2.1. Signals Selection
For having a large spectrum of PPG signal morphology, multiple databases should be investigated. The topic addressed by the presented study is to funnel various waveforms into a few main categories sorted by clearly defined criteria. In this way, specific key metrics correlated to certain population group types can be identified. The first step into this investigation was to visualize signals from available free-access databases. We found recordings with different health metrics which are summarized in
Table 1. The primary criterion was for datasets to contain PPG signals and associated BP information. Three recording databases have been used to highlight morphology key metrics, but only two where used in the final algorithm development procedure. In total, 359 PPG recordings with corresponding BP class have been used as described:
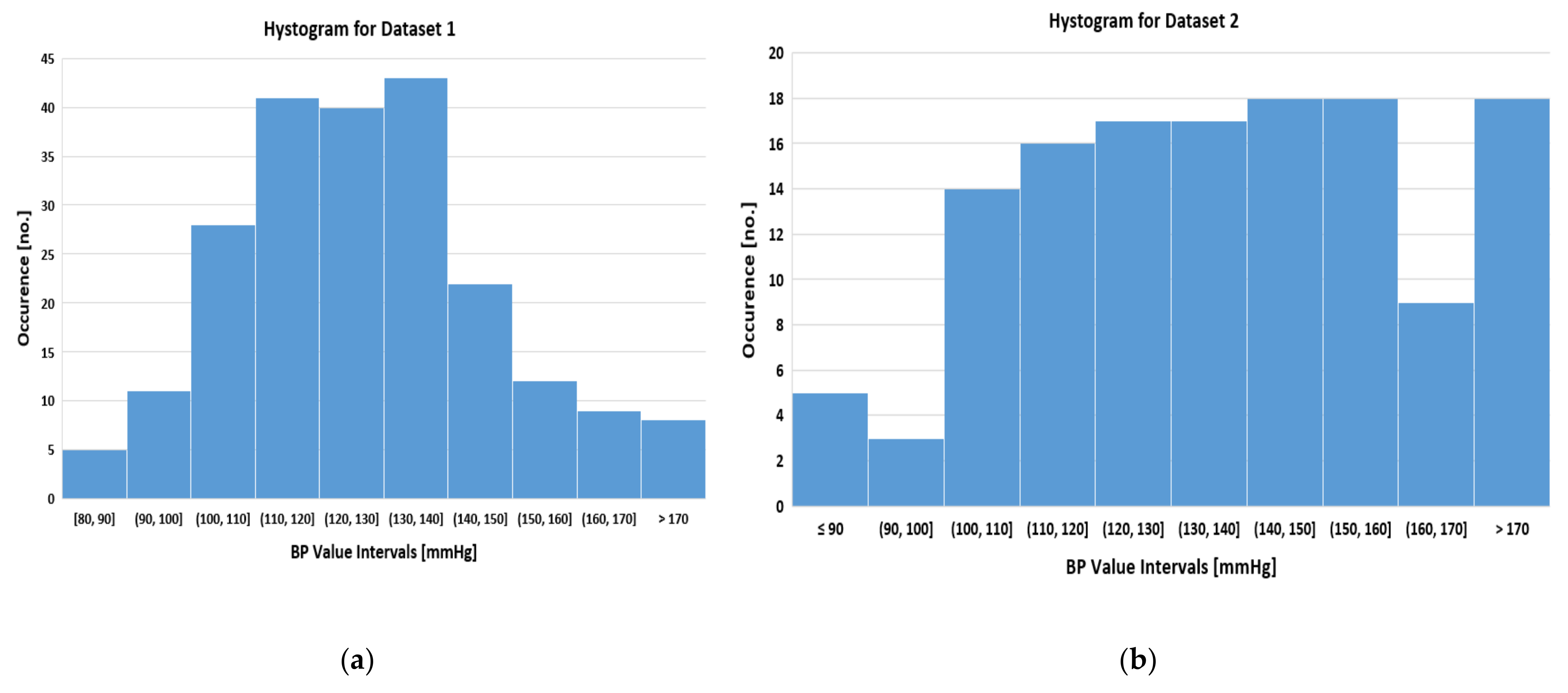
Dataset 1 contains a total of 219 recordings from volunteers where the BP distribution is represented in
Figure 2a. It is observable that distribution follows a Gaussian trend where normotensive and hypertensive groups are balanced. The protocol of signal acquisition uses a sampling frequency of 1 kHz where 3 clusters of 3 periods were electronically saved. Blood pressure recordings were carried out by oscillometric methods while the patients were sitting in a relaxed position.
Dataset 2 contains a total of 12,000 recordings but by an iterative visual inspection it was deduced that clusters of consecutive 10–30 recordings belonged to the same patients. The protocol of signal acquisition uses a sampling frequency of 125 Hz where the periods vary from 5 to 20 cardiac cycles. Associated BP information was taken by an invasive method using the catheter technique. The monitored patients were in an Intensive Care Unit or in surgery procedure. Therefore, a manual dataset with the same label was created with signals coming from each individual patient. With this procedure, a total number of 140 recordings were electronically sorted where the secondary criterion was to obtain a uniform distribution among BP classes as shown in
Figure 2b.
Dataset 3 contains a total number of 42 patients but since the BP information is missing it was not used in the final step of the algorithm development. Its available information was used only to help the presented investigation in the key metrics extraction procedure.
The last dataset which does not have an allocated label was used only for visualizing the PPG morphology under the entire time frame of the surgery procedure. This dataset helps to find the relevant key metrics for the next steps which will be presented.
It is important to note that signals come from motionless context since the patients were being monitored in an Intensive Care Unit or in related stationary cases. However, this topic does not represent a blocking point in healthcare algorithm development. During 24 h a person can certainly experience time frames where motionless events occur, such as sleeping (around 8 h of stationary state), sitting in front of the desk, reading, waiting in front of queue, and other related social activities. Therefore, these scenarios made a major topic for developing an algorithm specialized for PPG signal acquisition. In the presented research the focus is on signal analysis with the assumption that the provided recordings come from stationary events.
2.2. Signals Classification
The next step after database selection was to find relevant signal morphology characteristics among different patient groups as was described earlier. The main observations during recordings evaluation in different scenarios, while also having in mind the findings reported in the medical literature [
18,
19,
20,
21,
22] were:
Anacrotic limb features are found in many cases in the old patients group or for hypertensive ones. They represent a change in signal slope, PPG, or BP, during the systolic rising phase.
Dicrotic wave location moves away with respect to SYS points when vasodilators were administrated during the beginning of anesthesia. The vasoconstrictor drugs give the opposite effect by moving the dicrotic wave toward SYS peak. Therefore, this fiducial point can represent the state of vasomotor activity.
Dicrotic wave is mostly absent in the children group, under 10 years old, and very prominent in young groups with ages between 20 and 30. After these limits, in older populations it fades again.
Another observation, but related to signal acquisition, is the different protocols used for PPG recordings. One important highlight used sampling frequency but also the cutoff frequency for signal filtering. This variation is translated into different cardiovascular details which will be discussed in the Results and Limitations sections. Those differences among databases did not represent a blocking point for the current step but could influence the performance of the final algorithm.
After the signal characteristics arise, we needed a tool to translate it into a numerical value. A good domain to highlight signal morphology was first derivative (FD) since it represents the evolution of the signal gradient over time. This domain has the advantage to show a more detailed level of the investigated waveforms which are not visible by the eye. Therefore, after the initial pre-evaluation steps, we define four major classes among patients without cardiovascular disease which modulated PPG or BP signals such as pulsus bisferience. The defined classes take the dicrotic wave and anacrotic feature as the selection criteria:
Anacrotic type (A)—This class highlights the pre-systolic phase where signal slope is subject to a change [
18,
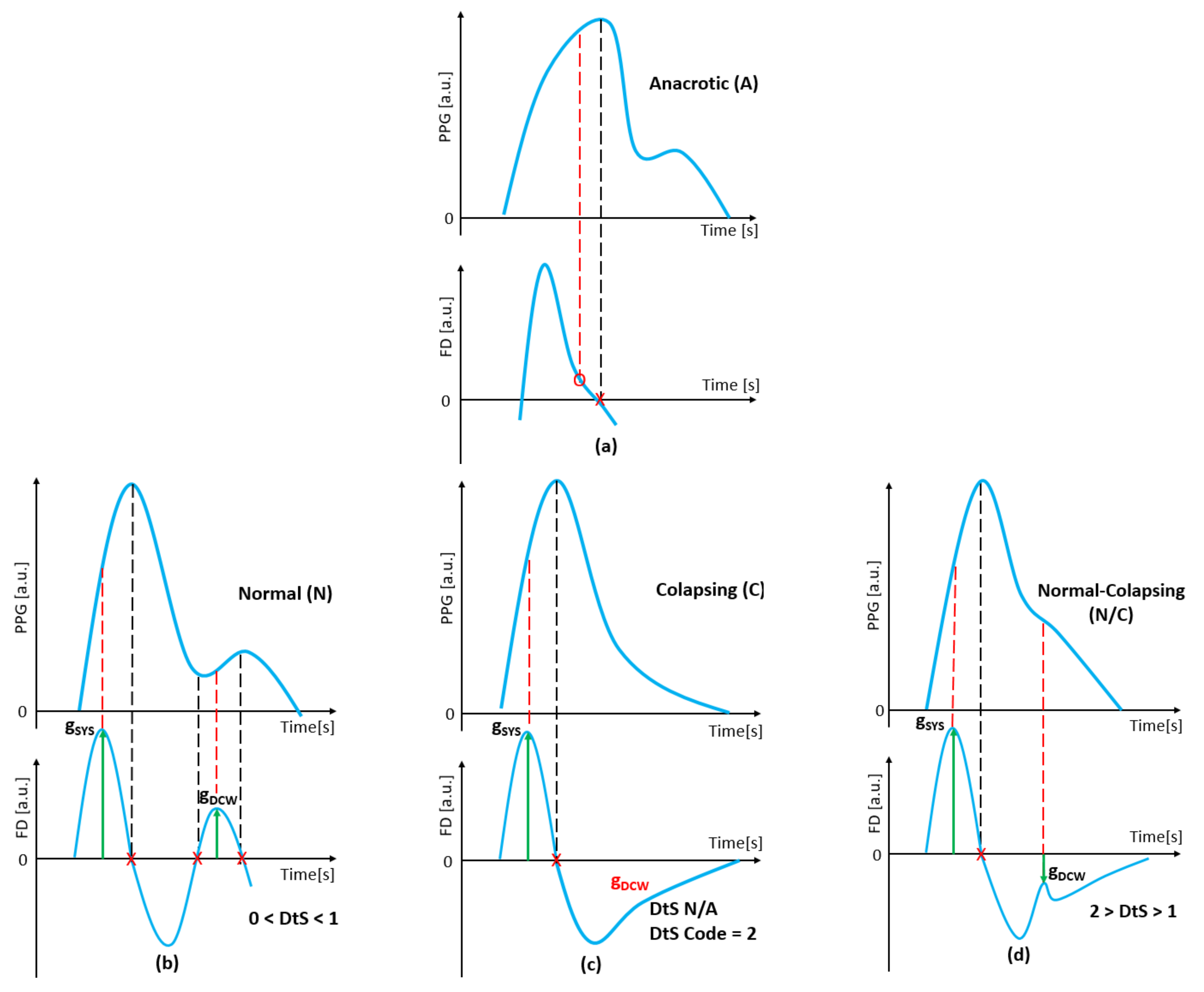
19]. This feature is translated into FD domain as a visible peak before SYS maximum point event as it is shown in
Figure 3a.
Normal type (N)—This class highlights the post-systolic phase where DCW generates a visible peak in the original analyzed signal. In FD domain, the associated gradient of the dicrotic wave beginning phase is greater than zero (or positive), building a peak as shown in
Figure 3b.
Collapsing type (C)—Also aims at the post-systolic phase where DCW is entirely absent in the analyzed signal. In FD domain its gradient does not appear as the result of a wave missing. After the SYS event, the returning gradient slowly rises towards zero axis, without generating a peak, until the next cardiac cycle begins [
20] as shown in
Figure 3c.
Normal Collapsing (NC) type—This class is a characterization between the previous two. DCW is barely visible in the investigated signal, therefore, it generates a gradient peak into FD domain but negative in absolute value as shown in
Figure 3d.
Note that multiple peaks after SYS event can occur due to different elastic characteristic of the arterial network. These peaks can be present even if the signal filtering is applied and are therefore not given by motion or acquisition artifacts. In our classification context, the dicrotic wave presence is flagged as the strongest gradient in FD domain in the defined search window.
Using this major classification, signals are characterized from a qualitative mean with an intuitive nomenclature. In order to cover a quantitative topic, a numerical term should be associated to gradients since it can range from any positive to negative value. As we anchor classification to the dicrotic wave gradient it needs to be related to another important key metric during the current cardiac cycle. Thus, a numerical parameter was defined, labelled as DtS which stands for Dicrotic to Systolic Ratio. The computed parameter translates into numbers of the human’s sense of the observed PPG morphologies during signal evaluation step. In this way, it is characterized how strong the dicrotic wave is with respect to the systolic one according to the presented classifications from
Figure 3. The formula for defining this morphological parameter is:
where g
SYS represents the value of systolic gradient extracted from the first derivative and g
DCW is the value of the dicrotic gradient part. While the SYS gradient is always positive, the other ones take both possibilities. This is why the DtS parameters compute the distance between the gradients of the respective fiducial points with respect to the positive ones. With this rule, the translation of defined classes was translated via DtS parameters as presented in
Table 2.
Note that DtS is computed per individual cardiac cycle. Thus, in N type signal where gDCW is defined to be positive, the above parameter will be lower than 1 value. While in NC type were DCW gradient is negative, the parameter will be greater than 1. In other words, DtS highlights how close the dictoric wave gradient is to the systolic one in the FD domain. For C type where dicrotic is entirely absent, DtS cannot be computed but is marked with value 2. This convention comes from the fact that a hypothetically maximum negative value taken by a second wave cannot exceed absolute value of the current systolic gradient. As we described earlier, a strong FD value represents a strong visible point back to the analyzed signal.
If a signal recording is evaluated during multiple periods, the above-described parameters is computed as a mean. With those classifications—nomenclature of waveform morphology by pre-systolic and post-systolic evaluation criteria—we built a test labelled ANC Test™ (
Anacrotic,
Normal,
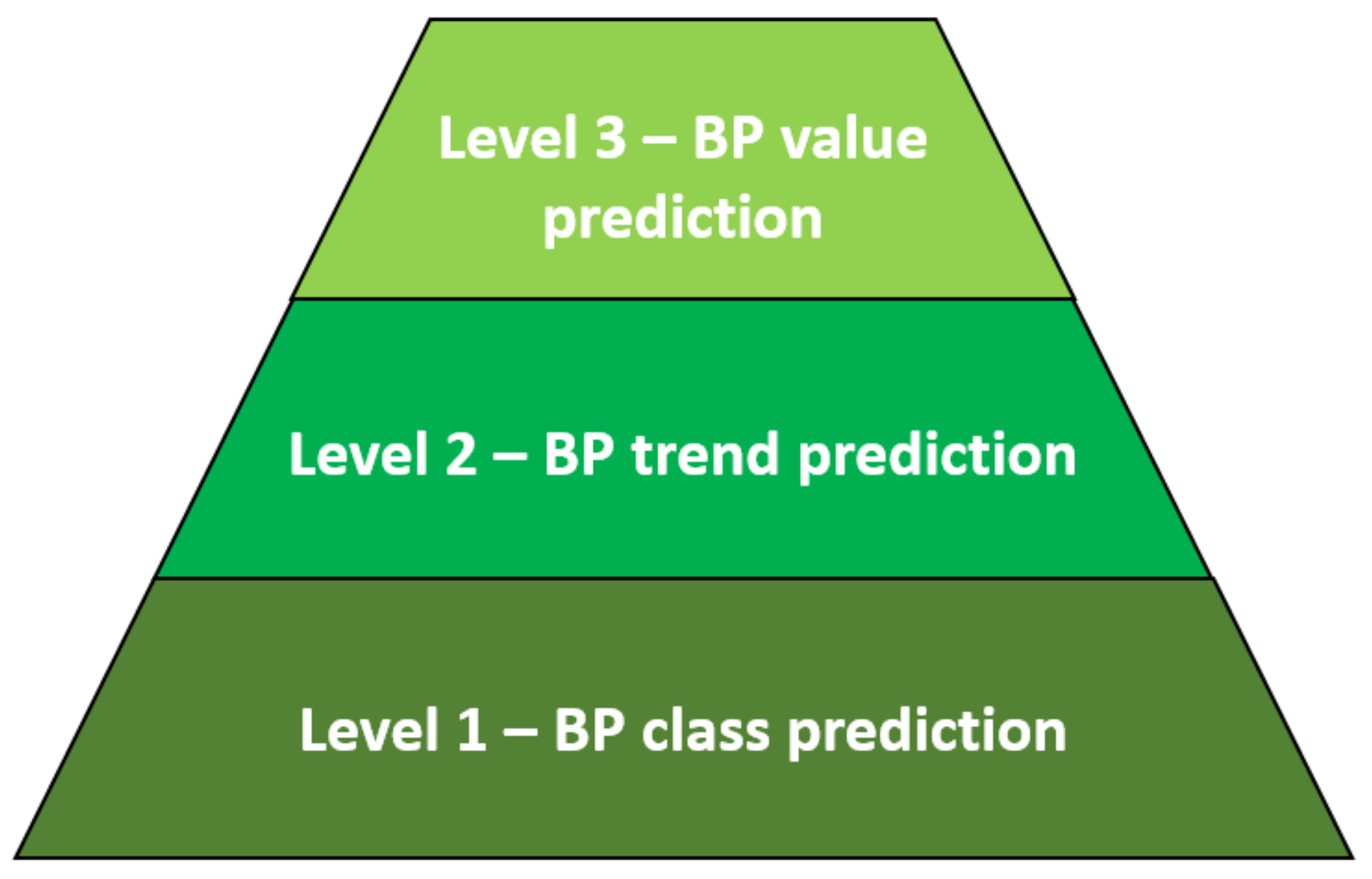
Collapsing) which stands for Level 1 class prediction described back in
Figure 1. Hence, the numerical outputs of this designed test, which are intended for multiple cardiac cycles evaluation, are:
Anacrotic occurrence if at least two cardiac cycles are evaluated within the pre-systolic phase. For a single-period analysis, the algorithm just marks if the Anacrotic feature is present or not.
Normal, Normal-Collapsing and Collapsing occurrence evaluated in the same manner as above but within the post-systolic phase.
DtS ratio evaluation for every individual analyzed cardiac cycle. In the collapsing case the ratio is marked with code 2 since mathematically it cannot be computed.
All the occurrence computations are done automatically since one part of the intended algorithm classified recordings by the defined features. In multiple periods of evaluation mode, the occurrence rate for the presented types can takes any value between 0% and 100%. But in the opposite case where just a single cardiac cycle is analyzed the occurrence rate can take only 0% or 100% value. It is a low probability that a patient’s key metrics will be investigated just based on one cardiac cycle, therefore the first mode will be frequently used.
2.3. ANC Test Pre-Evaluation
To evaluate what correspondence between defined feature and population group type arises, the built test was run in the following cases: Dataset 1 and Dataset 2 to check the results against BP groups and Dataset 1 and Dataset 3 to check against age groups. The splitting granularity of both groups was chosen to be 10 units. The overall results are presented into
Table 3 and
Table 4 for first group’s type and into
Table 5 and
Table 6 for the second one. The test was run in a multiple cardiac cycles evaluation mode where a patient takes the predominant ANC type where the occurrence threshold rate was chosen at 50%. For example, if within a recording length for A type the occurrence was around 60%, the patient would have the respective label. For the post-systolic evaluation, the occurrence sum of N, NC, and C cannot exceed 100%. Therefore, the predominant one was taken as the final label.
It can be observed from
Table 3 and
Table 4 that A type occurs more frequently in prehyper and hypertensive class (130+ mmHg) with 75.36% probability in Dataset 1 and with 53.18% in Dataset 2. For N type which indicates a visible DCW in analyzed signal according to our classification, in prehypertensive and hypertensive class it occurs with a probability of 39.63% in Dataset 1 and 37.10% in Dataset 2. The class with a low presence in both datasets is C type which does not have a visible trend against BP sorting criteria. The class with a high occurrence rate is NC type which represents a barely visible DCW in the analyzed signal. It appears to be more frequent in Dataset 1 than in Dataset 2 for the same BP ranges. At this point, A and N types represent promising key features to distinguish between normotensive patients and hypertensive ones.
By evaluating the ANC type against age sorting criteria, different trends can be observed especially for C type which lacks against BP assessment. Taking both
Table 5 and
Table 6 into consideration for a large age spectrum, it can be observed that this type occurs frequently in children under 10 years old and again in people over 40. Thus, C type does not have a linear trend by the current sorting criteria. For A type, the occurrence happens in an older population with a slightly positive trend. Again, NC type is the predominant one among age spectrums in both datasets. The other type, N, appears only in young persons as it is highlighted in
Table 5 within the 20–29 age group.
With these two sorting criteria, BP and age group, the summary of ANC type allocation among the population is presented. The scope is to avoid biases, like the belief that N type occurs only in a young population. However, as it was shown, this parameter is not dependent exclusively on the age since it is also distributed among various systolic blood pressure values.
2.4. ANC Test Enchanted by Machine Learning
The final step to predict the systolic blood pressure category based on the defined signal morphology classification is to enchant the ANC Test results with a powerful detection tool. In this way multiple machine learning (ML) architectures have been evaluated using classification learner tools from Matlab™ Software. The tools contain the following models: Decision Trees, Logistic Regression, Discriminant Analysis, Naive Bayes, Support Vector Machine, Nearest Neighbor Classifiers, and Ensemble Classifier. We tested every model to obtain the best metrics. Since the aim of the present study was to detect systolic hypertensive persons, to fulfil Level 1—BP prediction, two categories were defined:
Therefore, in Class I are clustered systolic hypotensive and normotensive datasets while in Class II are clustered prehypertensive and hypertension ones where the threshold value is 130 mmHg. Multiple clustering for each known BP category was avoided due to the low number of datasets and for uneven distribution as it was shown in the histogram back in
Figure 2.
The input parameters for ML models are represented by the results of the ANC Test™ where the occurrence rate for each type and DtS parameter were computed automatically on PPG signal. The output is represented by the previous defined BP binary clusters. Therefore, given an input PPG waveform, the developed algorithm extracted ANC features and then fed them into the ML model. The last step should give the result if the given PPG signal comes from a normotensive or hypertensive patient.
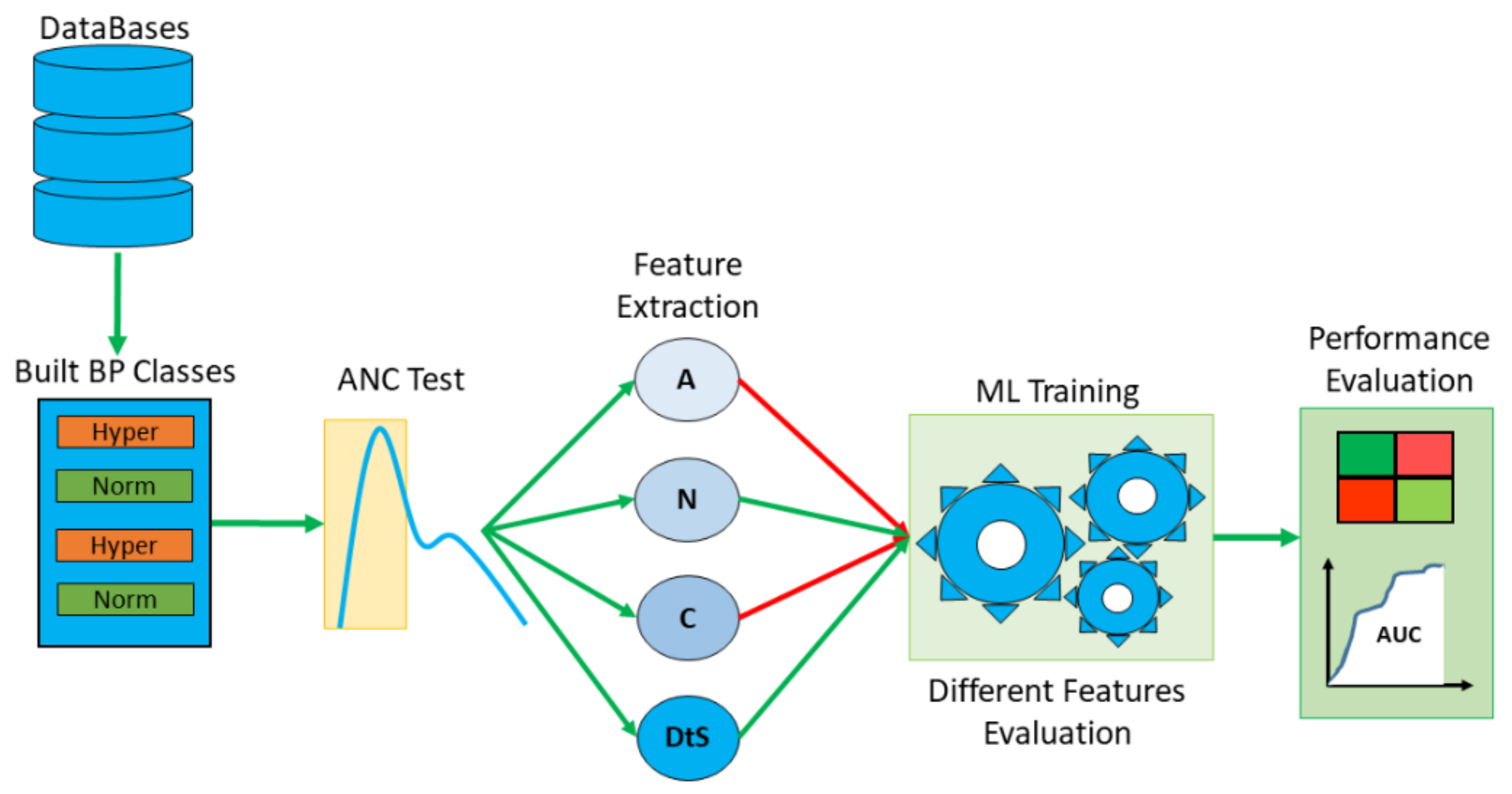
Since in pre-evaluation section ANC types have a different distribution among systolic BP groups, the last human intervention is to set which feature combination will give the best predicted results. The assessment was done in two ways: checking individual feature standalone against defined BP clusters and checking the combination of features. These two assessments were done separately for Dataset 1 and Dataset 2 but also in the case by merging the two. With this approach, the influence of the recordings distribution was evaluated: Gaussian against uniform. The overview of the entire process is described in the below
Figure 4:


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}