
Development of Robot Patient Lower Limbs to Reproduce the Sit-to-Stand Movement with Correct and Incorrect Applications of Transfer Skills by Nurses

 , , ,
, , ,
Abstract
:1. Introduction
1.1. Objective and Approach
1.2. Human Patient Simulator
1.3. Sit-to-Stand Transfer Skill
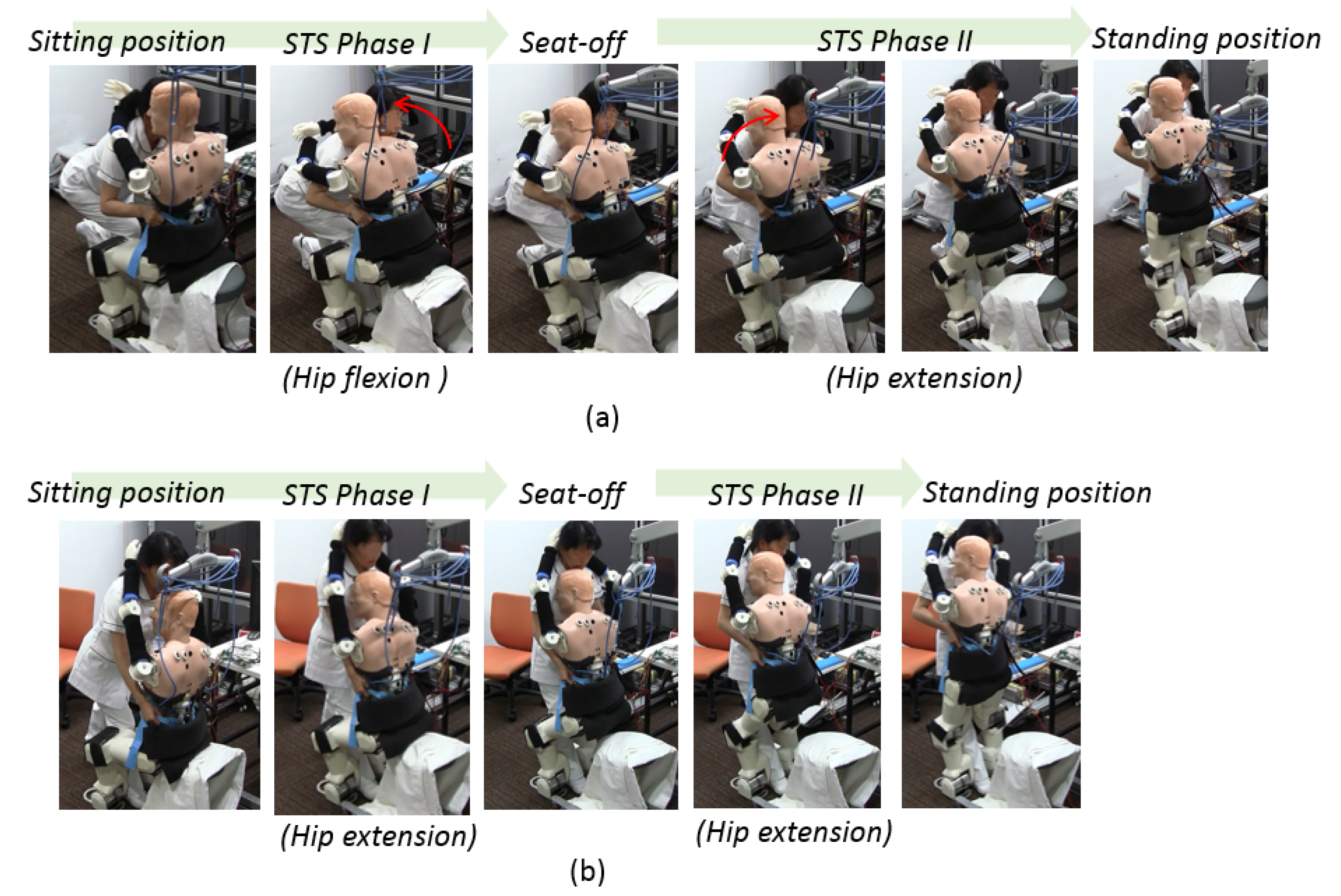
- Correct method: The nurse should squat down and lower their waist to prepare to help the patient with STS transfer.
- Incorrect method: The nurse does not bend their knees and lower the waist to assist the patient with the STS movement.
2. Requirements of the Robot Patient
2.1. Measured Parameters for Assessment
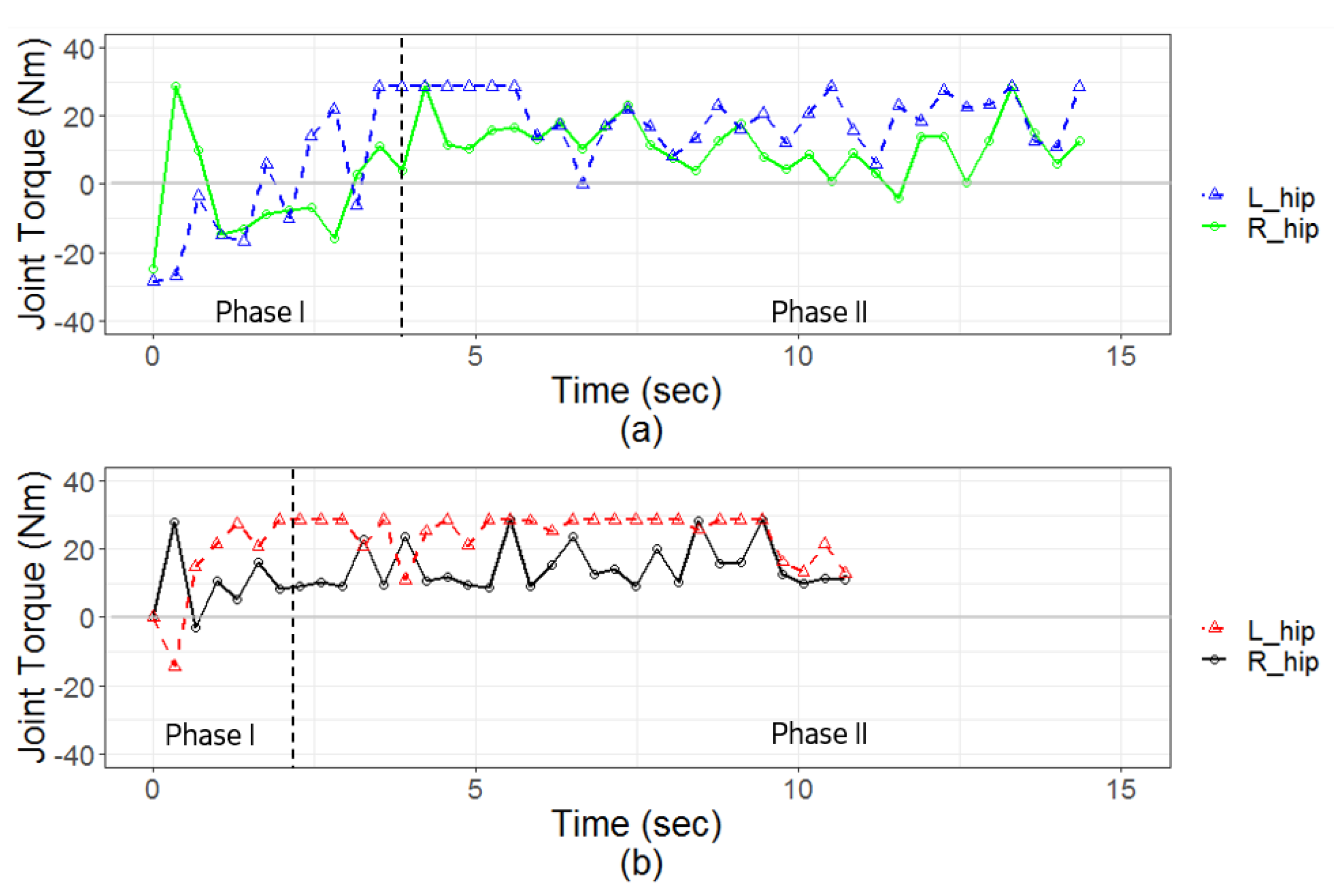
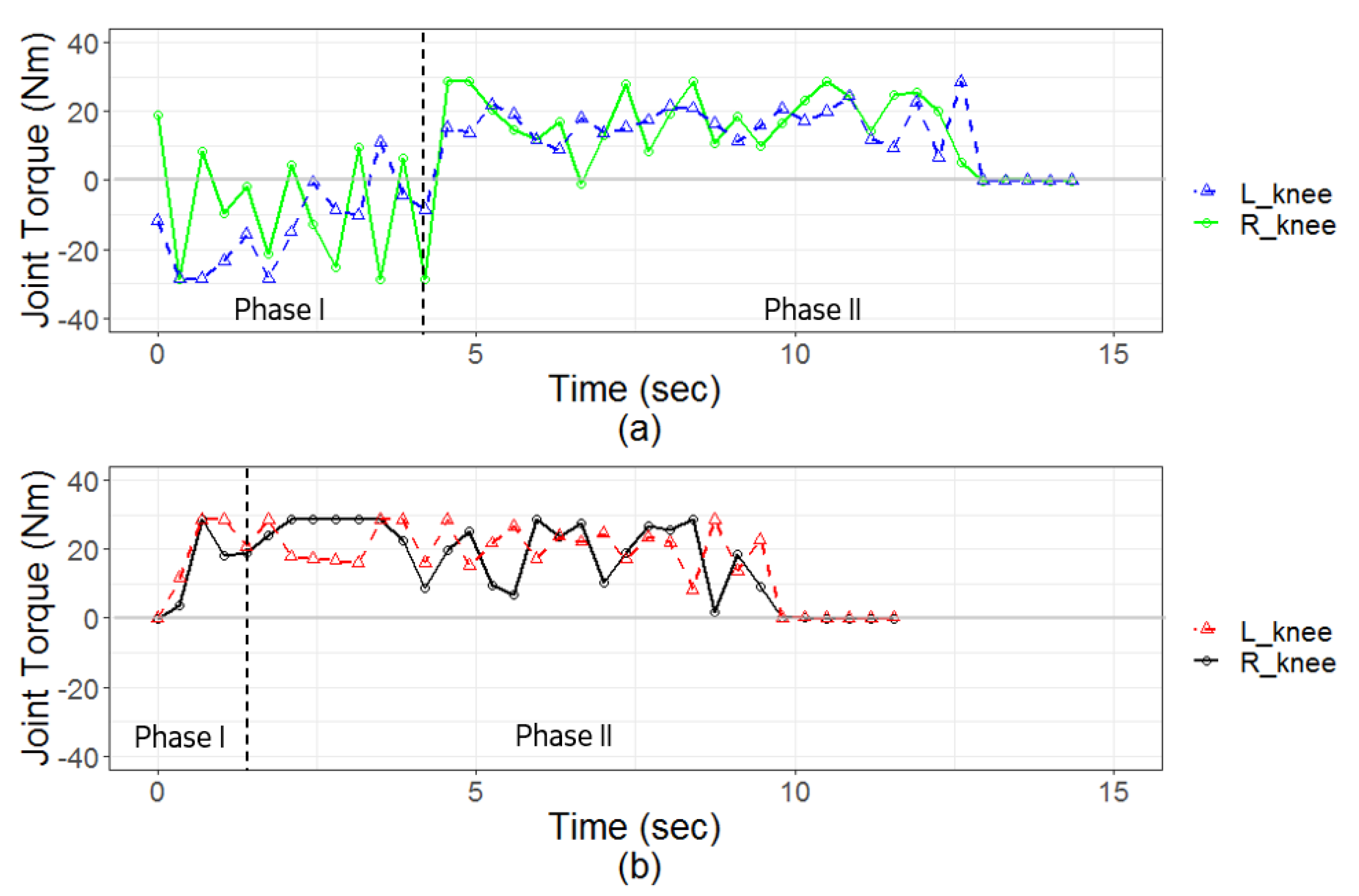
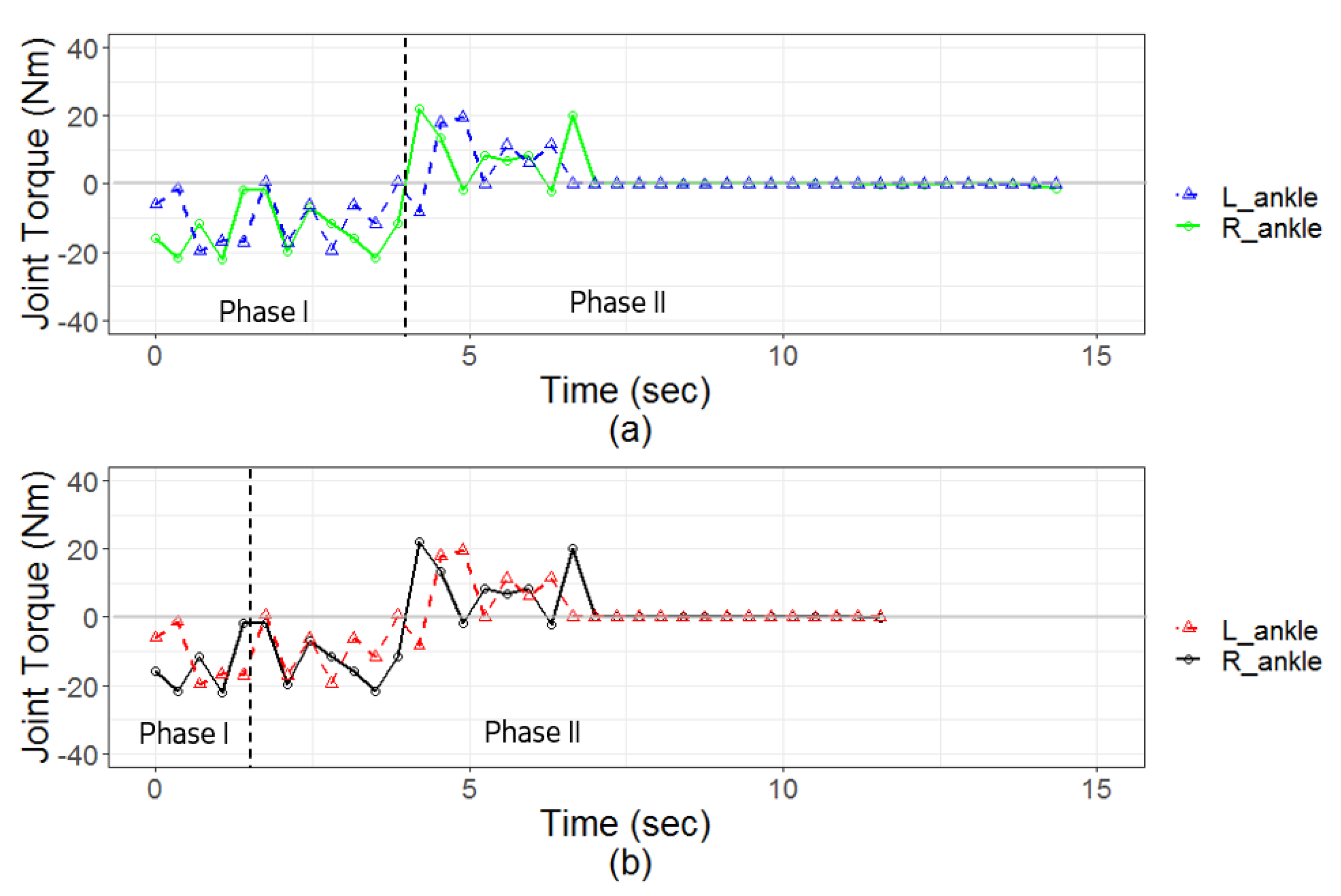
2.1.1. Joint Torque of Lower Limbs
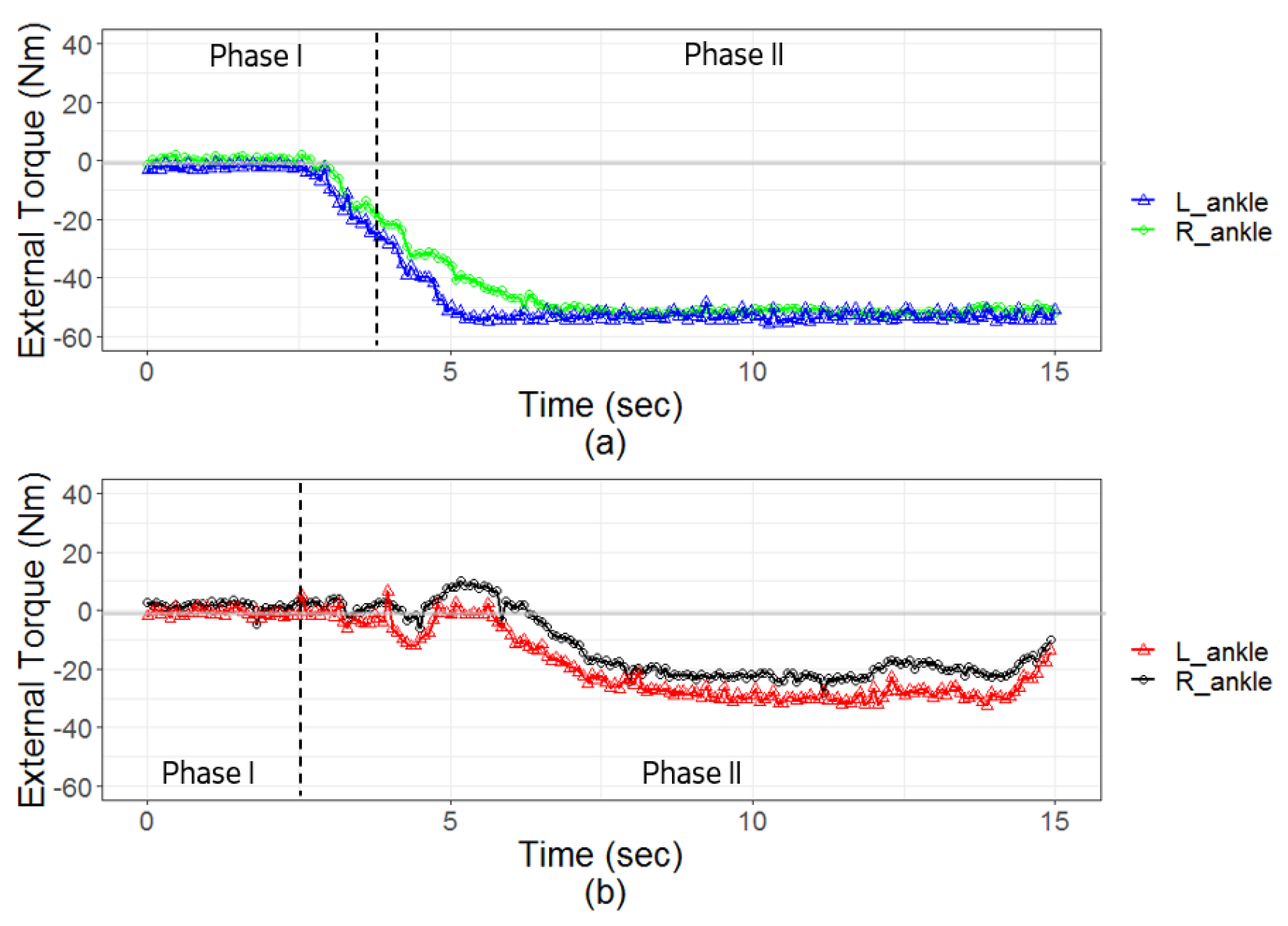
2.1.2. External Torque of Lower Limbs
2.2. Simulation of STS Movement by Robot Patient
2.2.1. Admittance Value of Physical Interaction
- Magnitude of Nurse’s Supporting ForceBased on the observations made during STS transfers, it was found that if the nurse exerted a larger force while supporting the patient, the patient was able to stand up more rapidly. In contrast, the patient stood up slowly when a smaller supporting force was applied by the nurse. This observation is also related to kinematics, with respect to the relation between force and acceleration. According to this relation, the magnitude of the nurse’s supporting force should proportionally influence the speed of the patient’s standing movement.
- Direction of Nurse’s Supporting ForceThe patient’s movement generally follows the direction of the supporting force applied by the nurse. For instance, if the nurse exerts a torque to bend the patient’s trunk, the patient’s hip joint will be flexed. If the nurse exerts a torque to extend the trunk, the patient’s trunk will be extended. Accordingly, the direction of the nurse’s supporting force was used as a factor in determining the direction of patient movement during STS transfer.
2.2.2. Correct and Incorrect Applications of Skills for Assisting STS Movement
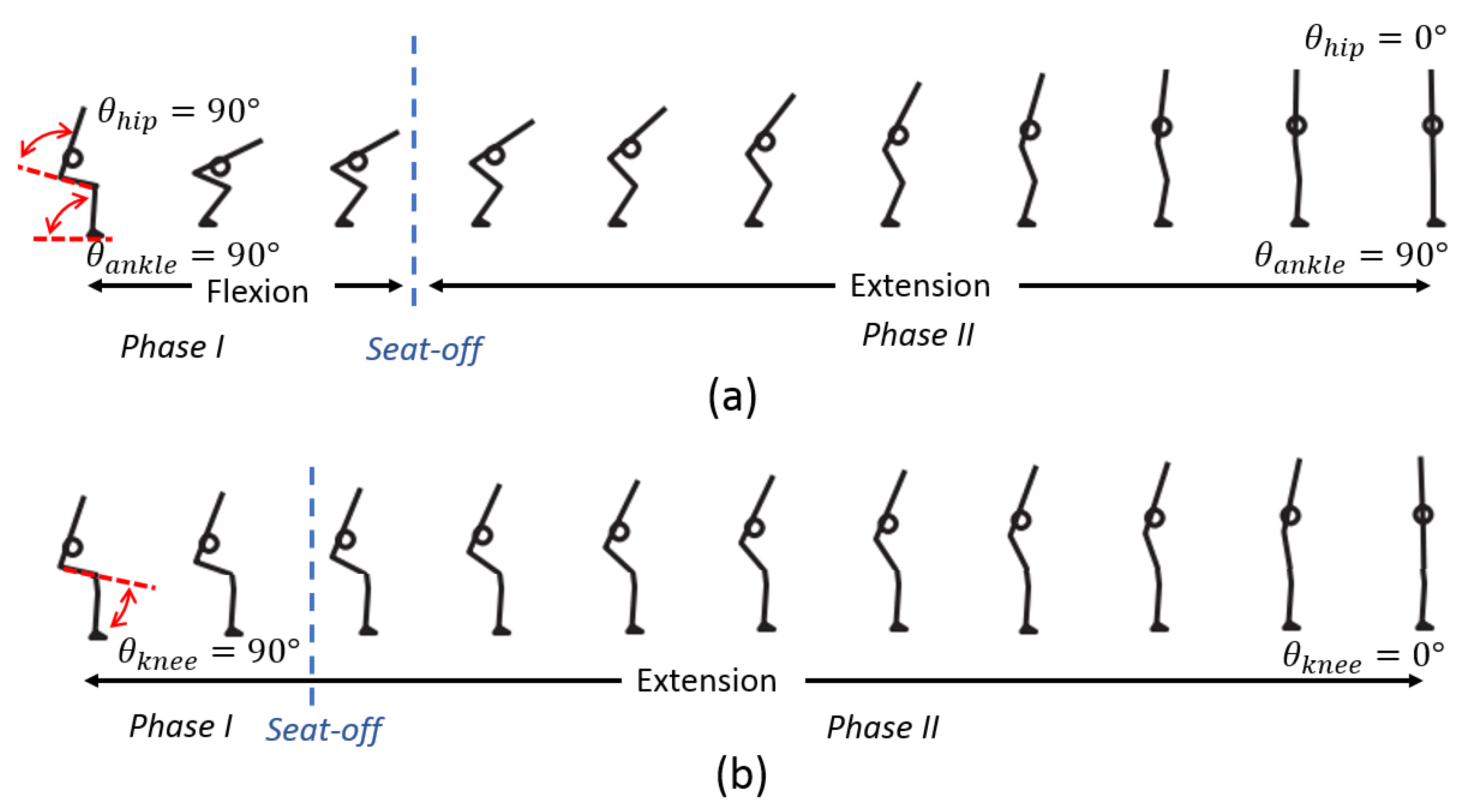
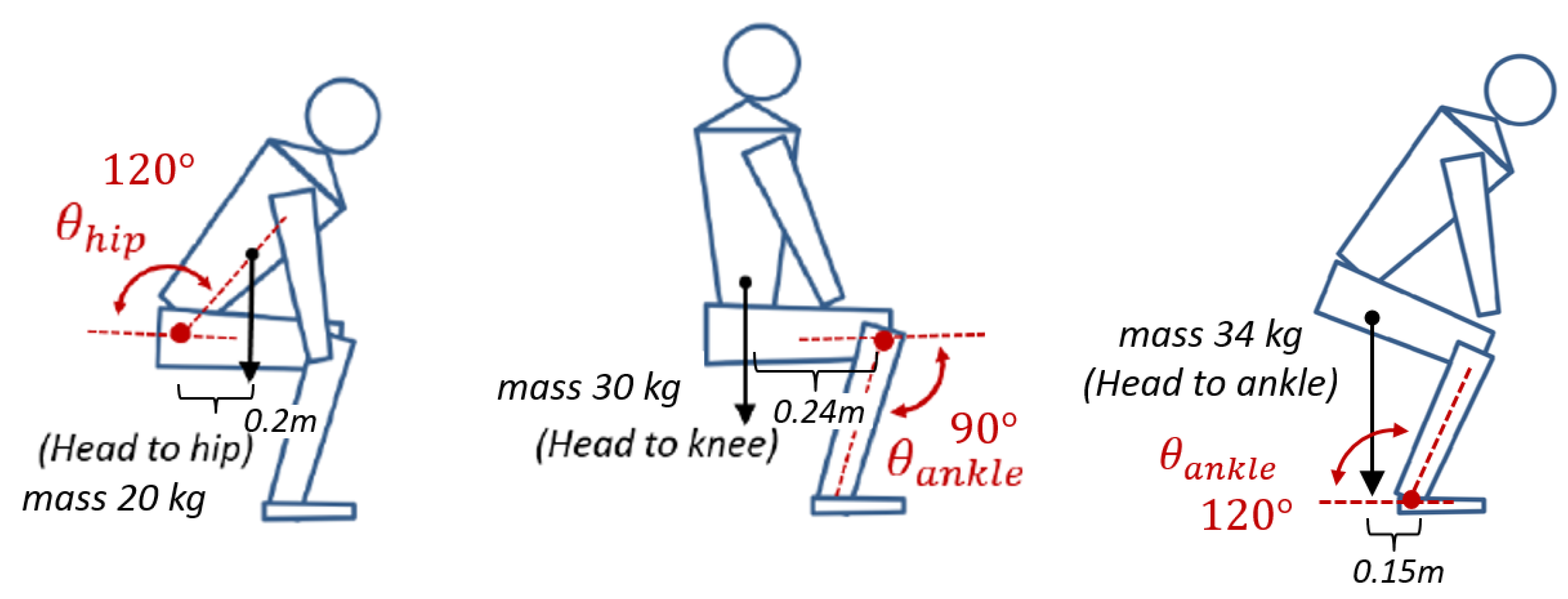
2.2.3. Range of Motion and Required Torque during STS Movement
2.3. Stiffness of Joint
3. Development of Robot Patient’s Lower Limbs
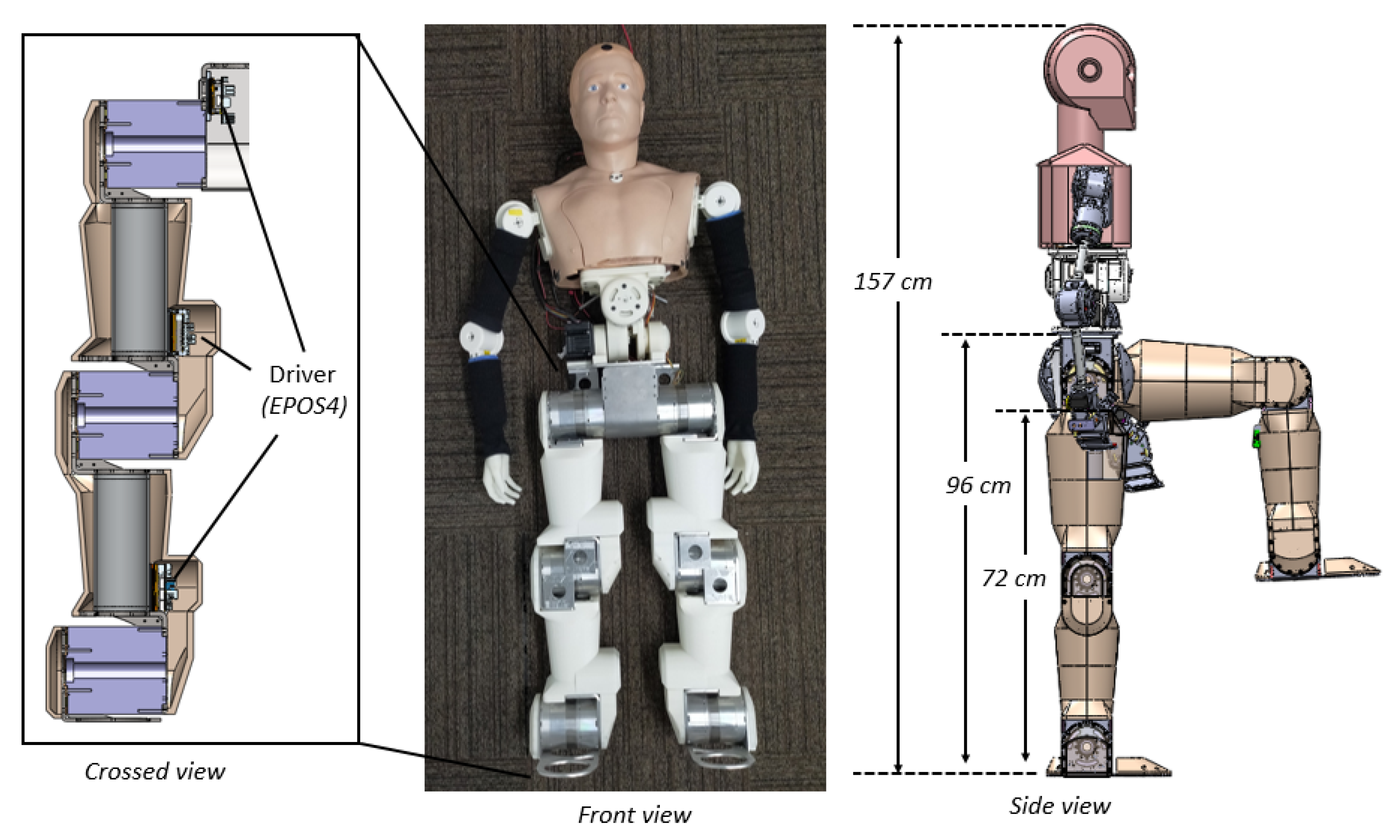
3.1. Robot Patient
3.2. Robot Patient’s Lower Limb
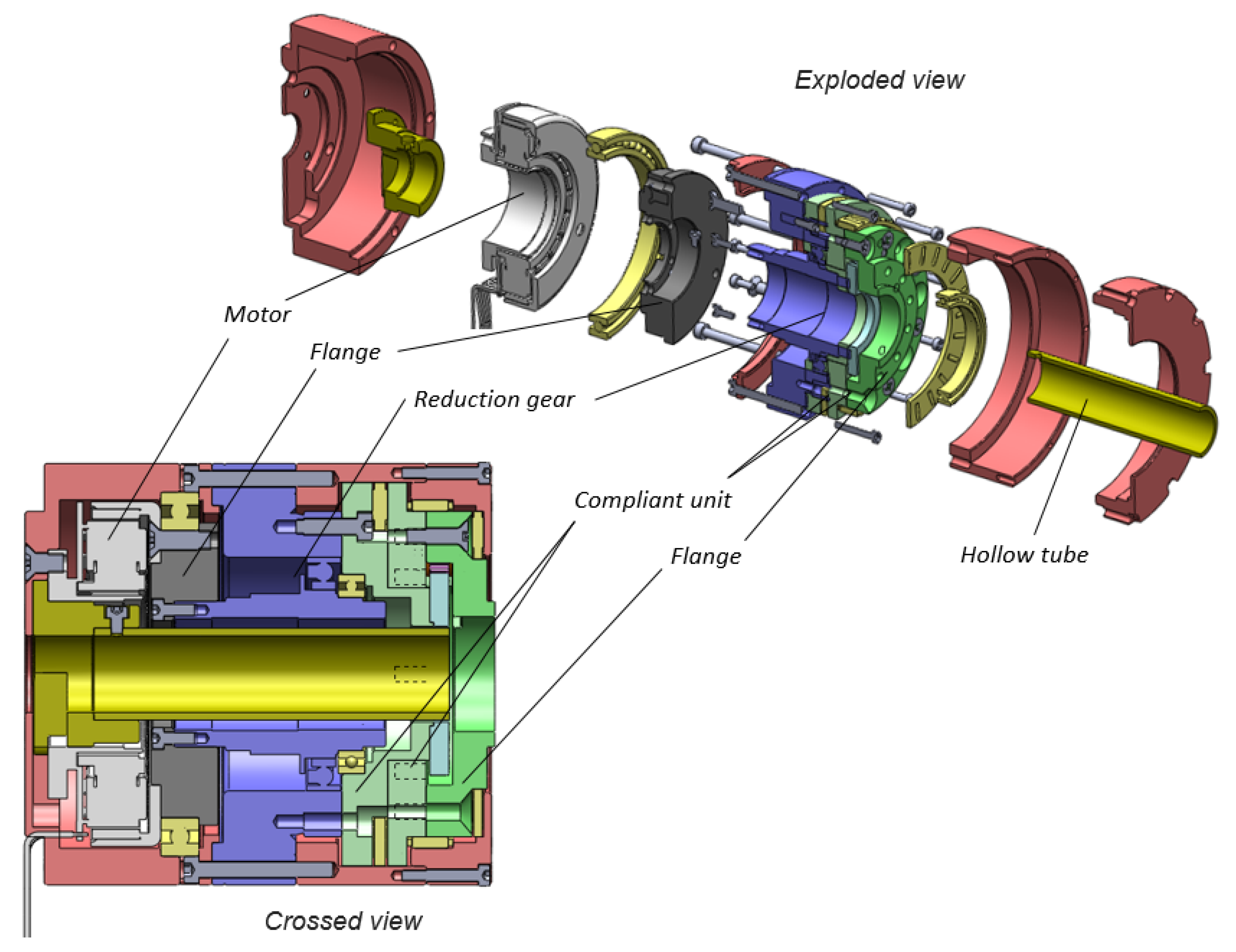
3.2.1. Hollow Modular Compliant Joint
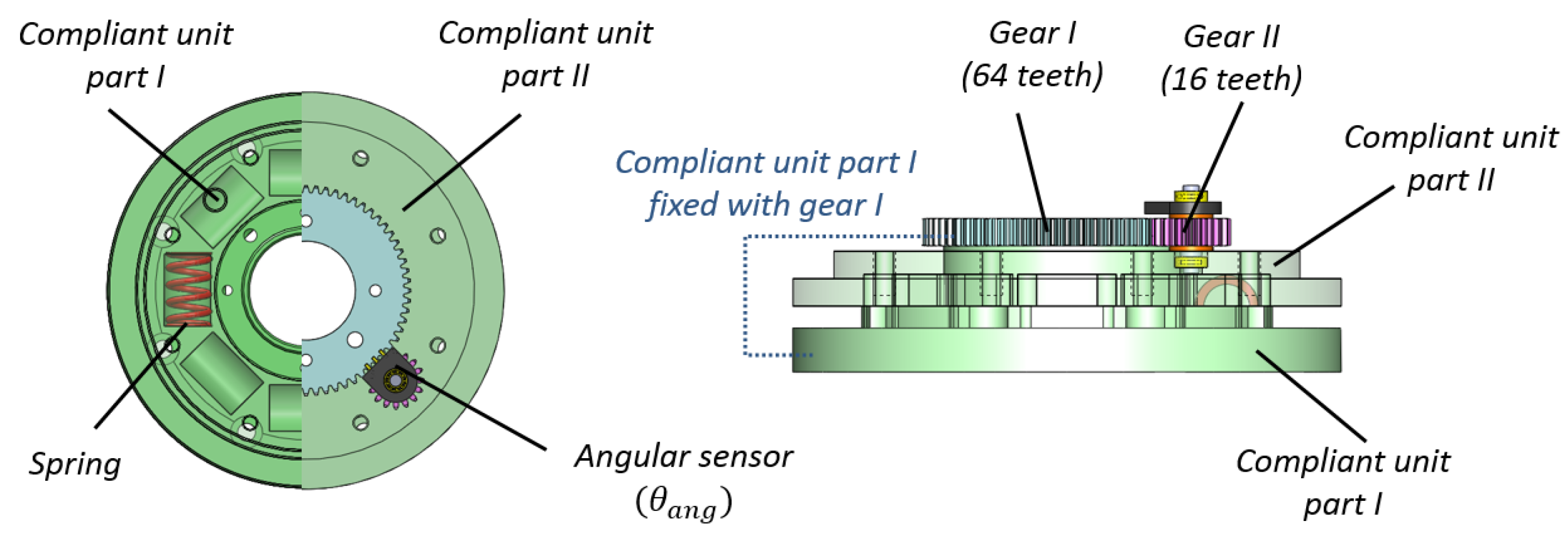
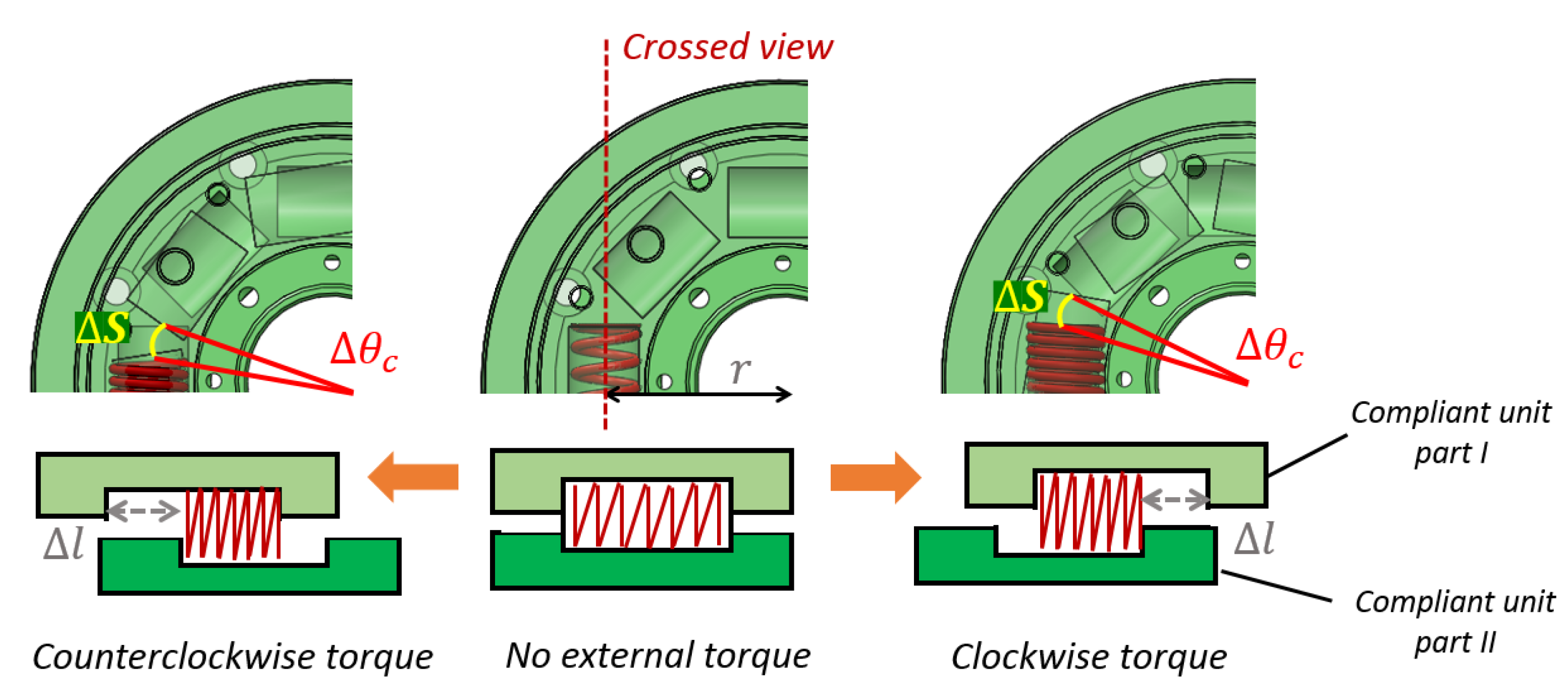
3.2.2. Compliant Unit
3.2.3. Measurement of External Torque
3.2.4. Measurement of Joint Torque
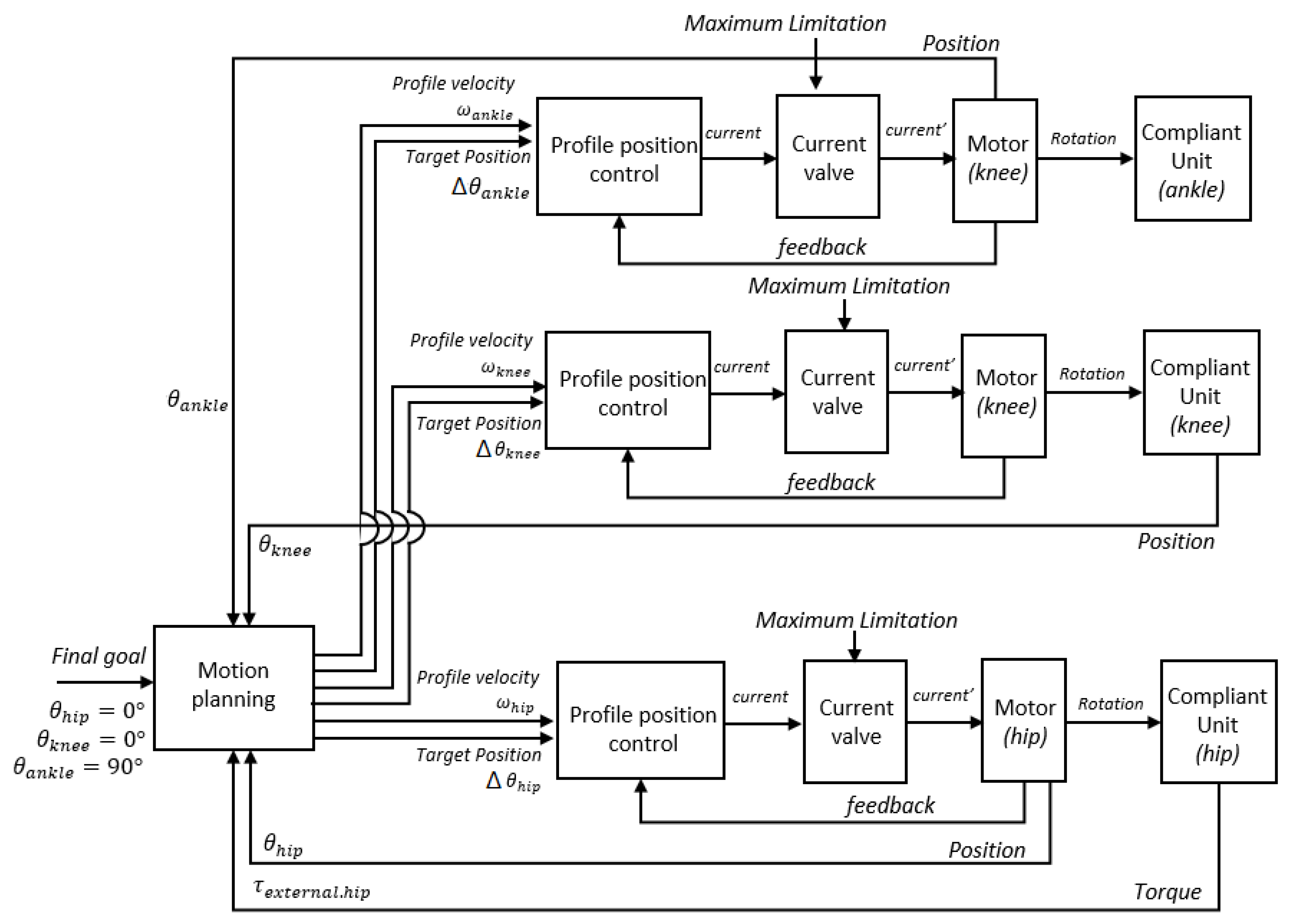
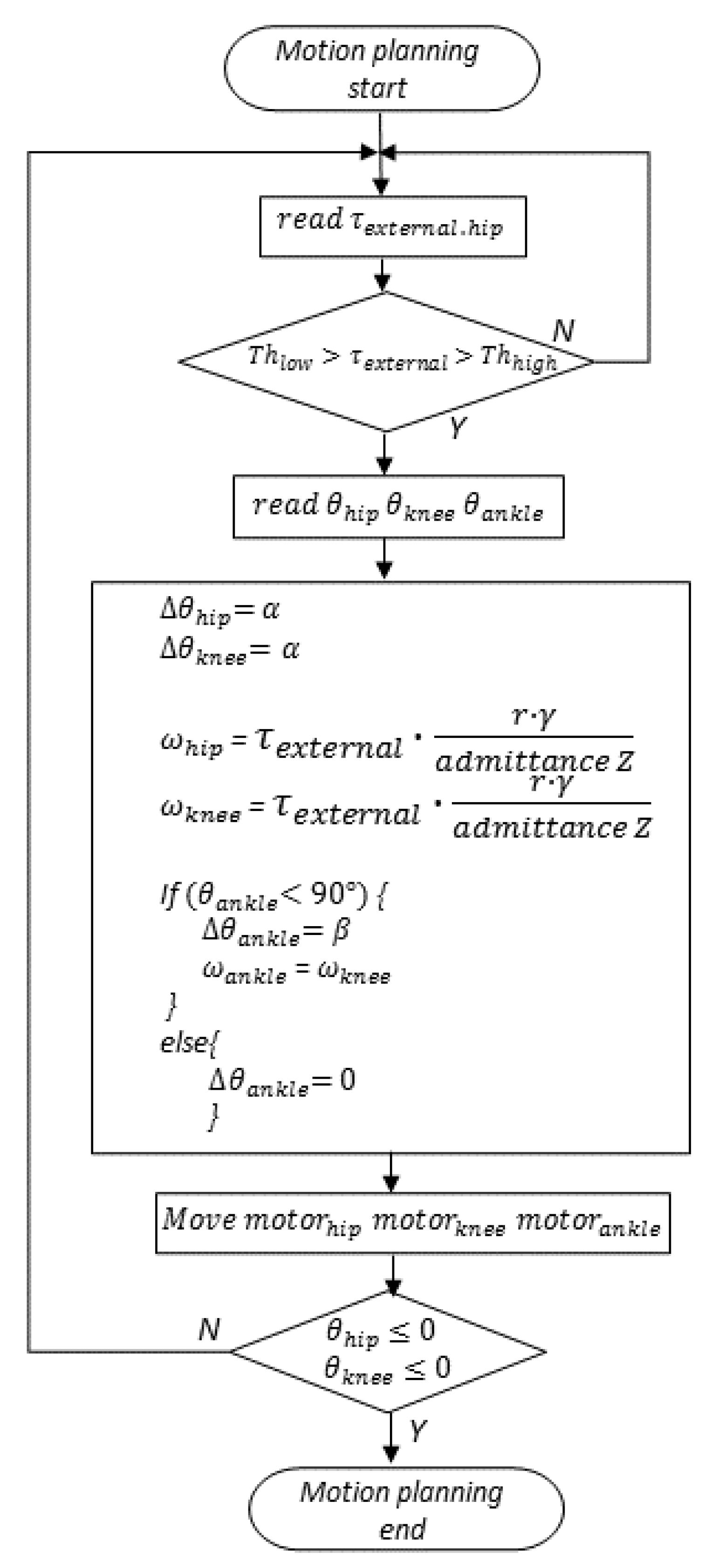
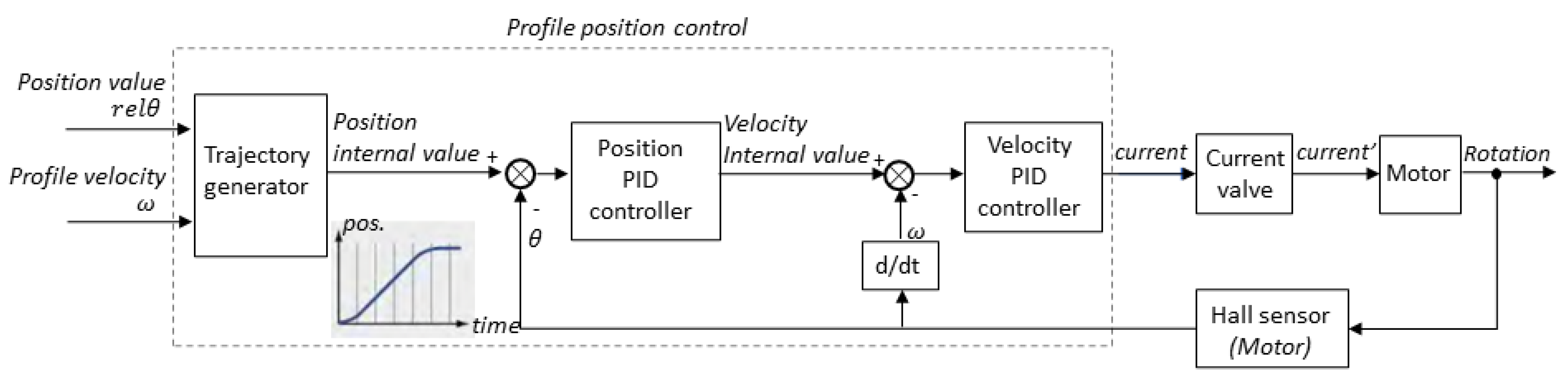
3.3. Control Method of STS Movement
4. Experiment
4.1. Purpose
4.2. Participants and Procedure
4.3. Experimental Setting
4.4. Analysis of the Two Phases of STS Movement
4.5. Result
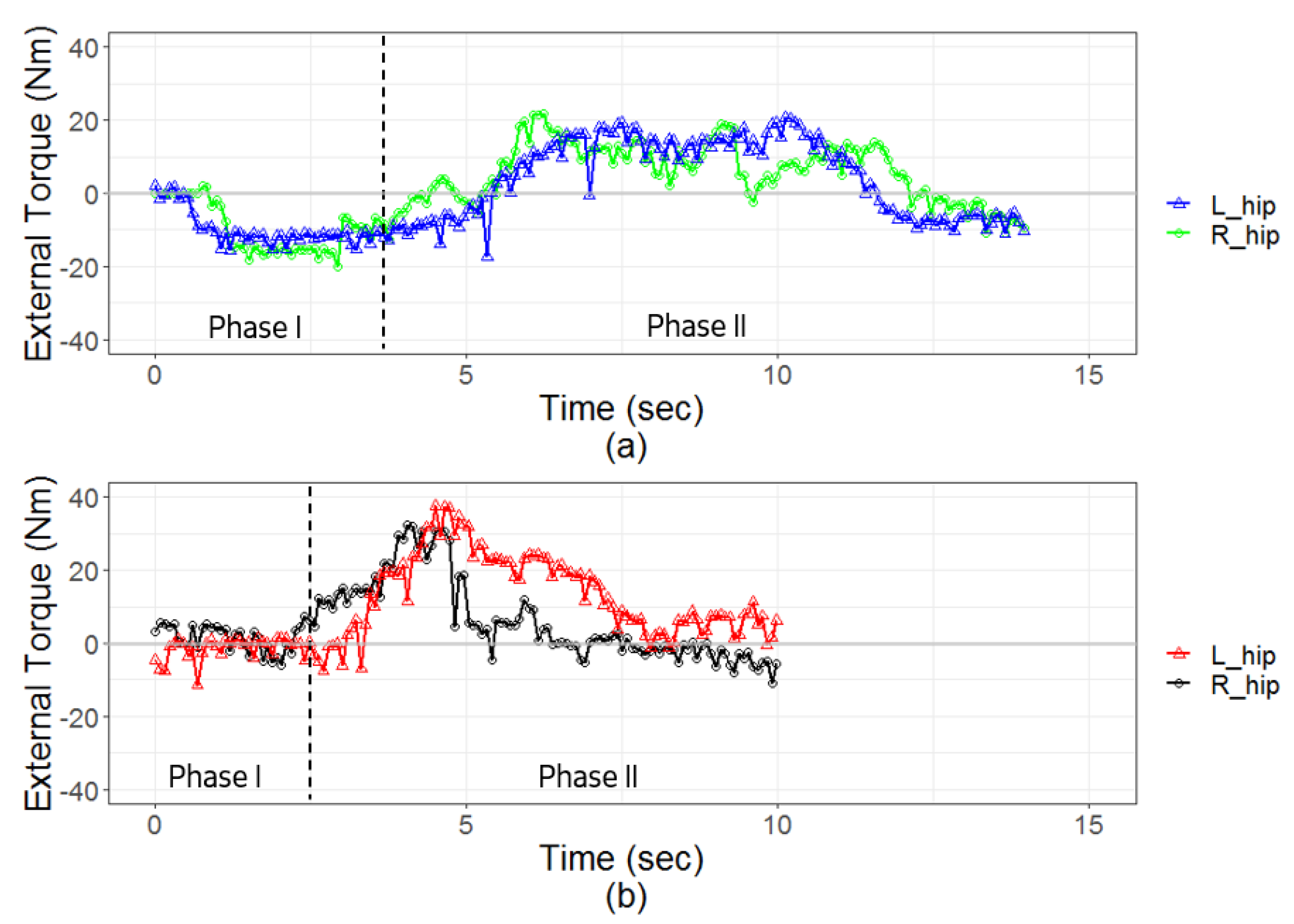
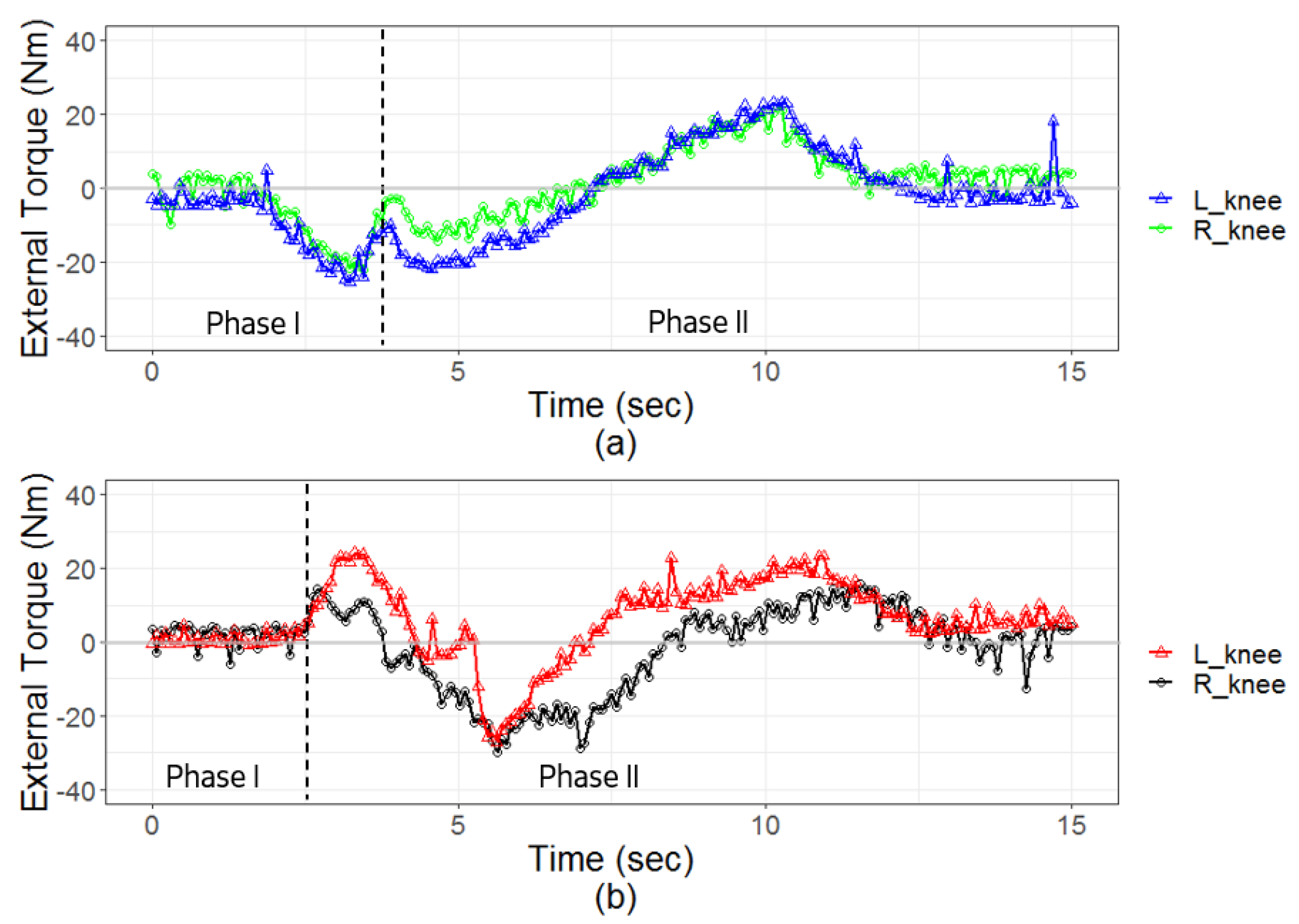
4.5.1. External Torque
4.5.2. Joint Torque
5. Discussion
5.1. External Torque
5.2. Joint Torque
6. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bell, J.T.; Tsai, P.C.; Yang, T.P.; Pidsley, R.; Nisbet, J.; Glass, D.; Mangino, M.; Zhai, G.; Zhang, F.; Valdes, A.; et al. Epigenome-wide scans identify differentially methylated regions for age and age-related phenotypes in a healthy ageing population. PLoS Genet. 2012, 8, e1002629. [Google Scholar] [CrossRef] [Green Version]
- Kjellberg, K.; Lagerström, M.; Hagberg, M. Patient safety and comfort during transfers in relation to nurses’ work technique. J. Adv. Nurs. 2004, 47, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Nardi, D.A.; Gyurko, C.C. The global nursing faculty shortage: Status and solutions for change. J. Nurs. Scholarsh. 2013, 45, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Kardong-Edgren, S.; Adamson, K.A.; Fitzgerald, C. A review of currently published evaluation instruments for human patient simulation. Clin. Simul. Nurs. 2010, 6, e25–e35. [Google Scholar] [CrossRef]
- Lin, C.; Kanai-Pak, M.; Maeda, J.; Kitajima, Y.; Nakamura, M.; Kuwahara, N.; Ogata, T.; Ota, J. Translational Acceleration, Rotational Speed, and Joint Angle of Patients Related to Correct/Incorrect Methods of Transfer Skills by Nurses. Sensors 2018, 18, 2975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peteani, L.A. Enhancing clinical practice and education with high-fidelity human patient simulators. Nurse Educ. 2004, 29, 25–30. [Google Scholar] [CrossRef]
- Park, H.S.; Kim, J.; Damiano, D.L. Development of a haptic elbow spasticity simulator (HESS) for improving accuracy and reliability of clinical assessment of spasticity. IEEE Trans. Neural Syst. Rehabil. Eng. 2012, 20, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, Y.; Komeda, T.; Koyama, H.; Yamamoto, S.I.; Arimatsu, T.; Kawakami, Y.; Inoue, K.; Ito, Y. Development of an upper limb patient simulator for physical therapy exercise. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–4. [Google Scholar]
- Che, D.; Zhang, W. GCUA humanoid robotic hand with tendon mechanisms and its upper limb. Int. J. Soc. Robot. 2011, 3, 395–404. [Google Scholar] [CrossRef]
- Marshall, R.L.; Smith, J.S.; Gorman, P.J.; Krummel, T.M.; Haluck, R.S.; Cooney, R.N. Use of a human patient simulator in the development of resident trauma management skills. J. Trauma Acute Care Surg. 2001, 51, 17–21. [Google Scholar] [CrossRef]
- Tanzawa, T.; Futaki, K.; Tani, C.; Hasegawa, T.; Yamamoto, M.; Miyazaki, T.; Maki, K. Introduction of a robot patient into dental education. Eur. J. Dent. Educ. 2012, 16, e195–e199. [Google Scholar] [CrossRef]
- Dang, T.; Annaswamy, T.M.; Srinivasan, M.A. Development and evaluation of an epidural injection simulator with force feedback for medical training. Stud. Health Technol. Inform. 2001, 97–102. [Google Scholar]
- Ogata, T.; Nagata, A.; Huang, Z.; Katayama, T.; Kanai-Pak, M.; Maeda, J.; Kitajima, Y.; Nakamura, M.; Aida, K.; Kuwahara, N.; et al. Mannequin system for the self-training of nurses in the changing of clothes. Kybernetes 2016, 45, 839–852. [Google Scholar] [CrossRef]
- Gerling, G.J.; Rigsbee, S.; Childress, R.M.; Martin, M.L. The design and evaluation of a computerized and physical simulator for training clinical prostate exams. IEEE Trans. Syst. Man Cybern.-Part A Syst. Hum. 2009, 39, 388–403. [Google Scholar] [CrossRef]
- Takashina, T.; Shimizu, M.; Katayama, H. A new cardiology patient simulator. Cardiology 1997, 88, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Noh, Y.; Segawa, M.; Sato, K.; Wang, C.; Ishii, H.; Solis, J.; Takanishi, A.; Katsumata, A.; Iida, Y. Development of a robot which can simulate swallowing of food boluses with various properties for the study of rehabilitation of swallowing disorders. In Proceedings of the 2011 IEEE International Conference on Robotics and Automation, Shanghai, China, 9–13 May 2011; pp. 4676–4681. [Google Scholar]
- Huang, Z.; Lin, C.; Kanai-Pak, M.; Maeda, J.; Kitajima, Y.; Nakamura, M.; Kuwahara, N.; Ogata, T.; Ota, J. Robot patient design to simulate various patients for transfer training. IEEE/ASME Trans. Mechatron. 2017, 22, 2079–2090. [Google Scholar] [CrossRef]
- Lin, C.; Zhong, Z.; Kanai-Pak, M.; Maeda, J.; Kitajima, Y.; Nakamura, M.; Kuwahara, N.; Ogata, T.; Ota, J. Development and Validation of Robot Patient Equipped with an Inertial Measurement Unit and Angular Position Sensors to Evaluate Transfer Skills of Nurses. Robot. Auton. Syst. 2020. [Google Scholar] [CrossRef]
- Akachi, K.; Kaneko, K.; Kanehira, N.; Ota, S.; Miyamori, G.; Hirata, M.; Kajita, S.; Kanehiro, F. Development of humanoid robot HRP-3P. In Proceedings of the 5th IEEE-RAS International Conference on Humanoid Robots, Tsukuba, Japan, 5 December 2005; pp. 50–55. [Google Scholar]
- Kanehiro, F.; Kaneko, K.; Fujiwara, K.; Harada, K.; Kajita, S.; Yokoi, K.; Hirukawa, H.; Akachi, K.; Isozumi, T. The first humanoid robot that has the same size as a human and that can lie down and get up. In Proceedings of the 2003 IEEE International Conference on Robotics and Automation (Cat. No. 03CH37422), Taipei, Taiwan, 14–19 September 2003; Volume 2, pp. 1633–1639. [Google Scholar]
- Kofinas, N. Forward and inverse kinematics for the NAO humanoid robot. Tech. Univ. Crete 2012. [Google Scholar]
- Vukobratovic, M.; Frank, A.A.; Juricic, D. On the stability of biped locomotion. IEEE Trans. Biomed. Eng. 1970, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, T.; Matsumoto, T.; Yoshiike, T. Real time motion generation and control for biped robot-1 st report: Walking gait pattern generation. In Proceedings of the 2009 IEEE/RSJ International Conference on Intelligent Robots and Systems, St. Louis, MO, USA, 10–15 October 2009; pp. 1084–1091. [Google Scholar]
- Sentis, L.; Park, J.; Khatib, O. Compliant control of multicontact and center-of-mass behaviors in humanoid robots. IEEE Trans. Robot. 2010, 26, 483–501. [Google Scholar] [CrossRef] [Green Version]
- Palmieri, R.M.; Ingersoll, C.D.; Stone, M.B.; Krause, B.A. Center-of-pressure parameters used in the assessment of postural control. J. Sport Rehabil. 2002, 11, 51–66. [Google Scholar] [CrossRef] [Green Version]
- Terada, K.; Ohmura, Y.; Kuniyoshi, Y. Analysis and control of whole body dynamic humanoid motion-towards experiments on a roll-and-rise motion. In Proceedings of the 2003 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS 2003)(Cat. No. 03CH37453), Las Vegas, NV, USA, 27–31 October 2003; Volume 2, pp. 1382–1387. [Google Scholar]
- Liu, C.; Atkeson, C.G. Standing balance control using a trajectory library. In Proceedings of the 2009 IEEE/RSJ International Conference on Intelligent Robots and Systems, St. Louis, MO, USA, 10–15 October 2009; pp. 3031–3036. [Google Scholar]
- Gong, Y.; Hartley, R.; Da, X.; Hereid, A.; Harib, O.; Huang, J.K.; Grizzle, J. Feedback control of a Cassie bipedal robot: Walking, standing, and riding a segway. In Proceedings of the 2019 American Control Conference (ACC), Philadelphia, PA, USA, 10–12 July 2019; pp. 4559–4566. [Google Scholar]
- Erez, T.; Lowrey, K.; Tassa, Y.; Kumar, V.; Kolev, S.; Todorov, E. An integrated system for real-time model predictive control of humanoid robots. In Proceedings of the 2013 13th IEEE-RAS International conference on humanoid robots (Humanoids), Atlanta, GA, USA, 15–17 October 2013; pp. 292–299. [Google Scholar]
- Morimoto, J.; Doya, K. Acquisition of stand-up behavior by a real robot using hierarchical reinforcement learning. Robot. Auton. Syst. 2001, 36, 37–51. [Google Scholar] [CrossRef]
- Anan, M.; Ibara, T.; Kito, N.; Shinkoda, K. The clarification of the strategy during sit-to-stand motion from the standpoint of mechanical energy transfer. J. Phys. Ther. Sci. 2012, 24, 231–236. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; Nagata, A.; Kanai-Pak, M.; Maeda, J.; Kitajima, Y.; Nakamura, M.; Aida, K.; Kuwahara, N.; Ogata, T.; Ota, J. Self-help training system for nursing students to learn patient transfer skills. IEEE Trans. Learn. Technol. 2014, 7, 319–332. [Google Scholar] [CrossRef]
- Kim, S.; Lee, S.; Kang, H.; Jeong, J. Study of knee and hip joints’ moment estimation by biomechanical simulation during various motion changes. In Proceedings of the World Congress on Engineering and Computer Science, San Francisco, CA, USA, 20–22 October 2009. [Google Scholar]
- Saadé, A.; Pudlo, P.; Lempereur, M.; Rémy-Néris, O. The contribution of handgrip assistance on lower limb joint moments during sit-to-stand and stand-to-sit: A preliminary comparative study. Comput. Methods Biomech. Biomed. Eng. 2014, 17, 102–103. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, S. Handrail position and shape that best facilitate sit-to-stand movement. J. Back Musculoskelet. Rehabil. 2012, 25, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Tsukahara, A.; Hasegawa, Y.; Sankai, Y. Standing-up motion support for paraplegic patient with Robot Suit HAL. In Proceedings of the 2009 IEEE International Conference on Rehabilitation Robotics, Kyoto, Japan, 23–26 June 2009; pp. 211–217. [Google Scholar]
- Matsumoto, H.; Ueki, M.; Uehara, K.; Noma, H.; Nozawa, N.; Osaki, M.; Hagino, H. Comparison of healthcare workers transferring patients using either conventional or robotic wheelchairs: Kinematic, electromyographic, and electrocardiographic analyses. J. Healthc. Eng. 2016, 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, A.; Lloyd, J.D.; Menzel, N.; Gross, C. Preventing nursing back injuries: Redesigning patient handling tasks. AAOHN J. 2003, 51, 126–134. [Google Scholar] [CrossRef] [Green Version]
- Keir, P.J.; MacDonell, C.W. Muscle activity during patient transfers: A preliminary study on the influence of lift assists and experience. Ergonomics 2004, 47, 296–306. [Google Scholar] [CrossRef]
- Nadon, A.L.; Cudlip, A.C.; Dickerson, C.R. Joint moment loading interplay between the shoulders and the low back during patient handling in nurses. Occup. Ergon. 2017, 13, 81–90. [Google Scholar] [CrossRef] [Green Version]
- Ott, C.; Mukherjee, R.; Nakamura, Y. Unified impedance and admittance control. In Proceedings of the 2010 IEEE International Conference on Robotics and Automation, Anchorage, AK, USA, 3–7 May 2010; pp. 554–561. [Google Scholar]
- Hatze, H. The meaning of the term “biomechanics”. J. Biomech. 1974, 7, 189. [Google Scholar] [CrossRef]
- Yoshioka, S.; Nagano, A.; Himeno, R.; Fukashiro, S. Computation of the kinematics and the minimum peak joint moments of sit-to-stand movements. Biomed. Eng. Online 2007, 6, 26. [Google Scholar] [CrossRef] [Green Version]
- Luttgens, K.; Hamilton, N.; Deutsch, H. Kinesiology: Scientific Basis of Human Motion; Brown & Benchmark: Madison, WI, USA, 1997. [Google Scholar]
- Cholewicki, J.; Simons, A.P.; Radebold, A. Effects of external trunk loads on lumbar spine stability. J. Biomech. 2000, 33, 1377–1385. [Google Scholar] [CrossRef]
- NASA. (ST-E-1321) Japanese Female Body Size. National Space Deopment Agency of Japan. Man-Syst. Integr. Stand. 2000, 06–05–86. Available online: https://msis.jsc.nasa.gov/sections/section03.htm (accessed on 7 January 2021).
- Associates, W.; Springs, Y.; Project, O.A.R. Anthropometric Source Book; National Aeronautics and Space Administration, Scientific and Technical Information Office: Washington, DC, USA, 1978; Volume 2. [Google Scholar]
- Ham, R.V.; Sugar, T.; Vanderborght, B.; Hollander, K.; Lefeber, D. Compliant actuator designs. IEEE Robot. Autom. Mag. 2009, 3, 81–94. [Google Scholar] [CrossRef]
- Pratt, G.A.; Williamson, M.M. Series elastic actuators. In Proceedings of the 1995 IEEE/RSJ International Conference on Intelligent Robots and Systems. Human Robot Interaction and Cooperative Robots, Pittsburgh, PA, USA, 5–9 August 1995; Volume 1, pp. 399–406. [Google Scholar]
- Robinson, D.W. Design and Analysis of Series Elasticity in Closed-Loop Actuator Force Control. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 2000. [Google Scholar]
- Tsagarakis, N.G.; Laffranchi, M.; Vanderborght, B.; Caldwell, D.G. A compact soft actuator unit for small scale human friendly robots. In Proceedings of the 2009 IEEE International Conference on Robotics and Automation, Kobe, Japan, 12–17 May 2009; pp. 4356–4362. [Google Scholar]
- Keemink, A.Q.; van der Kooij, H.; Stienen, A.H. Admittance control for physical human–robot interaction. Int. J. Robot. Res. 2018, 37, 1421–1444. [Google Scholar] [CrossRef] [Green Version]
- Mizner, R.L.; Snyder-Mackler, L. Altered loading during walking and sit-to-stand is affected by quadriceps weakness after total knee arthroplasty. J. Orthop. Res. 2005, 23, 1083–1090. [Google Scholar] [CrossRef]
- Jun, H.G.; Chang, Y.Y.; Dan, B.J.; Jo, B.R.; Min, B.H.; Yang, H.; Song, W.K.; Kim, J. Walking and sit-to-stand support system for elderly and disabled. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–5. [Google Scholar]
- Etnyre, B.; Thomas, D.Q. Event standardization of sit-to-stand movements. Phys. Ther. 2007, 87, 1651–1666. [Google Scholar] [CrossRef] [PubMed]
- Mak, M.K.; Levin, O.; Mizrahi, J.; Hui-Chan, C.W. Joint torques during sit-to-stand in healthy subjects and people with Parkinson’s disease. Clin. Biomech. 2003, 18, 197–206. [Google Scholar] [CrossRef]
- Yamada, T.; Demura, S.I. Relationships between ground reaction force parameters during a sit-to-stand movement and physical activity and falling risk of the elderly and a comparison of the movement characteristics between the young and the elderly. Arch. Gerontol. Geriatr. 2009, 48, 73–77. [Google Scholar] [CrossRef] [PubMed]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Content |
|---|---|
| Measurement of external torque | Range: 0.98–39.2 Nm |
| Admittance value | Z = 1.74 Nm · (/s). |
| Required torque during sit-to-stand movement | Hip joint: 19.6 Nm Knee joint: 35.2 Nm Ankle joint: 24.9 Nm |
| Range of movement | Hip joint: 0–120 Knee joint: 0–150 Ankle joint: 70–120 |
| Stiffness | Hip joint: 216–266 N·m/rad |
| Arm Joint | Waist Joint | Hip & Knee Joint | Ankle Joint | |
|---|---|---|---|---|
| Torque (Nm) | 2.74 | 52 | 45.8 | 36.64 |
| Voltage (V) | 7.2 | 30 | 30 | 30 |
| Motor | Futaba RC405CB | Moog Animatics SM23165DT | Maxon EC frameless 543673 | Maxon EC frameless 543673 |
| Reduction gear | — | Harmonic driver CSD-20-100-2UP | TPI TSH-25-100-HST | TPI TSH-25-80-HST |
| Reduction ratio | — | 100:1 | 100:1 | 80:1 |
| Correct | Incorrect | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Phase | Value | p-Value | ||||||||
| Teacher A | Teacher B | Teacher C | Teacher D | Teacher A | Teacher B | Teacher C | Teacher D | |||
| I | *min. hip joint external torque | -21.30 | −21.86 | −25.12 | −16.68 | −4.47 | −5.65 | −2.34 | −1.52 | 0.002 |
| *min. knee joint external torque | −26.08 | −27.40 | −22.00 | −21.21 | −3.80 | −3.77 | −7.20 | −1.41 | 0.002 | |
| *min. ankle joint external torque | −30.07 | −22.87 | −20.85 | −39.89 | −2.17 | −2.08 | −1.10 | −4.02 | 0.006 | |
| *average hip joint external torque | −5.39 | −7.74 | −9.05 | 2.30 | 3.37 | 0.35 | 2.60 | 5.20 | 0.023 | |
| *average knee joint external torque | −6.94 | −6.94 | −6.22 | −0.82 | 0.69 | 2.39 | −0.82 | 1.02 | 0.033 | |
| *average ankle joint external torque | −6.55 | −5.12 | −5.31 | −0.30 | 2.08 | 2.40 | 2.64 | 0.24 | 0.047 | |
| II | *max. hip joint external torque | 24.00 | 18.40 | 20.90 | 23.83 | 37.56 | 27.04 | 36.24 | 27.66 | 0.028 |
| max. knee joint external torque | 20.37 | 21.58 | 20.00 | 36.43 | 17.22 | 27.18 | 28.67 | 40.01 | 0.238 | |
| *min. ankle joint external torque | −36.9 | −33.36 | −35.7 | −46.13 | −14.17 | −16.59 | −30.04 | −30.55 | 0.023 | |
| *average hip joint external torque | 5.14 | 3.51 | 2.42 | 8.49 | 11.49 | 6.62 | 9.73 | 10.47 | 0.034 | |
| average knee joint external torque | 2.12 | 4.01 | −0.12 | 31.87 | −4.32 | 5.26 | −4.99 | 16.02 | 0.164 | |
| *average ankle joint external torque | −30.24 | −24.13 | −19.96 | −35.54 | −3.04 | −7.03 | −12.04 | −11.00 | 0.021 | |
| Correct | Incorrect | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Phase | Value | p-Value | ||||||||
| Teacher A | Teacher B | Teacher C | Teacher D | Teacher A | Teacher B | Teacher C | Teacher D | |||
| I | *average hip joint torque | −8.58 | −5.73 | −4.37 | −3.34 | 13.74 | 12.06 | 7.33 | 13.72 | 0.004 |
| *average knee joint torque | −14.94 | −10.86 | −7.74 | −9.89 | 16.94 | 11.96 | 2.26 | 11.74 | 0.017 | |
| *average ankle joint torque | −10.08 | −7.60 | −6.71 | −5.25 | −0.005 | −0.001 | −0.003 | −0.003 | 0.005 | |
| II | *average hip joint torque | 15.49 | 16.94 | 17.94 | 14.17 | 17.70 | 21.94 | 19.94 | 20.19 | 0.032 |
| *average knee joint torque | 12.62 | 9.43 | 11.99 | 11.38 | 15.62 | 15.00 | 13.25 | 16.20 | 0.032 | |
| *average ankle joint torque | 1.64 | 1.37 | 1.832 | 1.29 | −0.003 | −0.008 | 0.353 | −0.001 | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.; Ogata, T.; Zhong, Z.; Kanai-Pak, M.; Maeda, J.; Kitajima, Y.; Nakamura, M.; Kuwahara, N.; Ota, J. Development of Robot Patient Lower Limbs to Reproduce the Sit-to-Stand Movement with Correct and Incorrect Applications of Transfer Skills by Nurses. Appl. Sci. 2021, 11, 2872. https://doi.org/10.3390/app11062872
Lin C, Ogata T, Zhong Z, Kanai-Pak M, Maeda J, Kitajima Y, Nakamura M, Kuwahara N, Ota J. Development of Robot Patient Lower Limbs to Reproduce the Sit-to-Stand Movement with Correct and Incorrect Applications of Transfer Skills by Nurses. Applied Sciences. 2021; 11(6):2872. https://doi.org/10.3390/app11062872
Chicago/Turabian StyleLin, Chingszu, Taiki Ogata, Zhihang Zhong, Masako Kanai-Pak, Jukai Maeda, Yasuko Kitajima, Mitsuhiro Nakamura, Noriaki Kuwahara, and Jun Ota. 2021. "Development of Robot Patient Lower Limbs to Reproduce the Sit-to-Stand Movement with Correct and Incorrect Applications of Transfer Skills by Nurses" Applied Sciences 11, no. 6: 2872. https://doi.org/10.3390/app11062872