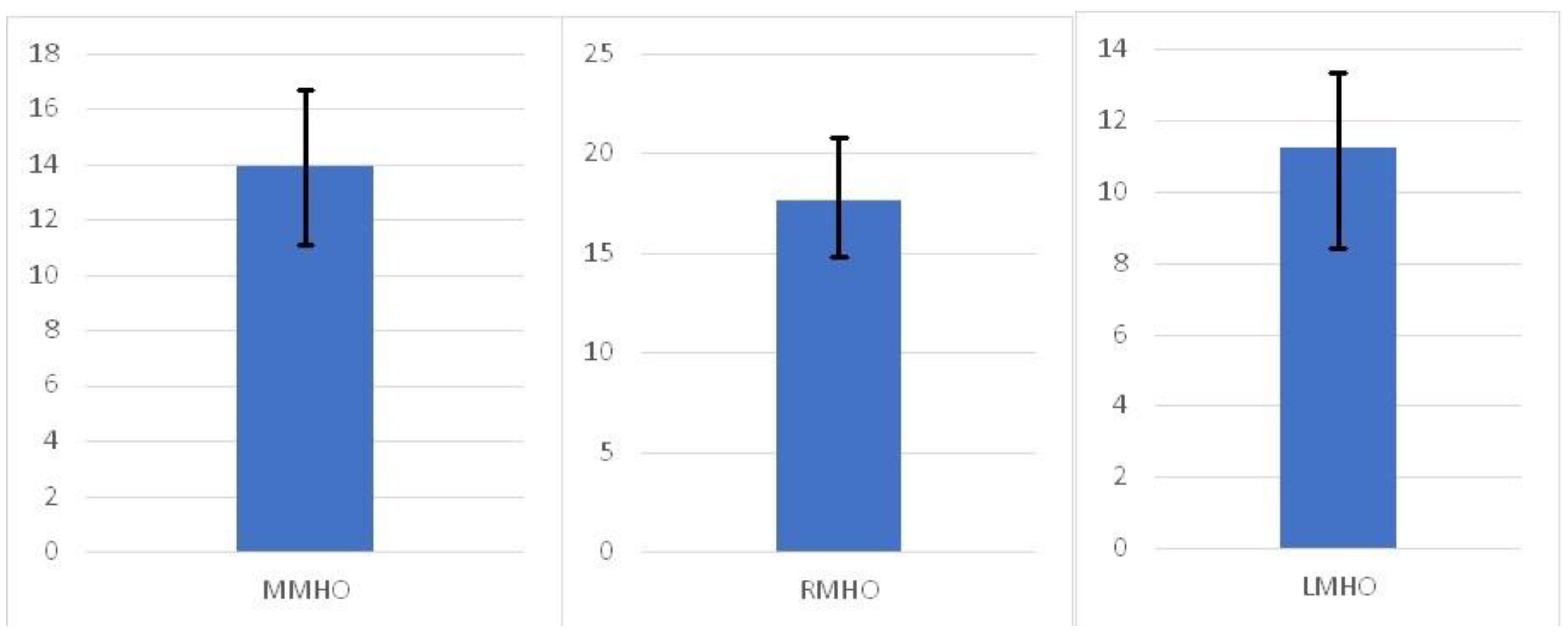
After the TENS procedure, the midline shift (MMT) compared to the mandibular midline in habitual occlusion (MMHO) was 1.41 ± 1.24 on the right molar side (RMT), the shift was 1.76 ± 1.39, and the left molar side (LMT) was 1.10 ± 0.99 (
Figure 3). No statistical significance was found comparing the midline mean (MMT) shift to the right molar side shift (RMT) (
p = 0.13) and to the left molar side shift (LMT) (
p = 0.24). A significant difference was revealed comparing the right molar side to the left molar side shift (
p = 0.041). All conditions except one showed a low correlation (r < 0.65). Only the midline (MMT) and the right molar side amount of shift after TENS (RMT) showed a positive correlation (r < 0.65). The mandibular midline (in habitual occlusion) asymmetry is not significantly located on the left side compared to the right one (
p = 0.6) (
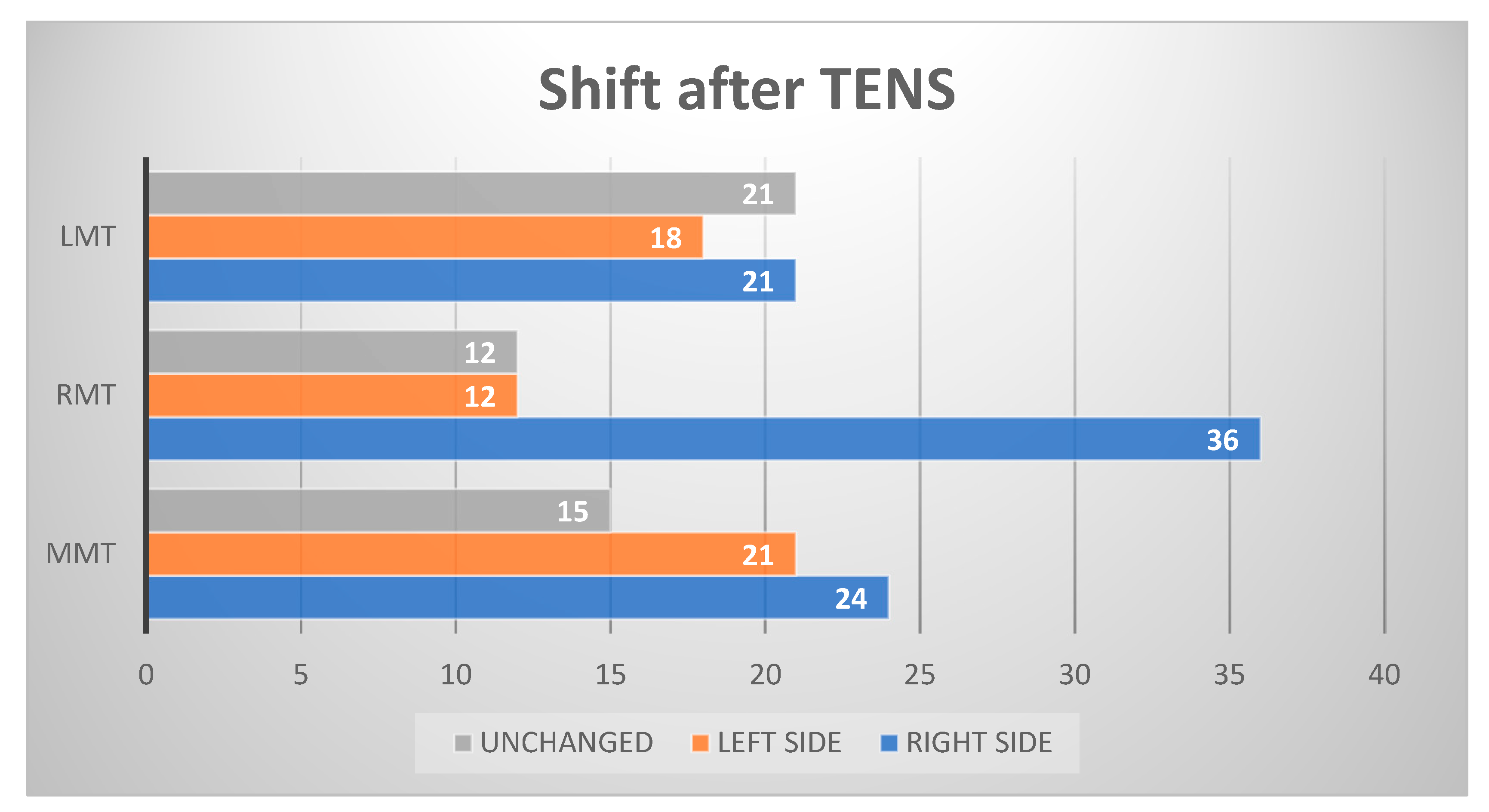
Figure 4). After the TENS procedure, 24 individuals shifted to the right of their midline, 21 to the left, and 15 did not change position. One sample proportion test failed to find a positive correlation between right and left shifts (
p = 0.29) with TENS. The right molar side after TENS shifted distally in 36 individuals, mesially in 12, and it did not change in the remaining 12. A statistically significant difference was shown between the right and left side shifts on the molar side (
p = 0.018). The left molar side after TENS shifted mesially in 21 individuals, distally in 18, and it did not change in 21. No statistically significant difference was found in the left molar side shift (
p = 0.39) (
Figure 5). After the TENS procedure, 30 subjects reduced midline asymmetry, 12 worsened, and 18 did not change midline asymmetry. Considering those patients whose midline asymmetry worsened or did not change and comparing them to those individuals with reduced asymmetry, the assessment of the intermaxillary relationship in terms of discrepancy from the midline did not show a statistically significant reduction of asymmetry after TENS (
p > 0.05).
The midline had the same shift direction compared to the left molar side in six individuals and the opposite shift direction in fifty-four individuals. The midline has the same shift direction compared to the right molar side in 12 individuals and the opposite shift direction in 48 individuals. The right–left molar side concordance was 30 out of 60 subjects; 30 out of 60 patients had the opposite shift direction on the left and right molar sides.
4. Discussion
Our results suggest that after muscle relaxation with dental sensory ULFTENS, the position of the jaw may or may not conform with the observation of laterodeviation made clinically or through plaster models through the position of the midline with closed teeth in habitual occlusion. Notably, in our study sample, a substantial group of the subjects worsens the midline asymmetry present in habitual occlusion, while another part does not change the asymmetry. Furthermore, considering the three-dimensional spatial displacement of the mandible as a whole, which can be represented by the simultaneous analysis of the position of the right and left molars, it can be observed that ULFTENS induces a resting position in which the right and left displacement in the laterolateral plane is frequently rather complex. For instance, the right side moves mesially, but the left end does not change position or it moves in a non-proportional way. If the mandible had simple translation movements on the horizontal plane, like those made on articulators or obtained with manual techniques on patients, the amount of lateral shift on the midline, left molar side, and right molar side would be proportional, and no significant difference in statistics would be found among the midline and left and right molar sides. This result suggests that functional lateral deviation could be an inhomogeneous diagnostic group and suggests that an approach with dental sensory ULFTENS to muscle balance could be useful in order to organize an actual functional orthodontic treatment. One of the assumptions of functional laterodeviations, in fact, is that in these subjects there exists a tonic imbalance of the musculature of the stomatognathic apparatus, and this would involve a deviated growth in relation to the continuous thrusts that the musculature would exert on the bone and dental matrix [
25,
26,
27,
28]. Our data with ULFTENS seem to confirm these observations. In fact, a substantial part of our sample shows that the muscular “relaxation” obtained with ULFTENS results in a different latero–lateral position of the mandible, a sign that, under “habitual” conditions, the “postural” and “functional” position of the mandible is maintained with an asymmetry of muscle tone. The muscle relaxation achieved with ULFTENS does not necessarily lead to a realignment of the midline and shows that the spatial relationships between the two arches can be rather complex, as already shown for the vertical and sagittal plane in a previous work [
1]. In relation to what has been observed, it could be useful, in latero-functional deviations, to evaluate the resting position of the mandible with relaxed musculature and, therefore, not “conditioned” by the need to adapt to the skeletal and dental structure, especially when guided by the habitual occlusion generally used for orthodontic diagnosis. In this way, it may be possible to integrate the treatment plan and suggest a therapy more aimed at obtaining spatial planes and occlusal and structural relationships in tune with muscular symmetry. Dental TENS is a valid aid used to achieve muscle relaxation, and this relaxation has been described in electromyographic and kinesiographic terms such as reduction of myoelectric tone, variation of interocclusal free space, and occlusal position after TENS [
29]. The use of this technique has the advantage that the resting position and the respective cranial–jaw relationship are obtained without direct manipulation of the jaw by an operator and without the direct will or voluntary mobility of the subject. The mechanism of action of TENS is complex and, although also present among its effects is that related to muscle tone on the musculature purely innervated by the V and VII pair of cranial nerves, some physiopathological responses to dental TENS may concern the overall capacity of adaptation to the environmental demands of the stimulated subject [
30]. The displacement of the rest position after TENS is not predictable based on the usual dental and skeletal characteristics, and the response to stimulation appears to be individual, probably associated with the complex mechanisms linked to the growth and development of the individual. What has been observed allows us to suggest that frequently, in the functional lateral deviations, the usual occlusal position and rest position are a form of compensation that can be shown with the TENS stimulation.
The causes of the asymmetry of the craniofacial district and consequently also of the cranial mandibular district can be many and different. Some of them have a pre- or neonatal origin, others are post-birth, some have been correlated with functional or parafunctional activities of the stomatognathic system, and still others with adaptations of the stomatognathic system to extrastomatognathic and postural requests in general [
31,
32,
33,
34,
35,
36]. All these causes can contribute to the structural asymmetry that arose at the time of the action of the case.
What could be interesting to evaluate at a clinical level is the persistence of an “unfavorable” adaptation in terms of lateral deviation in that this adaptation in place could prelude to a clinical, aesthetic deterioration of lateral deviation or even prevent an orthodontic treatment traditional. In other words, a clinical/therapeutic classification of functional laterodeviations could find support in the ability to observe the “relaxability” of the musculature and the degree and direction of the maxillo–mandibular growth compensation vectors consequent to it. In this sense, clinicians have often stressed the need to take into consideration not only the skeletal aspect and the static relationship between the maxilla and the jaw, but also the fascial, muscular, and articular aspects and the functions of other districts of the body adjacent to and far from the stomatognathic district [
37,
38,
39,
40]. In this perspective, one of the main goals of orthodontic treatment is not only to achieve satisfactory aesthetic results but also to create a functional occlusion, meaning an occlusion that does not require a neuromuscular compensation of adaptation passing from the resting position to the occlusal one and does not overload the systems mentioned above [
41,
42,
43]. Indeed, our work seems to suggest that the discrepancy between the resting position and habitual occlusion with respect to that obtainable with TENS is often in progress in children with functional lateral deviation and that, if it is shown that the musculature and the neuro fascial system after TENS is relaxed, it is necessary to work in relation to this neuro–muscular force and not contrary to it. In this way, the direction of the variation obtained with TENS should be taken into account in the treatment plan. It has been suggested that TENS acts on various physiological systems, including muscle, vision and accommodation, the autonomous one, pain control, and endorphins, and that, consequently, for this complex mechanism, its central action could be useful in the diagnosis and therapy of TM disorders [
44]. This mechanism of action and its clinical effect could also be implemented in children characterized by functional lateral deviation. These observations suggest that the use of TENS could improve the diagnostic and therapeutic possibilities in orthodontics by indicating the neuromuscular state of the resting position of the mandible and its adaptation to habitual occlusion. This work has its limitations, among them being the lack of a classical diagnosis based on Angle’s criteria. However, we must underline the fact that, within the logic in which it can be inscribed, the relevant aspect of our research was the functional lateral deviation that is independent of the type of dental class and skeletal class.
Another limitation of the work is that no comparison was made with other relaxation techniques of the stomatognathic musculature. On the other hand, our intention was to analyze the behavior of the resting position of the jaw precisely using the dental ULFTENS. The comparison with other techniques was not among the current aims of the work, although such a comparison could be the subject of new work. The recording of the cranio–mandibular relationship was obtained several times per child. This could result in different recordings leading to different resting and occlusal positions under TENS. In our study, the reproducibility of the recording was not performed through technical algorithms, but simply by observing the spatial “pattern” obtained. The type of displacement was always similar, so we chose to use the first recording in which the child is least “fatigued”. On the other hand, this limitation is difficult to overcome when, even with other techniques, one tries to propose an occlusal dimension different from the usual one. In our work, the starting point is to obtain a resting position with relaxed musculature. In this work, we have tried to represent the clinical work as closely as possible. Performing several tests makes the technique time-consuming and investigative and does not ensure the proper cooperation of the young patients. This work, therefore, attempts to represent a research development of clinical practice. As a matter of fact, we are currently conducting a study to assess the reliability and reproducibility of the technique, and the preliminary data as a whole seem to confirm the indications that have emerged from this work. A further limitation of this work is due to the lack of electromyographic and kinesiographic control of the application of TENS. Although previous works confirm that EMG values are reduced on average and interocclusal free space increases after TENS, indicating a relaxation of the stomatognathic musculature, and the parameters of the autonomous system of the accommodation move towards a lesser sympathetic control, this work has not instrumentally recorded the effect of TENS on muscles, free space, and autonomous control [
45]. On the other hand, the average values demonstrated elsewhere indicate that the TENS effect is generalizable and that only a minor sample can have a “paradoxical” effect, such as that reported by Konchak. In this sense, our work must be implemented with the use of other objective parameters of neuromuscular activity. Such research is difficult to perform with children due to its length and execution protocol and may not be decisive for the purposes of this research. The fact that the selected children did not present particular clinical disorders of the neuromuscular system, coordination, sight, and systems related to the stomatognathic system and that the research was concentrated on functional lateral deviations makes the possibility of misunderstanding the results less significant. Subsequent work will focus on the differences in response to the TENS of subjects with lateral deviations without the involvement of other districts (sight, posture, autonomous system, etc.) and subjects with definable “syndromic” forms in which other signs or symptoms of extrastomatognathic involvement are present.

 and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




