
Efficacy of Elastodontic Devices in Temporomandibular Disorder Reduction Assessed by Computer Aid Evaluation
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
- (1)
- Age between 18 and 50 years;
- (2)
- TMD diagnosis according to Axis I;
- (3)
- Index of orthodontic treatment needs (IOTN) ≤ 3;
- (4)
- Chronic orofacial pain (>3 months);
- (5)
- Impairment sEMG activity after TENS according to Konchak et al. [18];
- (6)
- Complete permanent dentition.
- (1)
- Systemic diseases;
- (2)
- History of local or general trauma;
- (3)
- Neurological or psychiatric disorders;
- (4)
- Pacemaker wearer;
- (5)
- Episodes of epileptic seizures;
- (6)
- Pregnancy;
- (7)
- Assumed use of FANS, steroidal anti-inflammatory drugs, analgesics, SSRIs or opiates.
2.1. Instrumentation
2.2. Statistical Analysis
3. Results
4. Discussion
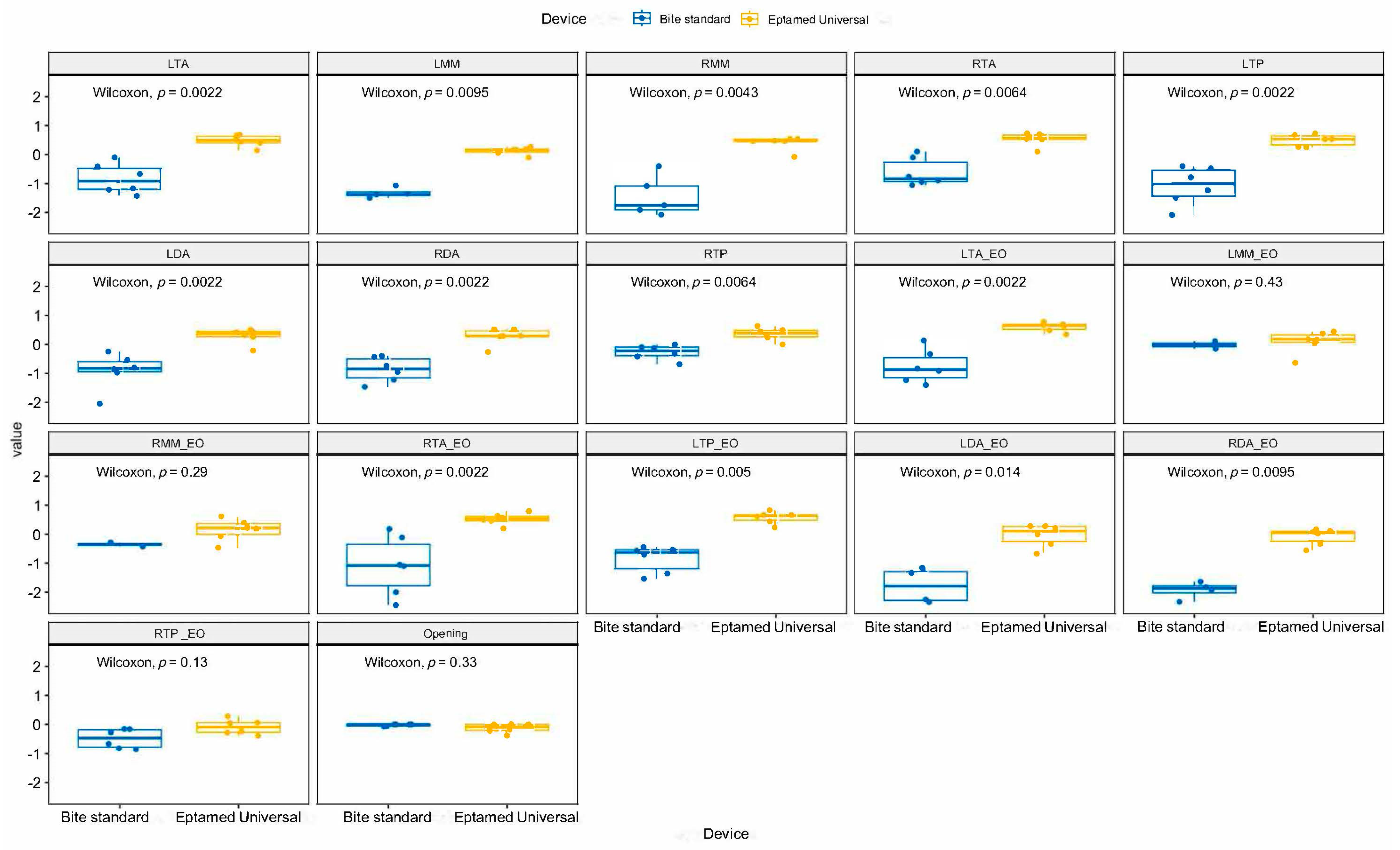
- The elastodontic device (EQ UNIVERSAL, Eptamed srl Via Ravennate, 979, 47522 Cesena (FC) ITALY) is capable of causing, in patients with temporomandibular disorders, a reduction in muscle tone at rest (scan 9) of the examined muscles (masseter, anterior temporal, digastric and sternocleidomastoid muscles) compared to a standard bite sold in pharmacies that, instead, causes an increase in muscle tension.
- The reduction of electromyographic activity with Eptamed is greater in the closed-eye condition than in the open-eye condition when scan 9 is recorded.
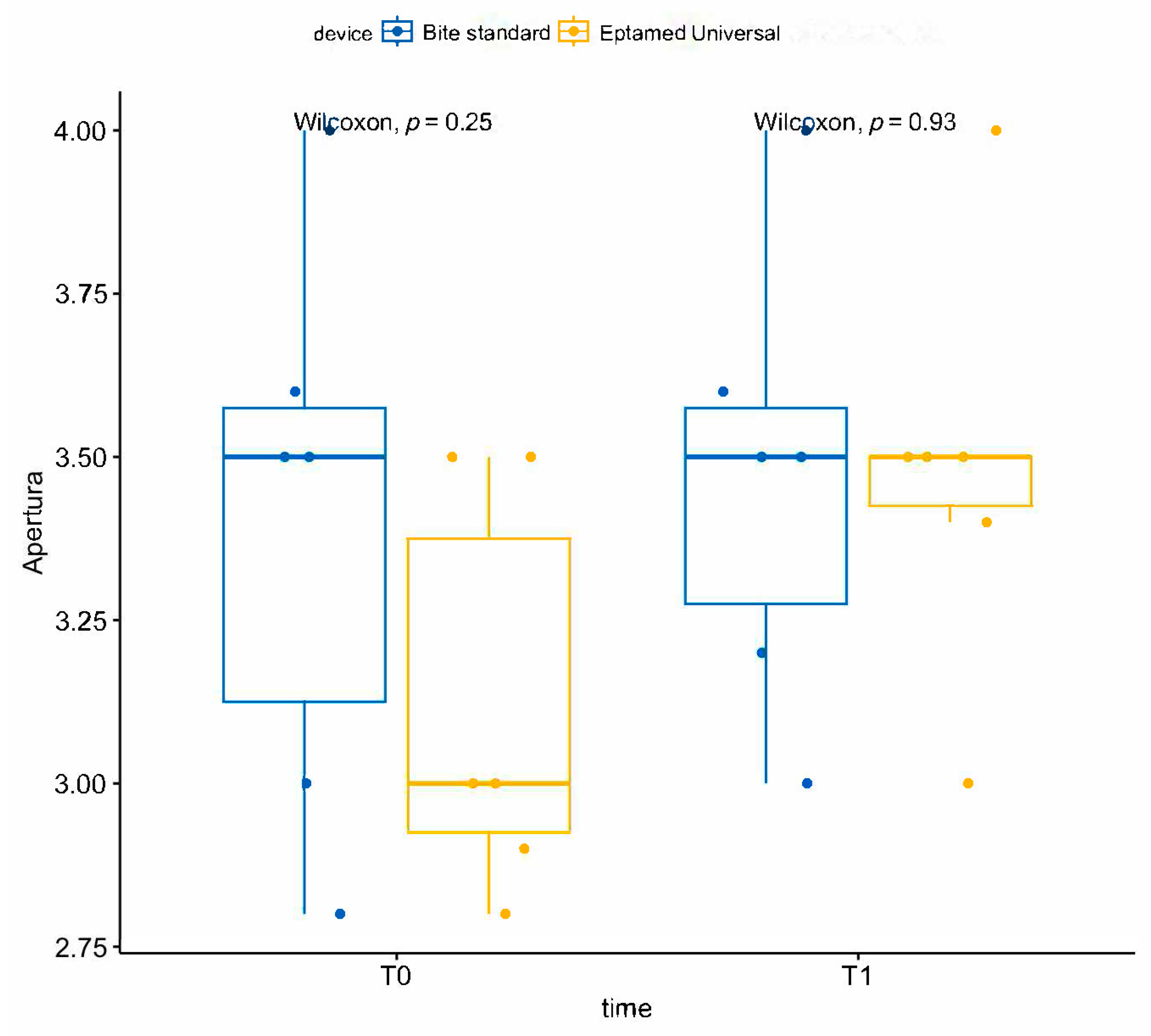
- No statistically significant difference was assessed during the kinesiographic examination at the maximum opening of the mouth in the comparison between the two groups at T0 and T1.
- No improvement in the electrical activity of the muscles was observed after 6 months of the use of the standard bite.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ohrbach, R.; Bair, E.; Fillingim, R.B.; Gonzalez, Y.; Gordon, S.M.; Lim, P.F.; Ribeiro-Dasilva, M.; Diatchenko, L.; Dubner, R.; Greenspan, J.D.; et al. Clinical orofacial characteristics associated with risk of first-onset TMD: The OPPERA prospective cohort study. J. Pain. 2013, 14 (Suppl. S12), T33–T50. [Google Scholar] [CrossRef]
- Sergio Paduano, M.D.; Rosaria Bucci, D.D.; Roberto Rongo, D.D.; Silva, R.; Michelotti, A. Prevalence of temporomandibular disorders and oral parafunctions in adolescents from public schools in Southern Italy. CRANIO® 2018, 38, 370–375. [Google Scholar] [CrossRef]
- Dworkin, S.F.; Von Korff, M.R.; LeResche, L. Multiple pains and psychiatric disturbance: An epidemiologic investigation. Arch. Gen. Psychiat. 1990, 47, 239–244. [Google Scholar] [CrossRef]
- Manfredini, D.; Ahlberg, J.; Winocur, E.; Guarda-Nardini, L.; Lobbezoo, F. Correlation of RDC/TMD axis I diagnoses and axis II pain-related disability. A multicenter study. Clin. Oral Investig. 2011, 15, 749–756. [Google Scholar] [CrossRef]
- Reis, P.H.F.; Laxe, L.A.C.; Lacerda-Santos, R.; Münchow, E.A. Distribution of anxiety and depression among different subtypes of temporomandibular disorder: A systematic review and meta-analysis. J. Oral Rehabil. 2022, 49, 754–767. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.U.; Chen, C.; Wong, H.C.; Yow, M.; Tan, E. Temporomandibular disorders in prospective orthodontic patients. Angle Orthod. 2021, 91, 377–383. [Google Scholar] [CrossRef] [PubMed]
- de Leeuw, R.; Klasser, G. (Eds.) Differential Diagnosis and Management of TMDs. Orofacial Pain: Guidelines, Assessment, Diagnosis, and Management, 6th ed.; Quintessence Publishing: Berlin, Germany, 2018; pp. 144–207. [Google Scholar]
- Andrews, L.F. Straightwire: The Concept and Appliance; LA Wells: San Diego, CA, USA, 1989. [Google Scholar]
- Masci, C.; Ciarrocchi, I.; Spadaro, A.; Necozione, S.; Marci, M.C.; Monaco, A. Does orthodontic treatment provide a real functional improvement? A case control study. BMC Oral Health 2013, 13, 57. [Google Scholar] [CrossRef] [PubMed]
- LeResche, L. Epidemiology of Temporomandibular disorders: Implication for investigation of etiologic factors. Crit. Rev. Oral Biol. Med. 1997, 8, 291–305. [Google Scholar] [CrossRef] [PubMed]
- Popa, C.; Solomon, S.M.; Rudnic, I.; Mârţu, I.; Luchian, I.; Mârţu, M.A.; Sava, N.; Mârţu, S. Evaluation of oclusal trauma as a risk factor in the ethiology of chronic periodontitis. Int. J. Med. Dent. 2018, 8, 83. [Google Scholar]
- Popa, C.G.; Luchian, I.; Ioanid, N.; Goriuc, A.; Martu, I.; Bosinceanu, D.; Martu, M.A.; Tirca, T.; Martu, S. ELISA Evaluation of RANKL Levels in Gingival Fluid in Patients with Periodontitis and Occlusal Trauma. Rev. Chim. 2018, 69, 1578–1580. [Google Scholar] [CrossRef]
- Al-Saleh, M.A.; Flores-Mir, C.; Thie, N.M. Electromyography in diagnosing temporomandibular disorders. J. Am. Dent. Assoc. 2012, 143, 351–362. [Google Scholar] [CrossRef] [PubMed]
- Santana-Mora, U.; López-Ratón, M.; Mora, M.J.; Cadarso-Suárez, C.; López-Cedrún, J.; Santana-Penín, U. Surface raw electromyography has a moderate discriminatory capacity for differentiating between healthy individuals and those with TMD: A diagnostic study. J. Electromyogr. Kinesiol. 2014, 24, 332–340. [Google Scholar] [CrossRef]
- Giannini, L.; Maspero, C.; Batia, C.; Galbiati, G. Valutazione elettromiografica ed elettrognatografica del trattamento ortodontico-chirurgico. Mondo Ortod. 2011, 36, 12–28. [Google Scholar] [CrossRef]
- Dworkin, S.F.; Le Resche, L. Research diagnostic criteria for temporomandibular disorders: Review, criteria, examinations and specifications, critique. J. Craniomandib. Disord. 1992, 6, 302–355. [Google Scholar]
- Brook, P.H.; Shaw, W.C. The development of an index of orthodontic treatment priority. Eur. J. Orthod. 1989, 11, 309–320. [Google Scholar] [CrossRef]
- Konchak, P.A.; Thomas, N.R.; Lanigan, D.T.; Devon, R.M. Freeway space measurement using mandibular kinesiograph and EMG before and after TENS. Angle Orthod. 1988, 58, 343–350. [Google Scholar] [PubMed]
- Ortu, E.; Pietropaoli, D.; Cova, S.; Marci, M.C.; Monaco, A. Efficacy of elastodontic devices in overjet and overbite reduction assessed by computer-aid evaluation. BMC Oral Health 2021, 21, 269. [Google Scholar] [CrossRef]
- Castroflorio, T.; Farina, D.; Bottin, A.; Piancino, M.G.; Bracco, P.; Merletti, R. Surface EMG of jaw elevator muscles: Effect of electrode location and inter-electrode distance. J. Oral Rehabil. 2005, 32, 411–417. [Google Scholar] [CrossRef]
- Castro, H.A.; Resende, L.A.; Berzin, F.; Konig, B. Electromyographic analysis of the superior belly of the omohyoid muscle and anterior belly of the digastric muscle in tongue and head movements. J. Electromyogr. Kinesiol. 1999, 9, 229–232. [Google Scholar] [CrossRef]
- Ortu, E.; Barrucci, G.; Aprile, G.; Guerrini, L.; Pietropaoli, D.; Monaco, A. Electromyographic evaluation during orthodontic therapy: Comparison of two elastodontic devices. J. Biol. Regul. Homeost. Agents 2020, 34, 1935–1939. [Google Scholar] [CrossRef]
- Kononen, M.; Nystrom, M.; Kleemola-Kujola, E.; Kataja, M.; Evalahti, M.; Pekka, L.; Peck, L. Signs and symptoms of craniomandibular disorders in a series of Finnish children. Acta Odontol. Scand. 1987, 45, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Hirata, R.H.; Heft, M.W.; Hernandez, B.; King, G.J. Longitudinal study of signs of temporomandibular disorders (TMD) in orthodontically treated and nontreated groups. Am. J. Orthod. Dentofacial. Orthop. 1992, 101, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Ricketts, R.M. Clinical implications of the temporomandibular joint. Am. J. Orthod. 1966, 52, 416–439. [Google Scholar] [CrossRef] [PubMed]
- Pollack, B. Cases of note: Michigan jury awards $850,000 in ortho case: A tempest in a teapot. J. Mich. Dent. Assoc. 1988, 70, 540–542. [Google Scholar] [PubMed]
- Stohler, C.S.; Zarb, G.A. On the management of temporomandibular disorders: A plea for a low-tech, high-prudence therapeutic approach. J. Orofac. Pain 1999, 13, 255–261. [Google Scholar] [PubMed]
- Sanjivan, K.; Donald, J.; Rinchuse, C.S.; Greene, L.; Johnston, E. Temporomandibular disorders and orthodontics: What have we learned from 1992–2022? Am. J. Orthod. Dentofac. Orthop. 2022, 161, 769–774. [Google Scholar] [CrossRef]
- Machen, D.E. Legal aspects of orthodontic practice: Risk management concepts. Excellent diagnostic informed consent practice and record keeping make a difference. Am. J. Orthod. Dentofacial. Orthop. 1990, 98, 381–382. [Google Scholar] [CrossRef]
- Castroflorio, T.; Titolo, C.; Deregibus, A.; Debernardi, C.; Bracco, P. The Orthodontic Treatment of TMD Patients: EMG Effects of a Functional Appliance. CRANIO® 2007, 25, 206–212. [Google Scholar] [CrossRef]
- Kecik, D.; Kocadereli, I.; Saatci, I. Evaluation of the treatment changes of functional posterior crossbite in the mixed dentition. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 202–215. [Google Scholar] [CrossRef]
- Chen, H.; Nackley, A.; Miller, V.; Diatchenko, L.; Maixner, W. Multisystem dysregulation in painful temporomandibular disorders. J. Pain 2013, 14, 983–996. [Google Scholar] [CrossRef]
- Monaco, A.; Ortu, E.; Giannoni, M.; D’Andrea, P.; Cattaneo, R.; Mummolo, A.; Pietropaoli, D. Standard Correction of Vision Worsens EMG Activity of Pericranial Muscles in Chronic TMD Subjects. Pain Res Manag. 2020, 2020, 3932476. [Google Scholar] [CrossRef] [PubMed]
- Kindler, L.L.; Bennett, R.M.; Jones, K.D. Central sensitivity syndromes: Mounting pathophysiologic evidence to link fibromyalgia with other common chronic pain disorders. Pain Manag. Nurs. 2011, 12, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, G.M.; Lodetti, G.; Paiva, G.; De Felicio, C.M.; Sforza, C. Surface electromyograpic assessment of patients with long lasting temporomandibular joint disorders pain. J. Electromyogr. Kinesiol. 2011, 21, 659–664. [Google Scholar] [CrossRef]
- Adibi, S.S.; Ogbureke, E.I.; Minavi, B.B.; Ogbureke, K.U. Why use oral splints for temporomandibular disorders(TMDs)? Tex. Dent. J. 2014, 131, 450–455. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Id | Device | Lta | Lmm | Rmm | Rta | Ltp | Lda | Rda | Rtp | Lta_eo | Lmm_eo | Rmm_eo | Rta_eo | Ltp_eo | Lda_eo | Rda_eo | Rtp_eo | Opening |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | BITE | −1.21 | −1.07 | −1.75 | −0.89 | −0.40 | −0.54 | −0.95 | −0.42 | −0.91 | −4.46 | −4.85 | −2.44 | −0.53 | −2.35 | −3.71 | −0.86 | 0.00 |
| 2 | BITE | −1.17 | −4.00 | −3.30 | −1.06 | −0.46 | −2.04 | −1.46 | −0.13 | −1.23 | −4.50 | −3.30 | −1.06 | −0.44 | −4.11 | −3.09 | −0.27 | 0.00 |
| 3 | BITE | −0.10 | −1.50 | −0.40 | 0.11 | −2.09 | −0.85 | −0.74 | −0.69 | 0.14 | 0.11 | −0.29 | 0.18 | −1.54 | −1.17 | −1.64 | −0.16 | 0.00 |
| 4 | BITE | −1.42 | −1.36 | −2.08 | −0.10 | −0.79 | −0.25 | −0.43 | 0.00 | −1.40 | −5.00 | −4.83 | −2.00 | −0.56 | −1.33 | −2.33 | −0.67 | −0.07 |
| 5 | BITE | −0.67 | −1.38 | −1.08 | −0.76 | −1.23 | −0.80 | −0.39 | −0.32 | −0.33 | −4.91 | −3.55 | −1.11 | −0.71 | −2.26 | −1.92 | −0.15 | −0.07 |
| 6 | BITE | −0.41 | −3.00 | −1.91 | −0.94 | −1.50 | −0.97 | −1.22 | −0.09 | −0.83 | −0.15 | −0.43 | −0.11 | −1.36 | −3.50 | −1.83 | −0.82 | 0.00 |
| 1 | EQ. U. | 0.69 | 0.06 | 0.55 | 0.71 | 0.74 | 0.25 | 0.27 | 0.64 | 0.78 | 0.38 | 0.62 | 0.80 | 0.67 | −0.33 | −0.33 | −0.28 | −0.21 |
| 2 | EQ. U. | 0.14 | −0.10 | −0.08 | 0.11 | 0.26 | −0.21 | −0.27 | 0.00 | 0.34 | −0.64 | −0.47 | 0.20 | 0.24 | 0.00 | 0.03 | −0.24 | −0.17 |
| 3 | EQ. U. | 0.44 | 0.19 | 0.47 | 0.74 | 0.68 | 0.46 | 0.52 | 0.24 | 0.68 | 0.04 | −0.07 | 0.64 | 0.83 | −0.67 | −0.56 | −0.39 | 0.00 |
| 4 | EQ. U. | 0.66 | 0.15 | 0.55 | 0.54 | 0.53 | 0.42 | 0.53 | 0.80 | 0.70 | 0.45 | 0.24 | 0.58 | 0.67 | 0.29 | 0.07 | 0.07 | 0.00 |
| 5 | EQ. U. | 0.40 | 0.17 | 0.46 | 0.59 | 0.53 | 0.51 | 0.29 | 0.33 | 0.63 | 0.18 | 0.41 | 0.50 | 0.61 | 0.22 | 0.12 | 0.28 | 0.00 |
| 6 | EQ. U. | 0.55 | 0.27 | 0.48 | 0.52 | 0.25 | 0.32 | 0.30 | 0.44 | 0.49 | 0.19 | 0.20 | 0.46 | 0.44 | 0.29 | 0.17 | 0.05 | −0.38 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortu, E.; Di Nicolantonio, S.; Cova, S.; Pietropaoli, D.; De Simone, L.; Monaco, A. Efficacy of Elastodontic Devices in Temporomandibular Disorder Reduction Assessed by Computer Aid Evaluation. Appl. Sci. 2024, 14, 1651. https://doi.org/10.3390/app14041651
Ortu E, Di Nicolantonio S, Cova S, Pietropaoli D, De Simone L, Monaco A. Efficacy of Elastodontic Devices in Temporomandibular Disorder Reduction Assessed by Computer Aid Evaluation. Applied Sciences. 2024; 14(4):1651. https://doi.org/10.3390/app14041651
Chicago/Turabian StyleOrtu, Eleonora, Sara Di Nicolantonio, Samuele Cova, Davide Pietropaoli, Lucia De Simone, and Annalisa Monaco. 2024. "Efficacy of Elastodontic Devices in Temporomandibular Disorder Reduction Assessed by Computer Aid Evaluation" Applied Sciences 14, no. 4: 1651. https://doi.org/10.3390/app14041651