
Effectiveness of Shock Wave Therapy versus Intra-Articular Corticosteroid Injection in Diabetic Frozen Shoulder Patients’ Management: Randomized Controlled Trial

 ,
,
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
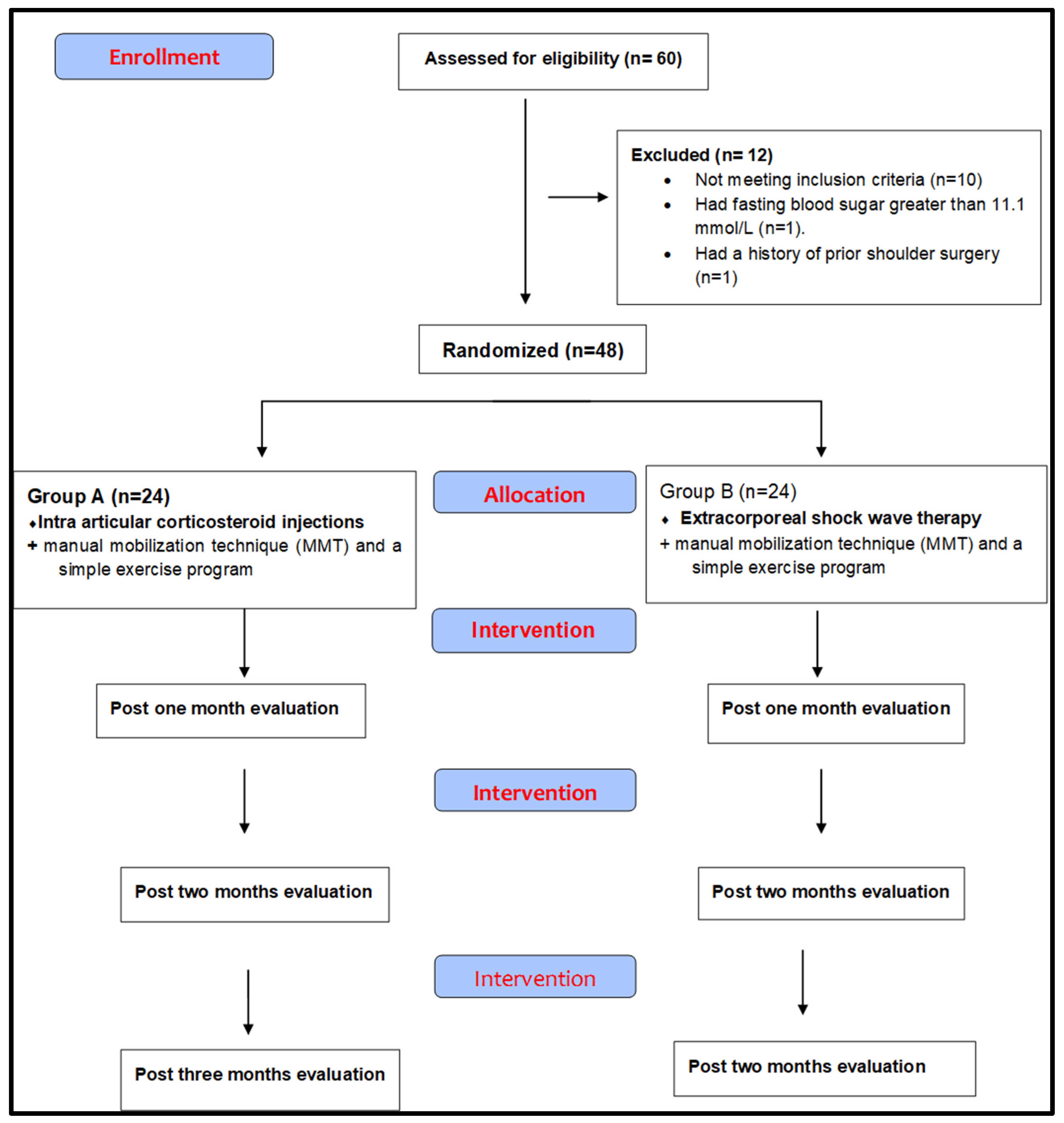
2.1. Design of the Study
2.2. Participants
2.3. Sample Size and Randomization
2.4. Outcome Measurements
2.4.1. The Primary Outcome Measurements
2.4.2. Secondary Outcome Measurements
2.5. Interventions
2.5.1. Traditional Physiotherapy Protocol
2.5.2. Intraarticular Corticosteroid Injection
2.5.3. Shock Wave Therapy
2.6. Data Analysis
Statistical Analysis
3. Results
3.1. Between-Groups Effect
3.2. Within-Group Effect
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Clinical Trial Registration
References
- Pai, L.-W.; Li, S.-F.; Chen, L.-L.; Liu, H.-L.; Hung, C.-T.; Chung, Y.-C. Musculoskeletal pain in people with and without type 2 diabetes in Taiwan: A population-based, retrospective cohort study. BMC Musculoskelet. Disord. 2015, 16, 364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larkin, M.E.; Barnie, A.; Braffett, B.H. Diabetes Control and Complications Trial/ Epidemiology of Diabetes Interventions and Complications Research Group. Musculoskeletal complications in type 1 diabetes. Diabetes Care 2014, 37, 1863–1869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zreik, N.H.; Malik, R.; Charalambous, C. Adhesive capsulitis of the shoulder and diabetes: A meta-analysis of prevalence. Muscle Ligaments Tendons J. 2019, 6, 26. [Google Scholar] [CrossRef]
- Laslett, L.L.; Burnet, S.P.; Jones, J.; Redmond, C.L.; McNeil, J.D. Musculoskeletal morbidity: The growing burden of shoulder pain and disability and poor quality of life in diabetic outpatients. Clin. Exp. Rheumatol. 2007, 25, 422–429. [Google Scholar] [PubMed]
- Le, H.V.; Lee, S.J.; Nazarian, A.; Rodriguez, E.K. Adhesive capsulitis of the shoulder: Review of pathophysiology and current clinical treatments. Shoulder Elb. 2017, 9, 75–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jainandn, K.; Sharma, K. The effectiveness of physiotherapeutic interventions in treatment of frozen shoulder/adhesive cap-sulitis: A systematic review. J. Back Musculoskelet. Rehabil. 2014, 27, 247–273. [Google Scholar]
- Elhafez, H.M.; Elhafez, S.M. Axillary Ultrasound and Laser Combined With Postisometric Facilitation in Treatment of Shoulder Adhesive Capsulitis: A Randomized Clinical Trial. J Manip. Physiol Ther. 2016, 39, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Baliwan, V.; Sen, S.; Badoni, N.; Khatri, N. Prevalence and management of the diabetic frozen shoulder. Int. J. Adv. Res. 2020, 8, 944–954. [Google Scholar] [CrossRef]
- Lorbach, O.; Anagnostakos, K.; Scherf, C.; Seil, R.; Kohn, D.; Pape, D. Nonoperative management of adhesive capsulitis of the shoulder: Oral cortisone application versus intra-articular cortisone injections. J. Shoulder Elb. Surg. 2010, 19, 172–179. [Google Scholar] [CrossRef]
- Sun, Y.; Chen, J.; Li, H. Steroid injection and nonsteroidal antiinflammatory agents for shoulder pain: Systematic review and meta-analysis of randomized controlled trials. Medicine 2015, 94, e2216. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, L.G.; Smith, M.G.; Khan, S.A.; Smith, K.; Joshi, M. Manipulation or intra-articular steroids in the management of adhesive capsulitis of the shoulder? A prospective randomized trial. J. Shoulder Elb. Surg. 2009, 18, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.T.; Lin, J.; Chang, C.J.; Lin, Y.T.; Hou, S.M. Therapeutic effects of hyaluronic acid on osteoarthritis of the knee: A me-ta-analysis of randomized controlled trials. J. Bone Jt. Surg. Am. 2004, 86, 538–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hannafinja, J.A.; Chiaiata, T.A. Adhesive capsulitis. A treatment approach. Clin. Orthop. Relat. Res. 2000, 372, 95–109. [Google Scholar] [CrossRef]
- Grecco, M.V.; Brech, G.C.; Greve, J.M.D. One-year treatment follow-up of plantar fasciitis: Radial shockwaves vs. conventional physiotherapy. Clinics 2013, 68, 1089–1095. [Google Scholar] [CrossRef]
- Elerian, A.E.; Ewidea, T.M.; Nour, A. Effect of shock wave therapy versus corticosteroid injection in management of knee os-teoarthritis. Int. J. Physiother. 2016, 68, 246–251. [Google Scholar]
- Moya, D.; Ramón, S.; Schaden, W.; Wang, C.-J.; Guiloff, L.; Cheng, J.-H. The Role of Extracorporeal Shockwave Treatment in Musculoskeletal Disorders. J. Bone Jt. Surg. 2018, 100, 251–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saggini, R.; Di Stefano, A.; Saggini, A.; Bellomo, R.G. Clinical Application of Shock Wave Therapy in Muscu-Loskeletal Disorders: Part I. J. Biol. Regul. Homeost. Agents 2015, 29, 533–545. [Google Scholar]
- Elerian, A.E. Effect of shockwaves versus traditional physiotherapy in treating de quervain tenosynovitis. Int. J. Recent Sci. Res. 2016, 7, 9902–9906. [Google Scholar]
- Aydın, C.G.; Örsçelik, A.; Gök, M.C.; Akman, Y.E. The Efficacy of Extracorporeal Shock Wave Therapy for Chronic Coccydynia. Med. Princ. Pract. 2020, 29, 444–450. [Google Scholar] [CrossRef]
- Lebiedz, O.; Kay, J. Rheumatic manifestations of diabetes mellitus. Rheum. Dis. Clin. 2010, 36, 681–699. [Google Scholar] [CrossRef] [PubMed]
- Macdermid, J.C.; Solomon, P.; Prkachin, K. The Shoulder Painand Disability Index demonstrates factor, construct and longitu-dinal validity. BMC Musculoskelet Disord. 2006, 7, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, J.-S.; MacDermid, J.C.; Woodhouse, L.J. Measuring shoulder function: A systematic review of four questionnaires. Arthritis Rheum. 2009, 61, 623–632. [Google Scholar] [CrossRef]
- Mullaney, M.; McHugh., M.P.; Johnson, C.P.; Tyler, T.F. Reliability of shoulder range of motion comparing a goniometer to a digital level. Physiother Theory Pract. 2010, 26, 327–333. [Google Scholar] [CrossRef]
- Gutiérrez, E.; Héctor, A.; Felipe, P.; Zavala, G.; Gana, H.; Cavero-Redondo, I.; Álvarez-Bueno, C. Effectiveness of supervised early exercise program in patients with arthroscopic rotator cuff repair. Medicine 2020, 99, e18846. [Google Scholar] [CrossRef]
- Kashid, M.; Rai, S.K.; Chakrabarty, B.; Upreti, V.; Shaki, O. Is it necessary to screen patient with adhesive capsulitis of shoulder for diabetes mellitus? J. Fam. Med. Prim. Care 2019, 8, 2927–2932. [Google Scholar] [CrossRef] [PubMed]
- Nakandala, P.; Nanayakkara, I.; Wadugodapitiya, S.; Gawarammana, I. Physiotherapy Interventions for Adhesive Capsulitis of Shoulder: A Systematic Review. Int. J. Physiother. Res. 2015, 3, 1318–1325. [Google Scholar] [CrossRef]
- Vermeulen, H.M.; Obermann, W.R.; Burger, B.J. End-range mobilization techniques in adhesive capsulitis of the shoulder joint: A multiple-subject case report. Phys. Ther. 2000, 80, 1204–1213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.-L.; Chang, C.-W.; Chen, S.-Y.; Wang, S.-F.; Lin, J.-J. Mobilization Techniques in Subjects With Frozen Shoulder Syndrome: Randomized Multiple-Treatment Trial. Phys. Ther. 2007, 87, 1307–1315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Çeliker, R.; Arslan, S. Comparison of the efficacy of local corticosteroid injection and physical therapy for the treatment of adhesive capsulitis. Rheumatol. Int. 2001, 21, 20–23. [Google Scholar] [CrossRef]
- Cho, C.-H.; Bae, K.-C.; Kim, D.-H. Treatment Strategy for Frozen Shoulder. Clin. Orthop. Surg. 2019, 11, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Santoboni, F.; Balducci, S.; D’Errico, V.; Haxhi, J.; Vetrano, M.; Piccinini, G.; Ferretti, A.; Pugliese, G.; Vulpiani, M.C. Extracorporeal Shockwave Therapy Improves Functional Outcomes of Adhesive Capsulitis of the Shoulder in Patients with Diabetes. Diabetes. Care Feb. 2017, 40, e12–e13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, R.; Cutts, S.; Massoud, S. Clinical Review: Frozen Shoulder. Br. Med. J. 2005, 331, 1453–1456. [Google Scholar] [CrossRef] [PubMed]
- Rizk, T.E.; Pinals, R.S. Frozen shoulder. Semin. Arthritis Rheum. 1982, 11, 440–452. [Google Scholar] [CrossRef]
- Koh, K.H. Corticosteroid injection for adhesive capsulitis in primary care: A systematic review of randomised clinical trials. Singap. Med. J. 2016, 57, 646–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vahdatpour, B.; Taheri, P.; Zade, A.Z.; Moradian, S. Efficacy of Extracorporeal Shockwave Therapy in Frozen Shoulder. Int. J. Prev. Med. 2014, 5, 875–881. [Google Scholar] [PubMed]
- Lee, S.; Lee, S.; Jeong, M.; Oh, H.; Lee, K. The effects of extracorporeal shock wave therapy on pain and range of motion in patients with adhesive capsulitis. J. Phys. Ther. Sci. 2017, 29, 1907–1909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loew, M.; Daecke, W.; Kusnierczak, D.; Rahmanzadeh, M.; Ewerbeck, V. Shock-wave therapy is effective for chronic calcifying tendinitis of the shoulder. J. Bone Jt. Surgery. Br. Vol. 1999, 81, 863–867. [Google Scholar] [CrossRef]
- Hammer, D.S.; Rupp, S.; Ensslin, S.; Kohn, D.; Seil, R. Extracorporal shock wave therapy in patients with tennis elbow and painful heel. Arch. Orthop. Trauma Surg. 2000, 120, 304–307. [Google Scholar] [CrossRef] [PubMed]
- Serizawa, F.; Ito, K.; Matsubara, M.; Sato, A.; Shimokawa, H.; Satomi, S. Extracorporeal Shock Wave Therapy Induces Therapeutic Lymphangiogenesis in a Rat Model of Secondary Lymphoedema. Eur. J. Vasc. Endovasc. Surg. 2011, 42, 254–260. [Google Scholar] [CrossRef] [Green Version]
- Mark, E. Current methods of assessing blood glucose control in diabetes. Br. J. Diabetes 2016, 16 (Suppl. 1), S7–S9. [Google Scholar]
- Choudhry, M.N.; Malik, R.A.; Charalambos, P. Blood glucose levels following intra-articular steroid injections in patients with diabetes: A systematic review. JBJS Rev. 2016, 4, 3. [Google Scholar] [CrossRef]
- Li, H.; Xiong, Y.; Zhou, W.; Liu, Y.; Liu, J.; Xue, H.; Hu, L.; Panayi, A.C.; Mi, B.; Liu, G. Shock-wave therapy improved outcome with plantar fasciitis: A meta-analysis of randomized controlled trials. Arch. Orthop. Trauma Surg. 2019, 139, 1763–1770. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, C.-C.; Lin, C.-C.; Hou, Y.-S.; Ko, J.-Y.; Wang, C.-J. Low-Energy Extracorporeal Shock Wave Ameliorates Streptozotocin Induced Diabetes and Promotes Pancreatic Beta Cells Regeneration in a Rat Model. Int. J. Mol. Sci. 2019, 20, 4934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsiao, C.-C.; Huang, W.-H.; Cheng, K.-H.; Lee, C.-T. Low-Energy Extracorporeal Shock Wave Therapy Ameliorates Kidney Function in Diabetic Nephropathy. Oxid. Med. Cell. Longev. 2019, 2019, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Shin, W.-Y.; An, M.-J.; Im, N.-G.; Oh, K.-R.; Choe, Y.; Yoon, S.-R.; Ryu, S.-R. Changes in Blood Glucose Level After Steroid Injection for Musculoskeletal Pain in Patients with Diabetes. Ann. Rehabil. Med. 2020, 44, 117–124. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Outcome Variables | Group A (n = 24) | Group B (n = 24) | MD(95%CI) | p-Value ** | |
|---|---|---|---|---|---|
| SPADI Score | post 1 month | 7.33 ± 1.03 | 7.04 ± 0.86 | 0.29 (−0.26, 0.84) | 0.29 |
| post 2 months | 6.23 ± 1.13 | 4.23 ± 1.2 | 2.0 (1.32, 2.67) | <0.0001 | |
| post 3 months | 4.77 ± 1.34 | 1.98 ± 0.74 | 2.79 (2.16, 3.42) | <0.0001 | |
| Shoulder Flexion ROM (deg.) | Post 1 month | 66.67 ± 15.23 | 113.8 ± 19.85 | −47.1 (−57.4, −36.8) | <0.0001 |
| Post 2 months | 74.38 ± 18.32 | 136.3 ± 18.31 | −61.9 (−72.5, −51.2) | <0.0001 | |
| Post 3 months | 91.67 ± 21.2 | 151.7 ± 8.93 | −60.0 (−69.5, −50.5) | <0.0001 | |
| Shoulder Abduction ROM (deg.) | Post 1 month | 51.25 ± 7.41 | 67.5 ± 13.19 | −16.3 (−22.5, −10.0) | <0.0001 |
| Post 2 months | 56.67 ± 6.86 | 82.5 ± 15.46 | −25.8 (−32.8, −18.9) | <0.0001 | |
| Post 3 months | 62.21 ± 12.47 | 101.5 ± 15.78 | −63.3 (−44.5, −28.0) | <0.0001 | |
| FBG (mg/dL) | Post 1 month | 148.1 ± 22.93 | 146.5 ± 14.56 | 1.67 (−9.49, 12.83) | 0.77 |
| Post 2 months | 181.3 ± 23.6 | 142.5 ± 12.94 | 38.75 (27.69, 49.81) | <0.0001 | |
| Post 3 months | 196.9 ± 25.49 | 136.7 ± 28.92 | 60.21 (44.37, 76.05) | <0.0001 | |
| PPBG (mg/dL) | Post 1 month | 201.7 ± 23.48 | 213.8 ± 24.99 | −12.1 (−26.2, 2.01) | 0.09 |
| Post 2 months | 252.5 ± 19.39 | 209.8 ± 22.48 | 42.71 (30.51, 54.91) | <0.0001 | |
| Post 3 months | 286.7 ± 33.74 | 195 ± 8.20.78 | 90.83 (74.55, 107.1) | <0.0001 | |
| HbA1C (mg/dL) | Post 3 months | 8.71 ± 1.01 | 6.91 ± 0.66 | 1.8 (1.3, 2.29) | <0.0001 |
| Characteristics | Group A (n = 24) | Group B (n = 24) |
|---|---|---|
| Age(years) | 51.33 ± 4.01 | 52.13 ± 3.06 |
| BMI (Kg/m2) | 37.65 ± 0.85 | 37.7 ± 1.07 |
| SPADI Score | 8.92 ± 0.76 | 8.92 ± 0.78 |
| Shoulder Flexion ROM (deg.) | 62.29 ± 14.82 | 64.38 ± 13.28 |
| Shoulder ABDUCTION ROM (deg.) | 45.00 ± 8.47 | 48.13 ± 13.97 |
| FBG (mg/dL) | 149.13 ± 23.93 | 151 ± 19.07 |
| PPBG mg/dL | 203.76 ± 24.5 | 228.54 ± 36.04 |
| HbA1c % | 6.53 ± 0.85 | 7.30 ± 0.83 |
| Baseline vs. 1 Month | Baseline vs. 2 Months | Baseline vs. 3 Months | ||||
|---|---|---|---|---|---|---|
| Outcomes | MD (95% CI) | p-Value | MD (95% CI) | p-Value | MD (95% CI) | p-Value |
| SPADI Score | 1.63 (1.13, 2.12) | 0.0001 | 2.73 (1.99, 3.46) | 0.0001 | 4.19 (3.47, 4.91) | 0.0001 |
| Flexion ROM (deg.) | 28.96 (−36.9, 94.81) | 0.99 | 21.25 (−45.0, −87.47) | 0.99 | 3.96 (−61.8, 69.69) | 0.99 |
| Abduction ROM (deg.) | −6.25 (−11.0, −1.46) | 0.005 | −11.67 (−19.0, −4.29) | 0.0004 | −20.21 (−29.1, −11.3) | 0.0001 |
| FBG (mg/dL) | 0.01 (−3.69,3.69) | 0.99 | −33.13 (−41.3, −25.0) | 0.0001 | −48.75 (−62.2, −35.3) | 0.0001 |
| PPBG mg/dL | 0.01 (−7.25,7.25) | 0.99 | −50.83 (−64.3, −37.4) | 0.0001 | −85.0 (−103.3, −66.7) | 0.0001 |
| HbA1c% | - | - | - | - | −2.18 (−2.67, −1.68) | 0.0001 |
| Baseline vs. 1 Month | Baseline vs. 2 Months | Baseline vs. 3 Months | ||||
|---|---|---|---|---|---|---|
| Outcomes | MD (95% CI) | p-Value | MD (95% CI) | p-Value | MD (95% CI *) | p-Value ** |
| SPADI Score | 1.88 (1.38, 2.37) | 0.0001 | 4.69 (3.95, 5.42) | 0.0001 | 6.94 (6.22, 7.66) | 0.0001 |
| Flexion ROM (deg.) | − | 0.69 | −60.88 (−127.0, 5.35) | 0.09 | −76.29 (−142.0, −10.6) | 0.01 |
| Abduction ROM (deg.) | −19.38 (−24.2, −14.6) | 0.0001 | −34.38 (−41.8, −27.0) | 0.0001 | −53.33 (−62.2, −44.5) | 0.0001 |
| FBG (mg/dL) | 4.79 (1.11,8.48) | 0.005 | 8.75 (0.58, 16.92) | 0.03 | 14.58 (1.11, 28.06) | 0.03 |
| PPBG mg/dL | 14.79 (7.55,22.04) | 0.0001 | 18.75 (5.32, 32.18) | 0.002 | 32.71 (14.37, 51.05) | 0.0001 |
| HbA1c % | - | - | - | - | 0.39 (−0.11, 0.89) | 0.21 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elerian, A.E.; Rodriguez-Sanz, D.; Abdelaziz Elsherif, A.; Dorgham, H.A.; Al-Hamaky, D.M.A.; El Fakharany, M.S.; Ewidea, M. Effectiveness of Shock Wave Therapy versus Intra-Articular Corticosteroid Injection in Diabetic Frozen Shoulder Patients’ Management: Randomized Controlled Trial. Appl. Sci. 2021, 11, 3721. https://doi.org/10.3390/app11083721
Elerian AE, Rodriguez-Sanz D, Abdelaziz Elsherif A, Dorgham HA, Al-Hamaky DMA, El Fakharany MS, Ewidea M. Effectiveness of Shock Wave Therapy versus Intra-Articular Corticosteroid Injection in Diabetic Frozen Shoulder Patients’ Management: Randomized Controlled Trial. Applied Sciences. 2021; 11(8):3721. https://doi.org/10.3390/app11083721
Chicago/Turabian StyleElerian, Ahmed Ebrahim, David Rodriguez-Sanz, Abdelaziz Abdelaziz Elsherif, Hend Adel Dorgham, Dina Mohamed Ali Al-Hamaky, Mahmoud S. El Fakharany, and Mahmoud Ewidea. 2021. "Effectiveness of Shock Wave Therapy versus Intra-Articular Corticosteroid Injection in Diabetic Frozen Shoulder Patients’ Management: Randomized Controlled Trial" Applied Sciences 11, no. 8: 3721. https://doi.org/10.3390/app11083721