
Advantages of Dynamic Navigation in Prosthetic Implant Treatment in Terms of the Clinical Evaluation and Salivary Pro-Inflammatory Biomarkers: A Clinical Study
 , ,
, ,
Abstract
:1. Introduction
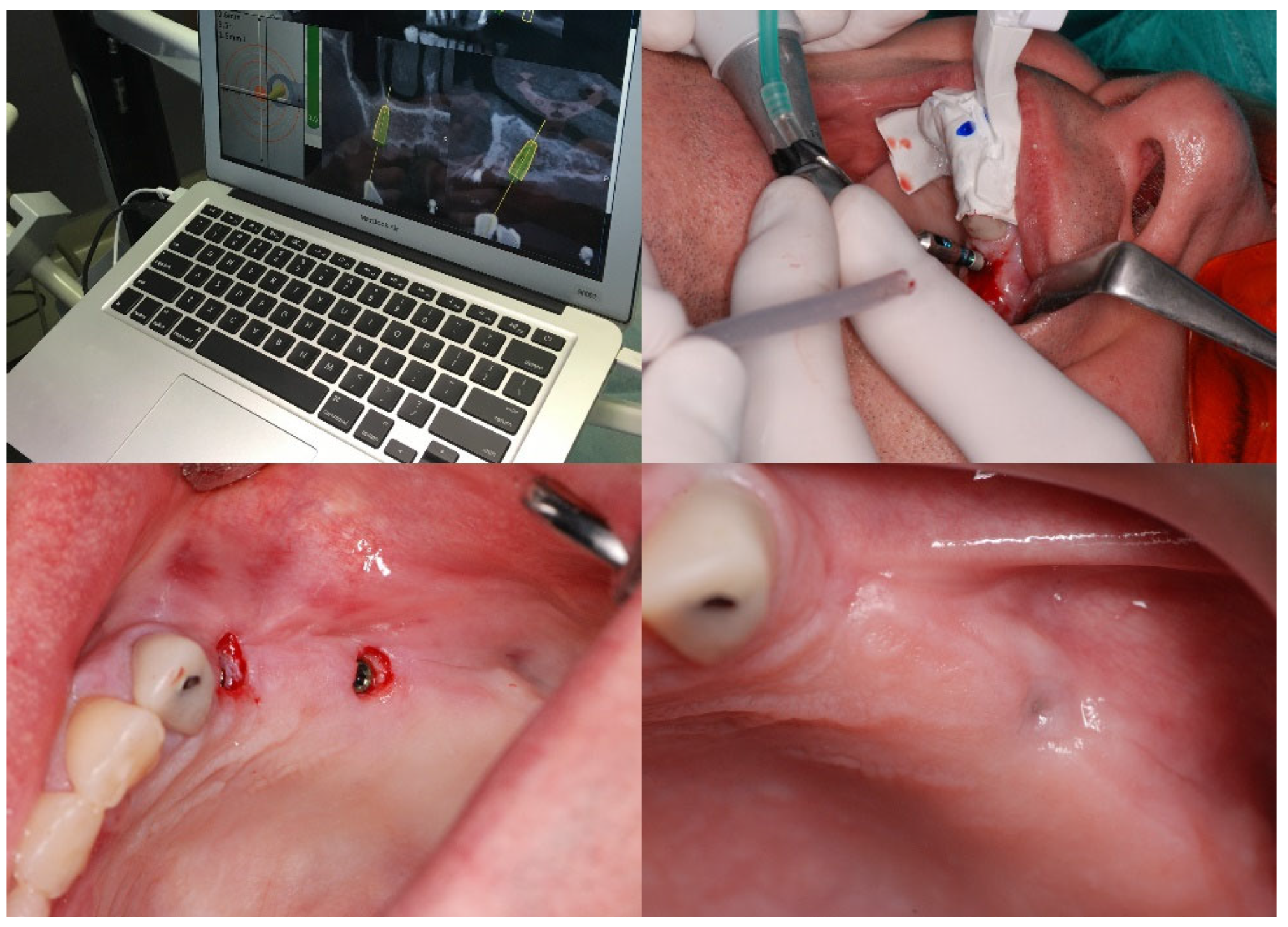
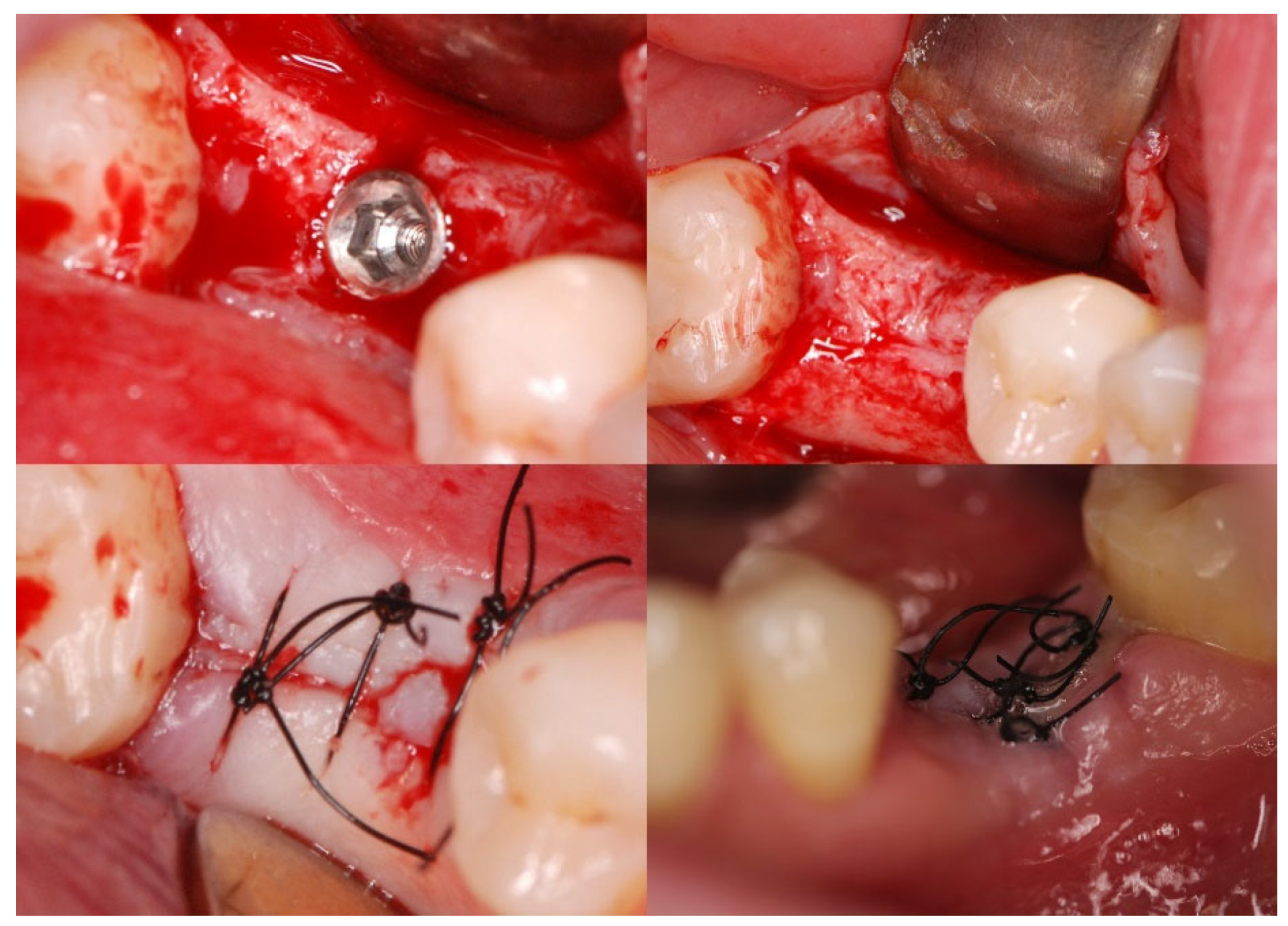
2. Materials and Methods
2.1. Patients
2.2. Saliva Samples
2.3. Determination of Saliva CRP Concentration
2.4. Determination of Saliva IL-6 Concentration
2.5. Statistical Analysis
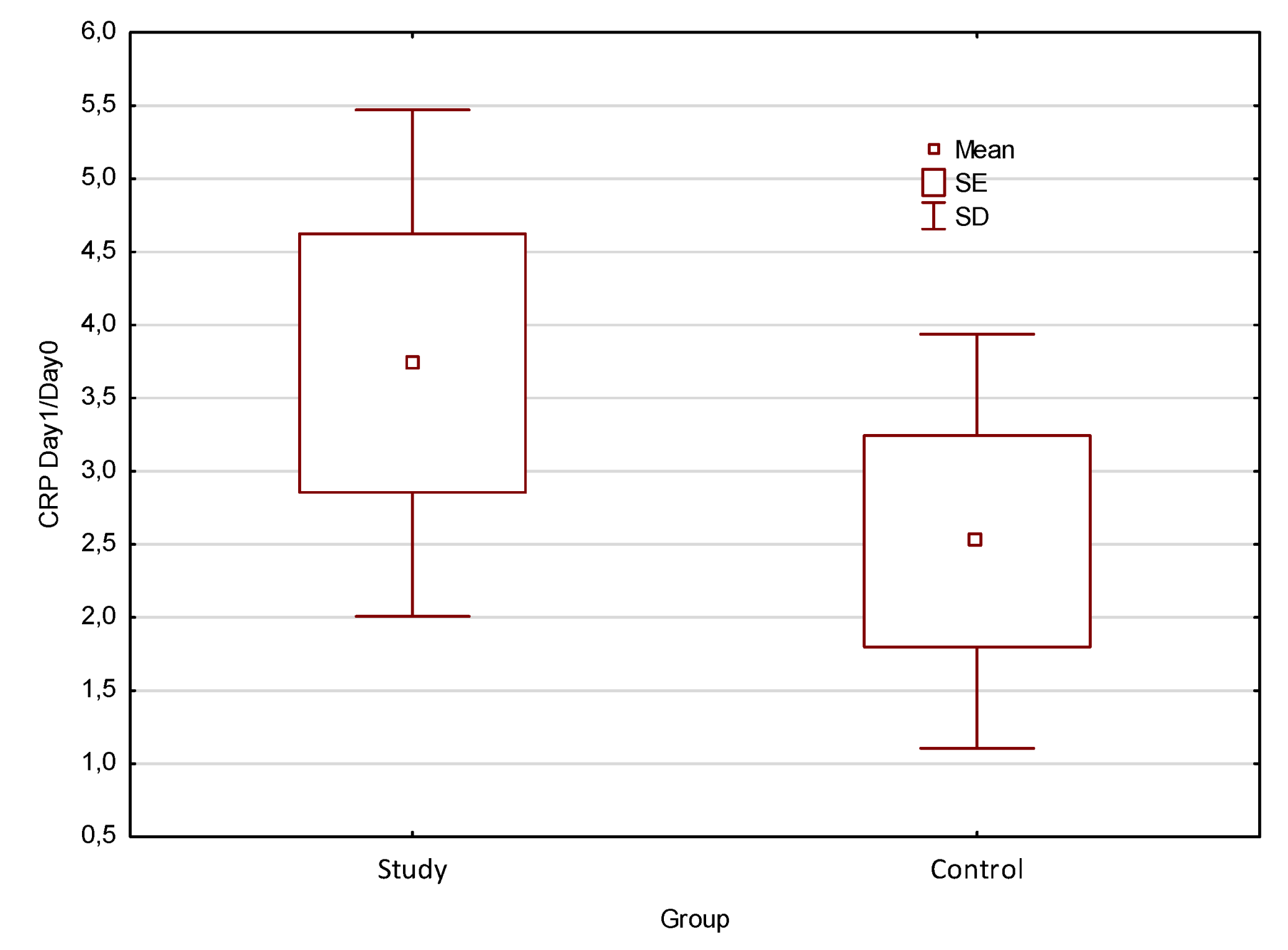
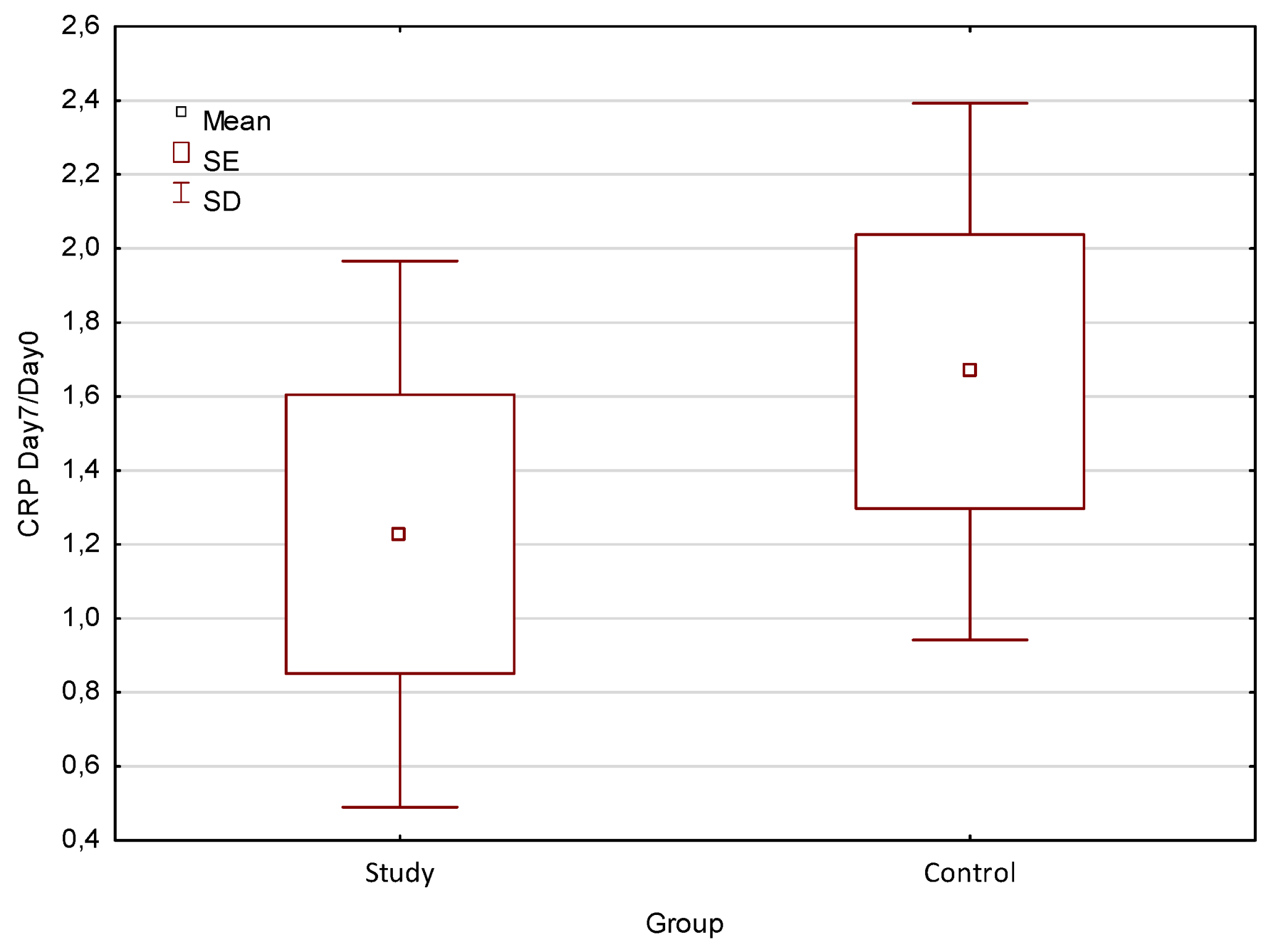
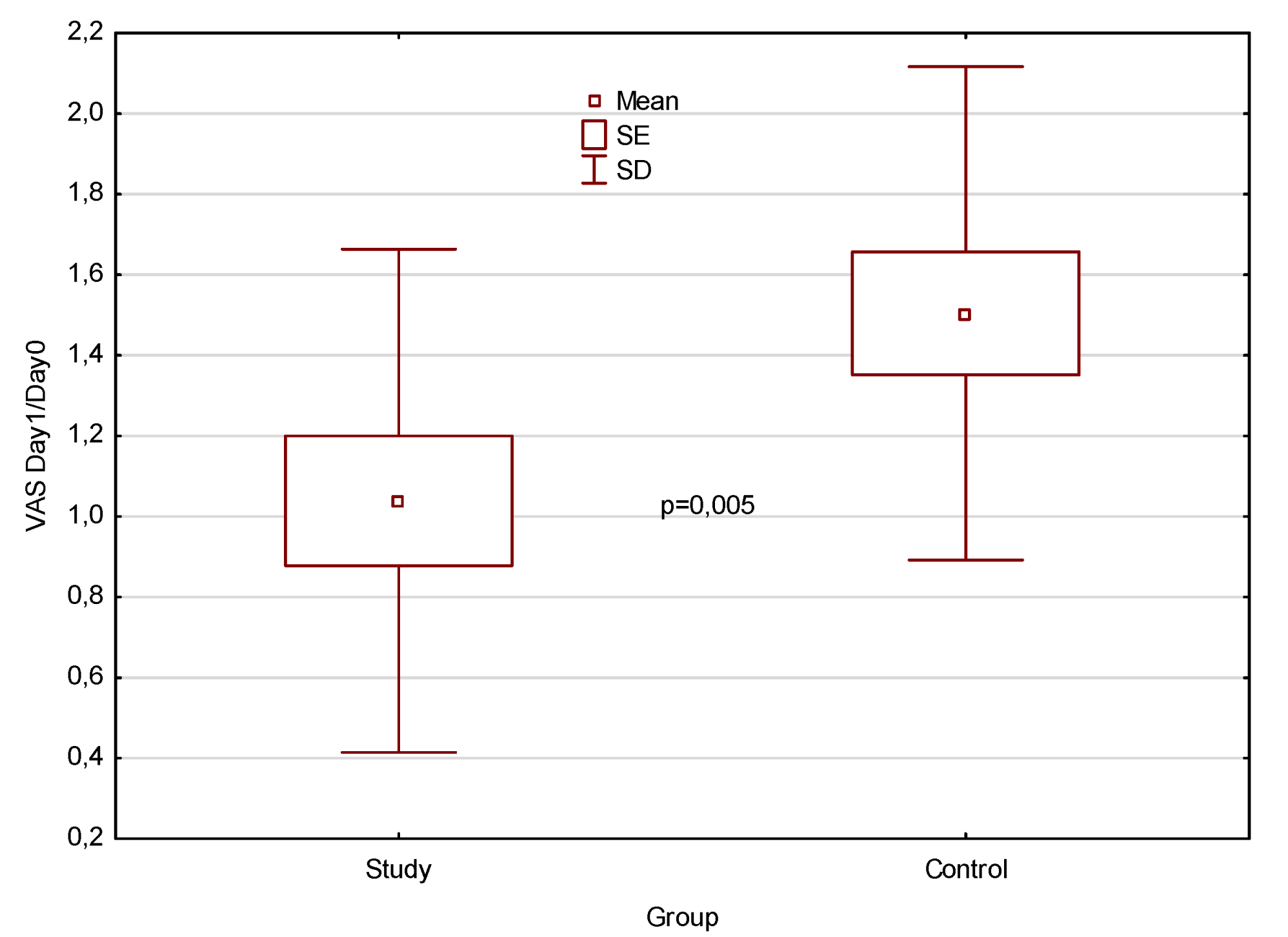
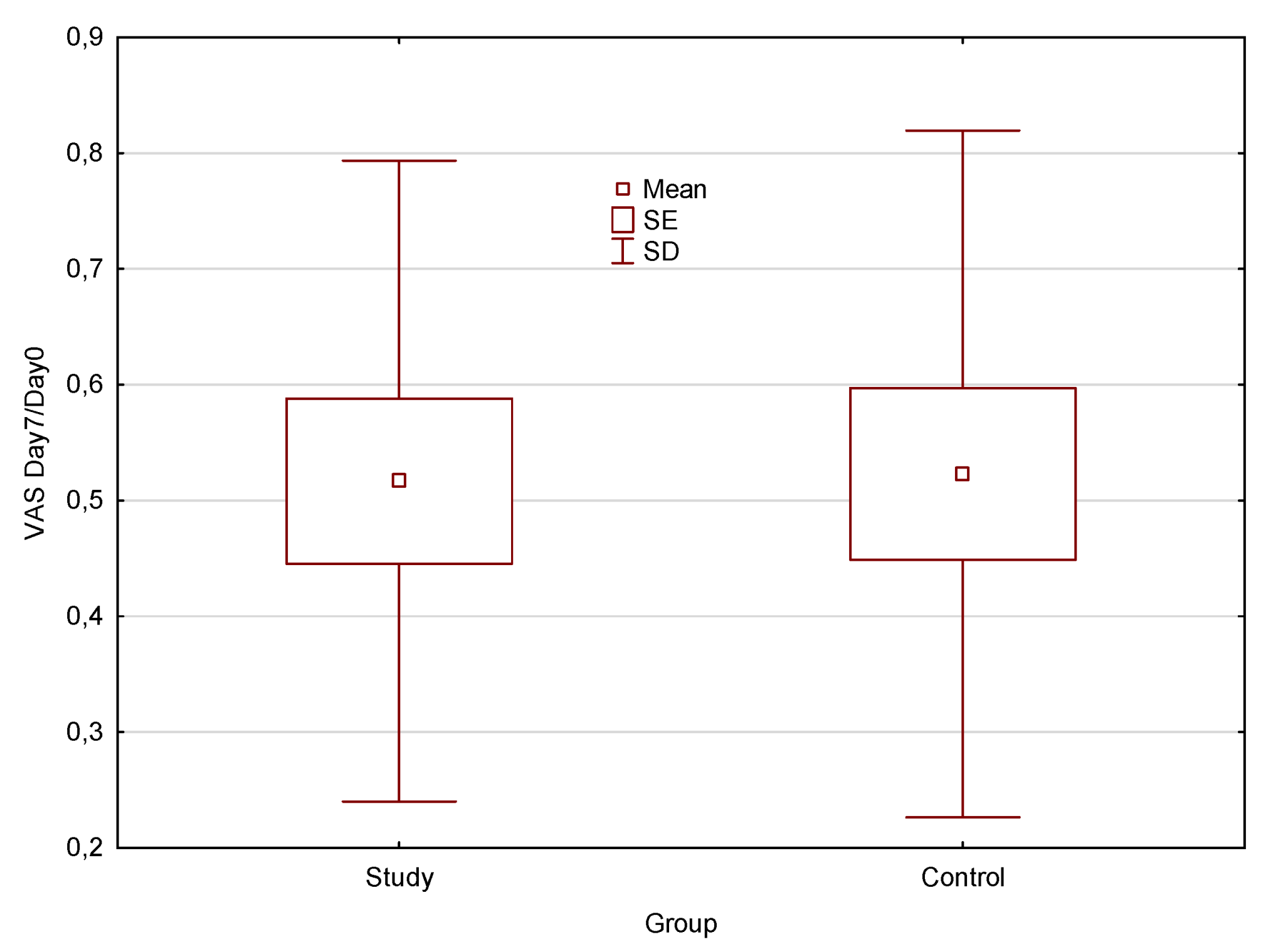
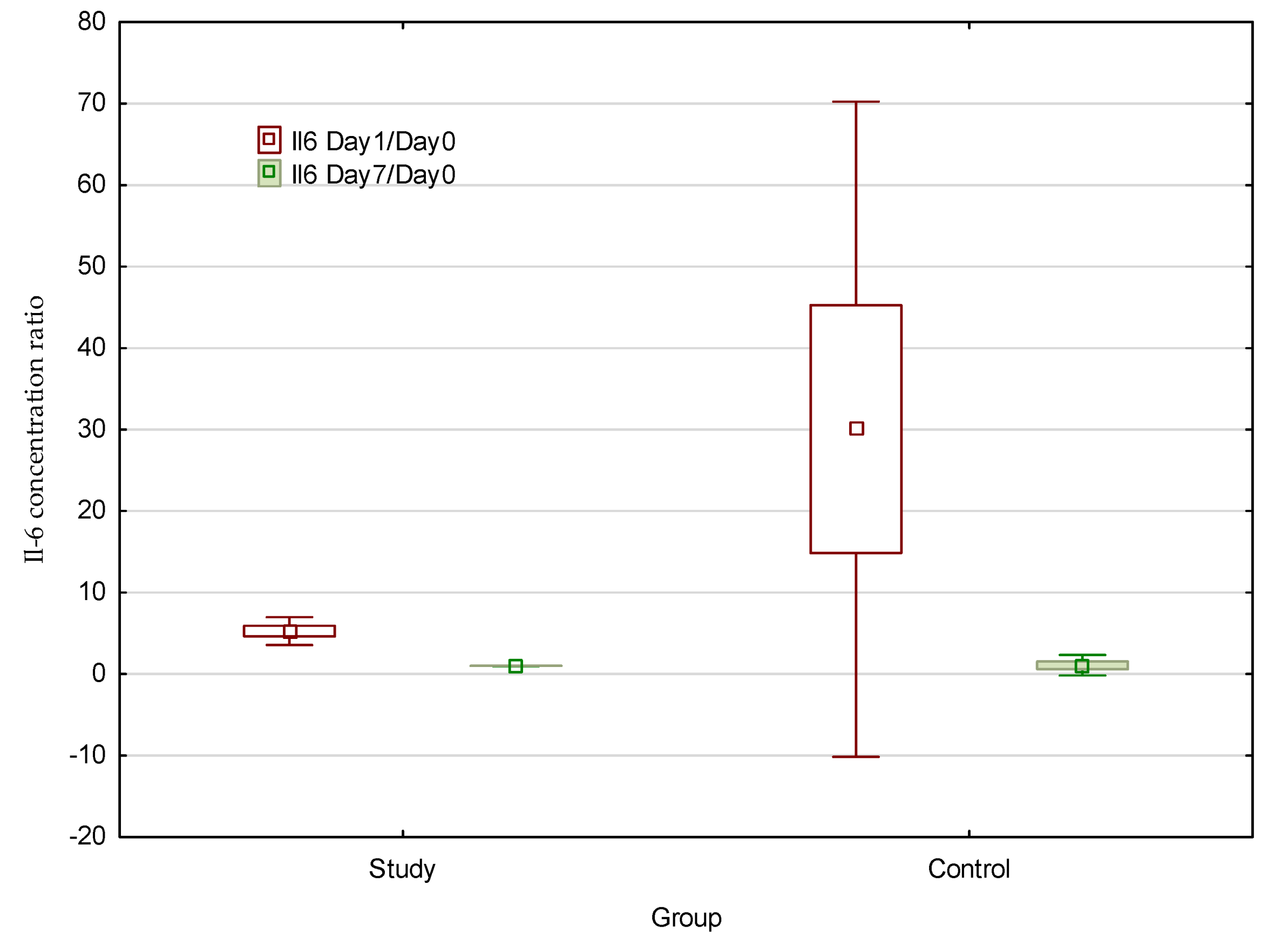
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kageyama, I.; Maeda, S.; Takezawa, K. Importance of anatomy in dental implant surgery. J. Oral Biosci. 2021, 63, 142–152. [Google Scholar] [CrossRef]
- Greenstein, G.; Cavallaro, J.; Tarnow, D. Practical Application of Anatomy for the Dental Implant Surgeon. J. Periodontol. 2008, 79, 1833–1846. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, Z.; Sima, C.; Glogauer, M. Bone Replacement Materials and Techniques Used for Achieving Vertical Alveolar Bone Augmentation. Materials 2015, 8, 2953–2993. [Google Scholar] [CrossRef]
- Gual-Vaques, P.; Polis-Yanes, C.; Estrugo-Devesa, A.; Ayuso-Montero, R.; Mari-Roig, A.; Lopez-Lopez, J. Autogenous teeth used for bone grafting: A systematic review. Med. Oral. Patol. Oral. Cir. Bucal. 2018, 23, e112–e119. [Google Scholar] [CrossRef] [PubMed]
- Kubaszek, B.; Morawiec, T.; Mertas, A.; Wachol, K.; Nowak-Wachol, A.; Śmieszek-Wilczewska, J.; Łopaciński, M.; Cholewka, A. Radiological and Microbiological Evaluation of the Efficacy of Alveolar Bone Repair Using Autogenous Dentin Matrix—Preliminary Study. Coatings 2022, 12, 909. [Google Scholar] [CrossRef]
- Fickl, S.; Kebschull, M.; Schupbach, P.; Zuhr, O.; Schlagenhauf, U.; Hürzeler, M.B. Bone loss after full-thickness and partial-thickness flap elevation. J. Clin. Periodontol. 2011, 38, 157–162. [Google Scholar] [CrossRef]
- Araujo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef]
- Araújo, M.G.; Lindhe, J. Ridge alterations following tooth extraction with and without flap elevation: An experimental study in the dog. Clin. Oral Implant. Res. 2009, 20, 545–549. [Google Scholar] [CrossRef]
- Volberg, R.; Mordanov, O. Canalis Sinuosus Damage after Immediate Dental Implant Placement in the Esthetic Zone. Case Rep. Dent. 2019, 2019, 3462794. [Google Scholar] [CrossRef]
- An, J.-H.; Park, S.-H.; Han, J.J.; Jung, S.; Kook, M.-S.; Park, H.-J.; Oh, H.-K. Treatment of dental implant displacement into the maxillary sinus. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 35. [Google Scholar] [CrossRef]
- Pellegrino, G.; Bellini, P.; Cavallini, P.F.; Ferri, A.; Zacchino, A.; Taraschi, V.; Marchetti, C.; Consolo, U. Dynamic Navigation in Dental Implantology: The Influence of Surgical Experience on Implant Placement Accuracy and Operating Time. An in Vitro Study. Int. J. Environ. Res. Public Health 2020, 17, 2153. [Google Scholar] [CrossRef] [PubMed]
- Vercruyssen, M.; Laleman, I.; Jacobs, R.; Quirynen, M. Computer-supported implant planning and guided surgery: A narrative review. Clin. Oral Implant. Res. 2015, 26 (Suppl. S11), 69–76. [Google Scholar] [CrossRef] [PubMed]
- Bover-Ramos, F.; Viña-Almunia, J.; Cervera-Ballester, J.; Peñarrocha-Diago, M.; García-Mira, B. Accuracy of Implant Placement with Computer-Guided Surgery: A Systematic Review and Meta-Analysis Comparing Cadaver, Clinical, and In Vitro Studies. Int. J. Oral Maxillofac. Implant. 2018, 33, 101–115. [Google Scholar] [CrossRef] [PubMed]
- Zian, Z.; Bouhoudan, A.; Mourabit, N.; Azizi, G.; Mechita, M.B. Salivary Cytokines as Potential Diagnostic Biomarkers for Systemic Lupus Erythematosus Disease. Mediat. Inflamm. 2021, 2021, 8847557. [Google Scholar] [CrossRef]
- Diesch, T.; Filippi, C.; Fritschi, N.; Filippi, A.; Ritz, N. Cytokines in saliva as biomarkers of oral and systemic oncological or infectious diseases: A systematic review. Cytokine 2021, 143, 155506. [Google Scholar] [CrossRef]
- Teles, R.P.; Likhari, V.; Socransky, S.S.; Haffajee, A.D. Salivary cytokine levels in subjects with chronic periodontitis and in periodontally healthy individuals: A cross-sectional study. J. Periodontal Res. 2009, 44, 411–417. [Google Scholar] [CrossRef]
- Gornowicz, A.; Bielawska, A.; Bielawski, K.; Grabowska, S.Z.; Wójcicka, A.; Zalewska, M.; Maciorkowska, E. Pro-inflammatory cytokines in saliva of adolescents with dental caries disease. Ann. Agric. Environ. Med. 2012, 19, 711–716. [Google Scholar]
- Ribeiro, C.C.C.; Pachêco, C.d.J.B.; Costa, E.L.; Ladeira, L.L.C.; Costa, J.F.; da Silva, R.A.; Carmo, C.D.S. Proinflammatory cytokines in early childhood caries: Salivary analysis in the mother/children pair. Cytokine 2018, 107, 113–117. [Google Scholar] [CrossRef]
- Zhu, Z.-D.; Ren, X.-M.; Zhou, M.-M.; Chen, Q.-M.; Hua, H.; Li, C.-L. Salivary cytokine profile in patients with oral lichen planus. J. Dent. Sci. 2022, 17, 100–105. [Google Scholar] [CrossRef]
- Fonseca, F.J.P.O.; Junior, M.M.; Lourenço, E.J.V.; Teles, D.d.M.; Figueredo, C.M. Cytokines expression in saliva and peri-implant crevicular fluid of patients with peri-implant disease. Clin. Oral Implant. Res. 2014, 25, e68–e72. [Google Scholar] [CrossRef]
- Vohra, F.; Alkhudhairy, F.; Al-Kheraif, A.A.; Akram, Z.; Javed, F. Peri-implant parameters and C-reactive protein levels among patients with different obesity levels. Clin. Implant. Dent. Relat. Res. 2018, 20, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Melguizo-Rodríguez, L.; Costela-Ruiz, V.J.; Manzano-Moreno, F.J.; Ruiz, C.; Illescas-Montes, R. Salivary Biomarkers and Their Application in the Diagnosis and Monitoring of the Most Common Oral Pathologies. Int. J. Mol. Sci. 2020, 21, 5173. [Google Scholar] [CrossRef] [PubMed]
- Decker, M.-L.; Gotta, V.; Wellmann, S.; Ritz, N. Cytokine profiling in healthy children shows association of age with cytokine concentrations. Sci. Rep. 2017, 7, 17842. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, A.; Yadav, S.S.; Dwivedi, P.; Lal, N.; Usman, K.; Khattri, S. Correlation of Serum and Salivary Cytokines Level with Clinical Parameters in Metabolic Syndrome With Periodontitis. J. Clin. Lab. Anal. 2016, 30, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Szabo, Y.Z.; Slavish, D.C. Measuring salivary markers of inflammation in health research: A review of methodological considerations and best practices. Psychoneuroendocrinology 2021, 124, 105069. [Google Scholar] [CrossRef]
- Cazalis, J.; Tanabe, S.; Gagnon, G.; Sorsa, T.; Grenier, D. Tetracyclines and chemically modified tetracycline-3 (CMT-3) modulate cytokine secretion by lipopolysaccharide-stimulated whole blood. Inflammation 2009, 32, 130–137. [Google Scholar] [CrossRef]
- Sorsa, T.; Tjäderhane, L.; Konttinen, Y.T.; Lauhio, A.; Salo, T.; Lee, H.M.; Golub, L.M.; Brown, D.L.; Mäntylä, P. Matrix metalloproteinases: Contribution to pathogenesis, diagnosis and treatment of periodontal inflammation. Ann. Med. 2006, 38, 306–321. [Google Scholar] [CrossRef]
- Shahidi, M.; Jafari, S.; Barati, M.; Mahdipour, M.; Gholami, M.S. Predictive value of salivary microRNA-320a, vascular en-dothelial growth factor receptor 2, CRP and IL-6 in Oral lichen planus progression. Inflammopharmacology 2017, 25, 577–583. [Google Scholar] [CrossRef]
- Shiva, A.; Arab, S.; Mousavi, S.J.; Zamanian, A.; Maboudi, A. Serum and Salivary Level of Nitric Oxide (NOx) and CRP in Oral Lichen Planus (OLP) Patients. J. Dent. 2020, 21, 6–11. [Google Scholar]
- Rose-John, S. Interleukin-6 Family Cytokines. Cold Spring Harb. Perspect. Biol. 2017, 10, a028415. [Google Scholar] [CrossRef]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in Inflammation, Immunity, and Disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef] [PubMed]
- Vilotić, A.; Nacka-Aleksić, M.; Pirković, A.; Bojić-Trbojević, Z.; Dekanski, D.; Krivokuća, M.J. IL-6 and IL-8: An Overview of Their Roles in Healthy and Pathological Pregnancies. Int. J. Mol. Sci. 2022, 23, 14574. [Google Scholar] [CrossRef] [PubMed]
- Novak, T.; Hamedi, M.; Bergmeier, L.A.; Fortune, F.; Hagi-Pavli, E. Saliva and Serum Cytokine Profiles During Oral Ulceration in Behçet’s Disease. Front. Immunol. 2021, 12, 724900. [Google Scholar] [CrossRef] [PubMed]
- Abboud, C.S.; Brandão, E.H.d.S.; Cunha, K.R.L.; Brito, K.d.S.; Gallo, C.d.B.; Molon, A.C.; Horliana, A.C.R.T.; Franco, A.S.L.; Thongprasom, K.; Rodrigues, M.F.S.D. Serum and salivary cytokines in patients with oral lichen planus treated with Photobiomodulation. Oral Dis. 2021, 29, 1250–1258. [Google Scholar] [CrossRef]
- Markanday, A. Acute Phase Reactants in Infections: Evidence-Based Review and a Guide for Clinicians. Open Forum Infect. Dis. 2015, 2, ofv098. [Google Scholar] [CrossRef]
- Broyles, S.T.; Staiano, A.E.; Drazba, K.T.; Gupta, A.K.; Sothern, M.; Katzmarzyk, P.T. Elevated C-Reactive Protein in Children from Risky Neighborhoods: Evidence for a Stress Pathway Linking Neighborhoods and Inflammation in Children. PLoS ONE 2012, 7, e45419. [Google Scholar] [CrossRef]
- Kuppa, A.; Tripathi, H.; Al-Darraji, A.; Tarhuni, W.M.; Abdel-Latif, A. C-Reactive Protein Levels and Risk of Cardiovascular Diseases: A Two-Sample Bidirectional Mendelian Randomization Study. Int. J. Mol. Sci. 2023, 24, 9129. [Google Scholar] [CrossRef]
- Klimek, L.; Bergmann, K.-C.; Biedermann, T.; Bousquet, J.; Hellings, P.; Jung, K.; Merk, H.; Olze, H.; Schlenter, W.; Stock, P.; et al. Visual analogue scales (VAS): Measuring instruments for the documentation of symptoms and therapy monitoring in cases of allergic rhinitis in everyday health care: Position Paper of the German Society of Allergology (AeDA) and the German Society of Allergy and Clinical Immunology (DGAKI), ENT Section, in collaboration with the working group on Clinical Immunology, Allergology and Environmental Medicine of the German Society of Otorhinolaryngology, Head and Neck Surgery (DGHNOKHC). Allergo J. Int. 2017, 26, 16–24. [Google Scholar] [CrossRef]
- Sahibzada, H.A.; Khurshid, Z.; Khan, R.S.; Naseem, M.; Siddique, K.M.; Mali, M.; Zafar, M.S. Salivary IL-8, IL-6 and TNF-α as Potential Diagnostic Biomarkers for Oral Cancer. Diagnostics 2017, 7, 21. [Google Scholar] [CrossRef]
- Ouellet-Morin, I.; Danese, A.; Williams, B.; Arseneault, L. Validation of a high-sensitivity assay for C-reactive protein in human saliva. Brain, Behav. Immun. 2011, 25, 640–646. [Google Scholar] [CrossRef]
- Dineshkumar, T.; Ashwini, B.K.; Rameshkumar, A.; Rajashree, P.; Ramya, R.; Rajkumar, K. Salivary and Serum Interleukin-6 Levels in Oral Premalignant Disorders and Squamous Cell Carcinoma: Diagnostic Value and Clinicopathologic Correlations. Asian Pac. J. Cancer Prev. 2016, 17, 4899–4906. [Google Scholar] [CrossRef]
- Azar, R.; Richard, A. Elevated salivary C-reactive protein levels are associated with active and passive smoking in healthy youth: A pilot study. J. Inflamm. 2011, 8, 37. [Google Scholar] [CrossRef] [PubMed]
- Cennamo, N.; Piccirillo, A.; Bencivenga, D.; Arcadio, F.; Annunziata, M.; Della Ragione, F.; Guida, L.; Zeni, L.; Borriello, A. Towards a point-of-care test to cover atto-femto and pico-nano molar concentration ranges in interleukin 6 detection exploiting PMMA-based plasmonic biosensor chips. Talanta 2023, 256, 124284. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, J.; Lambert, M.; Karp, I.; McGrath, J.; Gray-Donald, K.; Barnett, T.A.; Delvin, E.E.; Levy, E.; Paradis, G. Association between cigarette smoking and C-reactive protein in a representative, population-based sample of adolescents. Nicotine Tob. Res. 2008, 10, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Zafar, M.S.; Fareed, M.A.; Riaz, S.; Latif, M.; Habib, S.R.; Khurshid, Z. Customized Therapeutic Surface Coatings for Dental Implants. Coatings 2020, 10, 568. [Google Scholar] [CrossRef]
- Lahoti, K.; Dandekar, S.; Gade, J.; Agrawal, M. Comparative evaluation of crestal bone level by flapless and flap techniques for implant placement: Systematic review and meta-analysis. J. Indian Prosthodont. Soc. 2021, 21, 328–338. [Google Scholar] [CrossRef]
- Carosi, P.; Lorenzi, C.; Lio, F.; Cardelli, P.; Pinto, A.; Laureti, A.; Pozzi, A. Accuracy of Computer-Assisted Flapless Implant Placement by Means of Mucosa-Supported Templates in Complete-Arch Restorations: A Systematic Review. Materials 2022, 15, 1462. [Google Scholar] [CrossRef]
- Wachol, K.; Morawiec, T.; Nowak-Wachol, A.; Kubaszek, B.; Kasprzyk-Kucewicz, T.; Baldi, D.; Machorowska-Pieniążek, A.; Skucha-Nowak, M.; Cholewka, A. Comparative Analysis of Implant Prosthesis Treatment Planning and Execution Following Bone Repair Procedures Using Dynamic Surgical Navigation in Augmented Areas. Coatings 2022, 12, 1099. [Google Scholar] [CrossRef]
- Bhalerao, A.; Marimuthu, M.; Wahab, A.; Ayoub, A. Flapless placement of zygomatic implants using dynamic navigation: An innovative technical note. Br. J. Oral Maxillofac. Surg. 2022, 61, 136–140. [Google Scholar] [CrossRef]
- Kasprzyk-Kucewicz, T.; Cholewka, A.; Bałamut, K.; Kownacki, P.; Kaszuba, N.; Kaszuba, M.; Stanek, A.; Sieroń, K.; Stransky, J.; Pasz, A.; et al. The applications of infrared thermography in surgical removal of retained teeth effects assessment. J. Therm. Anal. Calorim. 2020, 144, 139–144. [Google Scholar] [CrossRef]
- Kaszuba, N.; Kasprzyk-Kucewicz, T.; Szurko, A.; Wziatek-Kuczmik, D.; Stanek, A.; Morawiec, T.; Cholewka, A. How to use thermal imaging in selected surgical dental procedures? Thermol. Int. 2021, 31, 172–181. [Google Scholar]
- Morawiec, T.; Dziedzic, A.; Niedzielska, I.; Mertas, A.; Tanasiewicz, M.; Skaba, D.; Kasperski, J.; Machorowska-Pieniążek, A.; Kucharzewski, M.; Szaniawska, K.; et al. The Biological Activity of Propolis-Containing Toothpaste on Oral Health Environment in Patients Who Underwent Implant-Supported Prosthodontic Rehabilitation. Evidence-Based Complement. Altern. Med. 2013, 2013, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wiatrak, K.; Morawiec, T.; Rój, R.; Kownacki, P.; Nitecka-Buchta, A.; Niedzielski, D.; Wychowański, P.; Machorowska-Pieniążek, A.; Cholewka, A.; Baldi, D.; et al. Evaluation of Effectiveness of a Toothpaste Containing Tea Tree Oil and Ethanolic Extract of Propolis on the Improvement of Oral Health in Patients Using Removable Partial Dentures. Molecules 2021, 26, 4071. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.; Dhadse, P.; Bajaj, P.; Sethiya, K.; Subhadarsanee, C. Pre-procedural Antimicrobial Mouth Rinse: A Concise Review. Cureus 2022, 14, e30629. [Google Scholar] [CrossRef]
- Pałka, Ł.; Nowakowska-Toporowska, A.; Dalewski, B. Is Chlorhexidine in Dentistry an Ally or a Foe? A Narrative Review. Healthcare 2022, 10, 764. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| aged 18–65 years | critical systemic disease (ASA III-IV) |
| absence of systemic disease comorbidities | generalised immunodeficiency |
| adequate oral hygiene (API < 15%) | autoimmune disease |
| clinically and radiologically diagnosed inflammatory conditions (active caries, gingivitis and periodontitis, mucosal diseases, e.g., leukoplakia, lichen planus) | |
| active nicotinism | |
| use of antibiotics in the past 2 weeks |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wachol, K.; Morawiec, T.; Szurko, A.; Baldi, D.; Nowak-Wachol, A.; Śmieszek-Wilczewska, J.; Mertas, A. Advantages of Dynamic Navigation in Prosthetic Implant Treatment in Terms of the Clinical Evaluation and Salivary Pro-Inflammatory Biomarkers: A Clinical Study. Appl. Sci. 2023, 13, 9866. https://doi.org/10.3390/app13179866
Wachol K, Morawiec T, Szurko A, Baldi D, Nowak-Wachol A, Śmieszek-Wilczewska J, Mertas A. Advantages of Dynamic Navigation in Prosthetic Implant Treatment in Terms of the Clinical Evaluation and Salivary Pro-Inflammatory Biomarkers: A Clinical Study. Applied Sciences. 2023; 13(17):9866. https://doi.org/10.3390/app13179866
Chicago/Turabian StyleWachol, Kacper, Tadeusz Morawiec, Agnieszka Szurko, Domenico Baldi, Anna Nowak-Wachol, Joanna Śmieszek-Wilczewska, and Anna Mertas. 2023. "Advantages of Dynamic Navigation in Prosthetic Implant Treatment in Terms of the Clinical Evaluation and Salivary Pro-Inflammatory Biomarkers: A Clinical Study" Applied Sciences 13, no. 17: 9866. https://doi.org/10.3390/app13179866