
Analysis of Breath-Holding Capacity for Improving Efficiency of COPD Severity-Detection Using Deep Transfer Learning

 ,
,  ,
,  and
and
Abstract
:1. Introduction
- ○
- In order to maximize variance and minimize correlation between features of different lung disease types, a feature selection engine is deployed. This engine uses algorithms such as principal component analysis (PCA), independent component analysis (ICA), etc.
- ○
- The selected features are given to classification models like convolutional neural networks (CNNs), random forests (RF), support vector machines (SVMs), etc., for identification of disease types.
- ○
- The results of these models are post-processed via complex models like long-short-term-memory (LSTM) and gated recurrent units (GRUs) for performing temporal analysis on the classification results. These models aim at finding out results such as life expectancy and progression of disease.
2. Literature Review
3. Gated Recurrent Unit (GRU) Based Transfer Learning Model with Deep Convolutional Neural Networks (DCNNs) for COPD Analysis
- Horizontal flip and horizontal shift augmentation
- Vertical flip and vertical shift augmentation
- 2N Random rotation augmentation (N is the augmentation level)
- 2N Random Zoom Augmentation
- (2N) Random Brightness Augmentation
- Real time input images are given to an image augmentation layer, wherein 6N + 5 images are generated. These images are given to a feature extraction unit.
- The feature extraction unit is a combination of bidirectional GRU with recurrent neural networks, and produces a feature vector as shown in Figure 7.
- All of these features are given to a feature mapping unit that uses Quadratic support vector machine (QSVM) in order to find out the best matching training set image for the given input features as shown from Figure 8.
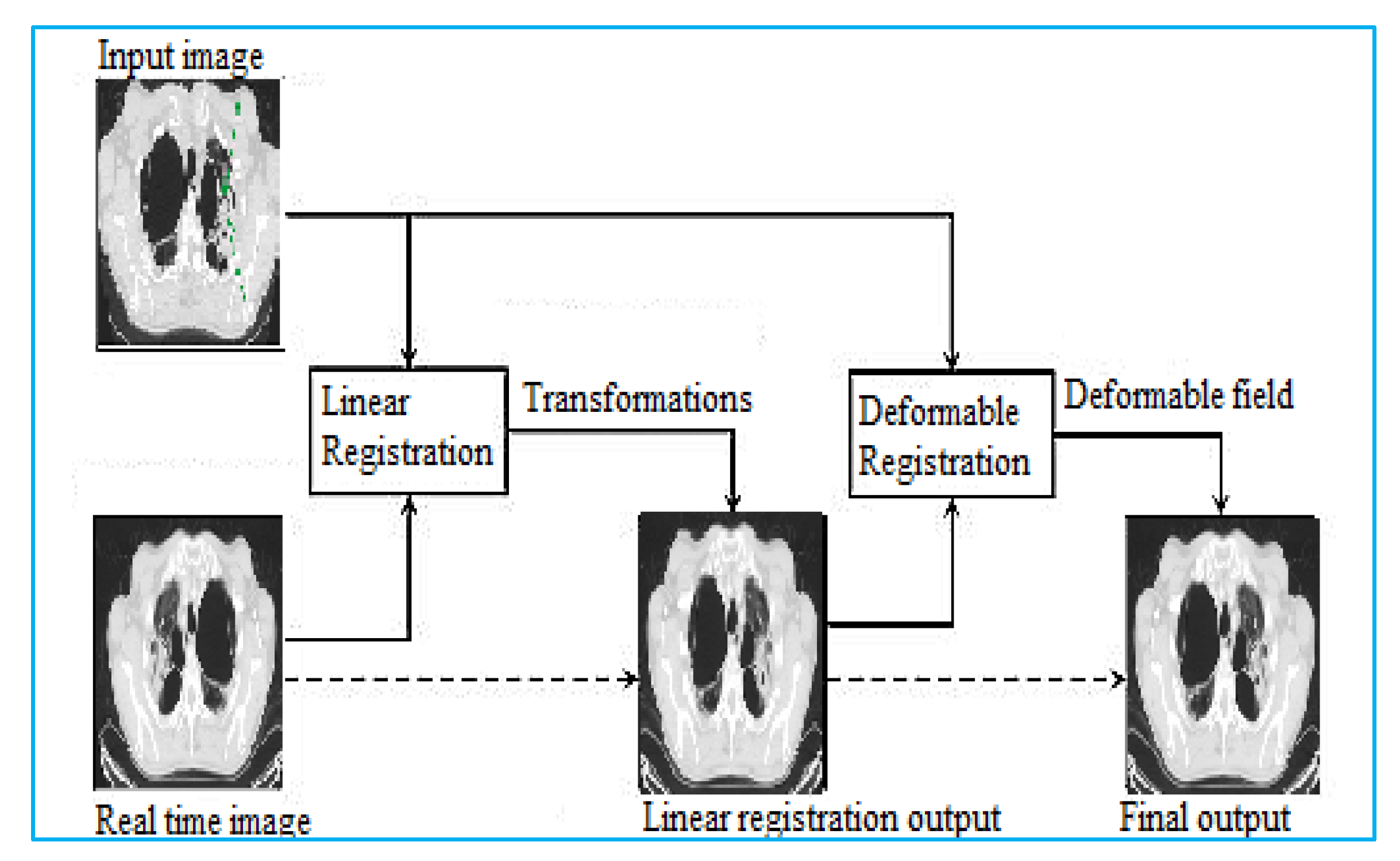
- Features of this selected training set image are merged with the input image using a linear & deformable image registration engine.
- The registration engine evaluates the input image (image from dataset) and the real time image (image to be classified), and passes them through linear registration model.
- The output of linear registration model is given to deformable registration model, wherein a deformable field is evaluated.
- Result of this field, is the deformable registered image, which can be further used for classification purposes as can be seen from Figure 9, where the entire registration process is shown.
- This registered image is given to the proposed ensemble CNN Model for final classification.
4. Results and Statistical Comparison
5. Conclusions & Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethical Approval
References
- Chronic Obstructive Pulmonary Disease (COPD). Available online: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd) (accessed on 10 May 2022).
- Rajasenbagam, T.; Jeyanthi, S.; Pandian, J.A. Detection of pneumonia infection in lungs from chest X-ray images using deep convolutional neural network and content-based image retrieval techniques. J. Ambient Intell. Humaniz. Comput. 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chagas, J.V.; Rodrigues, D.d.A.; Ivo, R.F.; Hassan, M.M.; de Albuquerque, V.H.; Filho, P.P. A new approach for the detection of pneumonia in children using CXR images based on an real-time IOT system. J. Real-Time Image Process. 2021, 18, 1099–1114. [Google Scholar] [CrossRef] [PubMed]
- El Asnaoui, K. Design ensemble deep learning model for pneumonia disease classification. Int. J. Multimed. Inf. Retr. 2021, 10, 55–68. [Google Scholar] [CrossRef] [PubMed]
- López-Cabrera, J.D.; Orozco-Morales, R.; Portal-Diaz, J.A.; Lovelle-Enríquez, O.; Pérez-Díaz, M. Current limitations to identify COVID-19 using artificial intelligence with chest X-ray imaging. Health Technol. 2021, 11, 411–424. [Google Scholar] [CrossRef]
- Rahman, S.; Sarker, S.; Miraj, M.A.; Nihal, R.A.; Nadimul Haque, A.K.; Noman, A.A. Deep learning–driven automated detection of COVID-19 from Radiography Images: A Comparative Analysis. Cogn. Comput. 2021. [Google Scholar] [CrossRef]
- Perumal, V.; Narayanan, V.; Rajasekar, S.J. Detection of COVID-19 using CXR and CT images using transfer learning and Haralick features. Appl. Intell. 2020, 51, 341–358. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Brown, L.G.; Foran, D.J.; Nosher, J.; Hacihaliloglu, I. Chest X-ray image phase features for improved diagnosis of COVID-19 using Convolutional Neural Network. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 197–206. [Google Scholar] [CrossRef]
- Ahuja, S.; Panigrahi, B.K.; Dey, N.; Rajinikanth, V.; Gandhi, T.K. Deep transfer learning-based automated detection of COVID-19 from lung CT scan slices. Appl. Intell. 2020, 51, 571–585. [Google Scholar] [CrossRef] [PubMed]
- Rasheed, J.; Hameed, A.A.; Djeddi, C.; Jamil, A.; Al-Turjman, F. A machine learning-based framework for diagnosis of COVID-19 from chest X-ray images. Interdiscip. Sci. Comput. Life Sci. 2021, 13, 103–117. [Google Scholar] [CrossRef]
- Ma, J.; Song, Y.; Tian, X.; Hua, Y.; Zhang, R.; Wu, J. Survey on deep learning for pulmonary medical imaging. Front. Med. 2019, 14, 450–469. [Google Scholar] [CrossRef]
- Sultan, L.R.; Chen, Y.T.; Cary, T.W.; Ashi, K.; Sehgal, C.M. Quantitative pleural line characterization outperforms traditional lung texture ultrasound features in detection of COVID-19. JACEP Open 2021, 2, e12418. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.; Nie, W.; Pan, L.; Zheng, B.; Shen, Z.; Huang, L.; Pei, C.; She, Y.; Chen, L. A dual-attention v-network for pulmonary lobe segmentation in CT scans. IET Image Process. 2021, 15, 1644–1654. [Google Scholar] [CrossRef]
- Irmak, E. COVID-19 Disease Severity Assessment using CNN model. IET Image Process. 2021, 15, 1814–1824. [Google Scholar] [CrossRef] [PubMed]
- Doddavarapu, V.N.; Kande, G.B.; Rao, B.P. Rotational invariant fractional derivative filters for lung tissue classification. IET Image Process. 2021, 15, 2202–2212. [Google Scholar] [CrossRef]
- Klimeš, F.; Voskrebenzev, A.; Gutberlet, M.; Kern, A.L.; Behrendt, L.; Grimm, R.; Suhling, H.; Crisosto, C.G.; Kaireit, T.F.; Pöhler, G.H.; et al. 3D phase-resolved functional lung ventilation MR imaging in healthy volunteers and patients with chronic pulmonary disease. Magn. Reson. Med. 2020, 85, 912–925. [Google Scholar] [CrossRef]
- Roy, S.; Menapace, W.; Oei, S.; Luijten, B.; Fini, E.; Saltori, C.; Huijben, I.; Chennakeshava, N.; Mento, F.; Sentelli, A.; et al. Deep learning for classification and localization of COVID-19 markers in point-of-care lung ultrasound. IEEE Trans. Med. Imaging 2020, 39, 2676–2687. [Google Scholar] [CrossRef]
- Anthimopoulos, M.; Christodoulidis, S.; Ebner, L.; Christe, A.; Mougiakakou, S. Lung pattern classification for interstitial lung diseases using a deep convolutional neural network. IEEE Trans. Med. Imaging 2016, 35, 1207–1216. [Google Scholar] [CrossRef]
- Neal Joshua, E.S.; Bhattacharyya, D.; Chakkravarthy, M.; Byun, Y.-C. 3D CNN with visual insights for early detection of lung cancer using gradient-weighted class activation. J. Healthc. Eng. 2021, 2021, 6695518. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Reddy Maddikunta, P.K.; Pham, Q.-V.; Gadekallu, T.R.; Krishnan, S.S.R.; Chowdhary, C.L.; Alazab, M.; Jalil Piran, M. Deep learning and medical image processing for coronavirus (COVID-19) pandemic: A survey. Sustain. Cities Soc. 2021, 65, 102589. [Google Scholar] [CrossRef]
- An, F.; Li, X.; Ma, X. Medical Image Classification algorithm based on visual attention mechanism-MCNN. Oxid. Med. Cell. Longev. 2021, 2021, 6280690. [Google Scholar] [CrossRef]
- Salem Salamh, A.B.; Salamah, A.A.; Akyüz, H.I. A study of a new technique of the CT Scan View and Disease Classification Protocol based on level challenges in cases of coronavirus disease. Radiol. Res. Pract. 2021, 2021, 5554408. [Google Scholar] [CrossRef] [PubMed]
- Zak, M.; Krzyżak, A. Classification of lung diseases using Deep Learning Models. In Proceedings of the International Conference on Computational Science, Amsterdam, The Netherlands, 3–5 June 2020; Lecture Notes in Computer Science. Springer: Berlin, Germany, 2020; pp. 621–634. [Google Scholar] [CrossRef]
- Muthazhagan, B.; Ravi, T.; Rajinigirinath, D. An enhanced computer-assisted lung cancer detection method using content based image retrieval and data mining techniques. J. Ambient Intell. Humaniz. Comput. 2020. [Google Scholar] [CrossRef]
- Trusculescu, A.A.; Manolescu, D.; Tudorache, E.; Oancea, C. Deep learning in interstitial lung disease—How long until daily practice. Eur. Radiol. 2020, 30, 6285–6292. [Google Scholar] [CrossRef]
- Farhat, H.; Sakr, G.E.; Kilany, R. Deep learning applications in Pulmonary Medical Imaging: Recent updates and insights on COVID-19. Mach. Vis. Appl. 2020, 31, 53. [Google Scholar] [CrossRef]
- Elaziz, M.A.; Hosny, K.M.; Salah, A.; Darwish, M.M.; Lu, S.; Sahlol, A.T. New Machine Learning Method for image-based diagnosis of COVID-19. PLoS ONE 2020, 15, e0235187. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Ji, G.P.; Zhou, Y.; Chen, G.; Fu, H.; Shen, J.; Shao, L. Inf-Net: Automatic COVID-19 Lung Infection Segmentation from CT Images. arXiv 2020, arXiv:2004.14133. [Google Scholar]
- Qin, R.X.; Wang, Z.; Jiang, L.Y.; Qiao, K.; Hai, J.; Chen, J.; Xu, J.; Shi, D.; Yan, B. Fine-grained lung cancer classification from PET and CT images based on multidimensional attention mechanism. Complexity 2020, 2020, 6153657. [Google Scholar] [CrossRef] [Green Version]
- Gupta, Y.K.; Agrawal, S. A Study of Lung Disease Using Image Processing in Big Data Environment. IOP Conf. Ser. Mater. Sci. Eng. 2021, 1022, 012030. Available online: https://iopscience.iop.org/article/10.1088/1757-899X/1022/1/012030/ (accessed on 2 June 2022).
- Du, R.; Qi, S.; Feng, J.; Xia, S.; Kang, Y.; Qian, W.; Yao, Y.-D. Identification of COPD from multi-view snapshots of 3D lung airway tree via Deep CNN. IEEE Access 2020, 8, 38907–38919. [Google Scholar] [CrossRef]
- Munawar, F.; Azmat, S.; Iqbal, T.; Gronlund, C.; Ali, H. Segmentation of lungs in chest x-ray image using generative adversarial networks. IEEE Access 2020, 8, 153535–153545. [Google Scholar] [CrossRef]
- Suzuki, K. Overview of deep learning in medical imaging. Radiol. Phys. Technol. 2017, 10, 257–273. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhou, Y.; Du, P.; Lang, G.; Xu, M.; Wu, W. A deep learning system that generates quantitative CT reports for diagnosing pulmonary tuberculosis. Appl. Intell. 2020, 51, 4082–4093. [Google Scholar] [CrossRef]
- Mlodzinski, E.; Stone, D.J.; Celi, L.A. Machine learning for pulmonary and Critical Care Medicine: A narrative review. Pulm. Ther. 2020, 6, 67–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, H.; Zhang, N.D.; Wu, X.; Zhang, Y.D. Multimodal Lung Tumor Image recognition algorithm based on integrated convolutional Neural Network. Concurr. Comput. Pract. Exper. 2018, 32, e4965. [Google Scholar] [CrossRef]
- Peng, J.; Chen, C.; Zhou, M.; Xie, X.; Zhou, Y.; Luo, C.-H. A machine-learning approach to forecast aggravation risk in patients with acute exacerbation of chronic obstructive pulmonary disease with clinical indicators. Sci. Rep. 2020, 10, 3118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mei, X.; Lee, H.-C.; Diao, K.-y.; Huang, M.; Lin, B.; Liu, C.; Xie, Z.; Ma, Y.; Robson, P.M.; Chung, M.; et al. Artificial Intelligence–enabled rapid diagnosis of patients with COVID-19. Nat. Med. 2020, 26, 1224–1228. [Google Scholar] [CrossRef] [PubMed]
- Parsa Hosseini, M.; Soltanian-Zadeh, H.; Akhlaghpoor, S. Detection and severity scoring of chronic obstructive pulmonary disease using volumetric analysis of lung CT images. Iran. J. Radiol. 2012, 9, 22–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Zhao, R.; Pang, M. A fully automatic segmentation algorithm for CT lung images based on random forest. Med. Phys. 2019, 47, 518–529. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Hasebe, T.; Tomita, K.; Kamei, S.; Matsumoto, T.; Imai, Y.; Takahashi, G.; Kondo, Y.; Ito, Y.; Sakamaki, F. Pulmonary perfusion by Chest Digital Dynamic Radiography: Comparison between breath-holding and Deep-breathing acquisition. J. Appl. Clin. Med. Phys. 2020, 21, 247–255. [Google Scholar] [CrossRef]
- Kirby, M.; Hatt, C.; Obuchowski, N.; Humphries, S.M.; Sieren, J.; Lynch, D.A.; Fain, S.B. Inter- and intra-software reproducibility of computed tomography lung density measurements. Med. Phys. 2020, 47, 2962–2969. [Google Scholar] [CrossRef]
- Hasse, K.; Hsieh, S.S.; O’Connell, D.; Stiehl, B.; Min, Y.; Neylon, J.; Low, D.A.; Santhanam, A.P. Systematic feasibility analysis of performing elastography using reduced dose CT Lung Image pairs. Med. Phys. 2020, 47, 3369–3375. [Google Scholar] [CrossRef] [PubMed]
- Hossain, S.; Umer, S.; Asari, V.; Rout, R.K. A unified framework of deep learning-based facial expression recognition system for diversified applications. Appl. Sci. 2021, 11, 9174. [Google Scholar] [CrossRef]
- Rout, R.K.; Choudhury, P.P.; Sahoo, S.; Ray, C. Partitioning 1-variable boolean functions for various classification of n-variable boolean functions. Int. J. Comput. Math. 2015, 92, 2066–2090. [Google Scholar] [CrossRef]
- Umer, S.; Mondal, R.; Pandey, H.M.; Rout, R.K. Deep features based convolutional neural network model for text and non-text region segmentation from document images. Appl. Soft Comput. 2021, 113, 107917. [Google Scholar] [CrossRef]
- Rout, R.K.; Hassan, S.S.; Sheikh, S.; Umer, S.; Sahoo, K.S.; Gandomi, A.H. Feature-extraction and analysis based on spatial distribution of amino acids for SARS-CoV-2 Protein sequences. Comput. Biol. Med. 2022, 141, 105024. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.S.; Rout, R.K.; Sahoo, K.S.; Jhanjhi, N.; Umer, S.; Tabbakh, T.A.; Almusaylim, Z.A. A Vicenary analysis of SARS-CoV-2 genomes. CMC-Comput. Mater. Contin. 2021, 3477–3493. [Google Scholar] [CrossRef]
- Sitaula, C.; Hossain, M.B. Attention-based VGG-16 model for COVID-19 chest X-ray image classification. Appl. Intell. 2021, 51, 2850–2863. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. of Images | TA (%) [7] | TA (%) [19] | TA (%) [28] | TA (%) Proposed |
|---|---|---|---|---|
| 100 | 79.50 | 79.85 | 79.98 | 91.50 |
| 200 | 80.20 | 80.35 | 80.41 | 91.70 |
| 300 | 80.50 | 80.60 | 80.65 | 91.90 |
| 500 | 80.70 | 80.80 | 80.81 | 92.30 |
| 700 | 80.90 | 80.83 | 80.85 | 92.50 |
| 900 | 80.76 | 80.89 | 80.94 | 92.60 |
| 1000 | 81.02 | 81.10 | 81.13 | 92.70 |
| 1200 | 81.18 | 81.25 | 81.28 | 92.90 |
| 1500 | 81.32 | 81.38 | 82.37 | 93.10 |
| 1800 | 81.44 | 85.35 | 86.56 | 93.40 |
| 2000 | 89.26 | 90.19 | 90.49 | 93.80 |
| 2250 | 91.13 | 91.39 | 91.74 | 93.90 |
| 2500 | 91.65 | 92.78 | 93.07 | 94.60 |
| 2800 | 93.91 | 93.93 | 94.27 | 96.90 |
| 3000 | 93.95 | 95.27 | 95.55 | 98.15 |
| 3250 | 96.58 | 96.41 | 96.39 | 98.85 |
| 3500 | 96.25 | 96.30 | 96.32 | 98.81 |
| 3800 | 96.36 | 96.36 | 96.42 | 98.95 |
| 4000 | 96.36 | 96.61 | 96.75 | 99.32 |
| 4250 | 96.86 | 97.15 | 97.27 | 99.86 |
| 4500 | 97.45 | 97.62 | 97.85 | 99.95 |
| No. of Images | TP (%) [7] | TP (%) [19] | TP (%) [28] | TP (%) Proposed |
|---|---|---|---|---|
| 100 | 77.90 | 78.15 | 78.24 | 89.37 |
| 200 | 78.39 | 78.51 | 78.57 | 89.56 |
| 300 | 78.63 | 78.73 | 78.76 | 89.85 |
| 500 | 78.83 | 78.84 | 78.86 | 90.15 |
| 700 | 78.86 | 78.89 | 78.92 | 90.29 |
| 900 | 78.92 | 79.02 | 79.06 | 90.39 |
| 1000 | 79.12 | 79.19 | 79.23 | 90.54 |
| 1200 | 79.27 | 79.33 | 79.83 | 90.73 |
| 1500 | 79.39 | 81.33 | 82.40 | 90.98 |
| 1800 | 83.27 | 85.63 | 86.37 | 91.32 |
| 2000 | 87.99 | 88.58 | 88.89 | 91.56 |
| 2250 | 89.16 | 89.84 | 90.15 | 91.95 |
| 2500 | 90.52 | 91.08 | 91.38 | 93.42 |
| 2800 | 91.64 | 92.29 | 92.59 | 95.15 |
| 3000 | 92.94 | 93.50 | 93.63 | 96.09 |
| 3250 | 94.06 | 94.01 | 94.00 | 96.42 |
| 3500 | 93.95 | 93.98 | 94.02 | 96.47 |
| 3800 | 94.01 | 94.13 | 94.23 | 96.72 |
| 4000 | 94.26 | 94.52 | 94.64 | 97.16 |
| 4250 | 94.78 | 95.01 | 95.18 | 97.47 |
| 4500 | 94.82 | 95.66 | 95.68 | 98.95 |
| No. of Images | TR (%) [7] | TR (%) [19] | TR (%) [28] | TR (%) Proposed |
|---|---|---|---|---|
| 100 | 76.78 | 77.07 | 77.18 | 88.23 |
| 200 | 77.36 | 77.49 | 77.55 | 88.42 |
| 300 | 77.63 | 77.72 | 77.76 | 88.66 |
| 500 | 77.82 | 77.88 | 77.88 | 89.00 |
| 700 | 77.93 | 77.91 | 77.93 | 89.17 |
| 900 | 77.89 | 78.00 | 78.05 | 89.26 |
| 1000 | 78.11 | 78.19 | 78.23 | 89.38 |
| 1200 | 78.27 | 78.33 | 78.59 | 89.58 |
| 1500 | 78.39 | 79.37 | 80.38 | 89.79 |
| 1800 | 80.34 | 83.40 | 84.35 | 90.11 |
| 2000 | 86.46 | 87.20 | 87.50 | 90.42 |
| 2250 | 87.94 | 88.40 | 88.73 | 90.66 |
| 2500 | 88.86 | 89.69 | 89.98 | 91.72 |
| 2800 | 90.52 | 90.84 | 91.15 | 93.68 |
| 3000 | 91.17 | 92.08 | 92.28 | 94.75 |
| 3250 | 93.00 | 92.89 | 92.87 | 95.25 |
| 3500 | 92.78 | 92.82 | 92.85 | 95.26 |
| 3800 | 92.86 | 92.92 | 93.00 | 95.45 |
| 4000 | 92.99 | 93.23 | 93.36 | 95.84 |
| 4250 | 93.48 | 93.74 | 93.88 | 96.26 |
| 4500 | 93.79 | 94.28 | 94.40 | 97.02 |
| No. of Images | TF (%) [7] | TF (%) [19] | TF (%) [28] | TF (%) Proposed |
|---|---|---|---|---|
| 100 | 77.34 | 77.61 | 77.70 | 88.79 |
| 200 | 77.87 | 78.00 | 78.06 | 88.99 |
| 300 | 78.13 | 78.22 | 78.26 | 89.25 |
| 500 | 78.32 | 78.36 | 78.37 | 89.57 |
| 700 | 78.39 | 78.40 | 78.42 | 89.73 |
| 900 | 78.40 | 78.51 | 78.55 | 89.82 |
| 1000 | 78.61 | 78.69 | 78.72 | 89.96 |
| 1200 | 78.76 | 78.83 | 79.20 | 90.15 |
| 1500 | 78.89 | 80.34 | 81.38 | 90.38 |
| 1800 | 81.78 | 84.50 | 85.35 | 90.71 |
| 2000 | 87.22 | 87.88 | 88.19 | 90.99 |
| 2250 | 88.55 | 89.12 | 89.43 | 91.30 |
| 2500 | 89.69 | 90.38 | 90.68 | 92.56 |
| 2800 | 91.08 | 91.56 | 91.87 | 94.41 |
| 3000 | 92.05 | 92.79 | 92.95 | 95.42 |
| 3250 | 93.53 | 93.45 | 93.43 | 95.83 |
| 3500 | 93.36 | 93.40 | 93.43 | 95.86 |
| 3800 | 93.43 | 93.53 | 93.61 | 96.08 |
| 4000 | 93.62 | 93.87 | 94.00 | 96.50 |
| 4250 | 94.13 | 94.37 | 94.52 | 96.86 |
| 4500 | 94.30 | 94.97 | 95.04 | 97.98 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rout, N.K.; Parida, N.; Rout, R.K.; Sahoo, K.S.; Jhanjhi, N.Z.; Masud, M.; AlZain, M.A. Analysis of Breath-Holding Capacity for Improving Efficiency of COPD Severity-Detection Using Deep Transfer Learning. Appl. Sci. 2023, 13, 507. https://doi.org/10.3390/app13010507
Rout NK, Parida N, Rout RK, Sahoo KS, Jhanjhi NZ, Masud M, AlZain MA. Analysis of Breath-Holding Capacity for Improving Efficiency of COPD Severity-Detection Using Deep Transfer Learning. Applied Sciences. 2023; 13(1):507. https://doi.org/10.3390/app13010507
Chicago/Turabian StyleRout, Narendra Kumar, Nirjharinee Parida, Ranjeet Kumar Rout, Kshira Sagar Sahoo, N. Z. Jhanjhi, Mehedi Masud, and Mohammed A. AlZain. 2023. "Analysis of Breath-Holding Capacity for Improving Efficiency of COPD Severity-Detection Using Deep Transfer Learning" Applied Sciences 13, no. 1: 507. https://doi.org/10.3390/app13010507