
Foot Contact Dynamics and Fall Risk among Children Diagnosed with Idiopathic Toe Walking

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Kinetic Data Analysis
3.2. Gait Assessments
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Sobel, E.; Caselli, M.; Velez, Z. Effect of persistent toe walking on ankle equinus. Analysis of 60 idiopathic toe walkers. J. Am. Podiatr. Med. Assoc. 1997, 87, 17–22. [Google Scholar] [CrossRef]
- Sutherland, D.H.; Olshen, R.; Cooper, L.; Woo, S.L. The development of mature gait. J. Bone Jt. Surg. Am. 1980, 62, 336–353. [Google Scholar] [CrossRef] [Green Version]
- Fox, A.; Deakin, S.; Pettigrew, G.; Paton, R. Serial casting in the treatment of idiopathic toe-walkers and review of the literature. Acta Orthop. Belg. 2006, 72, 722–730. [Google Scholar]
- Hirsch, G.; Wagner, B. The natural history of idiopathic toe-walking: A long-term follow-up of fourteen conservatively treated children. Acta Paediatr. 2004, 93, 196–199. [Google Scholar] [CrossRef]
- Tabrizi, P.; McIntyre, W.M.J.; Quesnel, M.B.; Howard, A.W. Limited dorsiflexion predisposes to injuries of the ankle in children. J. Bone Jt. Surg. Br. 2000, 82, 1103–1106. [Google Scholar] [CrossRef]
- Tardieu, C.; Lespargot, A.; Tabary, C.; Bret, M.D. Toe-walking in children with cerebral palsy: Contributions of contracture and excessive contraction of triceps surae muscle. Phys. Ther. 1989, 69, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Gross, R.; Leboeuf, F.; Hardouin, J.B.; Perrouin-Verbe, B.; Brochard, S.; Rémy-Néris, O. Does muscle coactivation influence joint excursions during gait in children with and without hemiplegic cerebral palsy? Relationship between muscle coactivation and joint kinematics. Clin. Biomech. 2015, 30, 1088–1093. [Google Scholar] [CrossRef]
- Kedem, P.; Scher, D.M. Foot deformities in children with cerebral palsy. Curr. Opin. Pediatr. 2015, 27, 67–74. [Google Scholar] [CrossRef]
- Edwards, W.B. Modeling overuse injuries in sport as a mechanical fatigue phenomenon. Exerc. Sport Sci. Rev. 2018, 46, 224–231. [Google Scholar] [CrossRef]
- Chao, E.; Laughman, R.; Schneider, E.; Stauffer, R. Normative data of knee joint motion and ground reaction forces in adult level walking. J. Biomech. 1983, 16, 219–233. [Google Scholar] [CrossRef]
- Rodda, J.M.; Graham, H.K.; Carson, L.; Galea, M.P.; Wolfe, R. Sagittal gait patterns in spastic diplegia. J. Bone Jt. Surg. Br. 2004, 86, 251–258. [Google Scholar] [CrossRef]
- Winters, T.F., Jr.; Gage, J.R.; Hicks, R. Gait patterns in spastic hemiplegia in children and young adults. J. Bone Jt. Surg. Am. 1987, 69, 437–441. [Google Scholar]
- Lin, C.-J.; Guo, L.-Y.; Su, F.-C.; Chou, Y.-L.; Cherng, R.-J. Common abnormal kinetic patterns of the knee in gait in spastic diplegia of cerebral palsy. Gait Posture 2000, 11, 224–232. [Google Scholar] [CrossRef]
- Armand, S.; Watelain, E.; Mercier, M.; Lensel, G.; Lepoutre, F.-X. Identification and classification of toe-walkers based on ankle kinematics, using a data-mining method. Gait Posture 2006, 23, 240–248. [Google Scholar] [CrossRef]
- Davids, J.R.; Foti, T.; Dabelstein, J.; Bagley, A. Voluntary (normal) versus obligatory (cerebral palsy) toe-walking in children: A kinematic, kinetic, and electromyographic analysis. J. Pediatr. Orthop. 1999, 19, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Hicks, R.; Durinick, N.; Gage, J.R. Differentiation of idiopathic toe-walking and cerebral palsy. J. Pediatr. Orthop. 1988, 8, 160–163. [Google Scholar] [CrossRef]
- Chu, V.; Anderson, L. Sensory-processing differences in children with idiopathic toe walking (ITW). Am. J. Occup. Ther. 2020, 74, 7411505130. [Google Scholar] [CrossRef]
- Williams, C.M.; Tinley, P.; Curtin, M. Idiopathic toe walking and sensory processing dysfunction. J. Foot Ankle Res. 2010, 3, 16. [Google Scholar] [CrossRef] [Green Version]
- Berger, W.; Quintern, J.; Dietz, V. Pathophysiology of gait in children with cerebral palsy. Electroencephalogr. Clin. Neurophysiol. 1982, 53, 538–548. [Google Scholar] [CrossRef]
- Gough, M.; Shortland, A.P. Could muscle deformity in children with spastic cerebral palsy be related to an impairment of muscle growth and altered adaptation? Dev. Med. Child Neurol. 2012, 54, 495–499. [Google Scholar] [CrossRef] [Green Version]
- Willerslev-Olsen, M.; Andersen, J.B.; Sinkjaer, T.; Nielsen, J.B. Sensory feedback to ankle plantar flexors is not exaggerated during gait in spastic hemiplegic children with cerebral palsy. J. Neurophysiol. 2014, 111, 746–754. [Google Scholar] [CrossRef] [Green Version]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—part I: Ankle, hip, and spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Grood, E.S.; Suntay, W.J. A joint coordinate system for the clinical description of three-dimensional motions: Application to the knee. J. Biomech. Eng. 1983, 105, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A. Biomechanics and Motor Control of Human Movement, 4th ed.; Wiley: Hoboken, NJ, USA, 2009. [Google Scholar]
- Lockhart, T.E.; Kim, S. Relationship between hamstring activation rate and heel contact velocity: Factors influencing age-related slip-induced falls. Gait Posture 2006, 24, 23–34. [Google Scholar] [CrossRef] [Green Version]
- Barrett, R.; Mills, P.; Begg, R. A systematic review of the effect of ageing and falls history on minimum foot clearance characteristics during level walking. Gait Posture 2010, 32, 429–435. [Google Scholar] [CrossRef]
- Khandoker, A.H.; Lynch, K.; Karmakar, C.K.; Begg, R.K.; Palaniswami, M. Regulation of minimum toe clearance variability in the young and elderly during walking on sloped surfaces. In Proceedings of the 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 23–26 August 2007; pp. 4887–4890. [Google Scholar]
- Murray, M.P.; Clarkson, B.H. The vertical pathways of the foot during level walking. I. Range of variability in normal men. Phys. Ther. 1966, 46, 585–589. [Google Scholar] [CrossRef]
- Nagano, H.; Begg, R.; Sparrow, W.A. Computation method for available response time due to tripping at minimum foot clearance. In Proceedings of the 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 4899–4902. [Google Scholar] [CrossRef]
- Hollman, J.H.; McDade, E.M.; Petersen, R.C. Normative spatiotemporal gait parameters in older adults. Gait Posture 2011, 34, 111–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lockhart, T.E.; Woldstad, J.C.; Smith, J.L. Effects of age-related gait changes on the biomechanics of slips and falls. Ergonomics 2003, 46, 1136–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollind, M.; Soangra, R.; Grant-Beuttler, M.; Aminian, A. Customized wearable sensor-based insoles for gait re-training in idiopathic toe walkers. Biomed. Sci. Instrum. 2019, 55, 192–198. [Google Scholar]
- Kim, S.; Soangra, R.; Grant-Beuttler, M.; Aminian, A. Wearable sensor-based gait classification in idiopathic toe walking adolescents. Biomed. Sci. Instrum. 2019, 55, 178–185. [Google Scholar]
- Sala, D.A.; Shulman, L.H.; Kennedy, R.F.; Grant, A.D.; Chu, M.L. Idiopathic toe-walking: A review. Dev. Med. Child. Neurol. 1999, 41, 846–848. [Google Scholar] [CrossRef] [PubMed]
- A Caselli, M.; Rzonca, E.C.; Lue, B.Y. Habitual toe-walking: Evaluation and approach to treatment. Clin. Podiatr. Med. Surg. 1988, 5, 547–559. [Google Scholar]
- Eastwood, D.M.; Dennett, X.; Shield, L.K.; Dickens, D.R.V. Muscle abnormalities in idiopathic toe-walkers. J. Pediatr. Orthop. B 1997, 6, 215–218. [Google Scholar] [CrossRef]
- Rose, J.; Martin, J.G.; Torburn, L.; Rinsky, L.A.; Gamble, J.G. Electromyographic differentiation of diplegic cerebral palsy from idiopathic toe walking: Involuntary coactivation of the quadriceps and gastrocnemius. J. Pediatr. Orthop. 1999, 19, 677–682. [Google Scholar] [CrossRef]
- Policy, J.F.; Torburn, L.; Rinsky, L.A.; Rose, J. Electromyographic test to differentiate mild diplegic cerebral palsy and idiopathic toe-walking. J. Pediatr. Orthop. 2001, 21, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Kelly, I.P.; Jenkinson, A.; Stephens, M.; O’Brien, T. The kinematic patterns of toe-walkers. J. Pediatr. Orthop. 1997, 17, 478–480. [Google Scholar] [CrossRef]
- Choi, H.S.; Baek, Y.S. Effects of the degree of freedom and assistance characteristics of powered ankle-foot orthoses on gait stability. PLoS ONE 2020, 15, e0242000. [Google Scholar] [CrossRef]
- Chen, S.K.; Voaklander, D.; Perry, D.; Jones, C.A. Falls and fear of falling in older adults with total joint arthroplasty: A scoping review. BMC Musculoskelet Disord. 2019, 20, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Allet, L.; Ijzerman, H.; Meijer, K.; Willems, P.; Savelberg, H. The influence of stride-length on plantar foot-pressures and joint moments. Gait Posture 2011, 34, 300–306. [Google Scholar] [CrossRef] [Green Version]
- Cleland, C.L.; Hayward, L.; Rymer, W.Z. Neural mechanisms underlying the clasp-knife reflex in the cat. II. Stretch-sensitive muscular-free nerve endings. J. Neurophysiol. 1990, 64, 1319–1330. [Google Scholar] [CrossRef]
- Cleland, C.L.; Rymer, W.Z.; Edwards, F.R.; Gabrielli, B.; Roy, L.; Maller, J. Force-sensitive interneurons in the spinal cord of the cat. Science 1982, 217, 652–655. [Google Scholar] [CrossRef] [PubMed]
- Rymer, W.Z.; Houk, J.C.; Crago, P.E. Mechanisms of the clasp-knife reflex studied in an animal model. Exp. Brain Res. 1979, 37, 93–113. [Google Scholar] [CrossRef] [PubMed]
- Duysens, J.; Clarac, F.; Cruse, H. Load-regulating mechanisms in gait and posture: Comparative aspects. Physiol. Rev. 2000, 80, 83–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neptune, R.R.; Burnfield, J.M.; Mulroy, S.J. The neuromuscular demands of toe walking: A forward dynamics simulation analysis. J. Biomech. 2007, 40, 1293–1300. [Google Scholar] [CrossRef] [PubMed]
- Gravel, D.; Richards, C.L.; Filion, M. Influence of contractile tension development on dynamic strength measurements of the plantarflexors in man. J. Biomech. 1988, 21, 89–96. [Google Scholar] [CrossRef]
- Nistor, L.; Markhede, G.; Grimby, G. A technique for measurements of plantar flexion torque with the Cybex II dynamometer. Scand. J. Rehabil. Med. 1982, 14, 163–166. [Google Scholar]
- Sale, D.; Quinlan, J.; Marsh, E.; McComas, A.J.; Bélanger, A.Y. Influence of joint position on ankle plantarflexion in humans. J. Appl. Physiol. 1982, 52, 1636–1642. [Google Scholar] [CrossRef]
- Rugg, S.; Gregor, R.; Mandelbaum, B.; Chiu, L. In vivo moment arm calculations at the ankle using magnetic resonance imaging (MRI). J. Biomech. 1990, 23, 495–501. [Google Scholar] [CrossRef]
- Rosenblatt, N.J.; Bauer, A.; Grabiner, M.D. Relating minimum toe clearance to prospective, self-reported, trip-related stumbles in the community. Prosthetics Orthot. Int. 2017, 41, 387–392. [Google Scholar] [CrossRef]
- Killeen, T.; Easthope, C.S.; Demkó, L.; Filli, L.; Lőrincz, L.; Linnebank, M.; Curt, A.; Zörner, B.; Bolliger, M. Minimum toe clearance: Probing the neural control of locomotion. Sci. Rep. 2017, 7, 1922. [Google Scholar] [CrossRef] [Green Version]
- Lockhart, T.E.; Woldstad, J.C.; Smith, J.L. Relationship between transitional acceleration of the whole body center-of-mass and friction demand characteristic during gait. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, Baltimore, MD, USA, 29 September–4 October 2002; SAGE Publications: Thousand Oaks, CA, USA, 2002; Volume 46, pp. 1186–1190. [Google Scholar]
- Kim, S.; Lockhart, T.; Yoon, H.-Y. Relationship between age-related gait adaptations and required coefficient of friction. Saf. Sci. 2005, 43, 425–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | ITW | |||
|---|---|---|---|---|
| Angles [Degrees] | Toe Walking | Typical Walking | Toe Walking | Typical Walking |
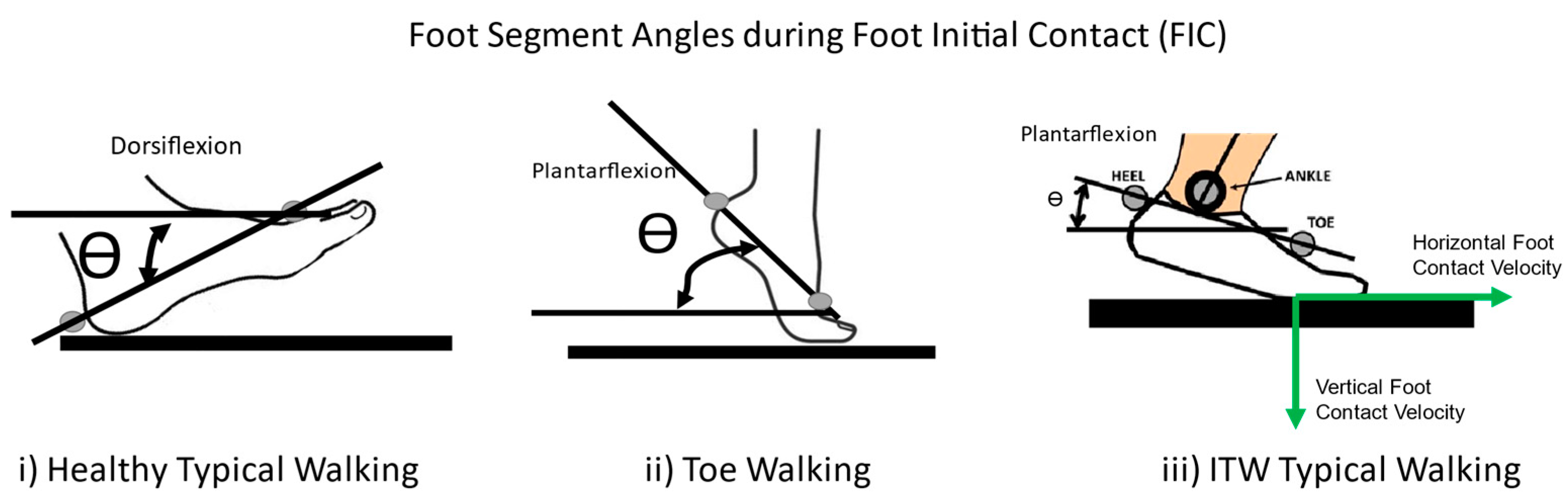
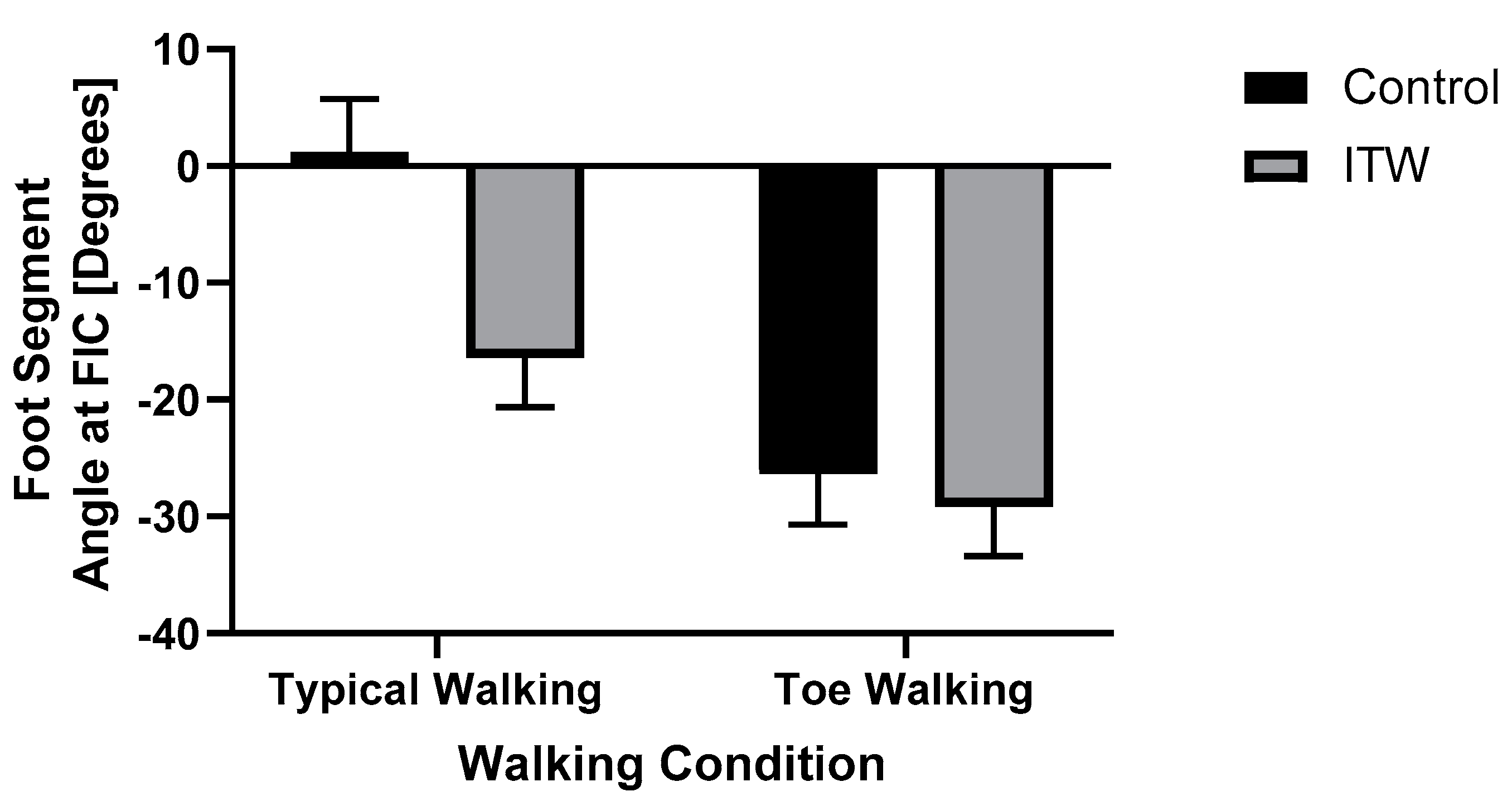
| Foot angle at FIC | −26.0 ± 17.1 | 1.6 ± 23.8 | −29.1 ± 17.5 | −16.3 ± 24.1 |
| Foot angle at Foot Off (FO) | −43.2 ± 36.0 | −41.1 ± 37.8 | −47.2 ± 35.0 | −34.0 ± 35.2 |
| Ankle angle at Loading | −19.2 ± 16.9 | −9.1 ± 13.4 | −24.5 ± 16.6 | −15.6 ± 12.7 |
| Ankle angle at Midstance | −16.4 ± 8.7 | 3.7 ± 6.2 | −22.8 ± 8.0 | −6.2 ± 10.9 |
| Ankle angle at Push−off | −25.8 ± 12.0 | 4.6 ± 8.8 | −27.7 ± 9.1 | −4.0 ± 11.5 |
| Knee angle at Loading | 25.2 ± 12.8 | 32.0 ± 14.2 | 25.5 ± 9.7 | 31.9 ± 16.4 |
| Knee angle at Midstance | 28.8 ± 23.0 | 30.2 ± 23.9 | 30.1 ± 23.3 | 38.5 ± 28.0 |
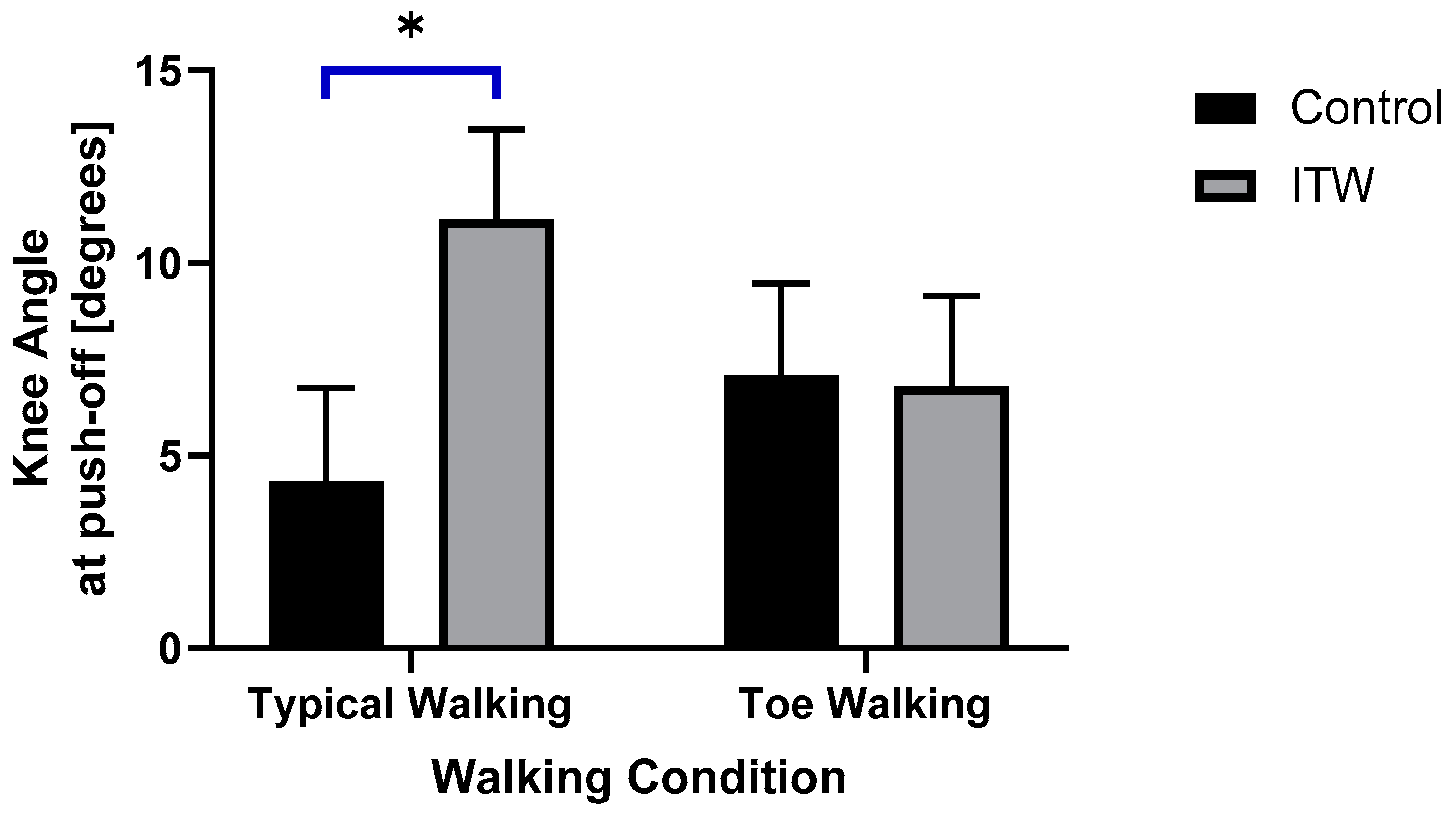
| Knee angle at Push−off * | 6.6 ± 13.0 | 4.1 ± 7.8 | 6.8 ± 8.9 | 11.1 ± 9.8 |
| Hip angle at Loading | 23.0 ± 36.6 | 24.7 ± 20.3 | 26.4 ± 22.9 | 25.2 ± 26.2 |
| Hip angle at Midstance | 19.3 ± 41.5 | 24.9 ± 16.0 | 28.9 ± 34.9 | 33.1 ± 20.3 |
| Hip angle at Push−off | 14.1 ± 39.4 | 14.1 ± 22.7 | 19.2 ± 39.9 | 28.2 ± 23.8 |
| Control | ITW | |||
|---|---|---|---|---|
| Toe Walking | Typical Walking | Toe Walking | Typical Walking | |
| Stride Length * [mm] | 921.4 ± 197.5 | 1066.0 ± 237.1 | 980.5 ± 169.3 | 911.2 ± 145.1 |
| Stride Time [s] | 0.8 ± 0.1 | 0.9 ± 0.1 | 0.8 ± 0.07 | 0.9 ± 0.1 |
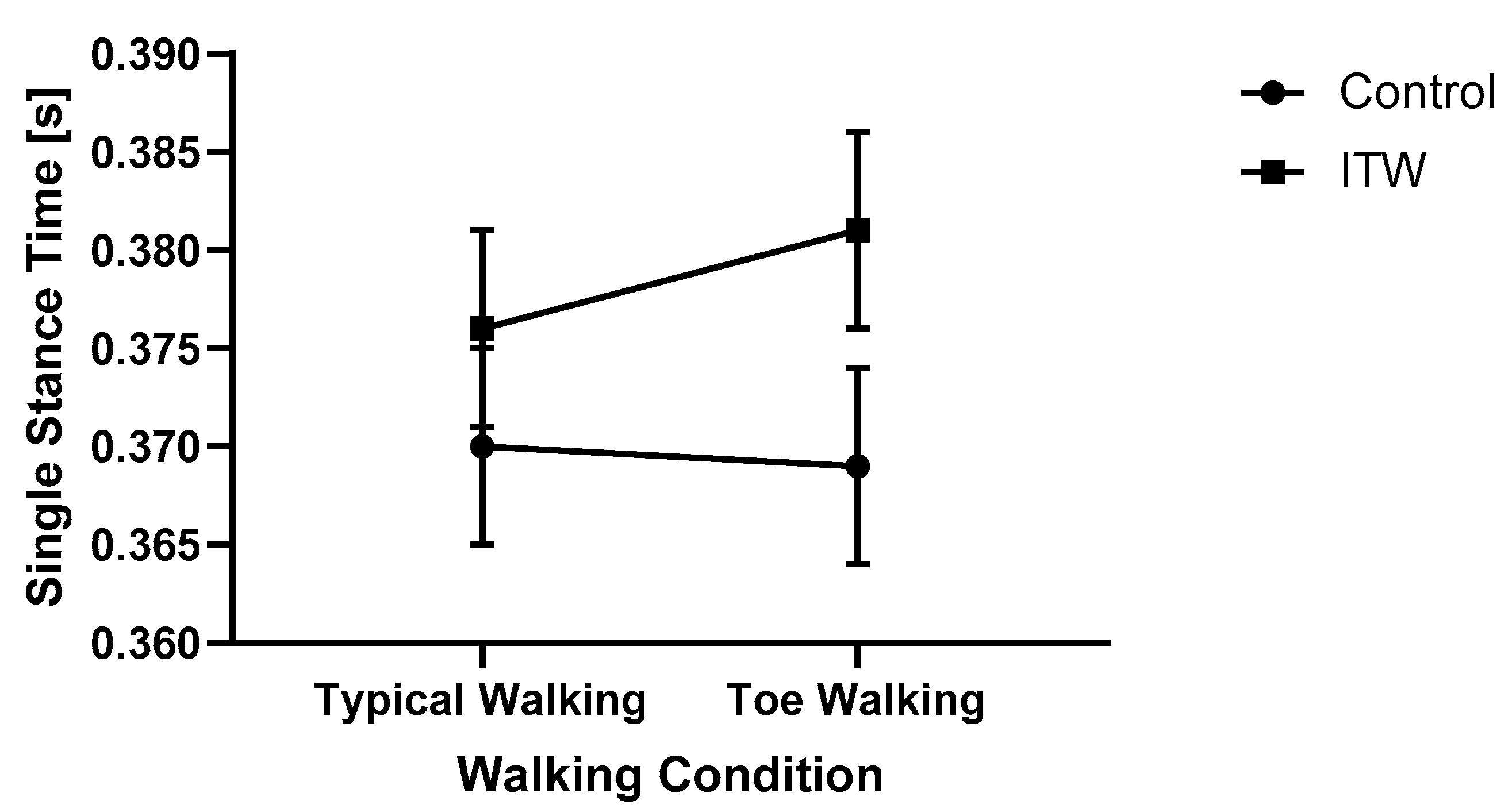
| Single Stance Duration [s] | 0.3 ± 0.03 | 0.3 ± 0.01 | 0.3 ± 0.01 | 0.3 ± 0.03 |
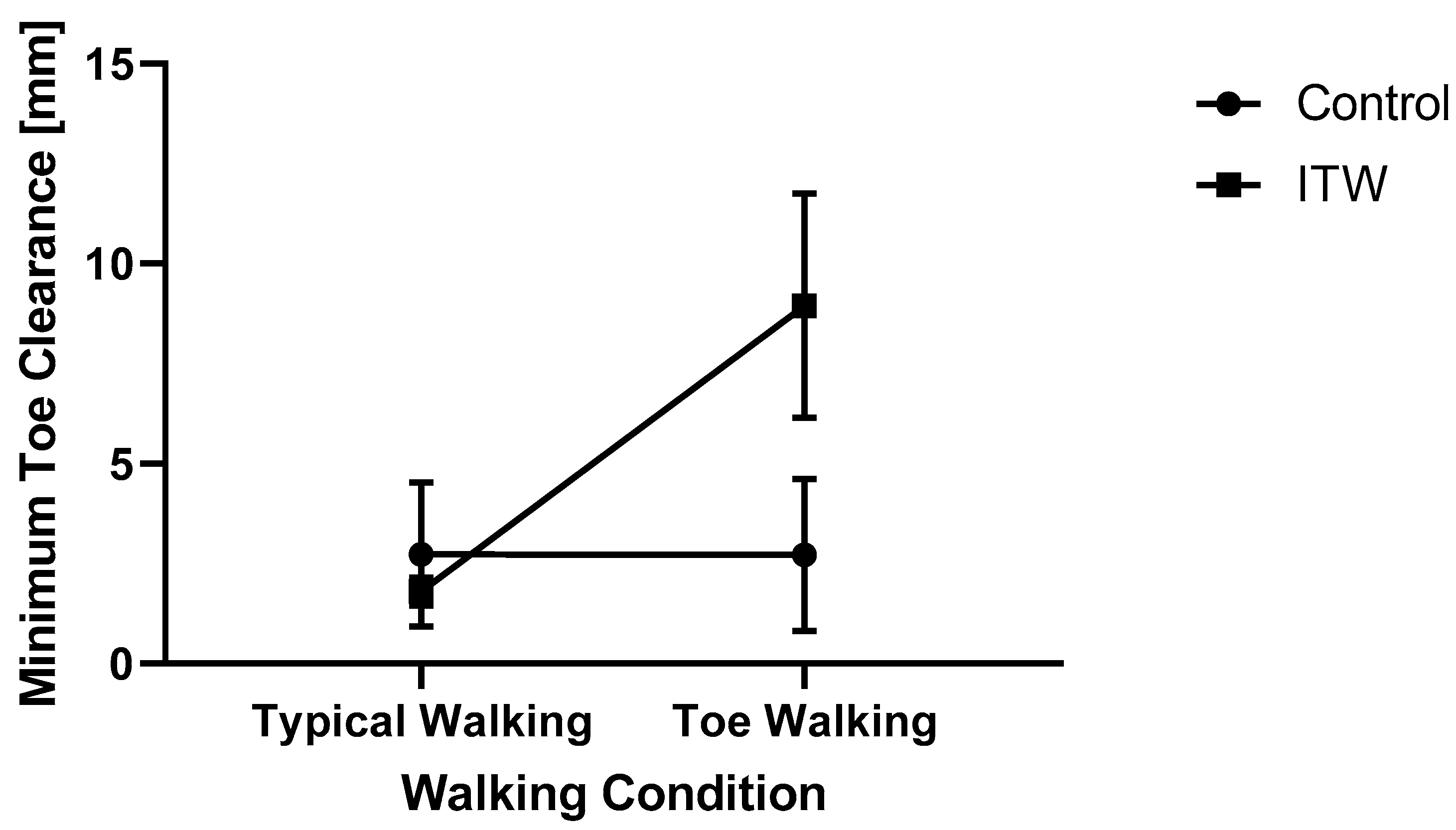
| Minimum Toe Clearance [mm] | 2.7 ± 10.5 | 2.7 ± 11.1 | 8.9 ± 17.1 | 0.3 ± 13.1 |
| Step Width [mm] | 147.0 ± 38.9 | 133.6 ± 28.6 | 167.3 ± 41.3 | 145.2 ± 47.4 |
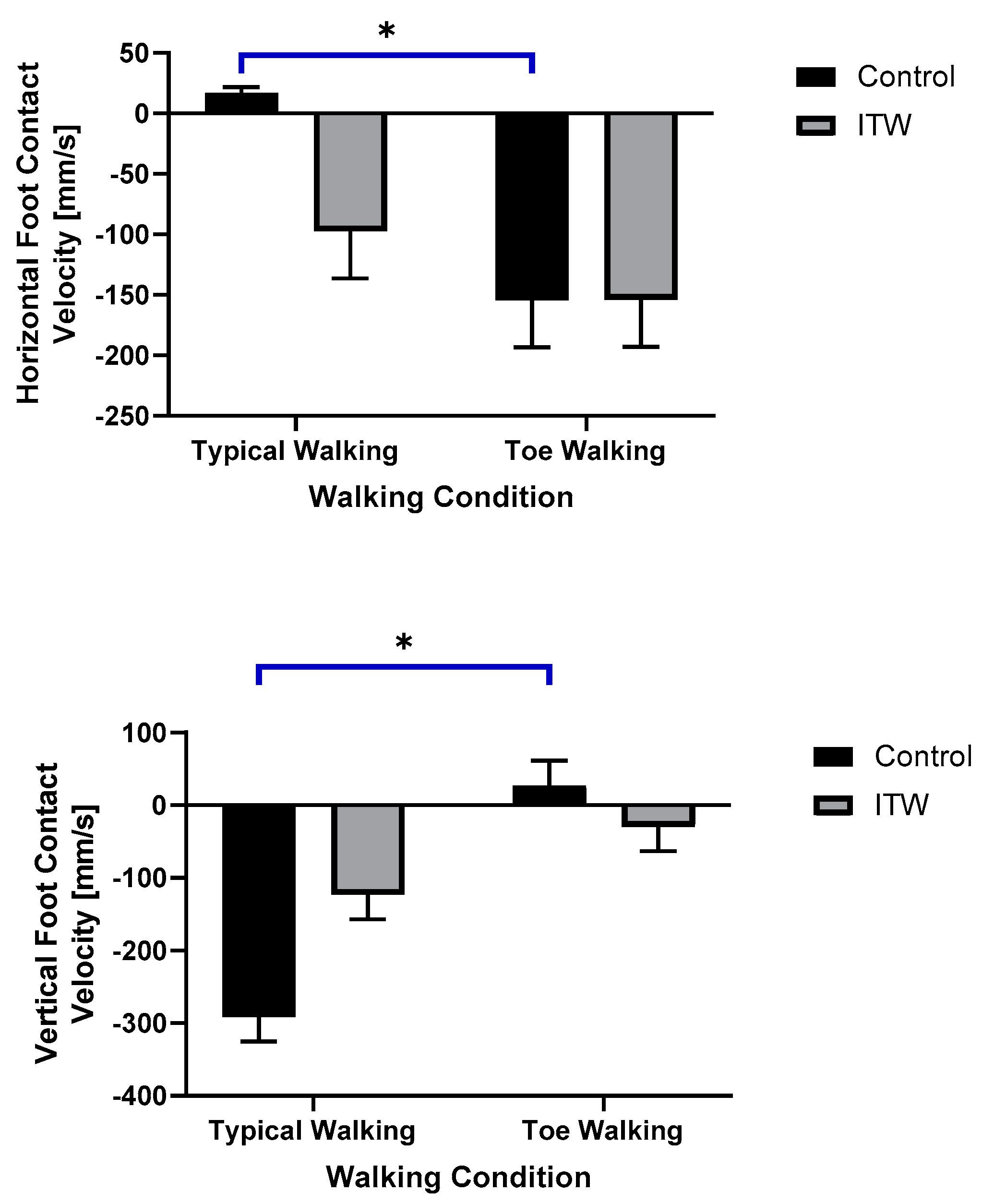
| Horizontal Foot Contact Velocity [mm/s] | −154.3 ± 316.4 | 16.7 ± 176.7 | −47.7 ± 220.0 | −97.4 ± 231.4 |
| Vertical Foot Contact Velocity * [mm/s] | 27.3 ± 172.1 | −291.2 ± 360.9 | −29.3 ± 108.1 | −123.1 ± 211.0 |
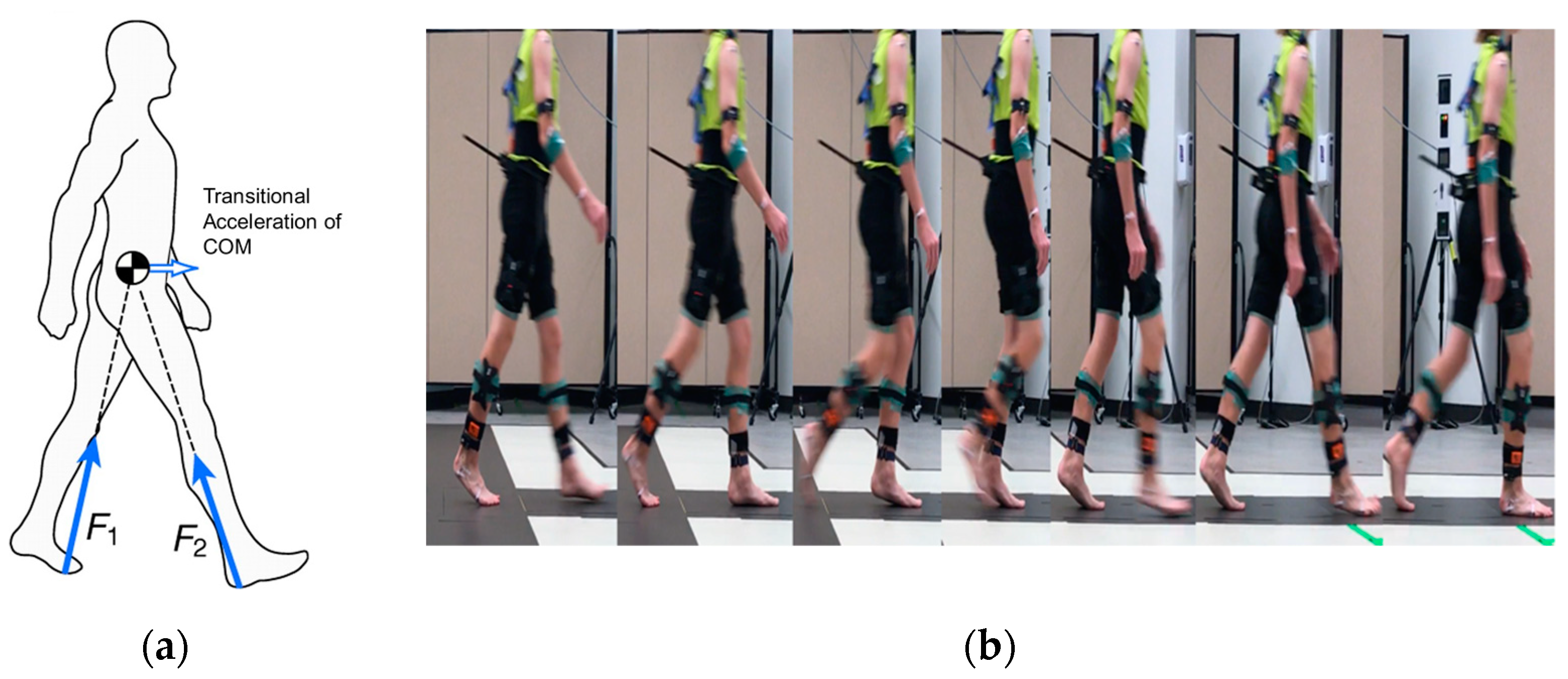
| Transitional Acceleration of COM * [mm/s2] | −288.0 ± 4771.5 | 782.94 ± 2631.8 | 1284.0 ± 3636.5 | 99.964 ± 2366.8 |
| Toe Walking | Typical Walking | ||||||
|---|---|---|---|---|---|---|---|
| Push-Off | Swing | FIC | Push-Off | Swing | FIC | ||
| Control [Degrees] | Ankle | −26.8 ± 12.4 | −34.2 ± 8.0 | −27.6 ± 10.3 | 1.8 ± 5.9 | −15.4 ± 6.4 | 0.2 ± 5.5 |
| Knee | 5.1 ± 9.8 | 25.6 ± 6.4 | 4.4 ± 8.7 | 1.5 ± 7.2 | 33.5 ± 6.6 | 1.7 ± 7.4 | |
| Hip | 38.0 ± 14.5 | 3.0 ± 12.9 | 36.3 ± 13.6 | 37.6 ± 12.8 | 2.2 ± 10.7 | 37.6 ± 11.3 | |
| ITW [Degrees] | Ankle | −34.6 ± 10.8 | −39.7 ± 10.3 | −33.5 ± 9.8 | −9.9 ± 7.1 | −19.1 ± 9.8 | −8.7 ± 6.8 |
| Knee | 1.4 ± 8.4 | 22.1 ± 5.7 | 1.8 ± 7.5 | 0.8 ± 5.0 | 32.2 ± 6.0 | 1.8 ± 5.1 | |
| Hip | 41.3 ± 15.2 | 4.5 ± 11.0 | 42.7 ± 13.8 | 38.7 ± 11.8 | 8.7 ± 12.2 | 40.0 ± 11.7 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soangra, R.; Shiraishi, M.; Beuttler, R.; Gwerder, M.; Boyd, L.; Muthukumar, V.; Trabia, M.; Aminian, A.; Grant-Beuttler, M. Foot Contact Dynamics and Fall Risk among Children Diagnosed with Idiopathic Toe Walking. Appl. Sci. 2021, 11, 2862. https://doi.org/10.3390/app11062862
Soangra R, Shiraishi M, Beuttler R, Gwerder M, Boyd L, Muthukumar V, Trabia M, Aminian A, Grant-Beuttler M. Foot Contact Dynamics and Fall Risk among Children Diagnosed with Idiopathic Toe Walking. Applied Sciences. 2021; 11(6):2862. https://doi.org/10.3390/app11062862
Chicago/Turabian StyleSoangra, Rahul, Michael Shiraishi, Richard Beuttler, Michelle Gwerder, LouAnne Boyd, Venkatesan Muthukumar, Mohamed Trabia, Afshin Aminian, and Marybeth Grant-Beuttler. 2021. "Foot Contact Dynamics and Fall Risk among Children Diagnosed with Idiopathic Toe Walking" Applied Sciences 11, no. 6: 2862. https://doi.org/10.3390/app11062862