
Evaluation of the Retentive Forces from Removable Partial Denture Clasps Manufactured by the Digital Method
 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
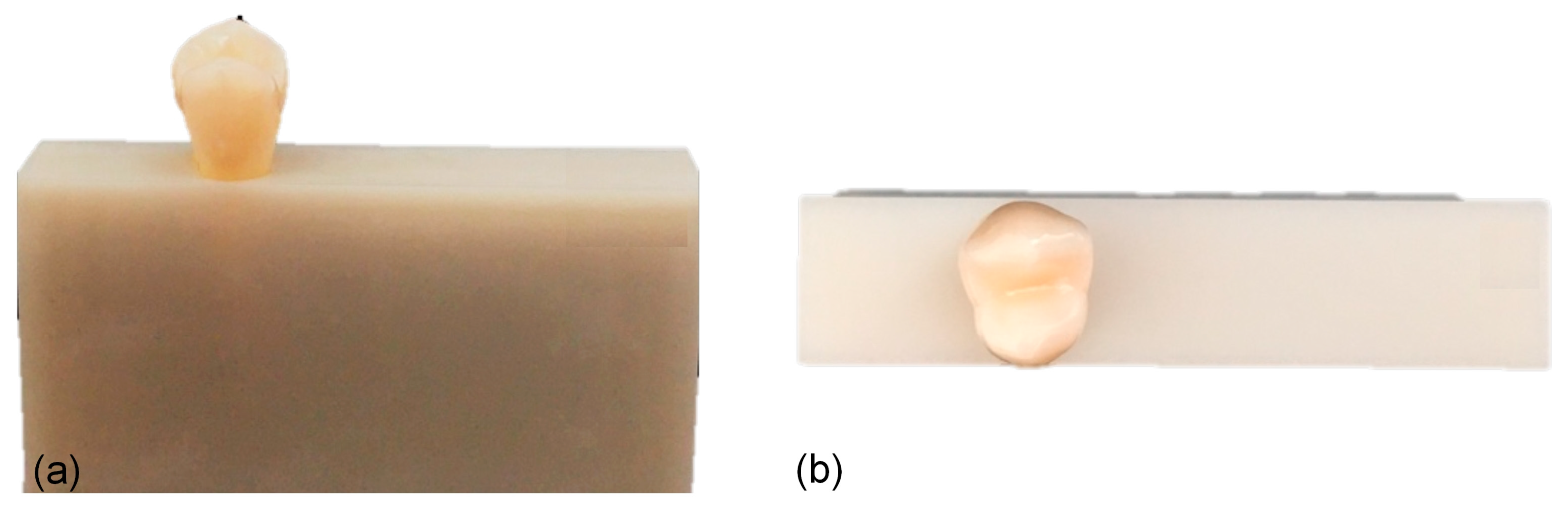
2.1. Production of Models
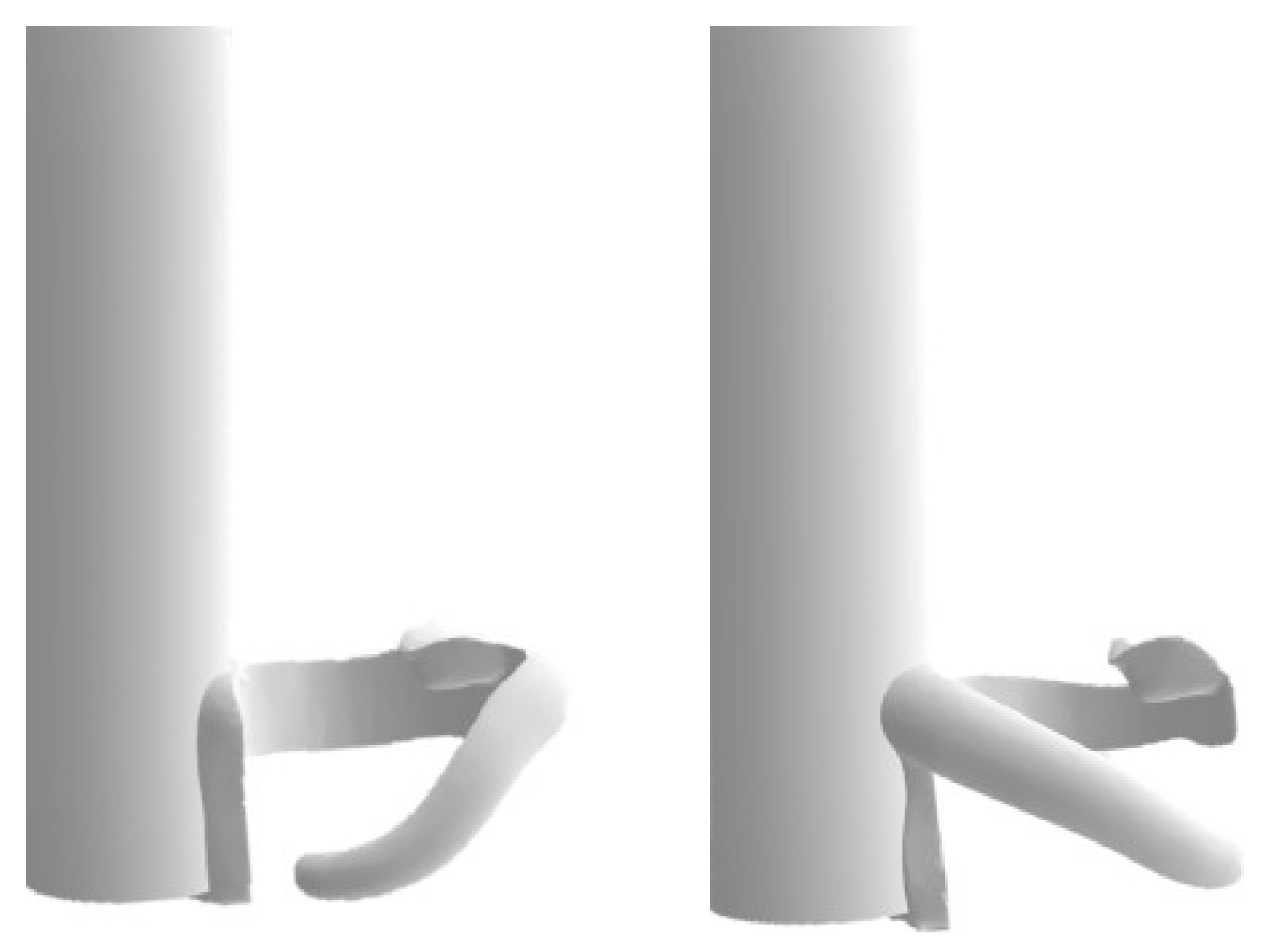
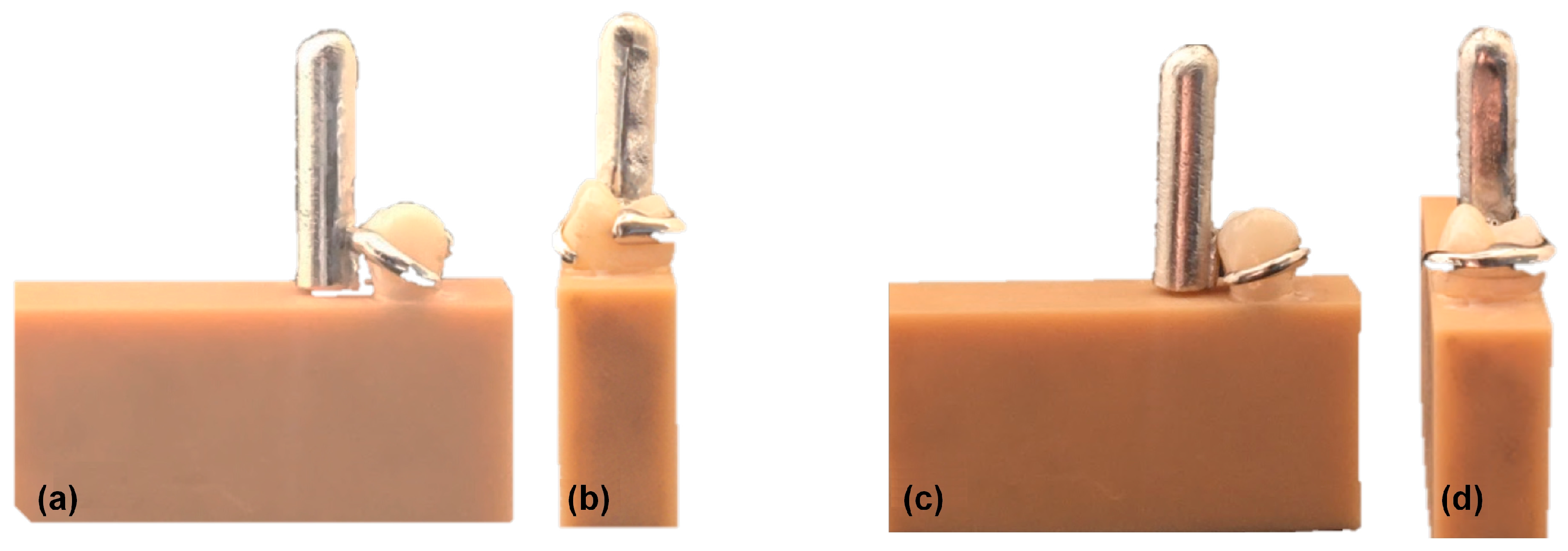
2.2. Production of Clasps
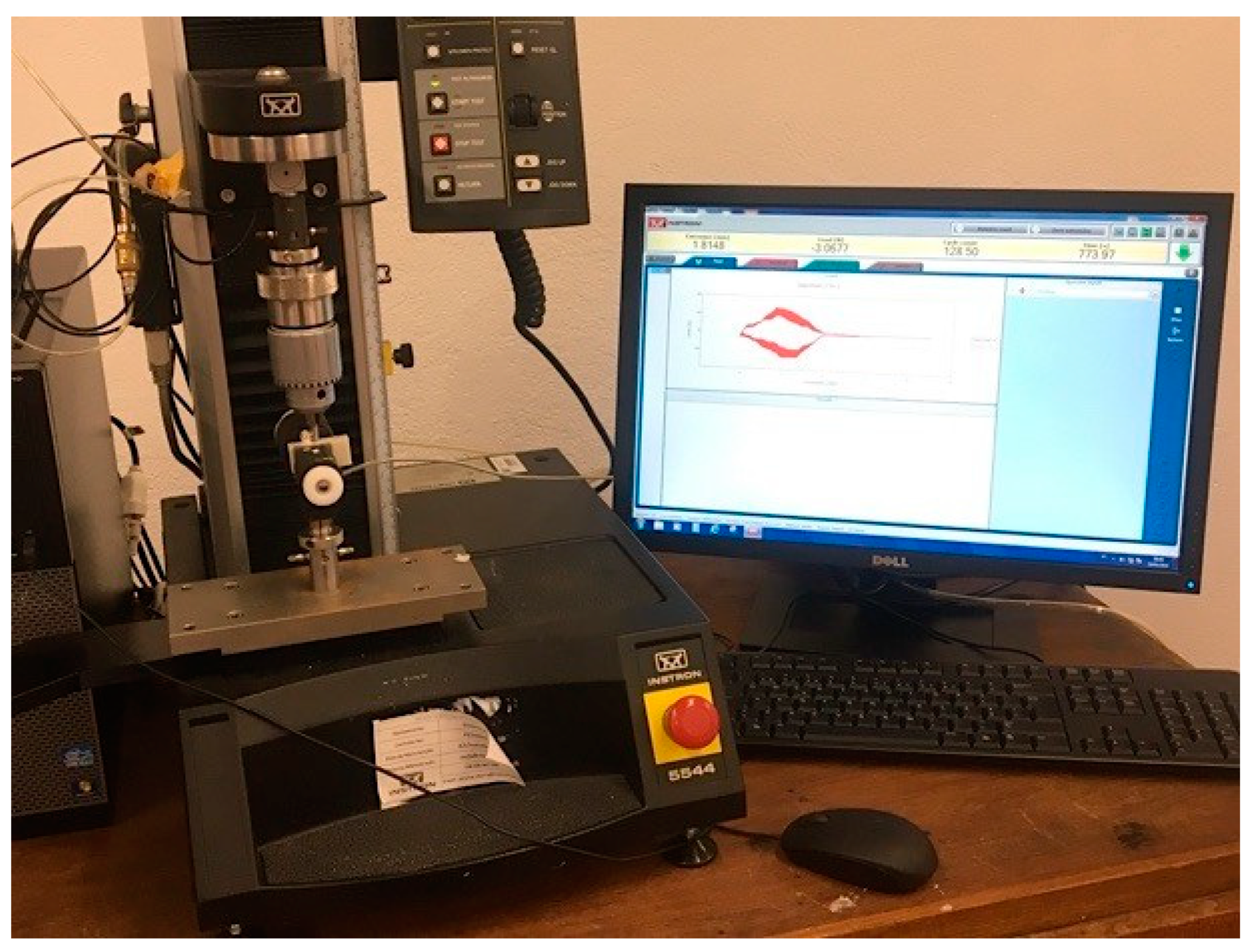
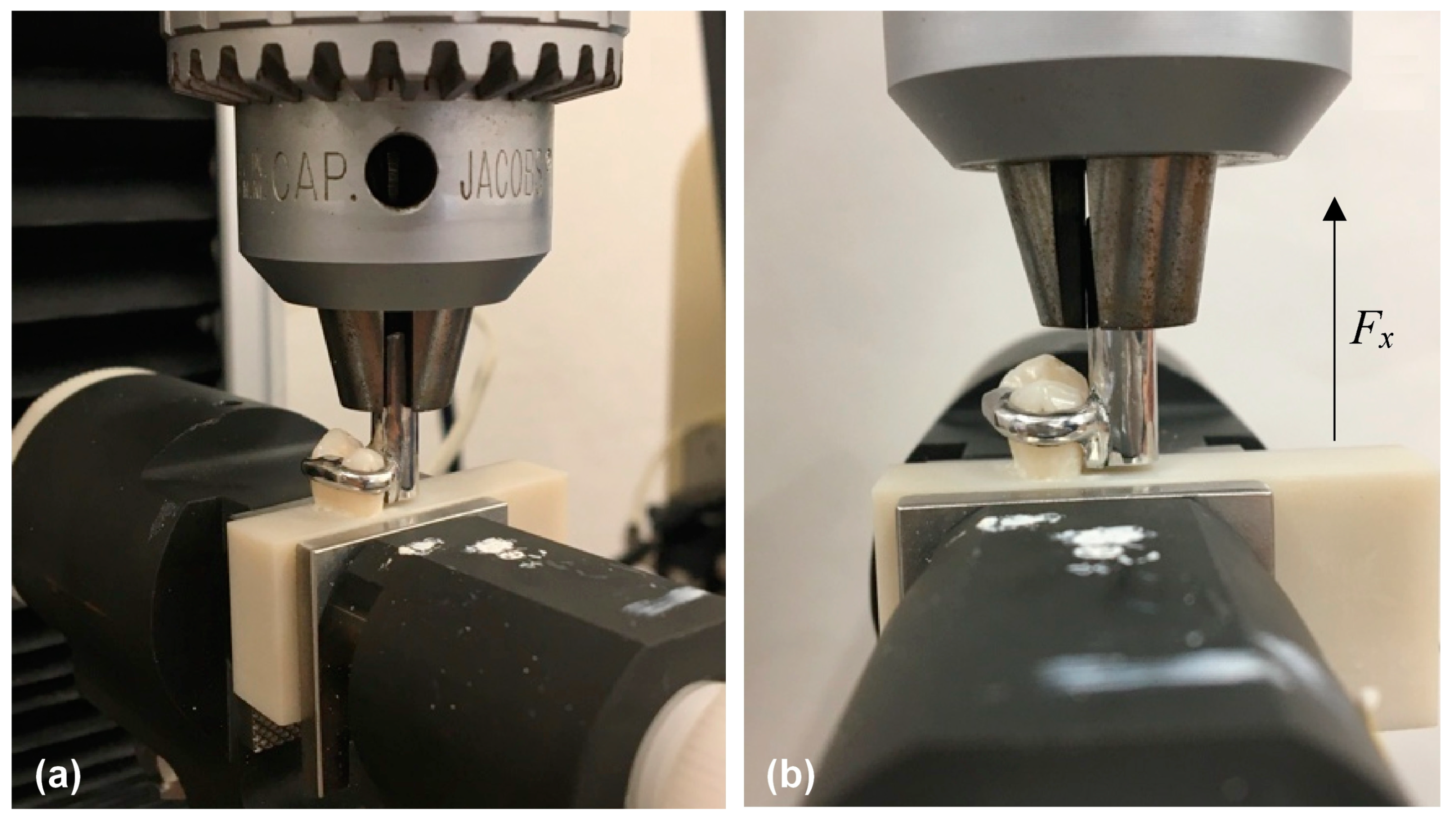
2.3. Test Conditions
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
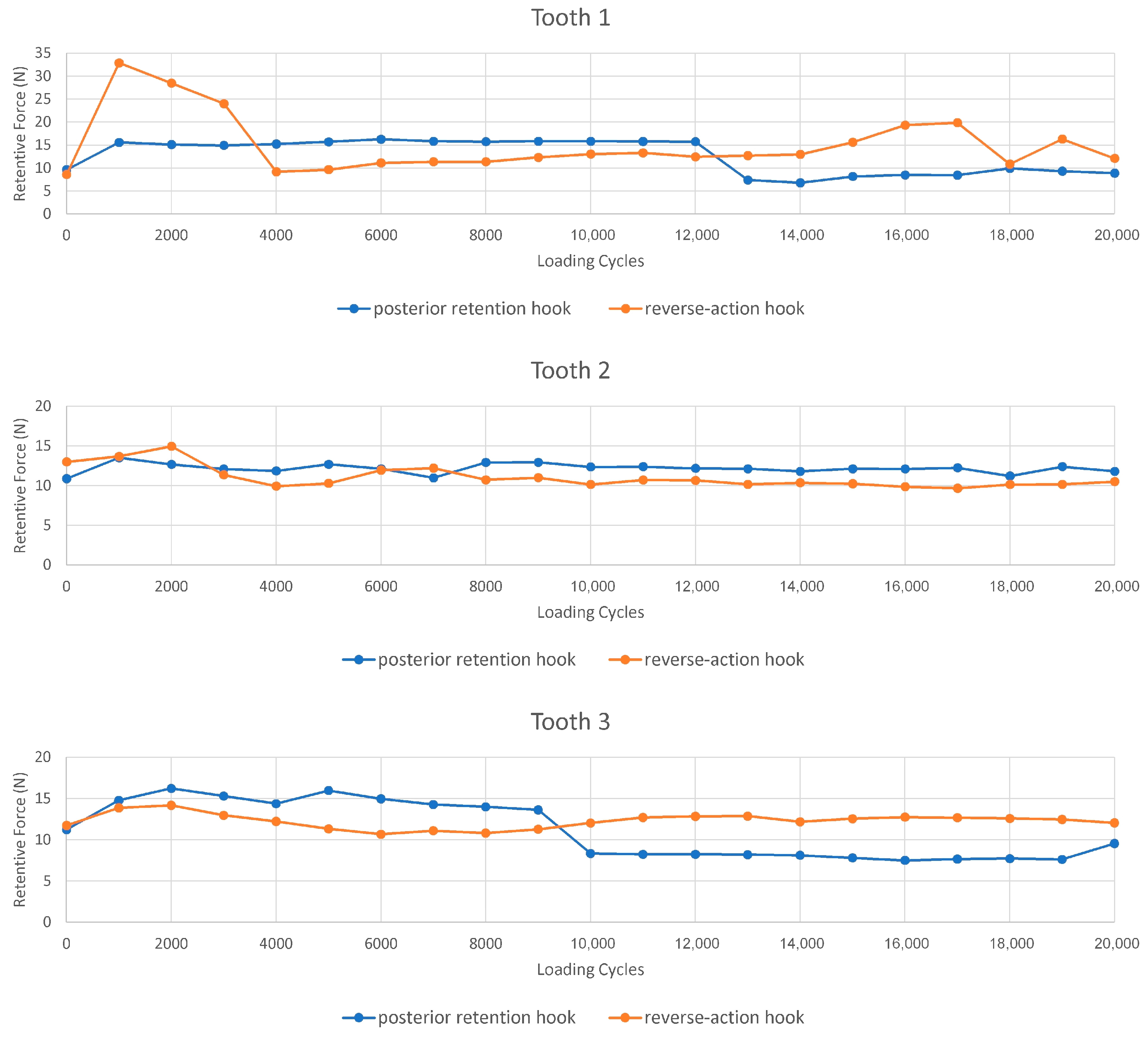
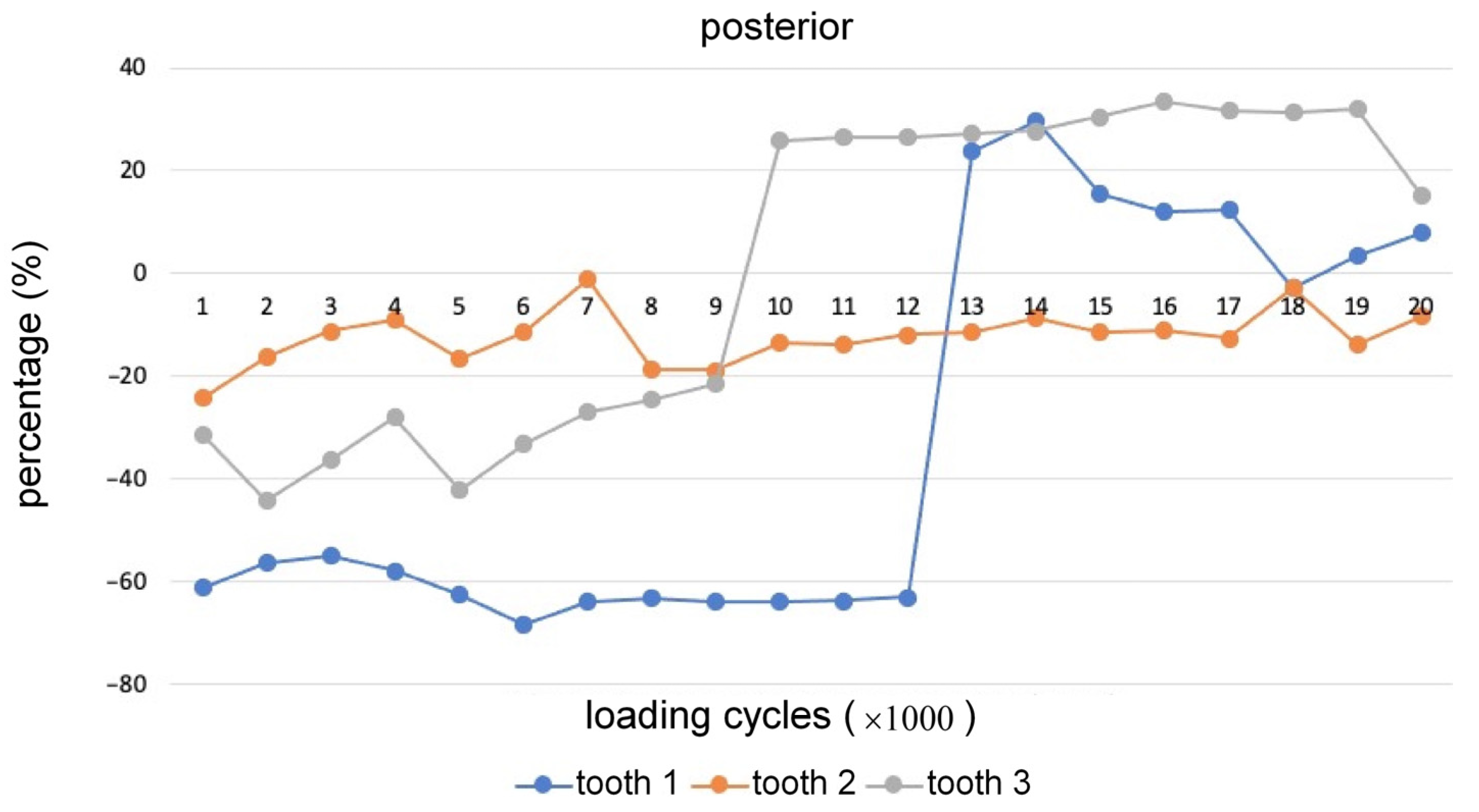
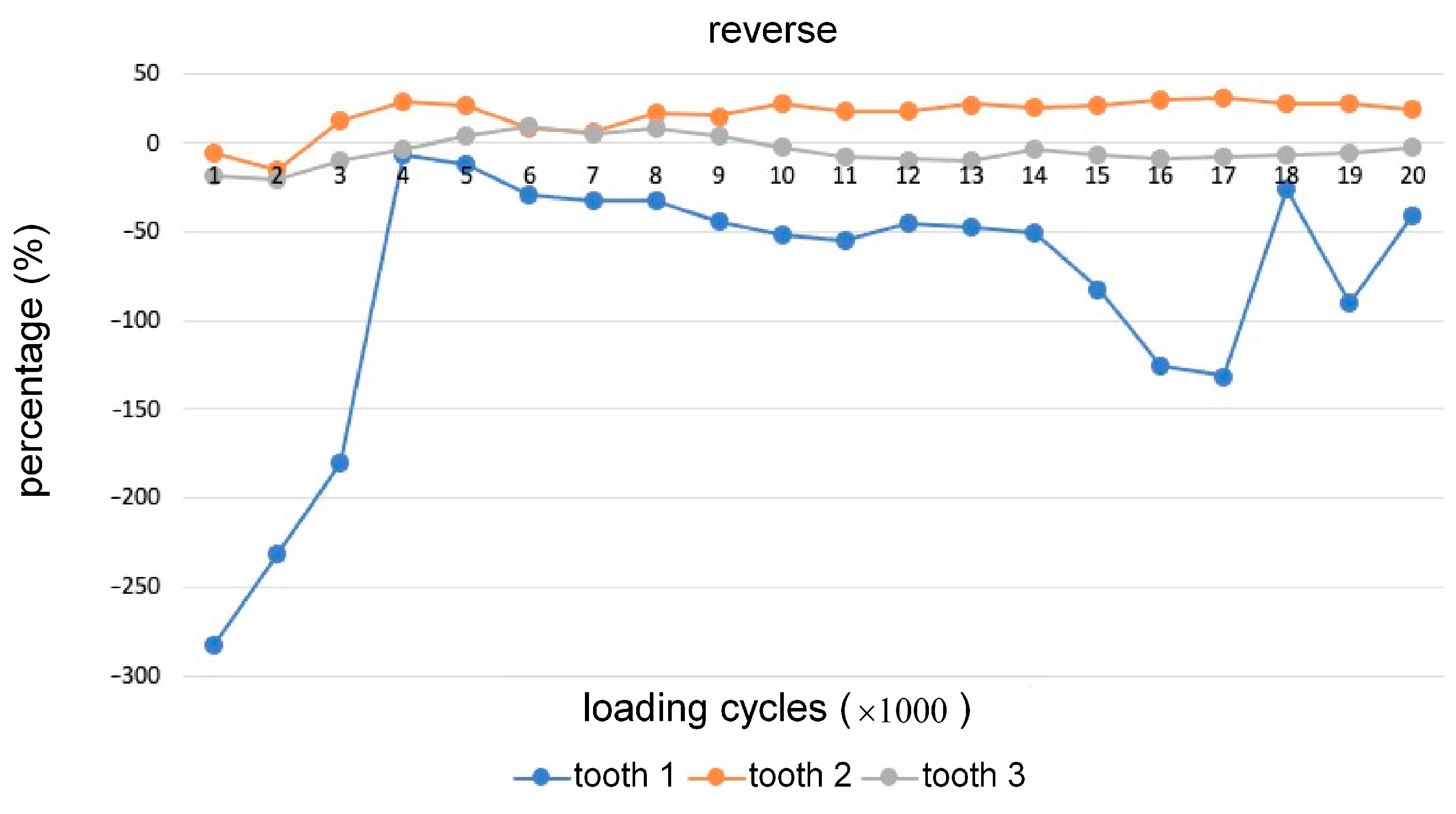
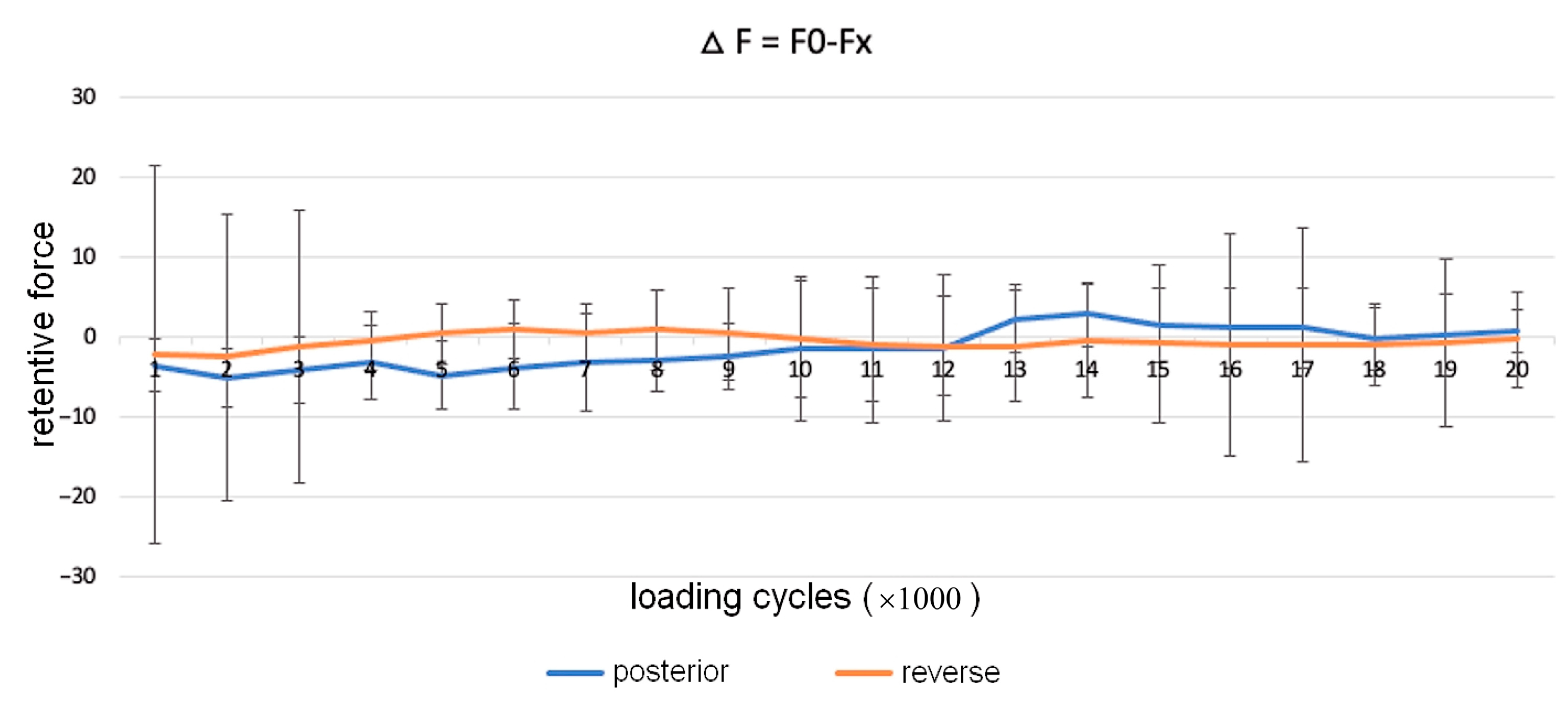
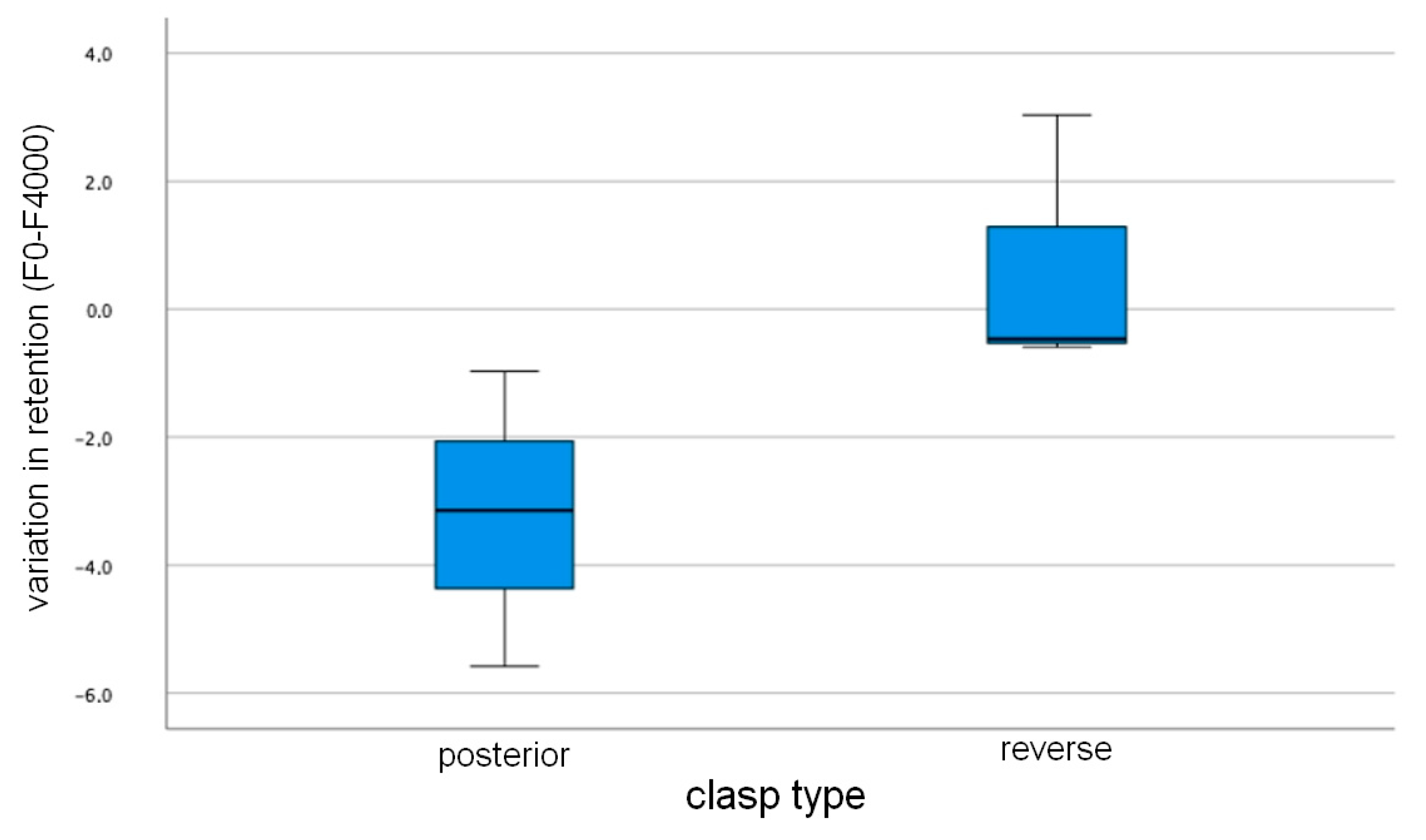
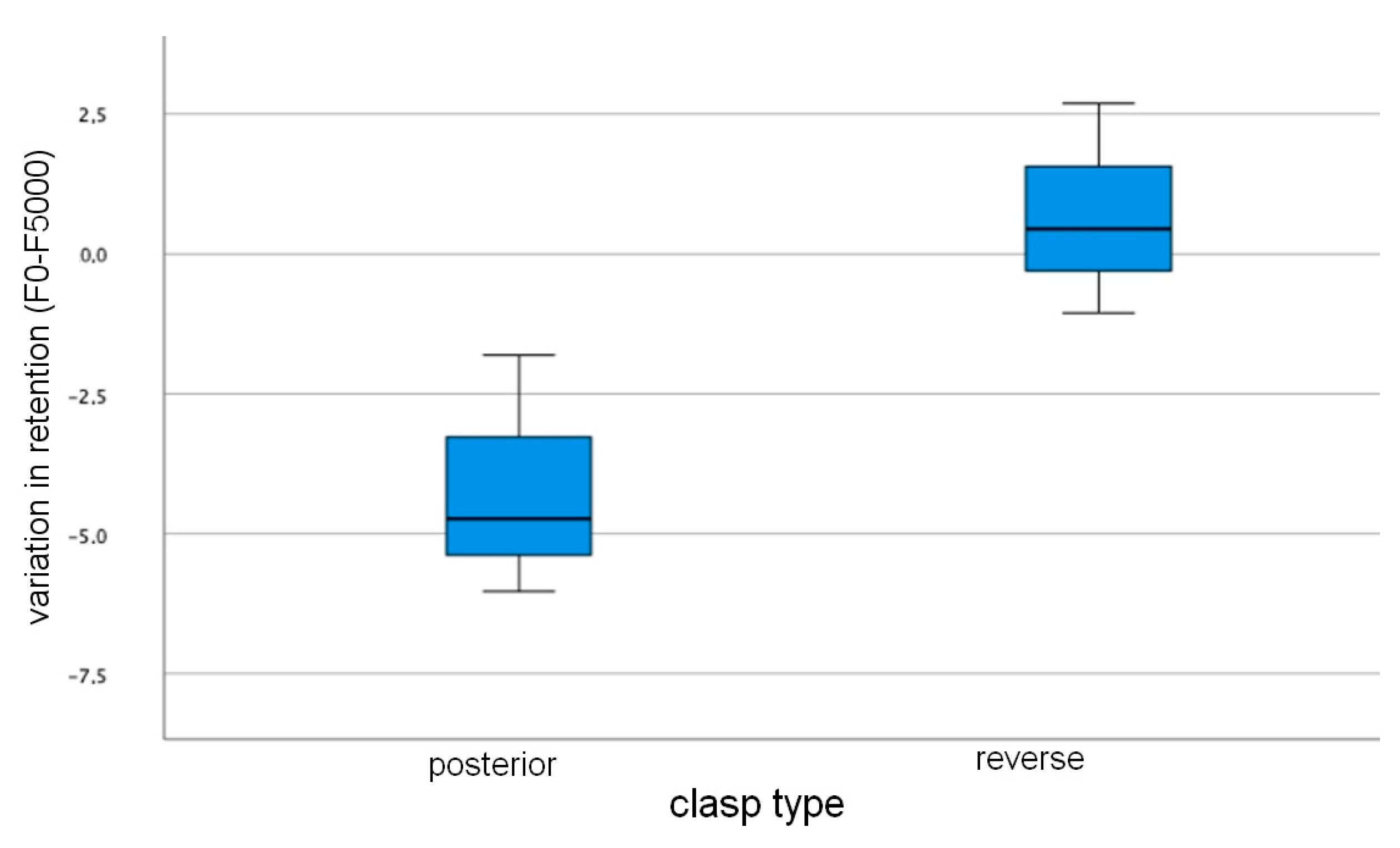
- Over 20,000 cycles, a reduced change in retention was verified in the clasps produced by the digital method, regardless of the type of clasp studied, which means that it will lose little retention over time.
- From this study, it can also be concluded that for most of the load cycles studied, no difference is observed between the changes in retention for the two types of clasps, leading to the conclusion that the design of the clasp does not have a great influence on the retentive force.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Bajunaid, S.O.; Altwaim, B.; Alhassan, M.; Alammari, R. The Fit Accuracy of Removable Partial Denture Metal Frameworks Using Conventional and 3D Printed Techniques: An in Vitro Study. J. Contemp. Dent. Pract. 2019, 20, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J. Revisiting the Removable Partial Denture. Dent. Clin. 2019, 63, 263–278. [Google Scholar] [CrossRef]
- Lima, J.M.C.; Anami, L.C.; Araujo, R.M.; Pavanelli, C.A. Removable Partial Dentures: Use of Rapid Prototyping. J. Prosthodont. 2014, 23, 588–591. [Google Scholar] [CrossRef] [PubMed]
- Schweiger, J.; Güth, J.-F.; Erdelt, K.-J.; Edelhoff, D.; Schubert, O. Internal Porosities, Retentive Force, and Survival of Cobalt-Chromium Alloy Clasps Fabricated by Selective Laser-Sintering. J. Prosthodont. Res. 2020, 64, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Benso, B.; Kovalik, A.C.; Jorge, J.H.; Campanha, N.H. Failures in the Rehabilitation Treatment with Removable Partial Dentures. Acta Odontol. Scand. 2013, 71, 1351–1355. [Google Scholar] [CrossRef] [PubMed]
- Almufleh, B.; Emami, E.; Alageel, O.; de Melo, F.; Seng, F.; Caron, E.; Abi Nader, S.; Al-Hashedi, A.; Albuquerque, R.; Feine, J. Patient Satisfaction with Laser-Sintered Removable Partial Dentures: A Crossover Pilot Clinical Trial. J. Prosthet. Dent. 2018, 119, 560–567. [Google Scholar] [CrossRef]
- Lang, L.A.; Tulunoglu, I. A Critically Appraised Topic Review of Computer-Aided Design/Computer-Aided Machining of Removable Partial Denture Frameworks. Dent. Clin. 2014, 58, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Tannous, F.; Steiner, M.; Shahin, R.; Kern, M. Retentive Forces and Fatigue Resistance of Thermoplastic Resin Clasps. Dent. Mater. 2012, 28, 273–278. [Google Scholar] [CrossRef] [Green Version]
- Alageel, O.; Abdallah, M.-N.; Alsheghri, A.; Song, J.; Caron, E.; Tamimi, F. Removable Partial Denture Alloys Processed by Laser-Sintering Technique. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018, 106, 1174–1185. [Google Scholar] [CrossRef]
- Campbell, S.D.; Cooper, L.; Craddock, H.; Hyde, T.P.; Nattress, B.; Pavitt, S.H.; Seymour, D.W. Removable Partial Dentures: The Clinical Need for Innovation. J. Prosthet. Dent. 2017, 118, 273–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, H.H.-M.; Chou, C.-W.; Chen, Y.-J.; Yao, C.-C.J. An Overview of Digital Intraoral Scanners: Past, Present and Future-from an Orthodontic Perspective. Taiwan. J. Orthod. 2018, 30, 3. [Google Scholar]
- Frank, R.P.; Brudvik, J.S.; Leroux, B.; Milgrom, P.; Hawkins, N. Relationship between the Standards of Removable Partial Denture Construction, Clinical Acceptability, and Patient Satisfaction. J. Prosthet. Dent. 2000, 83, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Bohnenkamp, D.M. Removable Partial Dentures: Clinical Concepts. Dent. Clin. 2014, 58, 69–89. [Google Scholar]
- Arnold, C.; Hey, J.; Schweyen, R.; Setz, J.M. Accuracy of CAD-CAM-Fabricated Removable Partial Dentures. J. Prosthet. Dent. 2018, 119, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Helal, M.A.; Baraka, O.A.; Sanad, M.E.; Ludwig, K.; Kern, M. Effects of Long-Term Simulated RPD Clasp Attachment/Detachment on Retention Loss and Wear for Two Clasp Types and Three Abutment Material Surfaces. J. Prosthodont. Implant Esthet. Reconstr. Dent. 2012, 21, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Kato, Y.; Tasaka, A.; Kato, M.; Wadachi, J.; Takemoto, S.; Yamashita, S. Effects of Repetitive Insertion/Removal Cycles and Simulated Occlusal Loads on Retention of Denture Retainers. Dent. Mater. J. 2021, 40, 1277–1283. [Google Scholar] [CrossRef] [PubMed]
- Tribst, J.P.M.; Dal Piva, A.M.d.O.; Borges, A.L.S.; Araújo, R.M.; da Silva, J.M.F.; Bottino, M.A.; Kleverlaan, C.J.; de Jager, N. Effect of Different Materials and Undercut on the Removal Force and Stress Distribution in Circumferential Clasps during Direct Retainer Action in Removable Partial Dentures. Dent. Mater. 2020, 36, 179–186. [Google Scholar] [CrossRef]
- Kim, S.Y.; Shin, S.-Y.; Lee, J.H. Effect of Cyclic Bend Loading on a Cobalt-Chromium Clasp Fabricated by Direct Metal Laser Sintering. J. Prosthet. Dent. 2018, 119, 1027-e1. [Google Scholar] [CrossRef]
- Hakkoum, M.A. New Clasp Assembly for Distal Extension Removable Partial Dentures: The Reverse RPA Clasp. J. Prosthodont. 2016, 25, 411–413. [Google Scholar] [CrossRef]
- Eliason, C.M. RPA Clasp Design for Distal-Extension Removable Partial Dentures. J. Prosthet. Dent. 1983, 49, 25–27. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Xu, M.; Zhang, H.; Wu, W.; Zheng, M.; Li, X. Cyclic Fatigue Properties of Cobalt-Chromium Alloy Clasps for Partial Removable Dental Prostheses. J. Prosthet. Dent. 2010, 104, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Puskar, T.; Jevremovic, D.; Williams, R.J.; Eggbeer, D.; Vukelic, D.; Budak, I. A Comparative Analysis of the Corrosive Effect of Artificial Saliva of Variable PH on DMLS and Cast Co-Cr-Mo Dental Alloy. Materials 2014, 7, 6486–6501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dikova, T. Properties of Co-Cr Dental Alloys Fabricated Using Additive Technologies; [Internet]; Biomaterials in Regenerative Medicine; InTech: London, UK, 2018. [Google Scholar] [CrossRef] [Green Version]
- Rist, K.; Cimic, S. Selective Laser Melting Technique in Fabrication of Partial Denture Metal Framework. Res. J. Pharm. Biol. Chem. Sci. 2016, 7, 2039–2043. [Google Scholar]
- Conceição, P.; Portugal, J.; Franco, M.; Alves, N.M.; Marques, D.; Neves, C.B. Comparison between Digital Superimposition and Microcomputed Tomography Methods of Fit Assessment of Removable Partial Denture Frameworks. J. Prosthet. Dent. 2023, 6. [Google Scholar] [CrossRef] [PubMed]
- Anan, M.T.M.; Al-Saadi, M.H. Fit Accuracy of Metal Partial Removable Dental Prosthesis Frameworks Fabricated by Traditional or Light Curing Modeling Material Technique: An in Vitro Study. Saudi Dent. J. 2015, 27, 149–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, A.L.C.; de Medeiros, A.K.B.; de Sousa Santos, K.; de Almeida, É.O.; Barbosa, G.A.S.; Carreiro, A. da F.P. Accuracy of CAD-CAM Systems for Removable Partial Denture Framework Fabrication: A Systematic Review. J. Prosthet. Dent. 2021, 125, 241–248. [Google Scholar] [CrossRef]
- Alghazzawi, T.F. Advancements in CAD/CAM Technology: Options for Practical Implementation. J. Prosthodont. Res. 2016, 60, 72–84. [Google Scholar] [CrossRef]
- Bilgin, M.S.; Baytaroğlu, E.N.; Erdem, A.; Dilber, E. A Review of Computer-Aided Design/Computer-Aided Manufacture Techniques for Removable Denture Fabrication. Eur. J. Dent. 2016, 10, 286–291. [Google Scholar] [CrossRef] [Green Version]
- Abduo, J.; Lyons, K.; Bennamoun, M. Trends in Computer-Aided Manufacturing in Prosthodontics: A Review of the Available Streams. Int. J. Dent. 2014, 2014, 783948. [Google Scholar] [CrossRef] [PubMed]
- Conceição, P.R.; Pinto, R.; Marques, D.; Portugal, J.; Neves, C.B.; Franco, M.; Alves, N. Fit Accuracy Assessment of RPD Metal Framework by Digital Superimposition. In Advances and Current Trends in Biomechanics; Belinha, J., Campos, J.C.R., Fonseca, E., Silva, M.H.F., Marques, M.A., Costa, M.F.G., Oliveira, S., Eds.; CRC Press: Boca Raton, FL, USA, 2022; pp. 331–334. [Google Scholar] [CrossRef]
- Venkatesh, K.V.; Nandini, V.V. Direct Metal Laser Sintering: A Digitised Metal Casting Technology. J. Indian Prosthodont. Soc. 2013, 13, 389–392. [Google Scholar] [CrossRef]
- Revilla-León, M.; Özcan, M. Additive Manufacturing Technologies Used for 3D Metal Printing in Dentistry. Curr. Oral Health Rep. 2017, 4, 201–208. [Google Scholar] [CrossRef] [Green Version]
- Torii, M.; Nakata, T.; Takahashi, K.; Kawamura, N.; Shimpo, H.; Ohkubo, C. Fitness and Retentive Force of Cobalt-Chromium Alloy Clasps Fabricated with Repeated Laser Sintering and Milling. J. Prosthodont. Res. 2018, 62, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Conceição, P.R.; Franco, M.C.; Alves, N.; Portugal, J.; Neves, C.B. Fit Accuracy of Removable Partial Denture Metal Frameworks Produced by CAD-CAM–a Clinical Study. Rev. Port. Estomatol. Med. Dentária Cir. Maxilofac. 2021, 62, 194–200. [Google Scholar] [CrossRef]
- Phillips, R.W.; Leonard, L.J. A Study of Enamel Abrasion as Related to Partial Denture Clasps. J. Prosthet. Dent. 1956, 6, 657–671. [Google Scholar] [CrossRef]
- Rodrigues, R.C.S.; Ribeiro, R.F.; de Mattos, M.d.G.C.; Bezzon, O.L. Comparative Study of Circumferential Clasp Retention Force for Titanium and Cobalt-Chromium Removable Partial Dentures. J. Prosthet. Dent. 2002, 88, 290–296. [Google Scholar] [CrossRef]
- Tanaka, A.; Miyake, N.; Hotta, H.; Takemoto, S.; Yoshinari, M.; Yamashita, S. Change in the Retentive Force of Akers Clasp for Zirconia Crown by Repetitive Insertion and Removal Test. J. Prosthodont. Res. 2019, 63, 447–452. [Google Scholar] [CrossRef]
- Sato, Y.; Tsuga, K.; Abe, Y.; Asahara, S.; Akagawa, Y. Finite Element Analysis on Preferable I-Bar Clasp Shape. J. Oral Rehabil. 2001, 28, 413–417. [Google Scholar] [CrossRef]
- Kim, H.R.; Jang, S.H.; Kim, Y.K.; Son, J.S.; Min, B.K.; Kim, K.H.; Kwon, T.Y. Microstructures and Mechanical Properties of Co-Cr Dental Alloys Fabricated by Three CAD/CAM-Based Processing Techniques. Materials 2016, 9, 596. [Google Scholar] [CrossRef] [Green Version]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Back-Action Clasp | Reverse Back-Action Clasp | |||||||
|---|---|---|---|---|---|---|---|---|
| Cycles | Median | Amplitude Interquartile | Maximum | Mínimum | Median | Amplitude Interquartile | Maximum | Minimum |
| It 1000 | −3.53 | 3.263 | −2.64 | −5.90 | −2.12 | 23.587 | −0.69 | −24.28 |
| 2000 | −4.98 | 3.655 | −1.77 | −5.43 | −2.42 | 17.883 | −1.97 | −19.85 |
| 3000 | −4.07 | 4.062 | −1.22 | −5.28 | −1.21 | 17.044 | 1.62 | −15.41 |
| 4000 | −3.14 | 4.611 | −0.97 | −5.58 | −0.46 | 3.627 | 3.03 | −0.58 |
| 5000 | −4.73 | 4.221 | −1.80 | −6.03 | 0.44 | 3.738 | 2.68 | −1.05 |
| 6000 | −3.72 | 5.36 | −1.23 | −6.59 | 1.03 | 3.623 | 1.09 | −2.53 |
| 7000 | −3.04 | 6.050 | −0.10 | −6.16 | 0.65 | 3.576 | 0.77 | −2.79 |
| 8000 | −2.75 | 4.079 | −2.02 | −6.10 | 0.93 | 5.045 | 2.24 | −2.80 |
| 9000 | −2.40 | 4.115 | −2.05 | −6.16 | 0.48 | 5.730 | 1.98 | −3.74 |
| 10,000 | −1.46 | 9.067 | 2.89 | −6.16 | −0.27 | 7.272 | 2.83 | −4.43 |
| 11,000 | −1.50 | 9.133 | 2.98 | −6.14 | −0.93 | 6.987 | 2.27 | −4.71 |
| 12,000 | −1.29 | 9.069 | 2.98 | −6.08 | −1.09 | 6.183 | 2.32 | −3.86 |
| 13,000 | 2.27 | 4.284 | 3.04 | −1.23 | −1.11 | 6.923 | 2.82 | −4.10 |
| 14,000 | 2.84 | 4.053 | 3.11 | −0.93 | −0.42 | 6.993 | 2.62 | −4.36 |
| 15,000 | 1.49 | 4.658 | 3.42 | −1.23 | −0.79 | 9.792 | 2.75 | −7.04 |
| 16,000 | 1.16 | 4.955 | 3.74 | −1.21 | −0.98 | 13.844 | 3.11 | −10.73 |
| 17,000 | 1.18 | 4.939 | 3.56 | −1.37 | −0.92 | 14.591 | 3.31 | −11.27 |
| 18,000 | −0.27 | 3.850 | 3.52 | −0.32 | −0.82 | 5.109 | 2.85 | −2.25 |
| 19,000 | 0.32 | 5.120 | 3.61 | −1.50 | −0.70 | 10.531 | 2.82 | −7.70 |
| 20,000 | 0.76 | 2.602 | 1.68 | −0.91 | −0.29 | 6.006 | 2.48 | −3.52 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anes, V.; Neves, C.B.; Bostan, V.; Gonçalves, S.B.; Reis, L. Evaluation of the Retentive Forces from Removable Partial Denture Clasps Manufactured by the Digital Method. Appl. Sci. 2023, 13, 8072. https://doi.org/10.3390/app13148072
Anes V, Neves CB, Bostan V, Gonçalves SB, Reis L. Evaluation of the Retentive Forces from Removable Partial Denture Clasps Manufactured by the Digital Method. Applied Sciences. 2023; 13(14):8072. https://doi.org/10.3390/app13148072
Chicago/Turabian StyleAnes, Vitor, Cristina B. Neves, Valeria Bostan, Sérgio B. Gonçalves, and Luís Reis. 2023. "Evaluation of the Retentive Forces from Removable Partial Denture Clasps Manufactured by the Digital Method" Applied Sciences 13, no. 14: 8072. https://doi.org/10.3390/app13148072