
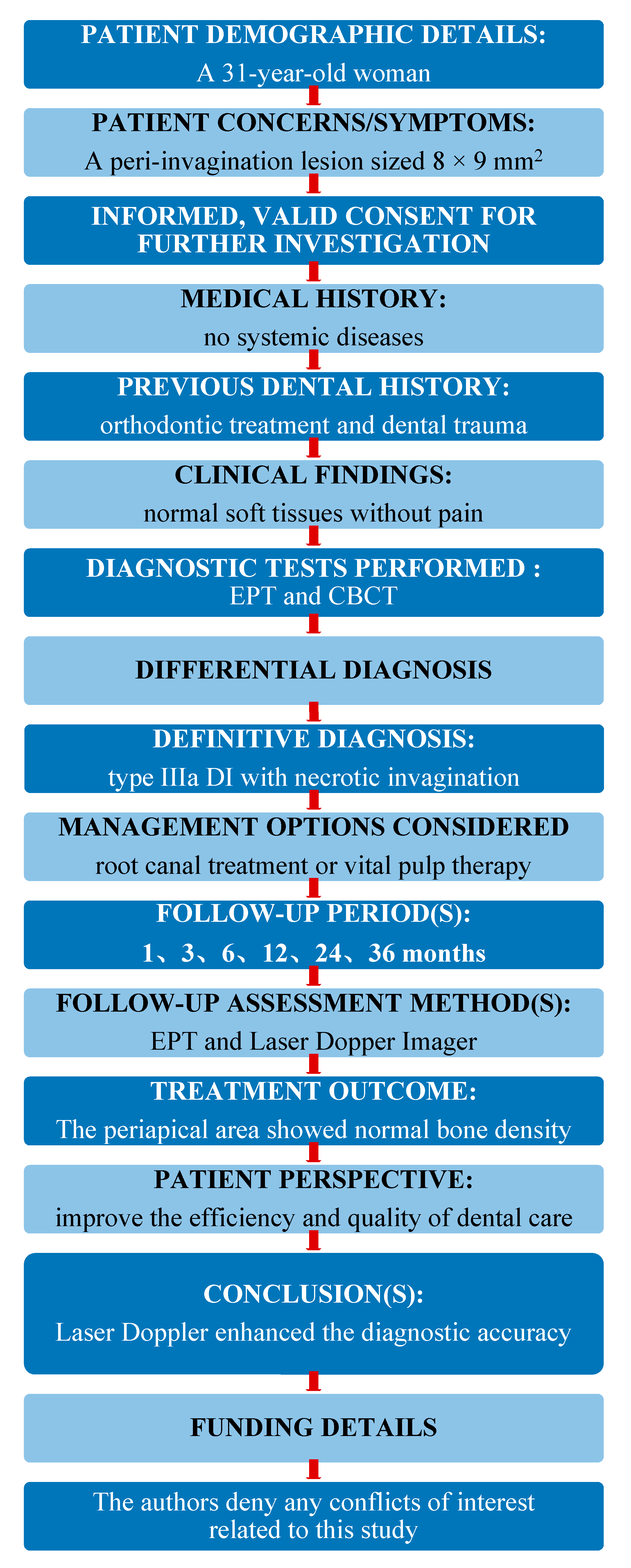
Laser Doppler for Accurate Diagnosis of Oehler’s Type III Dens Invaginatus: A Case Report

 and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alani, A.; Bishop, K. Dens invaginatus. Part 1: Classification, prevalence and aetiology. Int. Endod. J. 2008, 41, 1123–1136. [Google Scholar] [CrossRef]
- Agrawal, P.K.; Wankhade, J.; Warhadpande, M. A Rare Case of Type III Dens Invaginatus in a Mandibular Second Premolar and Its Nonsurgical Endodontic Management by Using Cone-beam Computed Tomography: A Case Report. J. Endod. 2016, 42, 669–672. [Google Scholar] [CrossRef]
- Capar, I.D.; Ertas, H.; Arslan, H.; Tarim Ertas, E. A retrospective comparative study of cone-beam computed tomography versus rendered panoramic images in identifying the presence, types, and characteristics of dens invaginatus in a Turkish population. J. Endod. 2015, 41, 473–478. [Google Scholar] [CrossRef]
- Liu, J.; Que, K.H.; Xiao, Z.H.; Wen, W. Endodontic management of the maxillary first molars with two root canals: A case report and review of the literature. World J. Clin. Cases. 2019, 7, 79–88. [Google Scholar] [CrossRef]
- Altuntas, A.; Cinar, C.; Akal, N. Endodontic treatment of immature maxillary lateral incisor with two canals: Type 3 dens invaginatus. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, e90–e93. [Google Scholar] [CrossRef]
- Brooks, J.K.; Ribera, M.J. Successful nonsurgical endodontic outcome of a severely affected permanent maxillary canine with dens invaginatus Oehlers type 3. J. Endod. 2014, 40, 1702–1707. [Google Scholar] [CrossRef]
- Keles, A.; Cakici, F. Endodontic treatment of a maxillary lateral incisor with vital pulp, periradicular lesion and type III dens invaginatus: A case report. Int. Endod. J. 2010, 43, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Kfir, A.; Telishevsky-Strauss, Y.; Leitner, A.; Metzger, Z. The diagnosis and conservative treatment of a complex type 3 dens invaginatus using cone beam computed tomography (CBCT) and 3D plastic models. Int. Endod. J. 2013, 46, 275–288. [Google Scholar] [CrossRef] [PubMed]
- Ghouth, N.; Duggal, M.S.; BaniHani, A.; Nazzal, H. The diagnostic accuracy of laser Doppler flowmetry in assessing pulp blood flow in permanent teeth: A systematic review. Dent. Traumatol. 2018, 34, 311–319. [Google Scholar] [CrossRef] [Green Version]
- Brignardello-Petersen, R. Laser Doppler flowmetry and pulse oximetry seem to have high accuracy in detecting vital and nonvital teeth and perform better than cold, heat, and electric pulp testing. J. Am. Dent. Assoc. 2018, 149, e152. [Google Scholar] [CrossRef] [PubMed]
- Civjan, S.; Barone, J.J.; Vaccaro, G.J. Electric pulp vitality testers. J. Dent. Res. 1973, 52, 120–126. [Google Scholar] [CrossRef]
- Karayilmaz, H.; Kirzioglu, Z. Comparison of the reliability of laser Doppler flowmetry, pulse oximetry and electric pulp tester in assessing the pulp vitality of human teeth. J. Oral. Rehabil. 2011, 38, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Olgart, L.; Gazelius, B.; Lindh-Stromberg, U. Laser Doppler flowmetry in assessing vitality in luxated permanent teeth. Int. Endod. J. 1988, 21, 300–306. [Google Scholar] [CrossRef]
- Ahn, S.Y.; Kim, D.; Park, S.H. Long-term Prognosis of Pulpal Status of Traumatized Teeth Exhibiting Contradictory Results between Pulp Sensibility Test and Ultrasound Doppler Flowmetry: A Retrospective Study. J. Endod. 2018, 44, 395–404. [Google Scholar] [CrossRef]
- Musu, D.; Shemesh, H.; Boccuzzi, M.; Dettori, C.; Cotti, E. Correction to: The effectiveness of ultrasound examination to assess the healing process of bone lesions of the jaws: A systematic review. Clin. Oral Investig. 2020, 24, 3739–3747. [Google Scholar] [CrossRef]
- Lee, J.K.; Hwang, J.J.; Kim, H.C. Treatment of peri-invagination lesion and vitality preservation in an immature type III dens invaginatus: A case report. BMC Oral Health 2020, 20, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gazelius, B.; Lindh-Stromberg, U.; Pettersson, H.; Oberg, P.A. Laser Doppler technique—A future diagnostic tool for tooth pulp vitality. Int. Endod. J. 1993, 26, 8–9. [Google Scholar] [CrossRef] [PubMed]
- Nosrat, A.; Schneider, S.C. Endodontic Management of a Maxillary Lateral Incisor with 4 Root Canals and a Dens Invaginatus Tract. J. Endod. 2015, 41, 1167–1171. [Google Scholar] [CrossRef]
- Teixido, M.; Abella, F.; Duran-Sindreu, F.; Moscoso, S.; Roig, M. The use of cone-beam computed tomography in the preservation of pulp vitality in a maxillary canine with type 3 dens invaginatus and an associated periradicular lesion. J. Endod. 2014, 40, 1501–1504. [Google Scholar] [CrossRef] [PubMed]
- Vier-Pelisser, F.V.; Pelisser, A.; Recuero, L.C.; So, M.V.; Borba, M.G.; Figueiredo, J.A. Use of cone beam computed tomography in the diagnosis, planning and follow up of a type III dens invaginatus case. Int. Endod. J. 2012, 45, 198–208. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Zhao, Y.; Qin, M.; Ge, L. Pulp revascularization of immature dens invaginatus with periapical periodontitis. J. Endod. 2013, 39, 288–292. [Google Scholar] [CrossRef]
- Zoya, A.; Ali, S.; Alam, S.; Tewari, R.K.; Mishra, S.K.; Kumar, A.; Andrabi, S.M.-U.-N. Double Dens Invaginatus with Multiple Canals in a Maxillary Central Incisor: Retreatment and Managing Complications. J. Endod. 2015, 41, 1927–1932. [Google Scholar] [CrossRef]
- Ersahan, S.; Sabuncuoglu, F.A.; Oktay, E.A. The Efficacy of Laser Doppler Flowmetry, Electric Pulp Test and Cold Test in Diagnosing Revascularization of Extrusively Luxated Immature Maxillary Incisors. Pak. J. Med. Sci. 2018, 34, 787–793. [Google Scholar] [CrossRef]
- Evans, D.; Reid, J.; Strang, R.; Stirrups, D. A comparison of laser Doppler flowmetry with other methods of assessing the vitality of traumatised anterior teeth. Endod. Dent. Traumatol. 1999, 15, 284–290. [Google Scholar] [CrossRef]
- Firestone, A.R.; Wheatley, A.M.; Thuer, U.W. Measurement of blood perfusion in the dental pulp with laser Doppler flowmetry. Int. J. Microcirc. Clin. Exp. 1997, 17, 298–304. [Google Scholar] [CrossRef]
- Gazelius, B.; Olgart, L.; Edwall, B. Restored vitality in luxated teeth assessed by laser Doppler flowmeter. Endod. Dent. Traumatol. 1988, 4, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Liao, Q.; Ye, W.; Yue, J.; Zhao, X.; Zhang, L.; Zhang, L.; Huang, D.; Zheng, Q. Self-repaired Process of a Traumatized Maxillary Central Incisor with Pulp Infarct after Horizontal Root Fracture Monitored by Laser Doppler Flowmetry Combined with Tissue Oxygen Monitor. J. Endod. 2017, 43, 1218–1222. [Google Scholar] [CrossRef]
- Ingolfsson, A.R.; Tronstad, L.; Hersh, E.V.; Riva, C.E. Efficacy of laser Doppler flowmetry in determining pulp vitality of human teeth. Endod. Dent. Traumatol. 1994, 10, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Ingolfsson, A.E.; Tronstad, L.; Riva, C.E. Reliability of laser Doppler flowmetry in testing vitality of human teeth. Endod. Dent. Traumatol. 1994, 10, 185–187. [Google Scholar] [CrossRef]
- Roy, E.; Alliot-Licht, B.; Dajean-Trutaud, S.; Fraysse, C.; Jean, A.; Armengol, V. Evaluation of the ability of laser Doppler flowmetry for the assessment of pulp vitality in general dental practice. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 106, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Park, S.H. Effects of age, sex, and blood pressure on the blood flow velocity in dental pulp measured by Doppler ultrasound technique. Microcirculation 2016, 23, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Raab, W.H.; Reithmayer, K.; Grund, P. Vitality tests of the tooth pulp using laser Doppler flowmetry. Dtsch. Zahnarztl. Z. 1990, 45, 725–727. [Google Scholar] [PubMed]
- Musselwhite, J.M.; Klitzman, B.; Maixner, W.; Burkes, E.J.J. Laser Doppler flowmetry: A clinical test of pulpal vitality. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1997, 84, 411–419. [Google Scholar] [CrossRef]
- Winzap-Kalin, C.; Chappuis, V.; von Arx, T. Laser Doppler flowmetry for vitality testing of traumatized maxillary incisors. Schweiz. Monatsschr. Zahnmed. 2005, 115, 12–17. [Google Scholar] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.-N.; Yan, D.-Y.; Huang, C.-Y.; Chen, S.-C.; Pan, C.-Y.; Jeng, J.-H.; Chen, Y.-K.; Chuang, F.-H. Laser Doppler for Accurate Diagnosis of Oehler’s Type III Dens Invaginatus: A Case Report. Appl. Sci. 2021, 11, 3848. https://doi.org/10.3390/app11093848
Lee H-N, Yan D-Y, Huang C-Y, Chen S-C, Pan C-Y, Jeng J-H, Chen Y-K, Chuang F-H. Laser Doppler for Accurate Diagnosis of Oehler’s Type III Dens Invaginatus: A Case Report. Applied Sciences. 2021; 11(9):3848. https://doi.org/10.3390/app11093848
Chicago/Turabian StyleLee, Hui-Na, Dah-You Yan, Chun-Yin Huang, Shih-Chieh Chen, Chin-Yun Pan, Jiiang-Huei Jeng, Yuk-Kwan Chen, and Fu-Hsiung Chuang. 2021. "Laser Doppler for Accurate Diagnosis of Oehler’s Type III Dens Invaginatus: A Case Report" Applied Sciences 11, no. 9: 3848. https://doi.org/10.3390/app11093848