
Skeletal Muscle Symptoms in Students of Health Majors with Dependence on Mobile Devices: An Observational Descriptive Study

 , ,
, ,
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
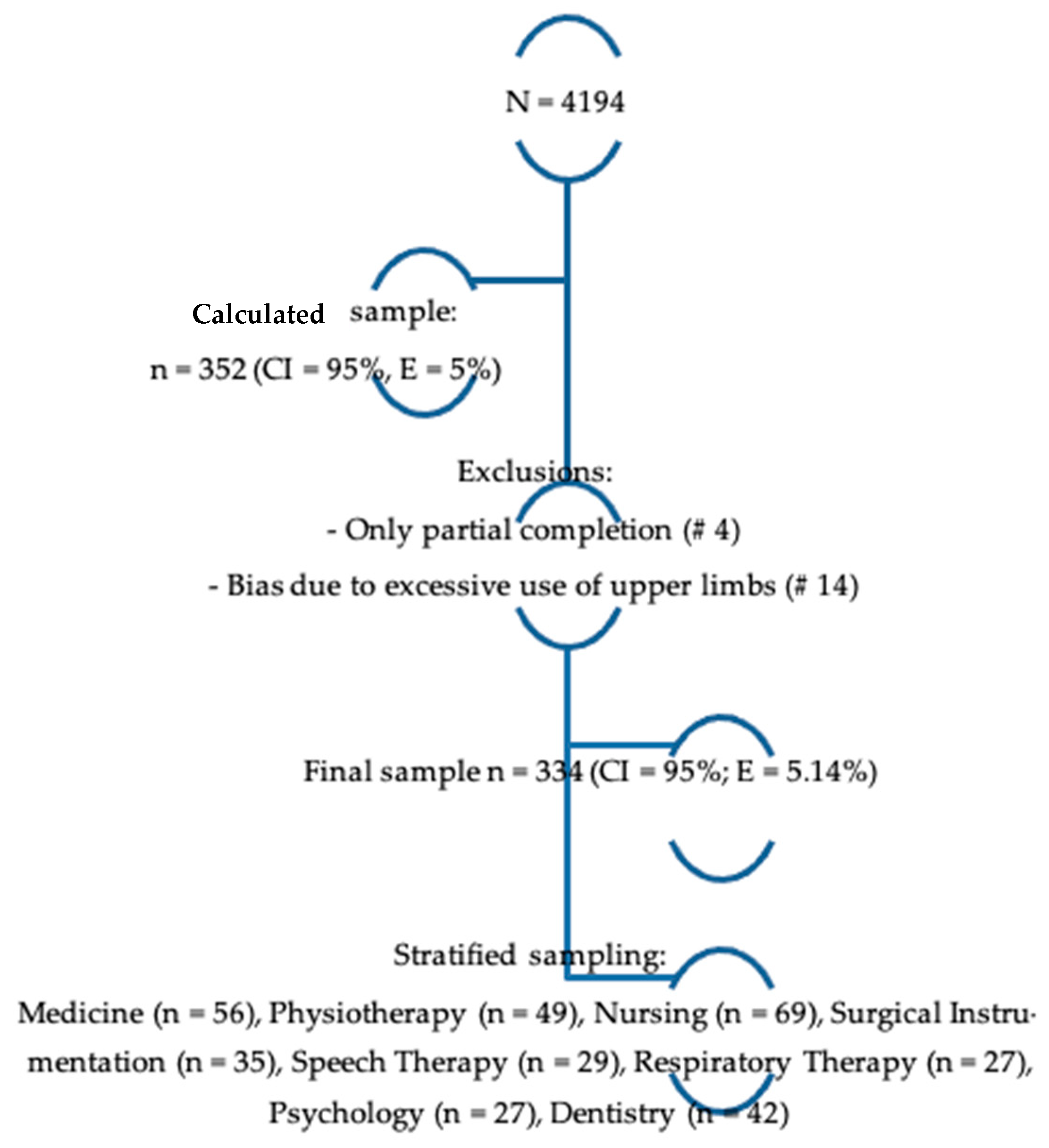
2.1. Type of Study, Design, Population, and Sample
2.2. Inclusion and Exclusion Criteria
2.3. Enrollment of Participants
2.4. Pilot
2.5. Test of Dependence on Mobile Devices and Sociodemographic Data
- (1)
- tolerance and abstinence, represented by items 11–22;
- (2)
- abuse and difficulty in controlling the impulse, corresponding to items 2, 4, 5, 6, 8, 12, and 20;
- (3)
- problems caused by excessive use, represented by items 1, 3, 7, 9, and 10.
2.6. Musculoskeletal Symptoms
2.7. Data Analysis
2.8. Ethical Aspects
3. Results
3.1. Pilot Test
3.2. Prevalence of MSS and Its Association with Sociodemographic and Academic Features
Nordic Questionnaire Results
3.3. Correlations between Musculoskeletal Symptoms, Nordic Questionnaire and Dependence on Mobile Divices
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministerio de Tecnologías de la Información y las Comunicaciones. Boletín Trimestral de las TIC. 2019. Available online: https://colombiatic.mintic.gov.co/679/articles-103108_archivo_pdf.pdf (accessed on 7 March 2022).
- Aguado, J.M.; Feijoó, C.; Martínez, I.J. La Comunicación Móvil; Gedisa: Barcelona, Spain, 2013. [Google Scholar]
- Muñoz Rivas, M.J.; Agustín, S. La adicción al teléfono móvil. Rev. Int. Psicol. Clínica Salud 2005, 13, 481–494. [Google Scholar]
- Ahmed, S.; Pokhrel, N.; Roy, S.; Samuel, A.J. Impact of nomophobia: A non-drug addiction among students of physiotherapy course using an online cross-sectional survey. Indian J. Psychiatry 2019, 61, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Cain, J.; Malcom, D.R. An assessment of pharmacy students’ psychological attachment to smartphones at two colleges of pharmacy. Am. J. Pharm. Educ. 2019, 83, 7136. [Google Scholar] [CrossRef]
- Jilisha, G.; Venkatachalam, J.; Menon, V.; Olickal, J. Nomophobia: A mixed-methods study on prevalence, associated factors, and perception among college students in Puducherry, India. Indian J. Psychol. Med. 2019, 41, 541–548. [Google Scholar] [CrossRef]
- Kwok, S.; Lee, P.; Lee, R. Smart Device Use and Perceived Physical and Psychosocial Outcomes among Hong Kong Adolescents. Int. J. Environ. Res. Public Health 2017, 14, 205. [Google Scholar] [CrossRef]
- Lui, D.P.Y.; Szeto, G.P.Y.; Jones, A.Y.M. The pattern of electronic game use and related bodily discomfort in Hong Kong primary school children. Comput. Educ. 2011, 57, 1665–1674. [Google Scholar] [CrossRef]
- Shan, Z.; Deng, G.; Li, J.; Li, Y.; Zhang, Y.; Zhao, Q. Correlational Analysis of neck/shoulder Pain and Low Back Pain with the Use of Digital Products, Physical Activity and Psychological Status among Adolescents in Shanghai. PLoS ONE 2013, 8, e78109. [Google Scholar] [CrossRef]
- Blair, B.; Gama, M.R.; Toberman, M. Prevalence and Risk Factors for Neck and Shoulder Musculoskeletal Symptoms in Users of Touch-Screen Tablet Computers. 2015. Available online: https://digitalscholarship.unlv.edu/thesesdissertations/2320/ (accessed on 7 March 2022).
- Giraldo-Jiménez, C.F.; Campo-Bermúdez, I.Y.; Muñoz-Hoyos, M.; Quintero-Puentes, I.; Botero-Carvajal, A.; Valderrama-Aguirre, A.; Millán-Estupiñan, J.C. Dependence on Mobile Devices among Health Science University Students: A cross-sectional analytical study. World Trans. Eng. Technol. Educ. 2022, 1, 45–51. [Google Scholar]
- Choliz, M. Mobile-phone addiction in adolescence: The Test of Mobile Phone Dependence (TMD). Prog. Health Sci. 2012, 2, 33–44. [Google Scholar]
- Gamero, K.; Flores, C.; Arias, W.L.; Ceballos, K.D.; Roman, A.; Marquina, E. Estandarización del Test de Dependencia al Celular para estudiantes universitarios de Arequipa. Rev. Fac. Psicol. 2016, 179–200. Available online: https://www.redalyc.org/articulo.oa?id=147149810011 (accessed on 7 March 2022).
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardized Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Dimate, A.E.; Rodríguez, D.C.; Rocha, A.I. Percepción de desórdenes musculoesqueléticos y aplicación del método RULA en diferentes sectores productivos: Una revisión sistemática de la literatura. Rev. Univ. Ind. Santander. Salud 2017, 49, 57–74. [Google Scholar] [CrossRef]
- Camp, B.; Mandivarapu, J.K.; Ramamurthy, N.; Wingo, J.; Bourgeois, A.G.; Cao, X.; Sunderraman, R. A new cross-platform architecture for epi-info software suite. BMC Bioinform. 2018, 19, 359. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Salud, R.C. Resolución Número 8430 de 1993: Por la Cual se Establecen las Normas Científicas, Técnicas y Administrativas para la Investigación en Salud. 1993; pp. 1–19. Available online: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/RESOLUCION-8430-DE-1993.PDF (accessed on 7 March 2022).
- World Medical Association. World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berolo, S.; Wells, R.P.; Amick, B.C., 3rd. Musculoskeletal symptoms among mobile hand-held device users and their relationship to device use: A preliminary study in a Canadian university population. Appl. Ergon. 2011, 42, 371–378. [Google Scholar] [CrossRef]
- Kalirathinam, D.; Manoharlal, M.A.; Mei, C.; Ling, C.K.; Sheng, T.W.Y.; Jerome, A.; Rao, M.U. Association between the usage of Smartphone as the risk factor for the prevalence of upper extremity and neck symptoms among University students: A cross-sectional survey based study. Res. J. Pharm. Technol 2017, 10, 1184–1190. [Google Scholar] [CrossRef]
- Barrantes, M.F.; López, A.M. Desórdenes del sistema musculoesquelético por trauma acumulativo en estudiantes universitarios de computación e informática. Rev. Cienc. Tecnol. 2010, 26, 1–18. [Google Scholar]
- Lee, S.-P.; Hsu, Y.-T.; Bair, B.; Toberman, M.; Chien, L.-C. Gender and posture are significant risk factors to musculoskeletal symptoms during touchscreen tablet computer use. J. Phys. Ther. Sci. 2018, 30, 855–861. [Google Scholar] [CrossRef]
- Almhdawi, K.A.; Mathiowetz, V.; Al-Hourani, Z.; Khader, Y.; Kanaan, S.F.; Alhasan, M. Musculoskeletal pain symptoms among allied health professions’ students: Prevalence rates and associated factors. J. Back. Musculoskelet. Rehabil. 2017, 30, 1291–1301. [Google Scholar] [CrossRef]
- Regiani Bueno, G.; Garcia, L.F.; Marques Gomes Bertolini, S.M.; Rodrigues Lucena, T.F. The Head Down Generation: Musculoskeletal Symptoms and the Use of Smartphones among Young University Students. Telemed. J. e-Health 2019, 25, 1049–1056. [Google Scholar] [CrossRef]
- Billieux, J.; Gay, P.; Rochat, L.; Van der Linden, M. The role of urgency and its underlying psychological mechanisms in problematic behaviours. Behav. Res. Ther. 2010, 48, 1085–1096. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.L.; Wang, H.Z.; Gaskin, J.; Wang, L.H. The role of stress and motivation in problematic smartphone use among college students. Comput. Hum. Behav. 2015, 53, 181–188. [Google Scholar] [CrossRef]
- Hagen, A.L. The relationship between exercise dependence symptoms and perfectionism. Am. J. Health Stud. 2003, 18, 133–137. [Google Scholar]
- Bragazzi, N.L.; Re, T.S.; Zerbetto, R. The relationship between nomophobia and maladaptive coping styles in a sample of Italian young adults: Insights and implications from a cross-sectional study. J. Med. Internet Res. 2019, 6, e13154. [Google Scholar] [CrossRef] [PubMed]
- Guterres, J.L.; Schmitt, F.S.; Oliveira, L.; Simón, C.; Lopes, A.R. Principais Queixas Relacionadas ao Uso Excessivo de Dispositivos Móveis. Physics 2017, 11, 39–45. [Google Scholar]
- Gomes-Neto, M.; Sampaio, G.S.; Santos, P.S. Frequência e fatores associados a dores musculoesqueléticas em Estudantes Universitários. Rev. Pesqui. Fisioter. 2016, 6, 26–34. [Google Scholar] [CrossRef]
- Martins, A.C.; Felli, V.E.A. Sintomas músculo-esqueléticos em graduandos de enfermagem. Enferm. Foco 2013, 4, 58–62. [Google Scholar] [CrossRef]
- Vandenberghe, L.B.C. Terapia de grupo embasada em psicoterapia analítica funcional como abordagem terapêutica para dor crônica: Possibilidades e perspectivas. Psicol. Teor. Prat. 2005, 7, 137–215. [Google Scholar]
- Haeffner, R.; Sarquis, L.M.M.; Haas, G.F.S.; Heck, R.M.; Jardim, V.M.R. Prevalência de lombalgia e fatores associados em trabalhadores de uma empresa agropecuária do sul do Brasil. Rev. Bras. Med. Trab. 2015, 13, 35–42. [Google Scholar]
- Yadav, M.S.; Kodi, S.M.; Deol, R. Impact of mobile phone dependence on behavior and academic performance of adolescents in selected schools of Uttarakhand, India. J. Educ. Health Promot. 2021, 10, 327. [Google Scholar] [CrossRef]
- Gangadharan, N.; Borle, A.L.; Basu, S. Mobile Phone Addiction as an Emerging Behavioral form of Addiction among Adolescents in India. Cureus 2022, 14, e23798. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Wu, X.; Zhen, R.; Zhou, X. Post-Traumatic Stress Disorder, Mobile Phone Dependence, and Academic Boredom in Adolescents During the COVID-19 Pandemic. Front. Psychol. 2021, 12, 724732. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Neck | Back (n) | Shoulder (n) | Wrist (n) | |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | ||
| Age | 18–19 | 60 (31.9) | 50 (30.3) | 34 (29.6) | 34 (24.3) |
| 20–21 | 54 (28.7) | 46 (27.9) | 32 (27.8) | 39 (27.9) | |
| 22–23 | 39 (20.7) | 40 (24.2) | 26 (22.6) | 37 (26.4) | |
| 24–25 | 15 (8.0) | 13 (7.9) | 12 (10.4) | 14 (10.0) | |
| 26–27 | 9 (4.8) | 7 (4.2) | 3 (2.6) | 7 (5.0) | |
| 28–29 | 7 (3.7) | 6 (3.6) | 6 (5.2) | 7 (5.0) | |
| ≥30 | 4 (2.1) | 3 (1.8) | 2 (1.7) | 2 (1.4) | |
| Total | 188 (100) | 165 (100) | 115 (100) | 140 (100) | |
| CI95 | 19.8–20.7 | 19.9–2.4 | 19.3–20.1 | 19.0–19.9 | |
| X2 | 35.1986 | 23.8927 | 76.7155 | 71.6564 | |
| P | 0.0191 | 0.2471 | 0.5833 | 0.7359 | |
| Sex | Male | 32 (22.2) | 30 (23.4) | 26 (30.2) | 27 (23.9) |
| Female | 112 (77.8) | 98 (76.6) | 60 (69.8) | 86 (76.1) | |
| Total | 144 (100) | 128 (100) | 86 (100) | 113 (100) | |
| X2 | 1.0439 | 0.1917 | 2.9574 | 2.6688 | |
| P | 0.306 | 0.661 | 0.398 | 0.614 | |
| Program | Nursing | 24 (12.8) | 21 (12.7) | 14 (12.4) | 14 (9.9) |
| Physiotherapy | 37 (19.7) | 36 (21.8) | 17 (15.0) | 32 (22.5) | |
| Phonoaudiology | 21 (11.2) | 21 (12.7) | 12 (10.6) | 17 (12.0) | |
| Instrumentation | 20 (10.6) | 17 (10.3) | 12 (10.6) | 17 (12.0) | |
| Medicine | 31 (16.5) | 27 (16.4) | 23 (20.4) | 22 (15.5) | |
| Dentistry | 19 (10.1) | 17 (10.3) | 9 (8.0) | 14 (9.9) | |
| Psychology | 18 (9.6) | 13 (7.9) | 14 (12.4) | 12 (8.5) | |
| Resp. Therapy | 18 (9.6) | 13 (7.9) | 12 (10.6) | 14 (9.9) | |
| Total | 188 (100) | 165 (100) | 113 (100) | 142 (100) | |
| X2 | 27.871 | 28.843 | 22.079 | 49.629 | |
| P | 0.0002 | 0.0002 | 0.395 | 0.007 | |
| Year of study | 1 | 41 (28.5) | 29 (22.7) | 21 (24.4) | 29 (25.7) |
| 2 | 41 (28.5) | 40 (31.3) | 23 (26.7) | 32 (28.3) | |
| 3 | 21 (14.6) | 24 (18.8) | 15 (17.4) | 17 (15.0) | |
| 4 | 26 (18.1) | 23 (18.0) | 21 (24.4) | 25 (22.1) | |
| 5 | 15 (10.4) | 12 (9.4) | 6 (7.0) | 10 (8.8) | |
| Total | 144 (100) | 128 (100) | 86 (100) | 113 (100) | |
| X2 | 12.51 | 4.789 | 11.21 | 20.849 | |
| P | 0.013 | 0.309 | 0.511 | 0.184 | |
| Variable | Neck | Shoulder | Back | Elbow | Wrist |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | |
| How long have you had the discomfort? | |||||
| No time recorded | 1 (1) | 0 (0) | 2 (2) | 0 (0) | 2 (2) |
| <1 month | 73 (51) | 39 (45) | 62 (48) | 32 (47) | 56 (50) |
| 2–3 months | 32 (22) | 17 (20) | 27 (21) | 14 (21) | 22 (19) |
| 4–6 months | 19 (13) | 13 (15) | 19 (15) | 11 (16) | 16 (14) |
| 7–9 months | 4 (3) | 4 (5) | 3 (2) | 2 (3) | 2 (2) |
| 10–12 months | 15 (10) | 13 (15) | 15 (12) | 9 (13) | 15 (13) |
| X2 | 117.12 | 71.376 | 87.421 | 50.989 | 89.296 |
| P | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Have you had to change places because of the inconvenience? | |||||
| Yes | 107 (74) | 46 (53) | 94 (73) | 36 (53) | 76 (67) |
| No | 37 (26) | 40 (47) | 34 (27) | 32 (47) | 37 (33) |
| X2 | 132.14 | 115.191 | 141.916 | 126.353 | 131.844 |
| P | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Has the discomfort prevented you from performing normal activities during the last 12 months? | |||||
| Yes | 32 (22) | 16 (19) | 28 (22) | 7 (10) | 21 (19) |
| No | 112 (78) | 70 (81) | 100 (78) | 61 (90) | 92 (81) |
| X2 | 26.535 | 52.761 | 29.591 | 26.636 | 32.955 |
| P | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Have you received treatment for the discomfort in the last 12 months? | |||||
| Yes | 20 (14) | 11 (13) | 33 (26) | 4 (6) | 14 (12) |
| No | 124 (86) | 75 (87) | 95 (74) | 64 (94) | 99 (88) |
| X2 | 15.712 | 25.541 | 35.686 | 13.894 | 22.662 |
| P | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Have you had discomfort in the last 7 days? | |||||
| Yes | 85 (59) | 42 (49) | 62 (48) | 16 (24) | 46 (41) |
| No | 59 (41) | 44 (51) | 66 (52) | 52 (76) | 67 (59) |
| X2 | 93.40 | 95.539 | 74.066 | 53.225 | 74.566 |
| P | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| What is the intensity of the discomfort? | |||||
| No discomfort | 2 (1) | 2 (2) | 4 (3) | 1 (1) | 4 (4) |
| Mild | 76 (53) | 51 (59) | 54 (42) | 55 (81) | 66 (58) |
| Moderate | 52 (36) | 20 (23) | 50 (39) | 10 (15) | 32 (28) |
| Strong | 12 (8) | 12 (14) | 17 (13) | 2 (3) | 9 (8) |
| Very strong | 2 (1) | 1 (1) | 3 (2) | 0 (0) | 2 (2) |
| X2 | 228.093 | 248.520 | 228.573 | 256.817 | 248.821 |
| P | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| What do you attribute the discomfort to? | |||||
| Does not know/Did not answer | 37 (26) | 40 (47) | 59 (46) | 39 (57) | 48 (42) |
| Pulled muscle | 1 (1) | 3 (3) | 0 (0) | 3 (4) | 2 (2) |
| Poor posture | 73 (51) | 24 (28) | 47 (37) | 13 (19) | 18 (16) |
| Stress | 23 (16) | 9 (10) | 13 (10) | 1 (1) | 3 (3) |
| Repetitive movement | 1 (1) | 4 (5) | 1 (1) | 4 (4) | 8 (7) |
| Cell phone | 9 (6) | 3 (3) | 3 (2) | 6 (9) | 30 (27) |
| Illness/Injury | 0 (0) | 3 (3) | 5 (4) | 2 (3) | 4 (4) |
| X2 | 132.27 | 145.622 | 86.140 | 142.428 | 127.413 |
| P | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Total | 144 (100) | 86 (100) | 128 (100) | 68 (100) | 113 (100) |
| Region | Spearman’s Rho | |
|---|---|---|
| Neck | Correlation coefficient | 0.171 |
| Sig. (bilateral) | 0.007 | |
| n | 248 | |
| Shoulder | Correlation coefficient | 0.142 |
| Sig. (bilateral) | 0.025 | |
| n | 248 | |
| Back | Correlation coefficient | 0.274 |
| Sig. (bilateral) | 0.000 | |
| n | 248 | |
| Elbow | Correlation coefficient | 0.072 |
| Sig. (bilateral) | 0.259 | |
| n | 248 | |
| Wrist | Correlation coefficient | 0.200 |
| Sig. (bilateral) | 0.002 | |
| n | 248 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giraldo-Jiménez, C.F.; Jembuel-Giraldo, A.M.; Galeano-Zapata, J.C.; Quintana-Caro, A.M.; Botero-Carvajal, A.; Valderrama-Aguirre, A.; Millán-Estupiñan, J.C. Skeletal Muscle Symptoms in Students of Health Majors with Dependence on Mobile Devices: An Observational Descriptive Study. Appl. Sci. 2022, 12, 8736. https://doi.org/10.3390/app12178736
Giraldo-Jiménez CF, Jembuel-Giraldo AM, Galeano-Zapata JC, Quintana-Caro AM, Botero-Carvajal A, Valderrama-Aguirre A, Millán-Estupiñan JC. Skeletal Muscle Symptoms in Students of Health Majors with Dependence on Mobile Devices: An Observational Descriptive Study. Applied Sciences. 2022; 12(17):8736. https://doi.org/10.3390/app12178736
Chicago/Turabian StyleGiraldo-Jiménez, Claudia F., Ana M. Jembuel-Giraldo, Juan C. Galeano-Zapata, Arleidis M. Quintana-Caro, Alejandro Botero-Carvajal, Augusto Valderrama-Aguirre, and Juan C. Millán-Estupiñan. 2022. "Skeletal Muscle Symptoms in Students of Health Majors with Dependence on Mobile Devices: An Observational Descriptive Study" Applied Sciences 12, no. 17: 8736. https://doi.org/10.3390/app12178736