Quantitative Analysis of Movements in Children with Attention-Deficit Hyperactivity Disorder Using a Smart Watch at School

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
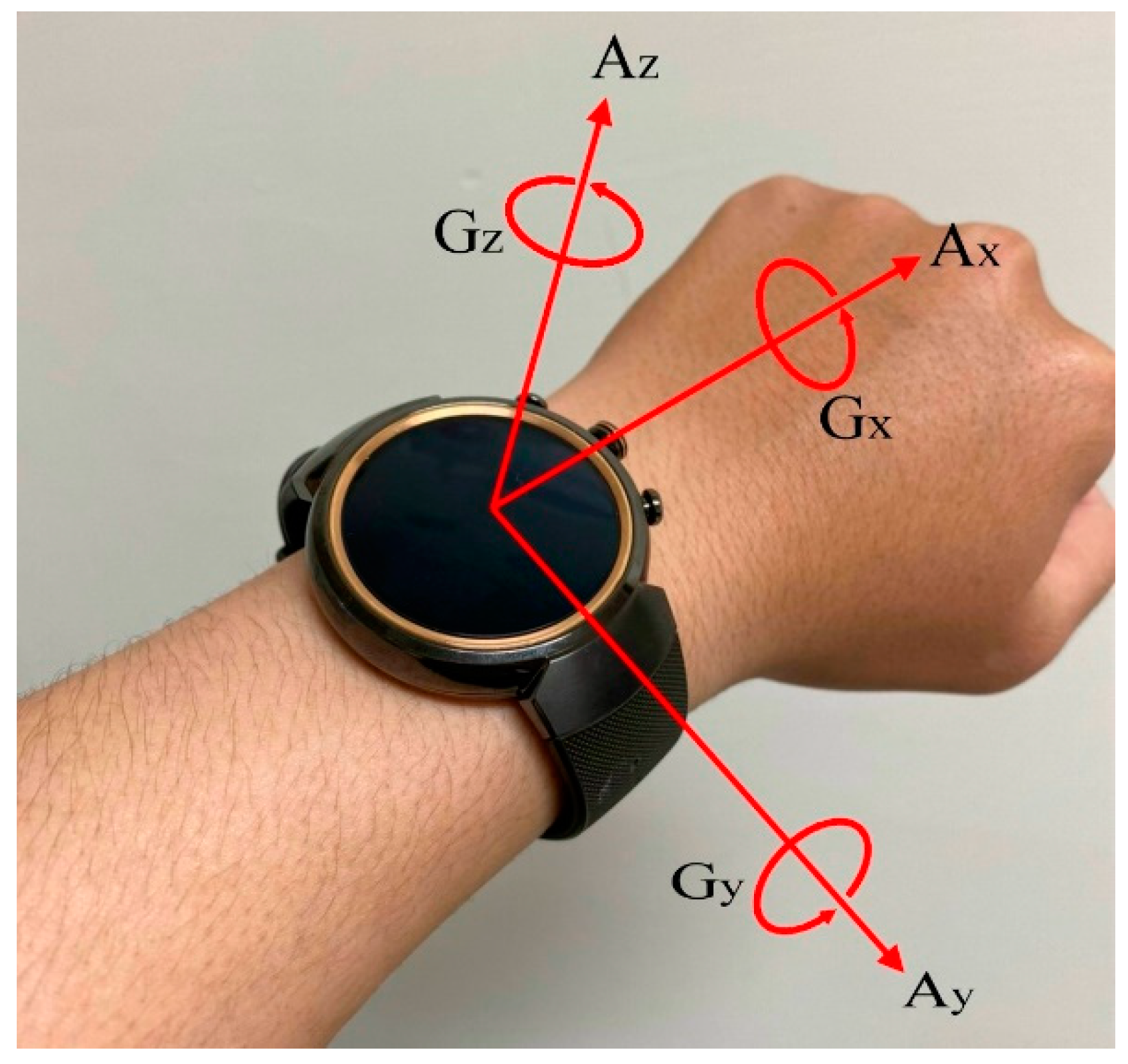
2.2. Gyroscope and Accelerometer Recordings
2.3. Feature Extraction
- Variance is the spread of the probability distribution of the signal subsequence. To estimate population variance, a sample variance was calculated using the following equation:
- ZCR is the rate of sign changes along the signal subsequence. It was calculated using the following equation:where is the sign function and is defined as follows:
2.4. Feature Discriminability Analysis
2.5. Statistical Analysis
3. Results
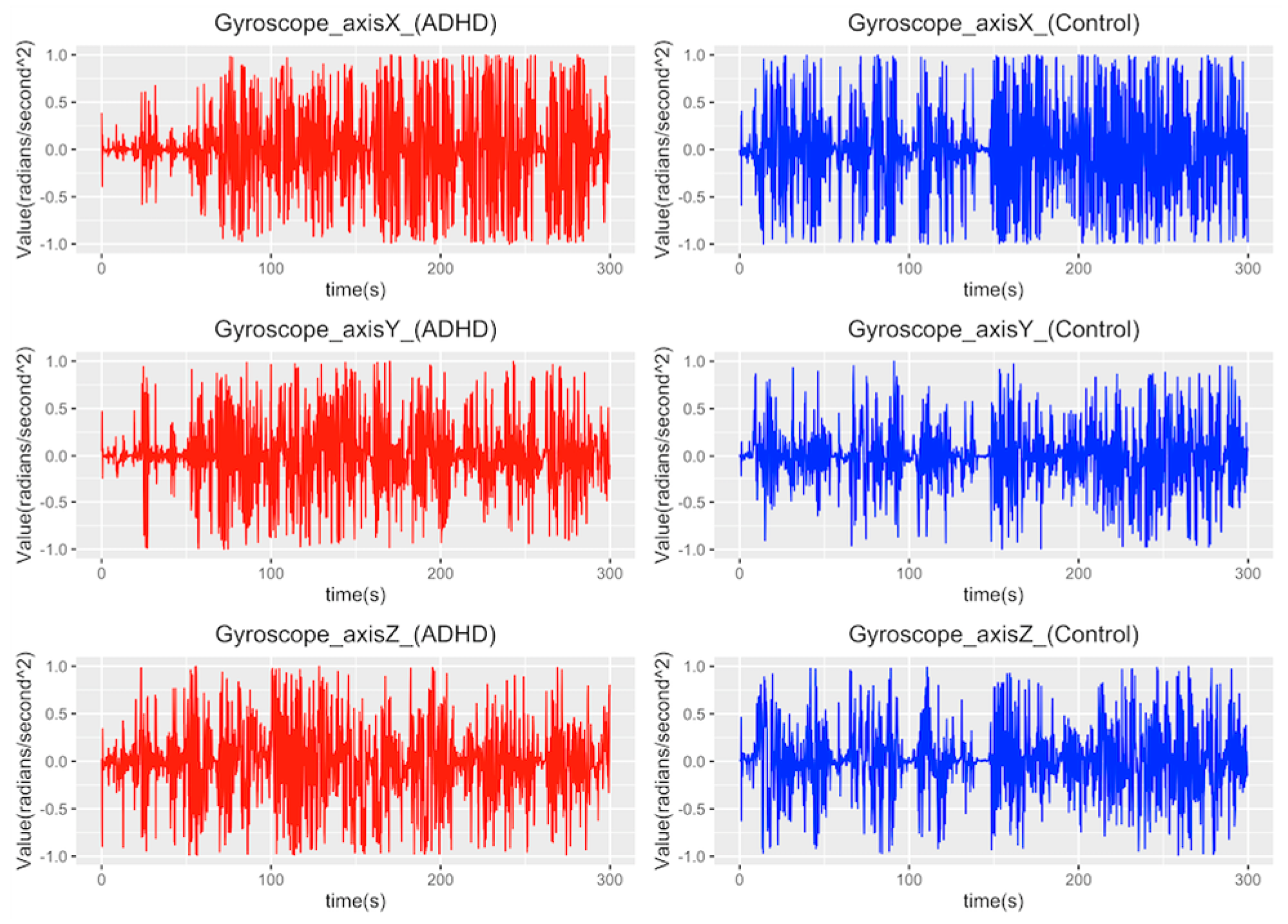
3.1. Comparison of Gyroscope Measurements between ADHD and Control Groups
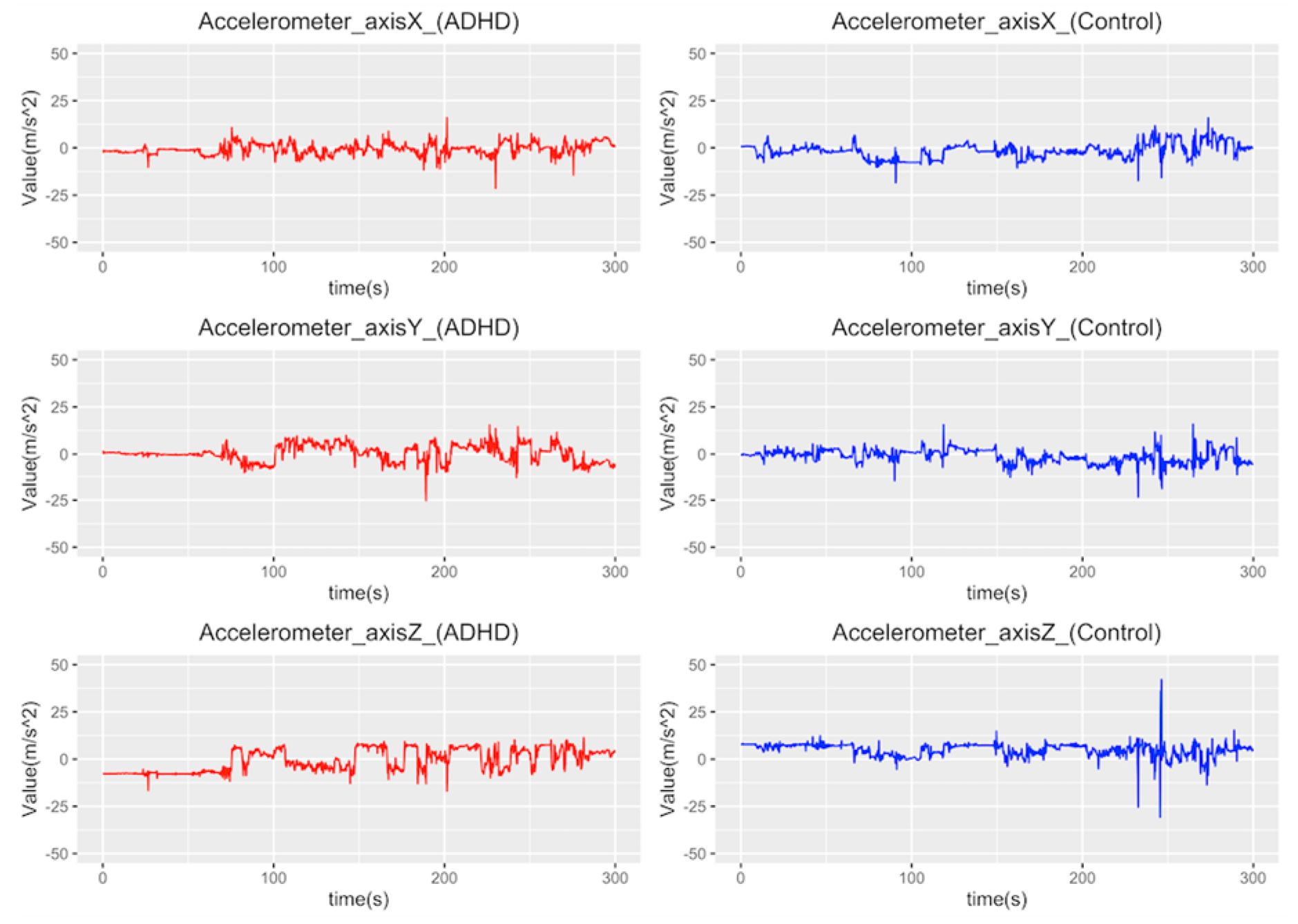
3.2. Comparison of Accelerometer Measurements between ADHD and Control Groups
3.3. Discriminating ADHD and Control Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Olfson, M.; Gameroff, M.J.; Marcus, S.C.; Jensen, P.S. National trends in the treatment of attention deficit hyperactivity disorder. Am. J. Psychiatry 2003, 160, 1071–1077. [Google Scholar] [CrossRef] [PubMed]
- Robison, L.M.; Sclar, D.A.; Skaer, T.L. Datapoints: Trends in adhd and stimulant use among adults: 1995–2002. Psychiatr. Serv. 2005, 56, 1497. [Google Scholar] [CrossRef] [PubMed]
- Toh, S. Datapoints: Trends in adhd and stimulant use among children, 1993–2003. Psychiatr. Serv. 2006, 57, 1091. [Google Scholar] [CrossRef] [PubMed]
- Gualtieri, C.T.; Johnson, L.G. Adhd: Is objective diagnosis possible? Psychiatry 2005, 2, 44–53. [Google Scholar] [PubMed]
- Lopez-Villalobos, J.A.; Andres-De Llano, J.; Lopez-Sanchez, M.V.; Rodriguez-Molinero, L.; Garrido-Redondo, M.; Sacristan-Martin, A.M.; Martinez-Rivera, M.T.; Alberola-Lopez, S. Criterion validity and clinical usefulness of attention deficit hyperactivity disorder rating scale iv in attention deficit hyperactivity disorder (adhd) as a function of method and age. Psicothema 2017, 29, 103–110. [Google Scholar] [PubMed]
- Edwards, M.C.; Gardner, E.S.; Chelonis, J.J.; Schulz, E.G.; Flake, R.A.; Diaz, P.F. Estimates of the validity and utility of the conners’ continuous performance test in the assessment of inattentive and/or hyperactive-impulsive behaviors in children. J. Abnorm. Child Psychol. 2007, 35, 393–404. [Google Scholar] [CrossRef]
- Halperin, J.M.; Sharma, V.; Greenblatt, E.; Schwartz, S.T. Assessment of the continuous performance test: Reliability and validity in a nonreferred sample. J. Psychol. Assess. 1991, 3, 603. [Google Scholar] [CrossRef]
- Stetter, B.J.; Krafft, F.C.; Ringhof, S.; Stein, T.; Sell, S. A machine learning and wearable sensor based approach to estimate external knee flexion and adduction moments during various locomotion tasks. Front. Bioeng. Biotechnol. 2020, 8, 9. [Google Scholar] [CrossRef]
- Rozin Kleiner, A.F.; Bellomo, A.; Pagnussat, A.S.; de Athayde Costa, E.S.A.; Sforza, C.; Cicuto Ferreira Rocha, N.A. Wearable sensors, cerebral palsy and gait assessment in everyday environments: Is it a reality?—A systematic review. Funct. Neurol. 2019, 34, 85–91. [Google Scholar]
- Channa, A.; Popescu, N.; Ciobanu, V. Wearable solutions for patients with parkinson’s disease and neurocognitive disorder: A systematic review. Sensors 2020, 20, 2713. [Google Scholar] [CrossRef]
- Compagnat, M.; Mandigout, S.; Batcho, C.S.; Vuillerme, N.; Salle, J.Y.; David, R.; Daviet, J.C. Validity of wearable actimeter computation of total energy expenditure during walking in post-stroke individuals. Ann. Phys. Rehabil. Med. 2020, 63, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Garcia Murillo, L.; Cortese, S.; Anderson, D.; Di Martino, A.; Castellanos, F.X. Locomotor activity measures in the diagnosis of attention deficit hyperactivity disorder: Meta-analyses and new findings. J. Neurosci. Methods 2015, 252, 14–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Infante, M.A.; Moore, E.M.; Nguyen, T.T.; Fourligas, N.; Mattson, S.N.; Riley, E.P. Objective assessment of adhd core symptoms in children with heavy prenatal alcohol exposure. Physiol. Behav. 2015, 148, 45–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert, H.; Qin, L.; Li, D.; Zhang, X.; Johnstone, S.J. Aiding the diagnosis of ad/hd in childhood: Using actigraphy and a continuous performance test to objectively quantify symptoms. Res. Dev. Disabil. 2016, 59, 35–42. [Google Scholar] [CrossRef]
- Martin-Martinez, D.; Casaseca-de-la-Higuera, P.; Alberola-Lopez, S.; Andres-de-Llano, J.; Lopez-Villalobos, J.A.; Ardura-Fernandez, J.; Alberola-Lopez, C. Nonlinear analysis of actigraphic signals for the assessment of the attention-deficit/hyperactivity disorder (adhd). Med. Eng. Phys. 2012, 34, 1317–1329. [Google Scholar] [CrossRef]
- De Crescenzo, F.; Armando, M.; Mazzone, L.; Ciliberto, M.; Sciannamea, M.; Figueroa, C.; Janiri, L.; Quested, D.; Vicari, S. The use of actigraphy in the monitoring of methylphenidate versus placebo in adhd: A meta-analysis. Atten. Deficit Hyperact. Disord. 2014, 6, 49–58. [Google Scholar] [CrossRef]
- De Crescenzo, F.; Licchelli, S.; Ciabattini, M.; Menghini, D.; Armando, M.; Alfieri, P.; Mazzone, L.; Pontrelli, G.; Livadiotti, S.; Foti, F.; et al. The use of actigraphy in the monitoring of sleep and activity in adhd: A meta-analysis. Sleep Med. Rev. 2016, 26, 9–20. [Google Scholar] [CrossRef]
- Tseng, M.H.; Henderson, A.; Chow, S.M.; Yao, G. Relationship between motor proficiency, attention, impulse, and activity in children with adhd. Dev. Med. Child. Neurol. 2004, 46, 381–388. [Google Scholar] [CrossRef]
- Wood, A.C.; Asherson, P.; Rijsdijk, F.; Kuntsi, J. Is overactivity a core feature in adhd? Familial and receiver operating characteristic curve analysis of mechanically assessed activity level. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 1023–1030. [Google Scholar] [CrossRef]
- Kam, H.J.; Lee, K.; Cho, S.M.; Shin, Y.M.; Park, R.W. High-resolution actigraphic analysis of adhd: A wide range of movement variability observation in three school courses—A pilot study. Healthc Inform. Res. 2011, 17, 29–37. [Google Scholar] [CrossRef] [Green Version]
- O’Mahony, N.; Florentino-Liano, B.; Carballo, J.J.; Baca-Garcia, E.; Rodriguez, A.A. Objective diagnosis of adhd using imus. Med. Eng. Phys. 2014, 36, 922–926. [Google Scholar] [CrossRef] [PubMed]
- Ricci, M.; Terribili, M.; Giannini, F.; Errico, V.; Pallotti, A.; Galasso, C.; Tomasello, L.; Sias, S.; Saggio, G. Wearable-based electronics to objectively support diagnosis of motor impairments in school-aged children. J. Biomech. 2018, 83, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Shandhi, M.M.H.; Semiz, B.; Hersek, S.; Goller, N.; Ayazi, F.; Inan, O.T. Performance analysis of gyroscope and accelerometer sensors for seismocardiography-based wearable pre-ejection period estimation. IEEE J. Biomed. Health Inform. 2019, 23, 2365–2374. [Google Scholar] [CrossRef] [PubMed]
- Alberts, J.L.; Hirsch, J.R.; Koop, M.M.; Schindler, D.D.; Kana, D.E.; Linder, S.M.; Campbell, S.; Thota, A.K. Using accelerometer and gyroscopic measures to quantify postural stability. J. Athl. Train. 2015, 50, 578–588. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, M.; Johnson, K. Applied Predictive Modeling; Springer: New York, NY, USA, 2013; ISBN 9781461468486. [Google Scholar]
- Gawrilow, C.; Kuhnhausen, J.; Schmid, J.; Stadler, G. Hyperactivity and motoric activity in adhd: Characterization, assessment, and intervention. Front. psychiatry 2014, 5, 171. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| ADHD | Control | p Value | |
|---|---|---|---|
| Age | 6 years 11 months ± 1 year 0 months | 6 years 9 months ± 1 years 1 months | 0.2765 |
| Sex (M/F) | 11/4 | 11/4 | NA |
| SNAP (teacher) | 43.38 ± 14.03 | 6.67 ± 5.38 | <0.0001 |
| SNAP (parents) | 44.73 ± 14.68 | 14.87 ± 10.29 | <0.0001 |
| ADHD | Control | p Value | ||
|---|---|---|---|---|
| Variance | Gx | 0.200 ± 0.052 | 0.174 ± 0.050 | 0.021 |
| Gy | 0.093 ± 0.029 | 0.075 ± 0.020 | 0.001 * | |
| Gz | 0.094 ± 0.026 | 0.080 ± 0.024 | 0.012 | |
| ZCR | Gx | 0.421 ± 0.010 | 0.415 ± 0.011 | 0.005 * |
| Gy | 0.414 ± 0.014 | 0.404 ± 0.018 | 0.003 * | |
| Gz | 0.401 ± 0.016 | 0.389 ± 0.021 | 0.004 * |
| ADHD | Control | p Value | ||
|---|---|---|---|---|
| Variance | Ax | 4.849 ± 3.173 | 3.071 ± 1.566 | 0.001 * |
| Ay | 5.149 ± 3.061 | 3.2093± 1.395 | <0.001 * | |
| Az | 4.866 ± 2.440 | 3.096 ± 1.280 | <0.001 * | |
| ZCR | Ax | 0.078 ± 0.015 | 0.068 ± 0.024 | 0.019 |
| Ay | 0.055 ± 0.021 | 0.045 ± 0.015 | 0.010 | |
| Az | 0.067 ± 0.030 | 0.051 ± 0.024 | 0.006 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, L.-C.; Ouyang, C.-S.; Chiang, C.-T.; Wu, R.-C.; Yang, R.-C. Quantitative Analysis of Movements in Children with Attention-Deficit Hyperactivity Disorder Using a Smart Watch at School. Appl. Sci. 2020, 10, 4116. https://doi.org/10.3390/app10124116
Lin L-C, Ouyang C-S, Chiang C-T, Wu R-C, Yang R-C. Quantitative Analysis of Movements in Children with Attention-Deficit Hyperactivity Disorder Using a Smart Watch at School. Applied Sciences. 2020; 10(12):4116. https://doi.org/10.3390/app10124116
Chicago/Turabian StyleLin, Lung-Chang, Chen-Sen Ouyang, Ching-Tai Chiang, Rong-Ching Wu, and Rei-Cheng Yang. 2020. "Quantitative Analysis of Movements in Children with Attention-Deficit Hyperactivity Disorder Using a Smart Watch at School" Applied Sciences 10, no. 12: 4116. https://doi.org/10.3390/app10124116