
Long-Term Changes of Positive Anomalies of Erythema-Effective UV Irradiance Associated with Low Ozone Events in Germany 1983–2019


Abstract
:1. Introduction
2. Materials and Methods
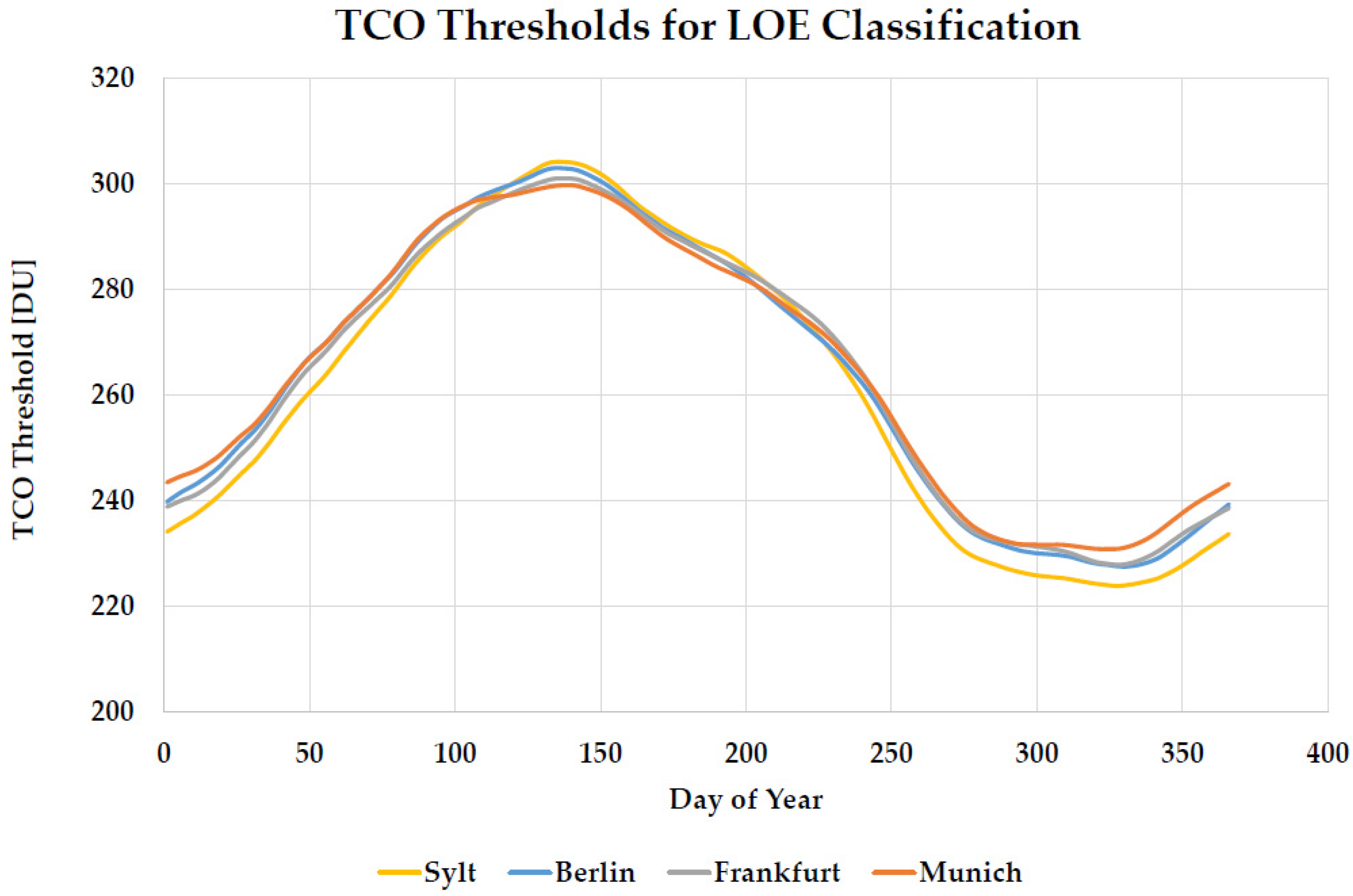
2.1. Total Column Ozone Data and Definition of Low-Ozone Events
2.2. Definition of Subperiods
2.3. Erythema-Effective UV Irradiance Data and Definition of Health-Relevant Low-Ozone Events
3. Results
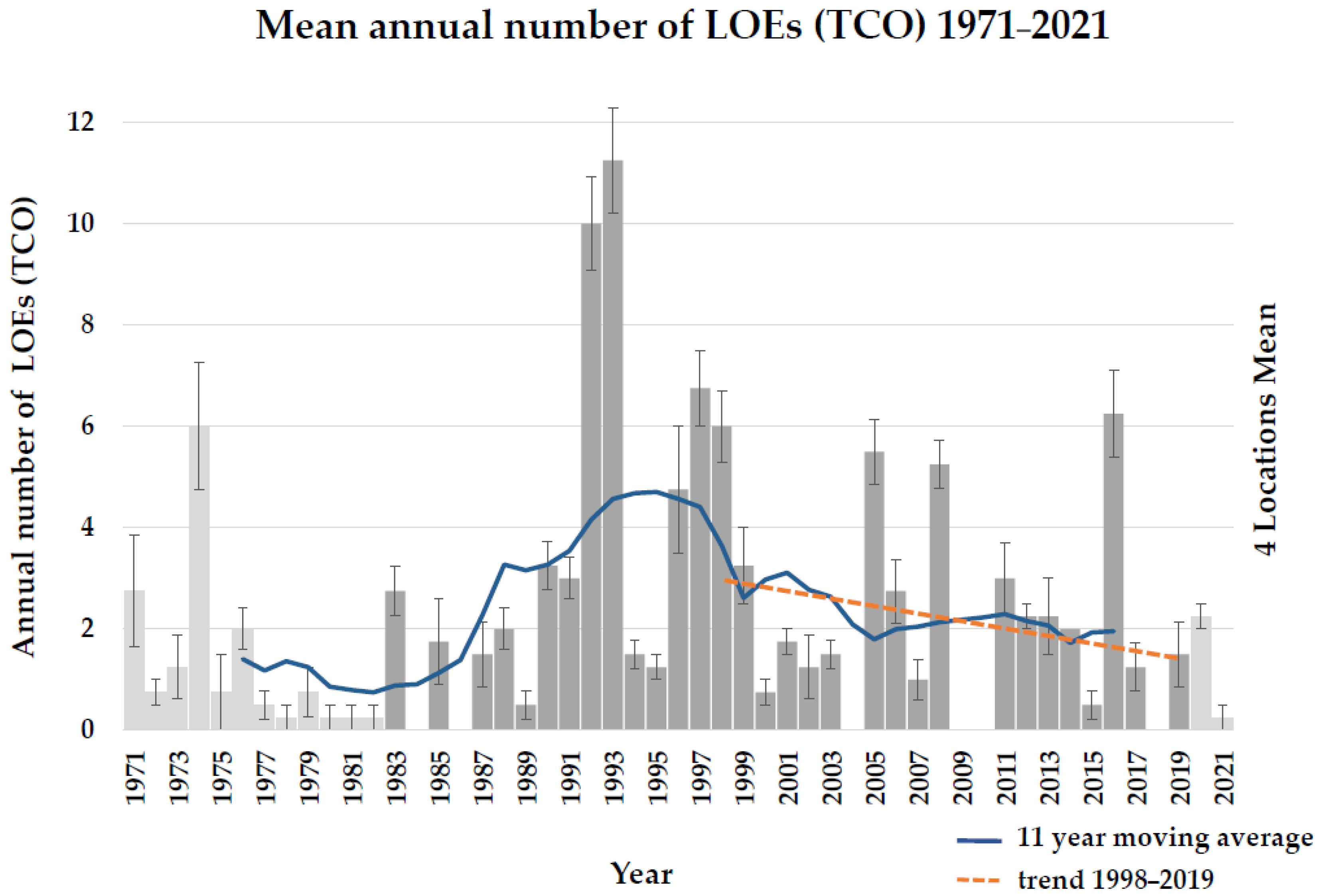
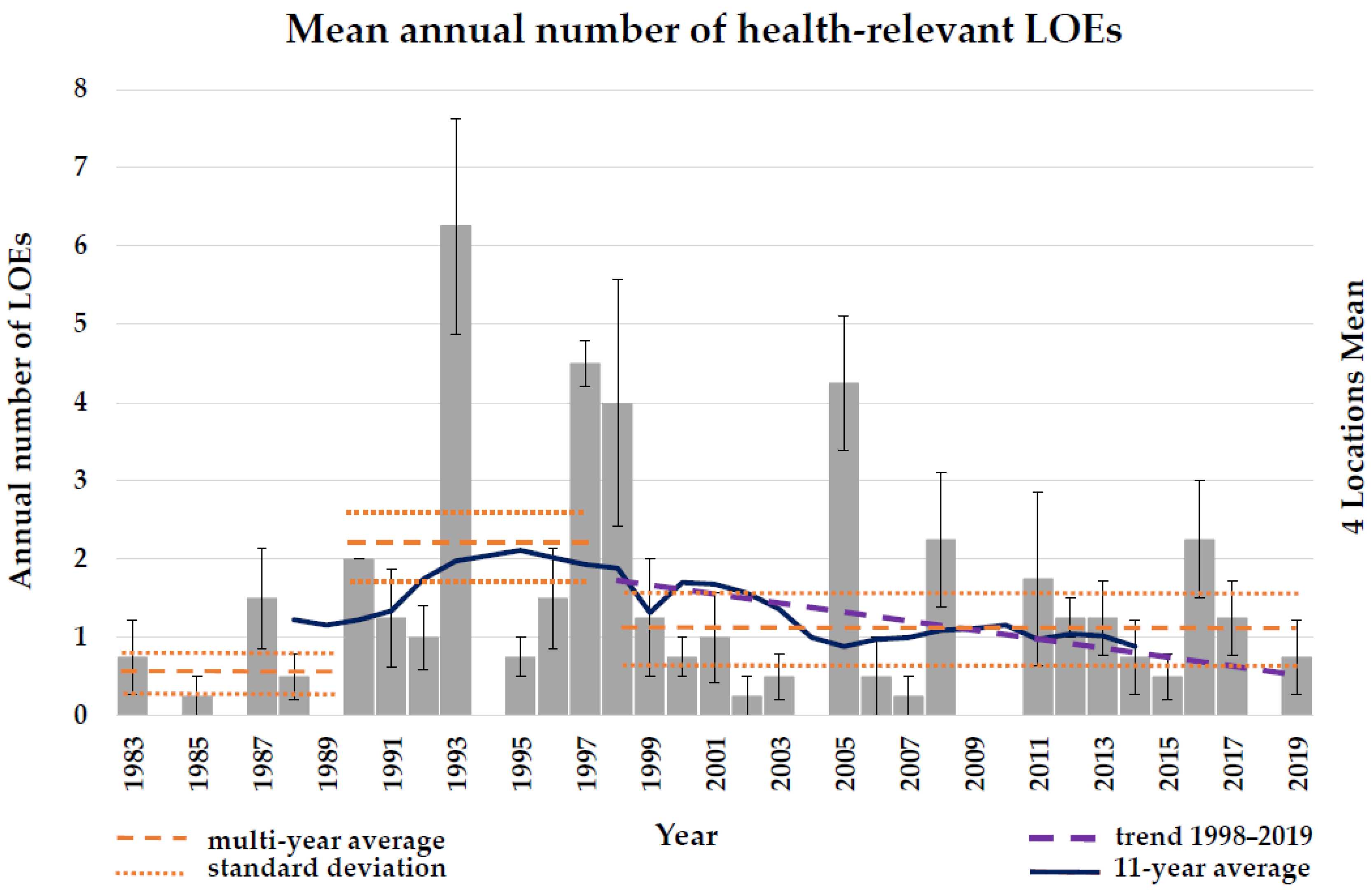
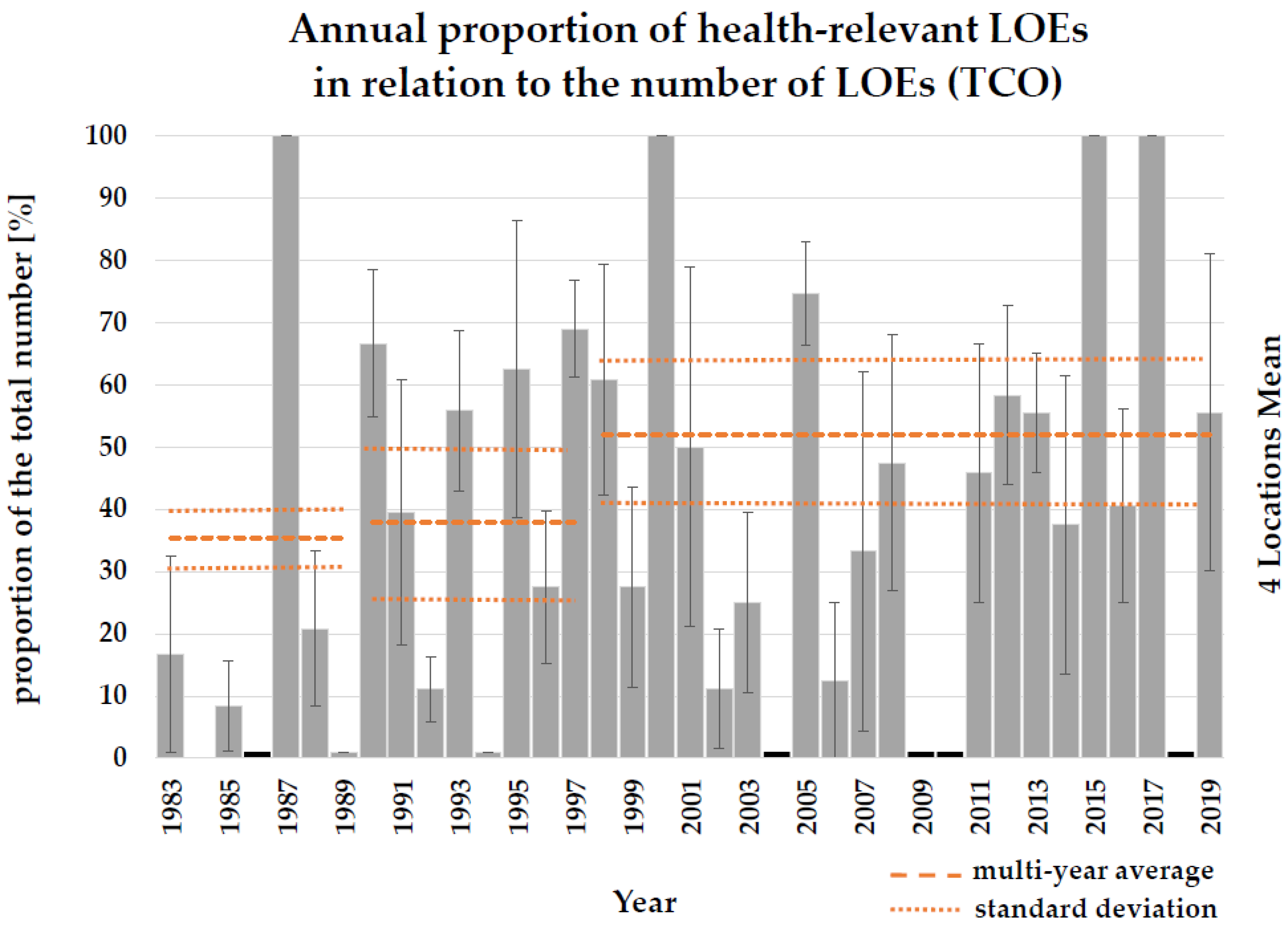
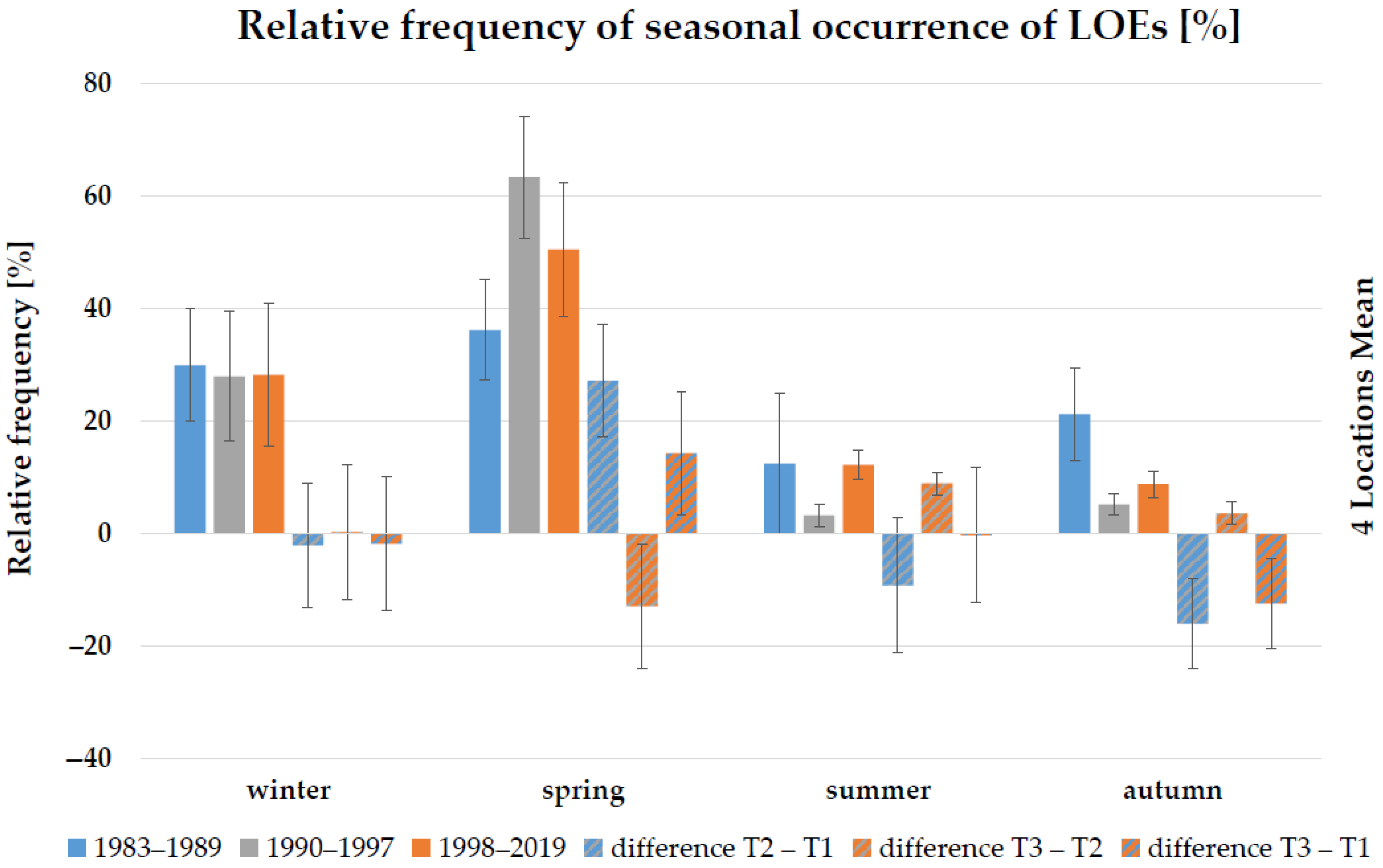
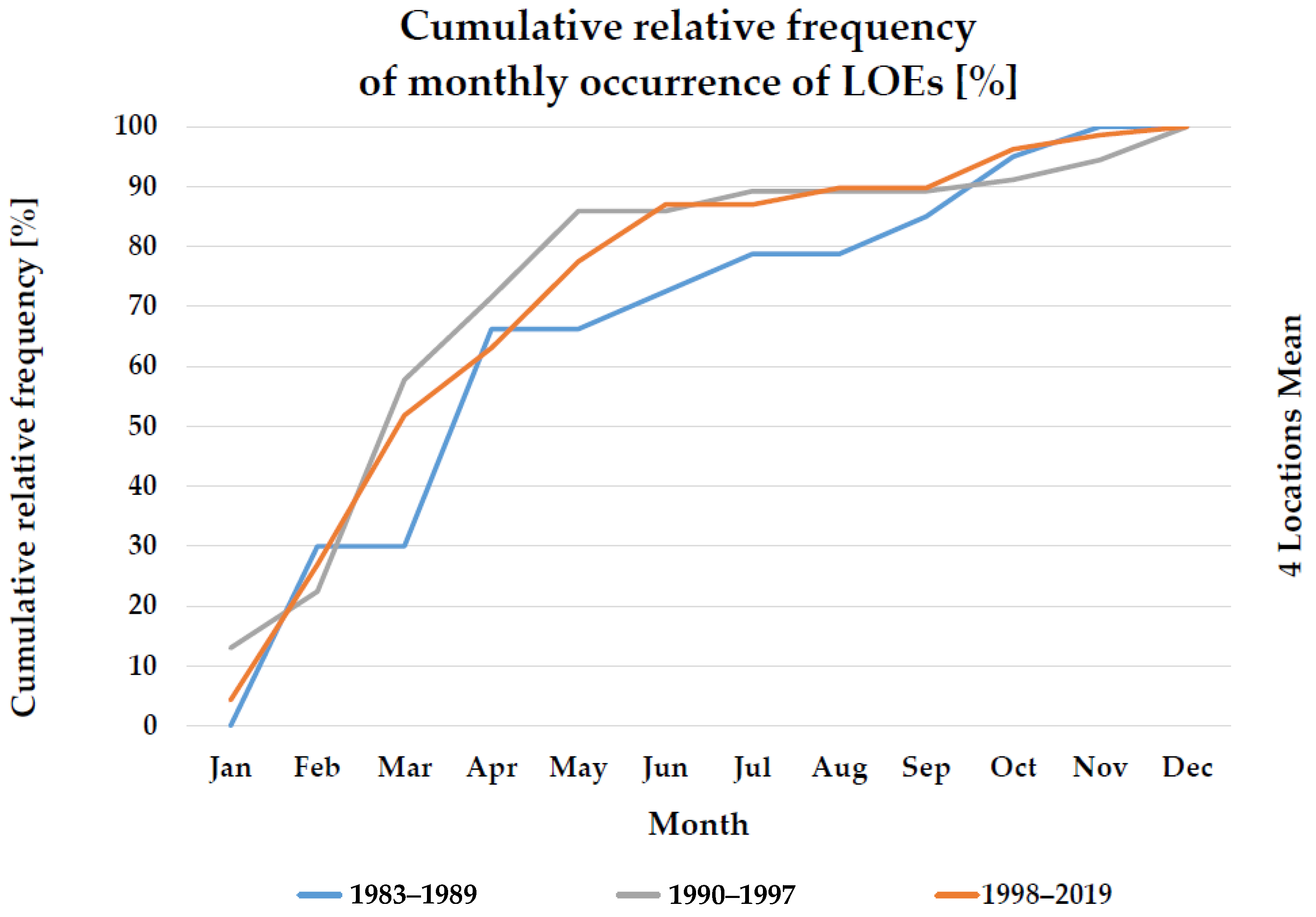
3.1. Occurrence of Human Health-Relevant Low-Ozone Events
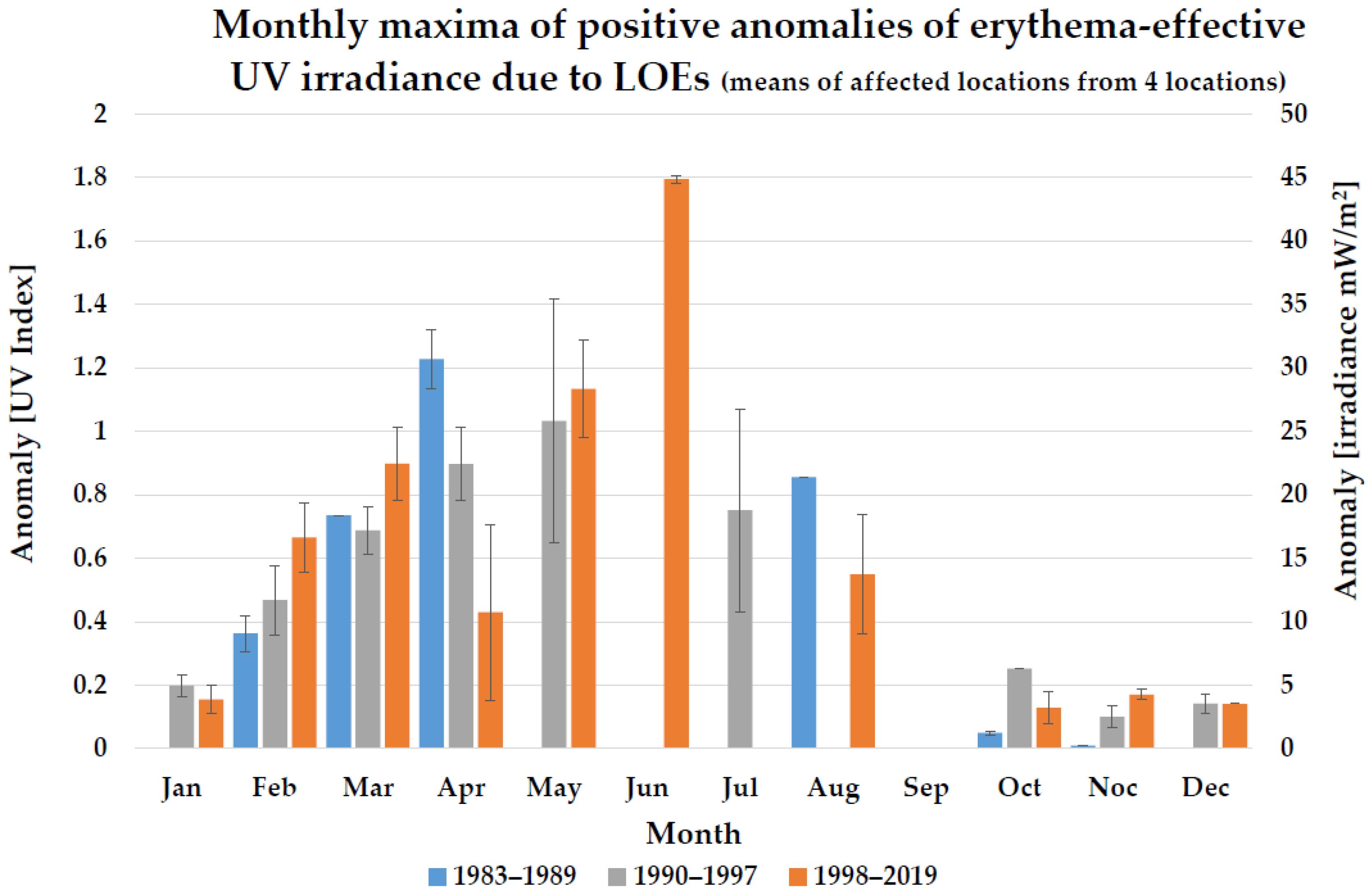
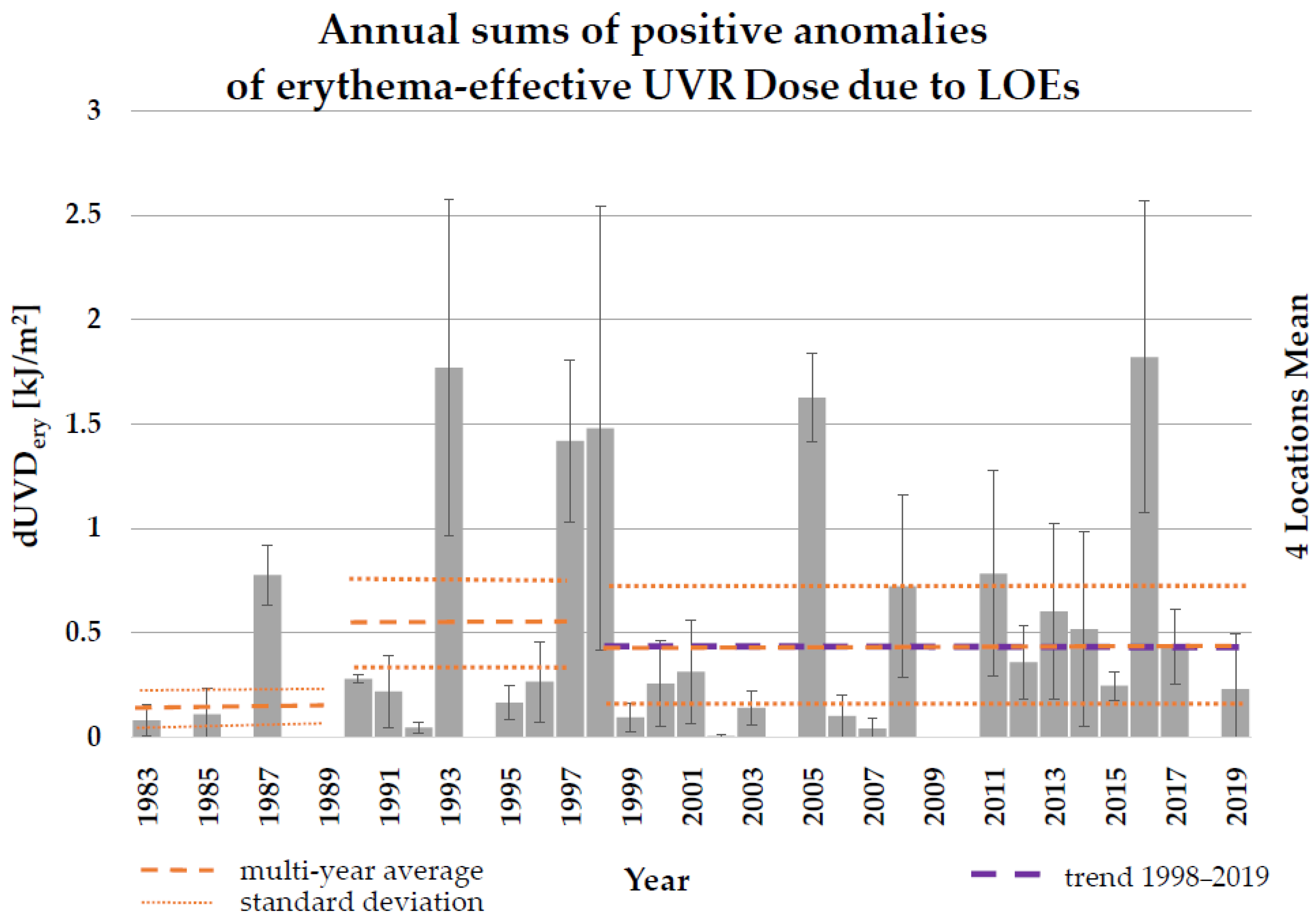
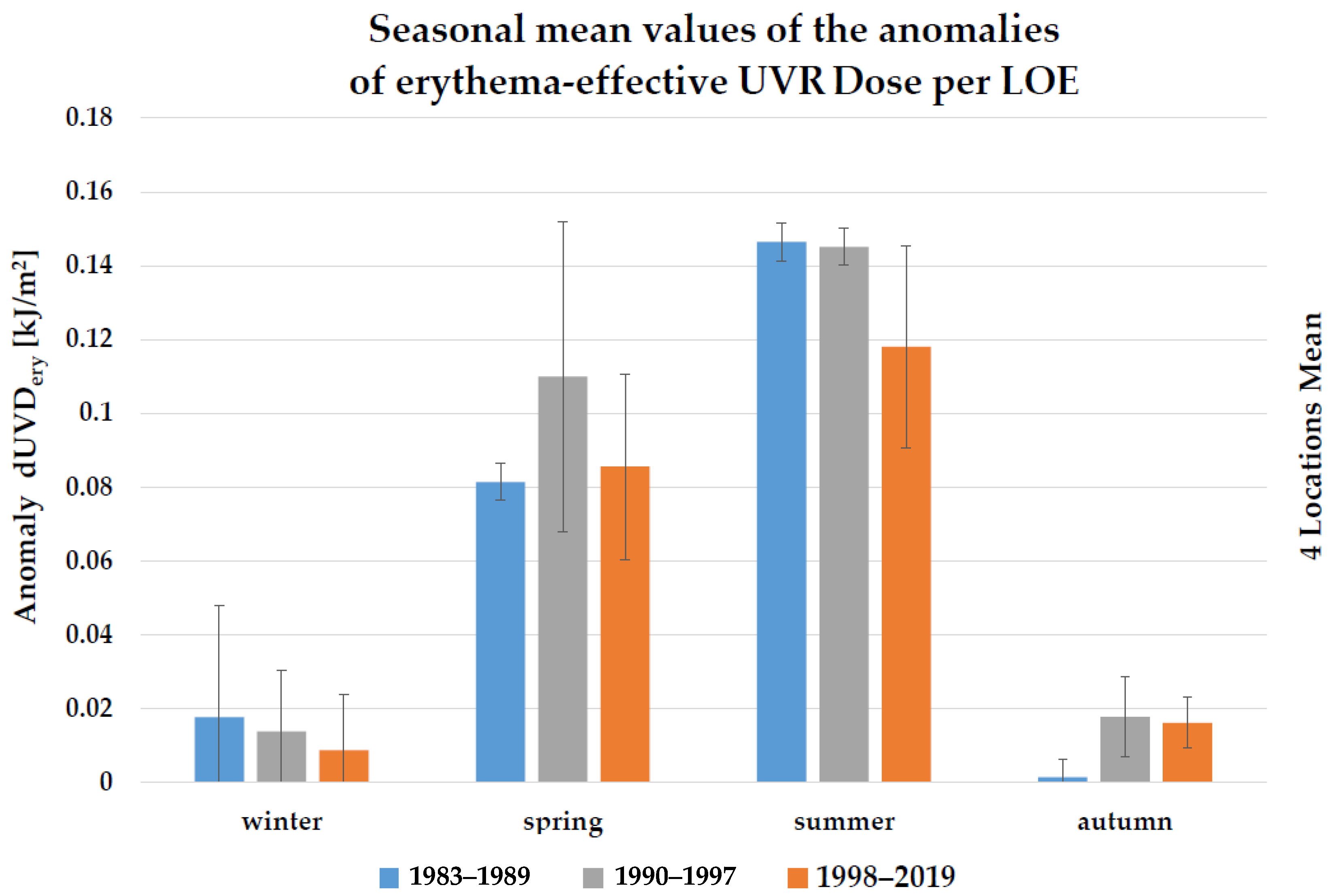
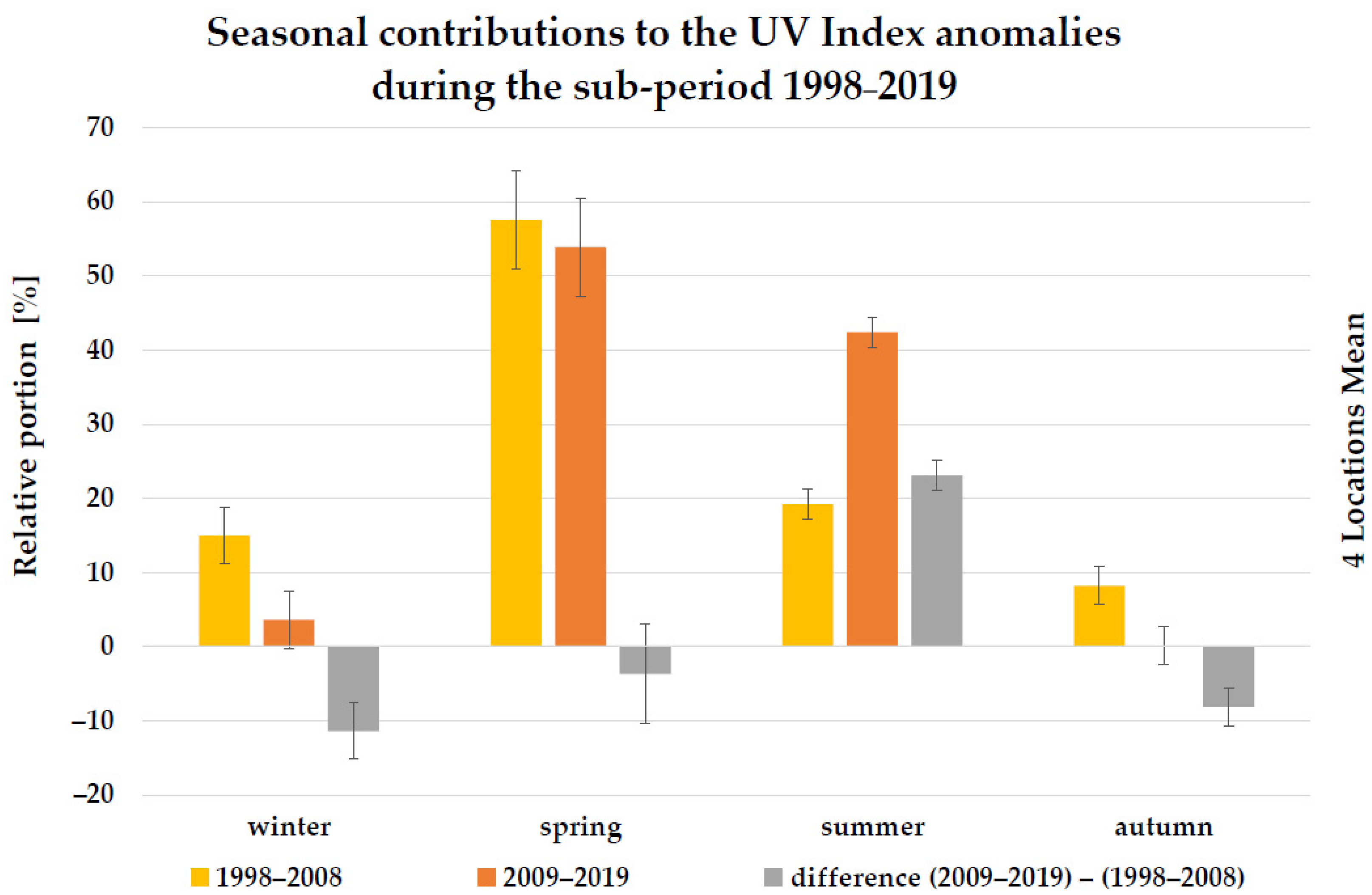
3.2. Anomalies of Erythema-Effective UV Irradiance and UVR Dose Associated with Low-Ozone Events
4. Discussion and Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Norval, M.; Lucas, R.; Cullen, P.; de Gruijl, F.R.; Longstreth, J.; Takizawa, Y.; van der Leun, J.C. The human health effects of ozone depletion and interactions with climate change. Photochem. Photobiol. Sci. 2011, 10, 199–225. [Google Scholar] [CrossRef] [PubMed]
- Lucas, R.M.; Yazar, S.; Young, A.R.; Norval, M.; de Gruijl, F.R.; Takizawa, Y.; Rhodes, L.E.; Sinclair, C.A.; Neale, R.E. Human health in relation to exposure to solar ultraviolet radiation under changing stratospheric ozone and climate. Photochem. Photobiol. Sci. 2019, 18, 641–680. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- WHO World Health Organization. Global Solar UV Index: A Practical Guide. A Joint Recommendation of the World Health Organization, World Meteorological Organization, United Nations Environmental Programme, and the International Commission on Non-Ionizing Radiation Protection; World Health Organization: Geneva, Switzerland, 2002; ISBN 92-4-159007-6. [Google Scholar]
- Yam, Y.; Kwok, A. Ultraviolet light and ocular diseases. Int. Ophthalmol. 2014, 34, 383–400. [Google Scholar] [CrossRef] [PubMed]
- Feretis, E.; Theodorakopoulos, P.; Varotsos, C.; Efstathiou, M.; Tzanis, C.; Xirou, T.; Alexandridou, N.; Aggelou, M. On the plausible association between environmental conditions and human eye damage. Environ. Sci. Pollut. Res. 2002, 9, 163–165. [Google Scholar] [CrossRef]
- Armstrong, B.K.; Kricker, A.; English, R. Sun exposure and skin cancer. Australas. J. Dermatol. 1997, 38 (Suppl. S1), S1–S6. [Google Scholar] [CrossRef]
- Armstrong, B.K.; Kricker, A. The epidemiology of UV induced skin cancer. J. Photochem. Photobiol. B 2001, 63, 8–18. [Google Scholar] [CrossRef]
- Kricker, A.; Weber, M.; Sitas, F.; Banks, E.; Rahman, B.; Goumas, C.; Kabir, A.; Hodgkinson, V.S.; van Kemenade, C.H.; Waterboer, T.; et al. Early life UV and risk of basal and squamous cell carcinoma in New South Wales, Australia. Photochem. Photobiol. 2017, 93, 1483–1491. [Google Scholar] [CrossRef]
- Arnold, M.; de Vries, E.; Whiteman, D.C.; Jemal, A.; Bray, F.; Parkin, D.M.; Soerjomataram, I. Global burden of cutaneous melanoma attributable to ultraviolet radiation in 2012. Int. J. Cancer 2018, 143, 1305–1314. [Google Scholar] [CrossRef]
- Savoye, I.; Olsen, C.M.; Whiteman, D.C.; Bijon, A.; Wald, L.; Dartois, L.; Clavel-Chapelon, F.; Boutron-Ruault, M.C.; Kvaskoff, M. Patterns of Ultraviolet Radiation Exposure and Skin Cancer Risk: The E3N-SunExp Study. J. Epidemiol. 2018, 28, 27–33. [Google Scholar] [CrossRef]
- Geller, A.C.; Jablonski, N.G.; Pagoto, S.L.; Hay, J.L.; Hillhouse, J.; Buller, D.B.; Kenney, W.L.; Robinson, J.K.; Weller, R.B.; Moreno, M.A.; et al. Interdisciplinary perspectives on sun safety. JAMA Dermatol. 2018, 154, 88–92. [Google Scholar] [CrossRef] [PubMed]
- John, S.M.; Garbe, C.; French, L.E.; Takala, J.; Yared, W.; Cardone, A.; Gehring, R.; Spahn, A.; Stratigos, A. Improved protection of outdoor workers from solar ultraviolet radiation: Position statement. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1278–1284. [Google Scholar] [CrossRef] [PubMed]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): S3-Leitlinie Prävention von Hautkrebs, Langversion 2.0, 2021, AWMF Registernummer 032/052OL. Available online: https://www.leitlinienprogramm-onkologie.de/leitlinien/hautkrebs-praevention/ (accessed on 30 July 2021).
- Kahlenborn, W.; Porst, L.; Voß, A.; Fritsch, U.; Renner, K.; Zebisch, M.; Schauser, I. Klimawirkungs-und Risikoanalyse 2021 für Deutschland (KWRA 2021)/Umweltbundesamt, Fachgebiet I 1.6 KomPass. Available online: https://www.umweltbundesamt.de/publikationen/KWRA-Zusammenfassung (accessed on 7 September 2022).
- Bais, A.F.; Bernhard, G.; McKenzie, R.L.; Aucamp, P.J.; Young, P.J.; Ilyas, M.; Jöckel, P.; Deushi, M. Ozone-climate interactions and effects on solar ultraviolet radiation. Photochem. Photobiol. Sci. 2019, 18, 602–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitt, R.; Laschewski, G.; Bais, A.F.; Diémoz, H.; Fountoulakis, I.; Siani, A.M.; Matzarakis, A. UV-Index climatology for Europe based on satellite data. Atmosphere 2020, 11, 727. [Google Scholar] [CrossRef]
- Varotsos, C. Solar ultraviolet radiation and total ozone, as derived from satellite and ground-based instrumentation. Geophys. Res. Lett. 1994, 21, 1787–1790. [Google Scholar] [CrossRef]
- Ipiña, A.; López-Padilla, G.; Retama, A.; Piacentini, R.D.; Madronich, S. Ultraviolet radiation environment of a tropical megacity in transition: Mexico City 2000–2019. Environ. Sci. Technol. 2021, 55, 10946–10956. [Google Scholar] [CrossRef]
- Craig, S.; Earnshaw, C.H.; Virós, A. Ultraviolet light and melanoma. J. Pathol. 2018, 244, 578–585. [Google Scholar] [CrossRef] [Green Version]
- Conforti, C.; Zalaudek, I. Epidemiology and risk factors of melanoma: A review. Dermatol. Pract. Concept. 2021, 11 (Suppl. S1), e2021161S. [Google Scholar] [CrossRef]
- White, E.; Kirkpatrick, C.S.; Lee, J.A. Case-control study of malignant melanoma in Washington State. I. Constitutional factors and sun exposure. Am. J. Epidemiol. 1994, 139, 857–868. [Google Scholar] [CrossRef]
- Newman, P.A.; Lait, L.R.; Schoeberl, M.R. The morphology and meteorology of southern hemisphere spring total ozone mini-holes. Geophys. Res. Lett. 1988, 15, 923–926. [Google Scholar] [CrossRef]
- Siani, A.; Casale, G.R.; Galliani, A. Investigation on a low ozone episode at the end of November 2000 and its effect on ultraviolet radiation. Opt. Eng. 2002, 41, 3082–3089. [Google Scholar] [CrossRef]
- Manney, G.L.; Santee, M.L.; Rex, M.; Livesey, N.J.; Pitts, M.C.; Veefkind, P.; Nash, E.R.; Wohltmann, I.; Lehmann, R.; Froidevaux, L.; et al. Unprecedented Arctic ozone loss in 2011. Nature 2011, 478, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Varotsos, C.A.; Cracknell, A.P.; Tzanis, C. The exceptional ozone depletion over the Arctic in January–March 2011. Remote Sens. Lett. 2012, 3, 343–352. [Google Scholar] [CrossRef]
- Pommereau, J.-P.; Goutail, F.; Pazmino, A.; Lefèvre, F.; Chipperfield, M.P.; Feng, W.; Van Roozendael, M.; Jepsen, N.; Hansen, G.; Kivi, R.; et al. Recent Arctic ozone depletion: Is there an impact of climate change? C. R. Geosci. 2018, 350, 347–353. [Google Scholar] [CrossRef]
- Wohltmann, I.; von der Gathen, P.; Lehmann, R.; Maturilli, M.; Deckelmann, H.; Manney, G.L.; Davies, J.; Tarasick, D.; Jepsen, N.; Kivi, R.; et al. Near-Complete Local Reduction of Arctic Stratospheric Ozone by Severe Chemical Loss in Spring 2020. Geophys. Res. Lett. 2020, 47, e2020GL089547. [Google Scholar] [CrossRef]
- Dameris, M.; Loyola, D.G.; Nützel, M.; Coldewey-Egbers, M.; Lerot, C.; Romahn, F.; van Roozendael, M. Record low ozone values over the Arctic in boreal spring 2020. Atmos. Chem. Phys. 2021, 21, 617–633. [Google Scholar] [CrossRef]
- Petkov, B.H.; Vitale, V.; Di Carlo, P.; Drofa, O.; Mastrangelo, D.; Smedley, A.R.D.; Diémoz, H.; Siani, A.M.; Fountoulakis, I.; Webb, A.R.; et al. An unprecedented Arctic ozone depletion event during spring 2020 and its impacts across Europe. J. Geophys. Res. Atmos. 2021, 128, e2022JD037581. [Google Scholar] [CrossRef]
- McCormack, J.P.; Hood, L.L. The frequency and size of ozone “mini-hole” events at northern midlatitudes in February. Geophys. Res. Lett. 1997, 24, 2647–2650. [Google Scholar] [CrossRef]
- James, P.M. A climatology of ozone mini-holes over the northern hemisphere. Int. J. Climatol. 1998, 18, 1287–1303. [Google Scholar] [CrossRef]
- Petzold, K. The role of dynamics in total ozone deviations from their long-term mean over the Northern Hemisphere. Ann. Geophys. 1999, 17, 231–241. [Google Scholar] [CrossRef]
- Bojkov, R.D.; Balis, D.S. Characteristics of episodes with extremely low ozone values in the northern middle latitudes 1957–2000. Ann. Geophys. 2001, 19, 797–807. [Google Scholar] [CrossRef] [Green Version]
- Hood, L.L.; Soukharev, B.E.; Fromm, M.; McCormack, J.P. Origin of extreme ozone minima at middle to high northern latitudes. J. Geophys. Res. 2001, 106, 20925–20940. [Google Scholar] [CrossRef] [Green Version]
- Krzyscin, J.W. Long-term changes in ozone mini-hole frequency over the Northern Hemisphere derived from ground-based measurements. Int. J. Climatol. 2002, 22, 1425–1439. [Google Scholar] [CrossRef]
- Brönnimann, S.; Hood, L.L. Frequency of low-ozone events over northwestern Europe in 1952–1963 and 1990–2000. Geophys. Res. Lett. 2003, 30, 2118. [Google Scholar] [CrossRef] [Green Version]
- Koch, G.; Wernli, H.; Schwierz, C.; Staehelin, J.; Peter, T. A composite study on the structure and formation of ozone miniholes and minihighs over central Europe. Geophys. Res. Lett. 2005, 32, L12810. [Google Scholar] [CrossRef]
- Iwao, K.; Hirooka, T. Dynamical quantifications of ozone minihole formation on both hemispheres. J. Geophys. Res. 2006, 111, D02104. [Google Scholar] [CrossRef]
- Anton, M.; Serrano, A.; Cancillo, M.L.; Garcia, J.A. Total ozone and solar erythemal irradiance in southwestern Spain: Day-to-day variability and extreme episodes. Geophys. Res. Lett. 2008, 35, L20804. [Google Scholar] [CrossRef]
- Patil, S.D.; Revadekar, J.V. Extremes in total ozone content over northern India. Int. J. Remote Sens. 2009, 30, 2389–2397. [Google Scholar] [CrossRef]
- Rieder, H.E.; Staehelin, J.; Maeder, J.A.; Peter, T.; Ribatet, M.; Davison, A.C.; Stuebi, R.; Weihs, P.; Holawe, F. Extreme events in total ozone over Arosa—Part 1: Application of extreme value theory. Atmos. Chem. Phys. 2010, 10, 10021–10031. [Google Scholar] [CrossRef] [Green Version]
- Rieder, H.E.; Staehelin, J.; Maeder, J.A.; Peter, T.; Ribatet, M.; Davison, A.C.; Stuebi, R.; Weihs, P.; Holawe, F. Extreme events in total ozone over Arosa—Part 2: Fingerprints of atmospheric dynamics and chemistry and effects on mean values and long-term changes. Atmos. Chem. Phys. 2010, 10, 10033–10045. [Google Scholar] [CrossRef]
- Rieder, H.E.; Jansco, L.M.; Di Rocco, S.; Staehelin, J.; Maeder, J.A.; Peter, T.; Ribatet, M.; Davison, A.C.; De Backer, H.; Koehler, U.; et al. Extreme events in total ozone over the Northern mid-latitudes: An analysis based on long-term data sets from five European ground-based stations. Tellus 2011, 63B, 860–874. [Google Scholar] [CrossRef]
- Rieder, H.E.; Frossard, L.; Ribatet, M.; Staehelin, J.; Maeder, J.A.; Di Rocco, S.; Davison, A.C.; Peter, T.; Weihs, P.; Holawe, F. On the relationship between total ozone and atmospheric dynamics and chemistry at mid-latitudes—Part 2: The effects of the El Nino/Southern Oscillation, volcanic eruptions and contributions of atmospheric dynamics and chemistry to long-term total ozone changes. Atmos. Chem. Phys. 2013, 13, 165–179. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Lozano, J.; Utrillas, M.; Nunez, J.; Tamayo, J.; Marin, M.; Esteve, A.; Canada, J.; Moreno, J. Ozone mini-holes over Valencia (Spain) and their influence on the UV erythemal radiation. Int. J. Climatol. 2011, 31, 1554–1566. [Google Scholar] [CrossRef] [Green Version]
- Frossard, L.; Rieder, H.E.; Ribatet, M.; Staehelin, J.; Maeder, J.A.; Di Rocco, S.; Davison, A.C.; Peter, T. On the relationship between total ozone and atmospheric dynamics and chemistry at mid-latitudes–Part 1: Statistical models and spatial fingerprints of atmospheric dynamics and chemistry. Atmos. Chem. Phys. 2013, 13, 147–164. [Google Scholar] [CrossRef] [Green Version]
- Fitzka, M.; Hadzimustafic, J.; Simic, S. Total ozone and Umkehr observations at Hoher Sonnblick 1994–2011: Climatology and extreme events. J. Geophys. Res. Atmos. 2014, 119, 739–752. [Google Scholar] [CrossRef]
- Petkov, B.; Vitale, V.; Tomasi, C.; Siani, A.; Seckmeyer, G.; Webb, A.; Smedley, A.; Casale, G.; Werner, R.; Lanconelli, C.; et al. Response of the ozone column over Europe to the 2011 Arctic ozone depletion event according to groundbased observations and assessment of the consequent variations in surface UV irradiance. Atmos. Environ. 2014, 85, 169–178. [Google Scholar] [CrossRef]
- Petropavlovskikh, I.; Evans, R.; McConville, G.; Manney, G.L.; Rieder, H.E. The influence of the North Atlantic Oscillation and El Niño–Southern Oscillation on mean and extreme values of column ozone over the United States. Atmos. Chem. Phys. 2015, 15, 1585–1598. [Google Scholar] [CrossRef] [Green Version]
- Fragkos, K.; Bais, A.F.; Fountoulakis, I.; Balis, D.S.; Tourpali, K.; Meleti, C.; Zanis, P. Extreme total column ozone events and effects on UV solar radiation at Thessaloniki, Greece. Theor. Appl. Climatol. 2016, 126, 505–517. [Google Scholar] [CrossRef]
- Schwarz, M.; Baumgartner, D.J.; Pietsch, H.; Blumthaler, M.; Weihs, P.; Rieder, H.E. Influence of low ozone episodes on erythemal UV-b radiation in Austria. Theor. Appl. Climatol. 2018, 133, 319–329. [Google Scholar] [CrossRef] [Green Version]
- Chubarova, N.; Nezval, Y.; Sviridenkov, I.; Smirnov, A.; Slutsker, I. Smoke aerosol and its radiative effects during extreme fire event over Central Russia in summer 2010. Atmos. Meas. Tech. 2012, 5, 557–568. [Google Scholar] [CrossRef]
- Kelbch, A.; Wittlich, M.; Bott, A. Quantifying the effects of a low-ozone event and shallow stratocumulus clouds on ultraviolet erythemal radiation exposure. Int. J. Biometeorol. 2019, 63, 359–369. [Google Scholar] [CrossRef]
- Bernhard, G.H.; Fioletov, V.E.; Grooß, J.-U.; Ialongo, I.; Johnsen, B.; Lakkala, K.; Manney, G.L.; Müller, R.; Svendby, T. Record-breaking increases in Arctic solar ultraviolet radiation caused by exceptionally large ozone depletion in 2020. Geophys. Res. Lett. 2020, 47, e2020GL090844. [Google Scholar] [CrossRef] [PubMed]
- Van der A, R.J.; Allaart, M.A.F.; Eskes, H.J. Extended and refined multi sensor reanalysis of total ozone for the period 1970–2012. Atmos. Meas. Tech. 2015, 8, 3021–3035. [Google Scholar] [CrossRef] [Green Version]
- Van der A, R.J.; Allaart, M.A.F.; Eskes, H.J. Multi-Sensor Reanalysis (MSR) of Total Ozone, Version 2; Royal Netherlands Meteorological Institute (KNMI): De Bilt, The Netherlands, 2015. [Google Scholar] [CrossRef]
- Weber, M.; Coldewey-Egbers, M.; Fioletov, V.E.; Frith, S.M.; Wild, J.D.; Burrows, J.P.; Long, C.S.; Loyola, D. Total ozone trends from 1979 to 2016 derived from five merged observational datasets—The emergence into ozone recovery. Atmos. Chem. Phys. 2018, 18, 2097–2117. [Google Scholar] [CrossRef] [Green Version]
- Ozone Trend and Variability Results. Available online: www.dwd.de/EN/research/observing_atmosphere/composition_atmosphere/ozone/cont_nav/o3_trends.html (accessed on 7 September 2022).
- World Meteorological Organization. Executive Summary. Scientific Assessment of Ozone Depletion: 2022; GAW Report No. 278; WMO: Geneva, Switzerland, 2022; p. 56. [Google Scholar]
- Allaart, M.; Van Weele, M.; Fortuin, P.; Kelder, H. An Empirical model to predict the UV-index based on Solar Zenith Angle and Total Ozone. Meteorol. Appl. 2004, 11, 59–65. [Google Scholar] [CrossRef] [Green Version]
- Herman, J.R.; Celarier, E.A. Earth surface reflectivity climatology at 340–380 nm from TOMS data. J. Geophys. Res. 1997, 102, 28003–28011. [Google Scholar] [CrossRef]
- Badosa, J.; van Weele, M. Effects of Aerosols on UV Index; KNMI Scientific Report WR-2002-07; Royal Netherlands Meteorological Institute (KNMI): De Bilt, The Netherlands, 2002. [Google Scholar]
- den Outer, P.N.; Slaper, H.; Kaurola, J.; Lindfors, A.; Kazantzidis, A.; Bais, A.F.; Feister, U.; Junk, J.; Janouch, M.; Josefsson, W. Reconstructing of erythemal ultraviolet radiation levels in Europe for the past 4 decades. J. Geophys. Res. 2010, 115, D10102. [Google Scholar] [CrossRef]
- Fitzpatrick, T.B. The validity and practicality of sun-reactive skin types I through VI. Arch. Dermatol. 1988, 124, 869–871. [Google Scholar] [CrossRef]
- Antonov, D.; Hollunder, M.; Schliemann, S.; Elsner, P. Ultraviolet Exposure and Protection Behavior in the General Population: A Structured Interview Survey. Dermatology 2016, 232, 11–16. [Google Scholar] [CrossRef]
- International Commission on Non-Ionizing Radiation Protection. Protection of workers against ultraviolet radiation. Health Phys. 2010, 99, 66–87. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, M. Untersuchungen zur Validität von Sonnenschutzempfehlungen für Tage mit Niedrigen UV-Index-Werten. Ph.D. Thesis, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany, 4 December 2019. [Google Scholar]
- Malinović-Milićević, S.; Radovanović, M.M.; Mijatović, Z.; Petrović, M.D. Reconstruction and variability of high daily erythemal ultraviolet doses and relationship with total ozone, cloud cover, and albedo in Novi Sad (Serbia). Int. J. Climatol. 2022, 42, 9088–9100. [Google Scholar] [CrossRef]
- McKenzie, R.L.; Paulin, K.J.; Kotkamp, M. Erythemal UV irradiances at Lauder, New Zealand: Relationship between horizontal and normal incidence. Photochem. Photobiol. 1997, 66, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Wittlich, M.; Westerhausen, S.; Strehl, B.; Versteeg, H.; Stöppelmann, W. The GENESIS-UV study on ultraviolet radiation exposure levels in 250 occupations to foster epidemiological and legislative efforts to combat non-melanoma skin cancer. Br. J. Dermatol. 2023, ljac093. [Google Scholar] [CrossRef] [PubMed]
- Commission Internationale De L’Eclairage; World Meteorological Organization. Rationalizing Nomenclature for UV Doses and Effects on Humans; CIE: Vienna, Austria, 2014; Available online: http://cie.co.at/publications/rationalizing-nomenclature-uv-doses-and-effects-humans (accessed on 4 November 2022).
- Laschewski, G.; Matzarakis, A. Weather-Related Human Outdoor Behavior with Respect to Solar Ultraviolet Radiation Exposure in a Changing Climate. Atmosphere 2022, 13, 1183. [Google Scholar] [CrossRef]
- Hitze- und UV-Warnungen. Available online: www.dwd.de/DE/wetter/warnungen_aktuell/kriterien/uv_hitze_warnungen.html?nn=508722 (accessed on 7 September 2022).
- Capellaro, M.; Sturm, D. Evaluation of Information Systems Relevant to Climate Change and Health. Volume 1: Adaption to Climate Change: Evaluation of Existing National Information Systems (UV-Index, Heat Warning System, Airborne Pollen, Ozone Forecasts) from a Public Health Perspective—How to Reach Vulnerable Populations. Umw. Gesundh. 2015, 3, 1–139. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health Risk in Case of Prolonged Exposure | Median of Daily Minimum Exposure Duration to Receive One MED 1 | Mean Proportion of LOEs in Winter in Northern Germany | Mean Proportion of LOEs in Winter in Southern Germany |
|---|---|---|---|
| Negligible | 9.3 h | 33–38% | 0% |
| Existing but low | 3.3 h | 62–67% | 21–43% |
| Consideration necessary | 1.5 h | 0% | 57–79% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laschewski, G.; Matzarakis, A. Long-Term Changes of Positive Anomalies of Erythema-Effective UV Irradiance Associated with Low Ozone Events in Germany 1983–2019. Environments 2023, 10, 31. https://doi.org/10.3390/environments10020031
Laschewski G, Matzarakis A. Long-Term Changes of Positive Anomalies of Erythema-Effective UV Irradiance Associated with Low Ozone Events in Germany 1983–2019. Environments. 2023; 10(2):31. https://doi.org/10.3390/environments10020031
Chicago/Turabian StyleLaschewski, Gudrun, and Andreas Matzarakis. 2023. "Long-Term Changes of Positive Anomalies of Erythema-Effective UV Irradiance Associated with Low Ozone Events in Germany 1983–2019" Environments 10, no. 2: 31. https://doi.org/10.3390/environments10020031