
Plywood Jig—A New Technique for Root Canal Curvature Measurement


 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
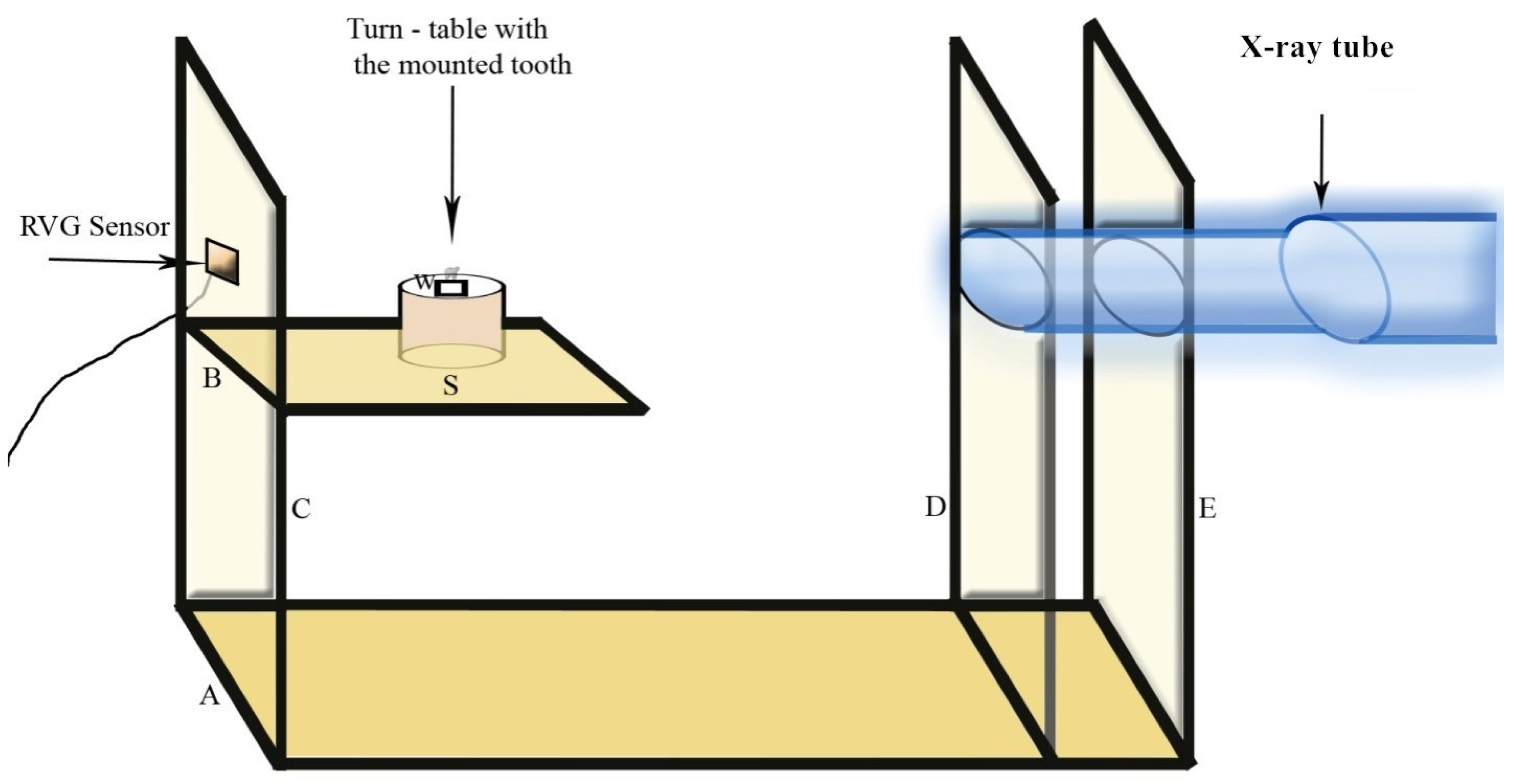
2.1. Construction of Plywoog Jig
2.2. Procedure
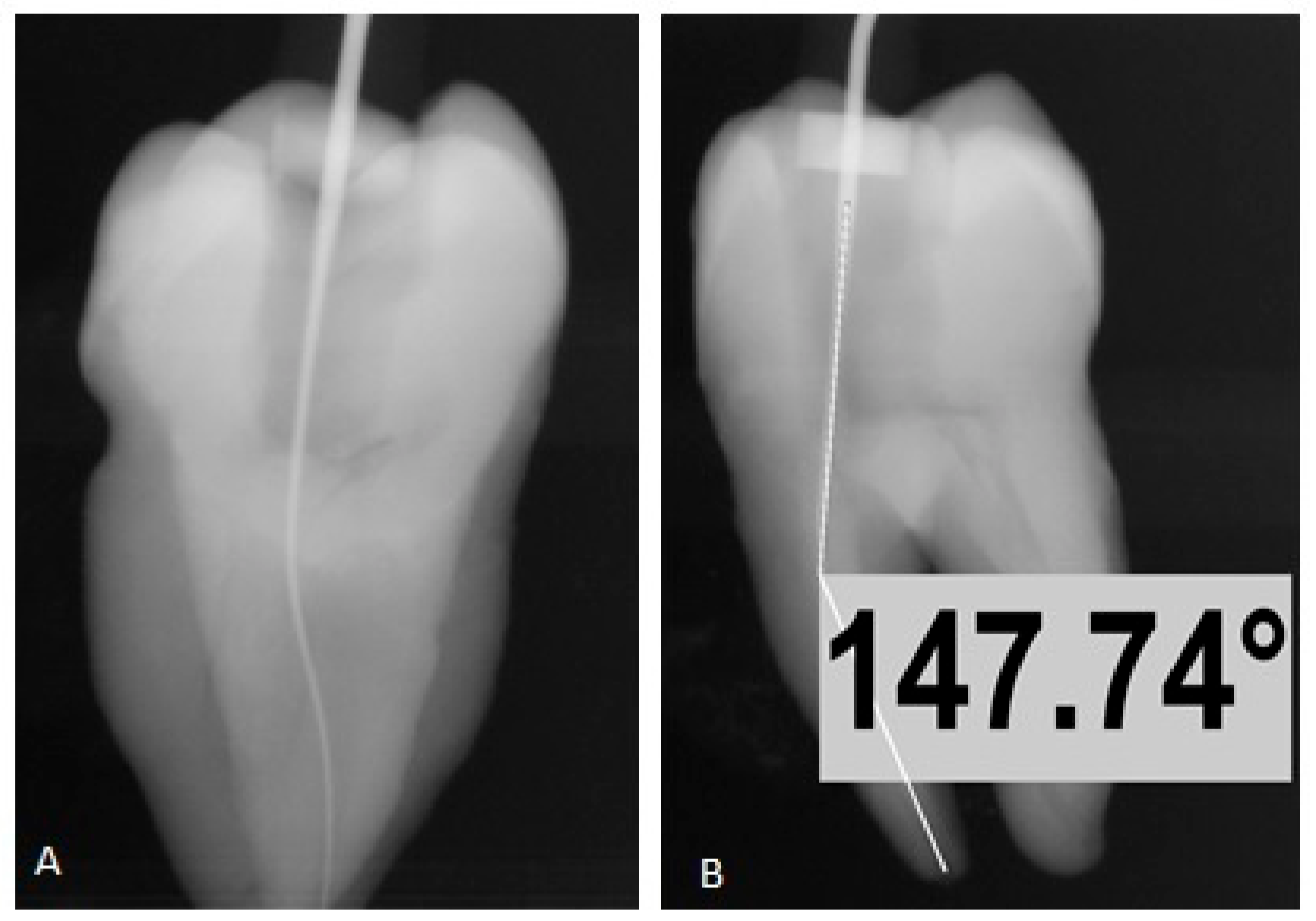
2.3. Determination of Canal Curvature Using Plywood Jig Technique
2.4. Determination of Canal Curvature Using Schneider Technique
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 1. Effects of study characteristics on probability of success. Int. Endod. J. 2007, 40, 921–939. [Google Scholar] [CrossRef] [PubMed]
- Karobari, M.I.; Noorani, T.Y.; Halim, M.S.; Ahmed, H.M.A. Root and canal morphology of the anterior permanent dentition in Malaysian population using two classification systems: A CBCT clinical study. Aust. Endod. J. 2020. [Google Scholar] [CrossRef]
- Schneider, S.W. A comparison of canal preparations in straight and curved root canals. Oral Surg. Oral Med. Oral Pathol. 1971, 32, 271–275. [Google Scholar] [CrossRef]
- Pineda, F.; Kuttler, Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg. Oral Med. Oral Pathol. 1972, 33, 101–110. [Google Scholar] [CrossRef]
- Estrela, C.; Bueno, M.R.; Sousa-Neto, M.D.; Pécora, J.D. Method for determination of root curvature radius using cone-beam computed tomography images. Braz. Dent. J. 2008, 19, 114–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Günday, M.; Sazak, H.; Garip, Y. A Comparative Study of Three Different Root Canal Curvature Measurement Techniques and Measuring the Canal Access Angle in Curved Canals. J. Endod. 2005, 31, 796–798. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Ha, B.H.; Choi, J.H.; Heo, S.M.; Perinpanayagam, H. Quantitative three-dimensional analysis of root canal curvature in maxillary first molars using micro-computed tomography. J. Endod. 2006, 32, 941–945. [Google Scholar] [CrossRef] [PubMed]
- Guelzow, A.; Stamm, O.; Martus, P.; Kielbassa, A.M. Comparative study of six rotary nickel-titanium systems and hand instrumentation for root canal preparation. Int. Endod. J. 2005, 38, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Carpegna, G.; Alovisi, M.; Paolino, D.S.; Marchetti, A.; Gibello, U.; Scotti, N.; Pasqualini, D.; Scattina, A.; Chiandussi, G.; Berutti, E. Evaluation of Pressure Distribution against Root Canal Walls of NiTi Rotary Instruments by Finite Element Analysis. Appl. Sci. 2020, 10, 2981. [Google Scholar] [CrossRef]
- Mazzoni, A.; Pacifici, A.; Zanza, A.; Giudice, A.; Reda, R.; Testarelli, L.; Gambarini, G.; Pacifici, L. Assessment of Real-Time Operative Torque during Nickel–Titanium Instrumentation with Different Lubricants. Appl. Sci. 2020, 10, 6201. [Google Scholar] [CrossRef]
- Plotino, G.; Grande, N.M.; Melo, M.C.; Bahia, M.G.D.A.; Testarelli, L.; Gambarini, G. Cyclic fatigue of NiTi rotary instruments in a simulated apical abrupt curvature. Int. Endod. J. 2010, 43, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Lopes, H.P.; Chiesa, W.M.; Correia, N.R.; de Souza Navegante, N.C.; Elias, C.N.; Moreira, E.J.; Chiesa, B.E. Influence of curvature location along an artificial canal on cyclic fatigue of a rotary nickel-titanium endodontic instrument. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 111, 792–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhagabati, N.; Yadav, S.; Talwar, S. An In Vitro Cyclic Fatigue Analysis of Different Endodontic Nickel-Titanium Rotary Instruments. J. Endod. 2012, 38, 515–518. [Google Scholar] [CrossRef]
- Bhandi, S.; Seracchiani, M.; Donfrancesco, O. Nickel–Titanium Rotary Instruments: An In Vitro Comparison. J. Contemp. Dent. Pract. 2021. [Google Scholar] [CrossRef]
- Gambarini, G.; Miccoli, G.; D’Angelo, M.; Seracchiani, M.; Obino, F.V.; Reda, R.; Testarelli, L. The relevance of operative torque and torsional resistance of nickel-titanium rotary instruments: A preliminary clinical investigation. Saudi Endod. J. 2020, 10, 260–264. [Google Scholar]
- Slowey, R.R. Root canal anatomy. Road map to successful endodontics. Dent. Clin. N. Am. 1979, 23, 555–573. [Google Scholar] [PubMed]
- Gu, Y.; Lu, Q.; Wang, P.; Ni, L. Root Canal Morphology of Permanent Three-rooted Mandibular First Molars: Part II—Measurement of Root Canal Curvatures. J. Endod. 2010, 36, 1341–1346. [Google Scholar] [CrossRef] [PubMed]
- Schilder, H. Cleaning and shaping the root canal. Dent. Clin. N. Am. 1974, 18, 269–296. [Google Scholar] [PubMed]
- Weine, F.S. Endodontic Therapy, 4th ed.; The C.V. Mosby Co.: St. Louis, MO, USA, 1989; p. 277. [Google Scholar]
- Abou-Rass, M.; Frank, A.L.; Glick, D.H. The Anticurvature Filing Method to Prepare the Curved Root Canal. J. Am. Dent. Assoc. 1980, 101, 792–794. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Angle of Curvature | Radius of Curvature | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Range | Mean | SD | Mean Values | Range | Mean | SD | Mean Values | ||
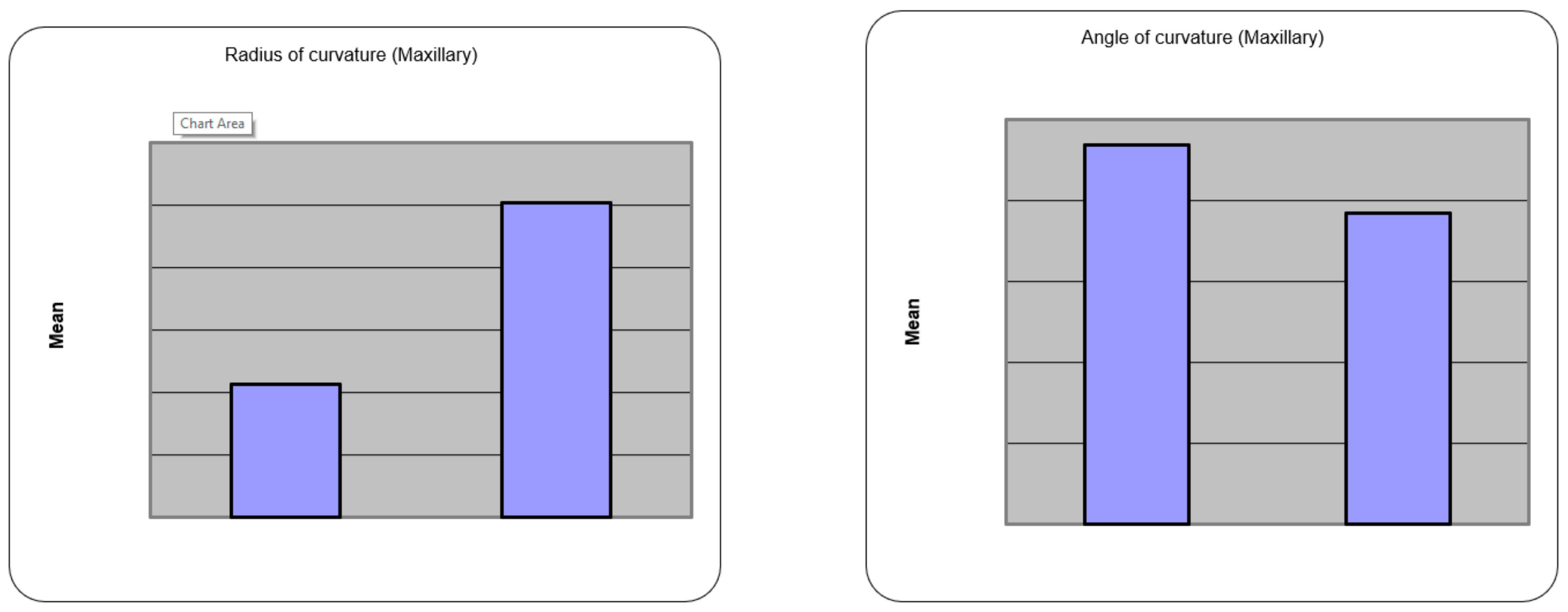
| Maxillary | Jig method | 009–70 | 23.40 | 11.36 | 23.40 | 4.2–36.6 | 16.06 | 8.12 | 16.06 |
| Schneiders method | 005–72 | 19.23 | 11.94 | 19.23 | 3.4–37.8 | 17.51 | 7.88 | 17.51 | |
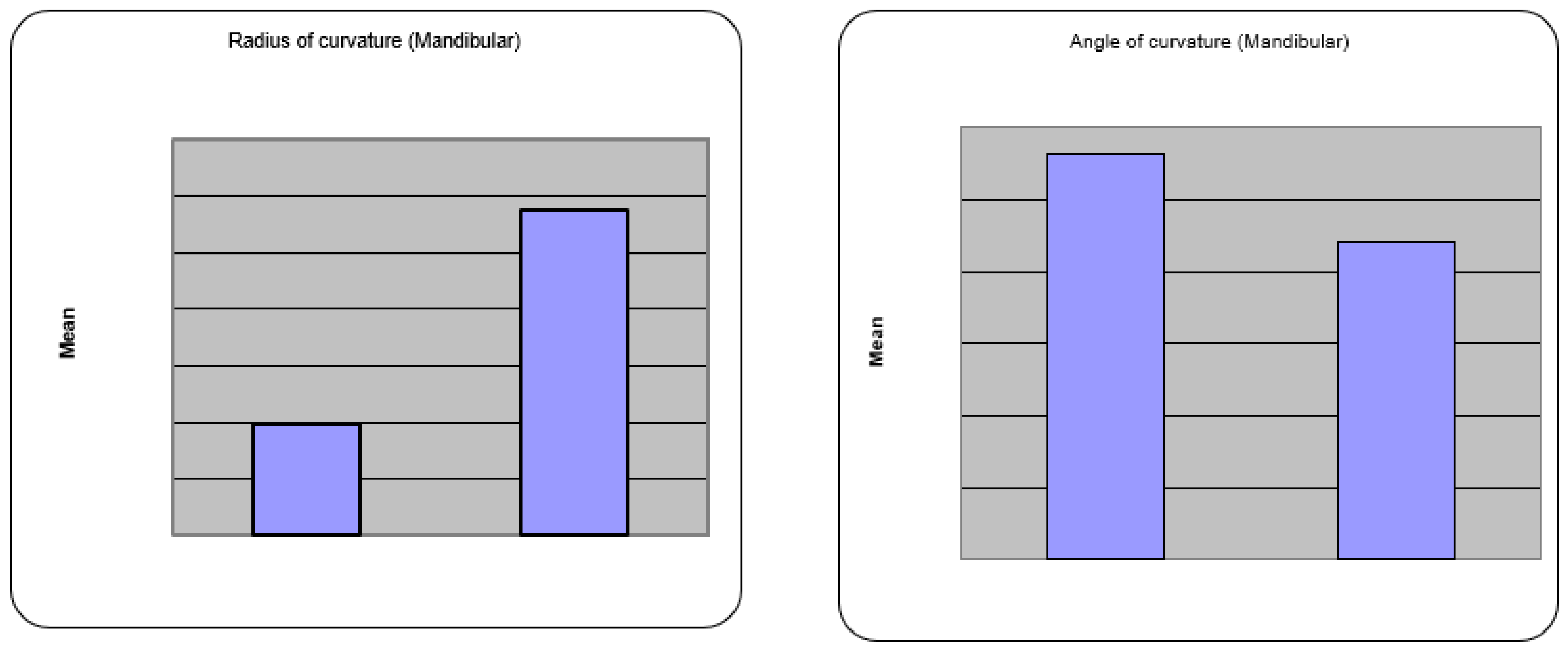
| Mandibular | Jig method | 0012–52 | 28.23 | 9.96 | 28.23 | 2.4–18.4 | 9.79 | 3.65 | 9.79 |
| Schneiders method | 008–44 | 22.07 | 9.46 | 22.07 | 2.8–18.4 | 10.55 | 3.34 | 10.55 | |
| Angle of Curvature | Radius of Curvature | Peak Height of Curvature | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| MD | PD | p Value | Sig | MD | PD | p Value | Sig | Mean | SD | |
| Maxillary | 4.17 | 22 | p < 0.001 | HS | 1.45 | 8 | p < 0.05 | S | 3.86 | 1.16 |
| Mandibular | 6.17 | 28 | p < 0.001 | HS | 0.75 | 7 | p < 0.001 | HS | 3.97 | 1.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makandar, S.D.; Khaiser, M.I.; Mali, S.R.; Karobari, M.I.; Marya, A.; Messina, P.; Scardina, G.A. Plywood Jig—A New Technique for Root Canal Curvature Measurement. Appl. Sci. 2021, 11, 3999. https://doi.org/10.3390/app11093999
Makandar SD, Khaiser MI, Mali SR, Karobari MI, Marya A, Messina P, Scardina GA. Plywood Jig—A New Technique for Root Canal Curvature Measurement. Applied Sciences. 2021; 11(9):3999. https://doi.org/10.3390/app11093999
Chicago/Turabian StyleMakandar, Saleem D., Mohammed Imran Khaiser, Sneha R. Mali, Mohmed Isaqali Karobari, Anand Marya, Pietro Messina, and Giuseppe Alessandro Scardina. 2021. "Plywood Jig—A New Technique for Root Canal Curvature Measurement" Applied Sciences 11, no. 9: 3999. https://doi.org/10.3390/app11093999