
Effects of Intra-Articular Autologous Adipose Micrograft for the Treatment of Osteoarthritis in Dogs: A Prospective, Randomized, Controlled Study

 , ,
, ,  ,
,  ,
,  ,
,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Eligibility Criteria and Dogs’ Enrollment
2.3. Clinical Trial Procedures
2.4. Anesthesiological Protocol
2.5. Control Group Therapy (Hyaluronic Group)
2.6. Study Group Therapy (MFAT Group)
2.7. Canine Brief Pain Inventory
2.8. Clinical Examination
2.9. Radiographic Examination
2.10. Synovial Fluid Examination
2.11. Synovial Cytokine Assay
2.12. Statistical Analysis
3. Results
3.1. Enrolled Patients
3.2. Short-Term Outcome
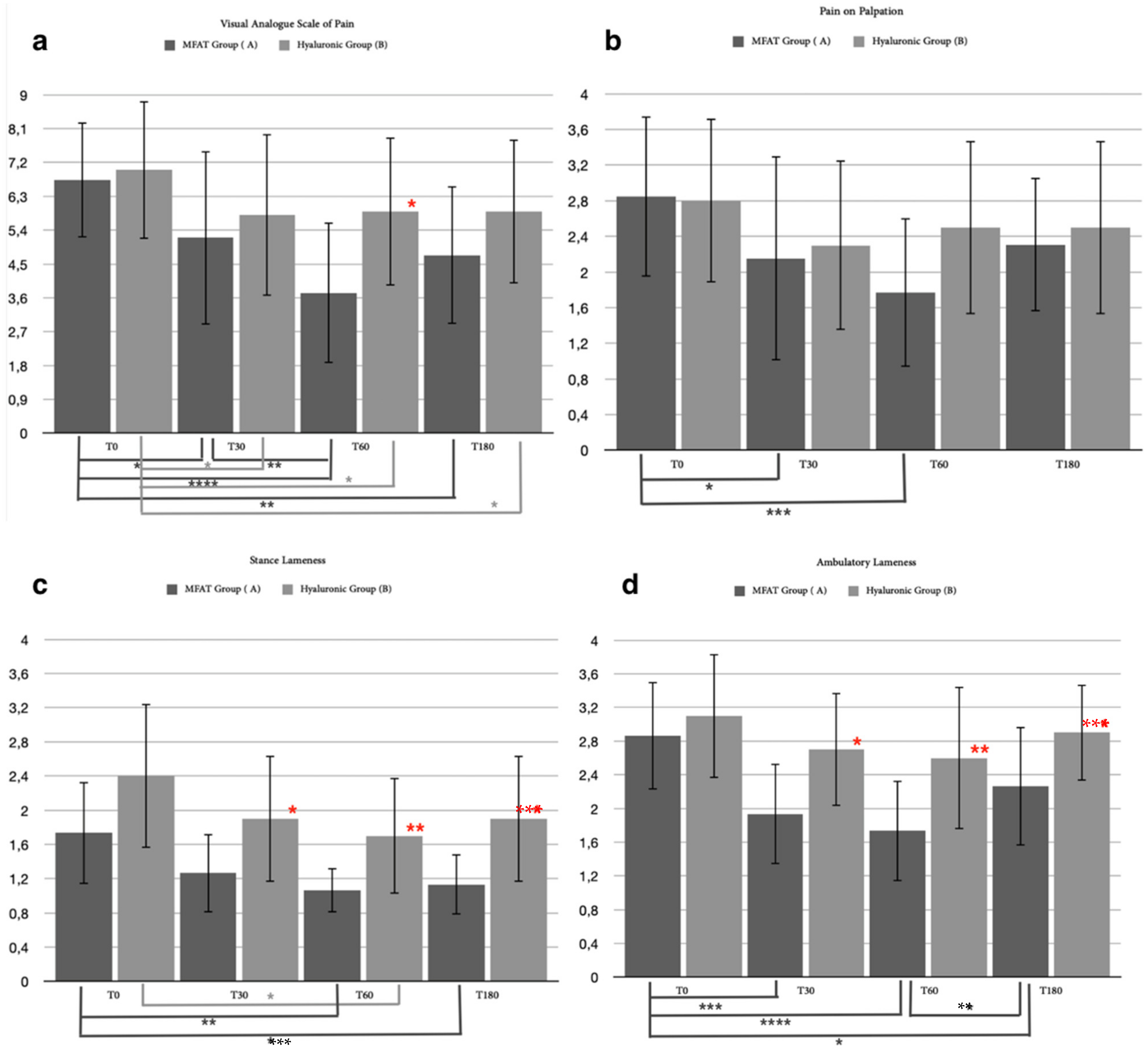
3.2.1. Clinical Examination
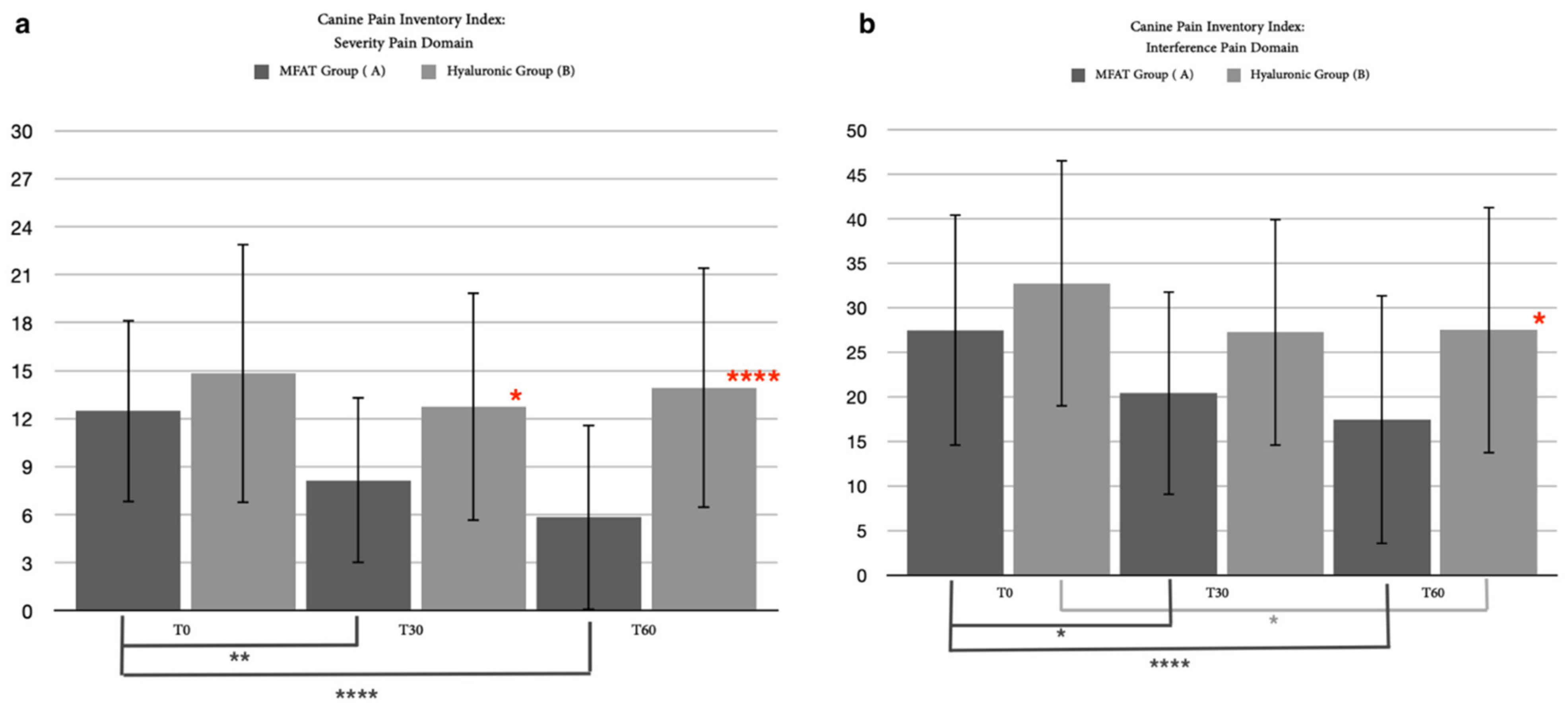
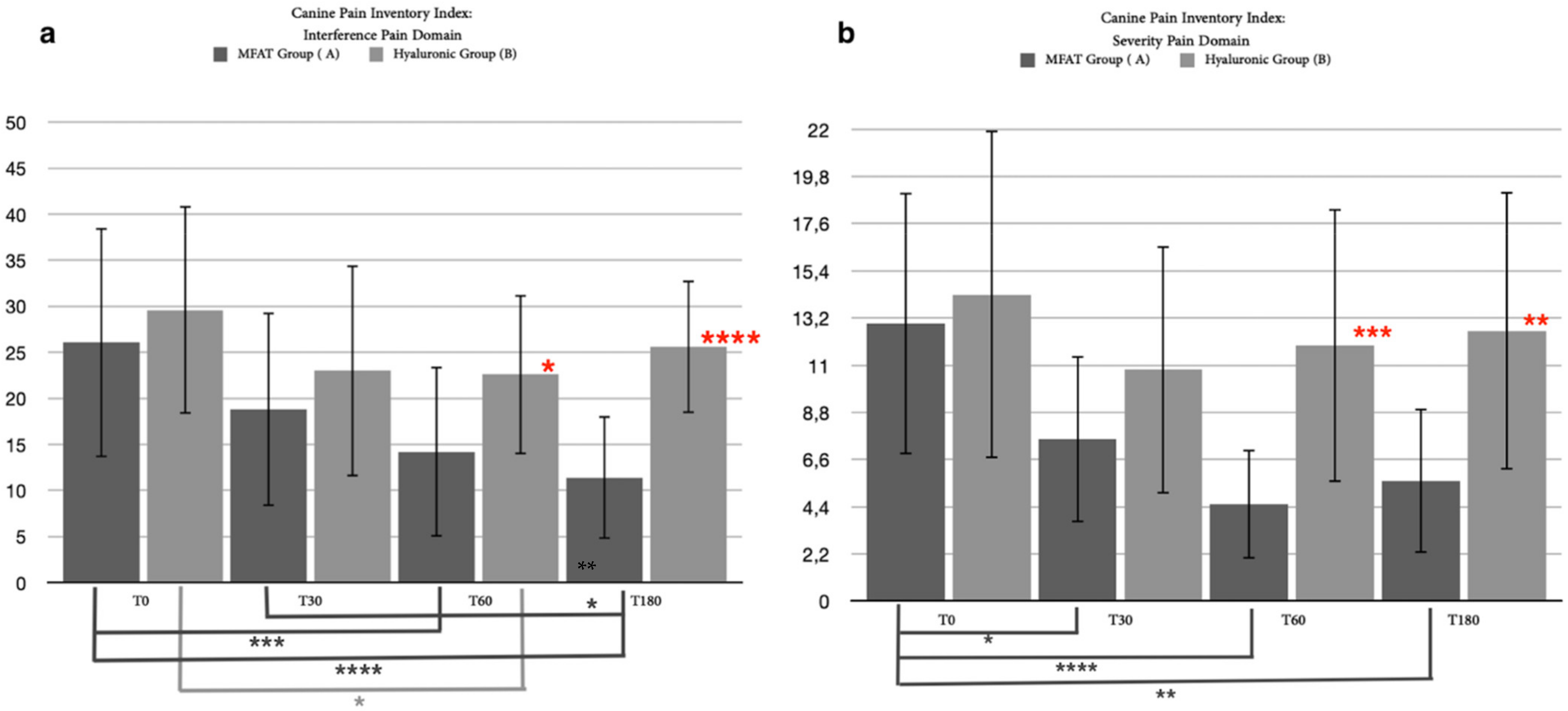
3.2.2. Canine Brief Pain Inventory Index (CBPI)
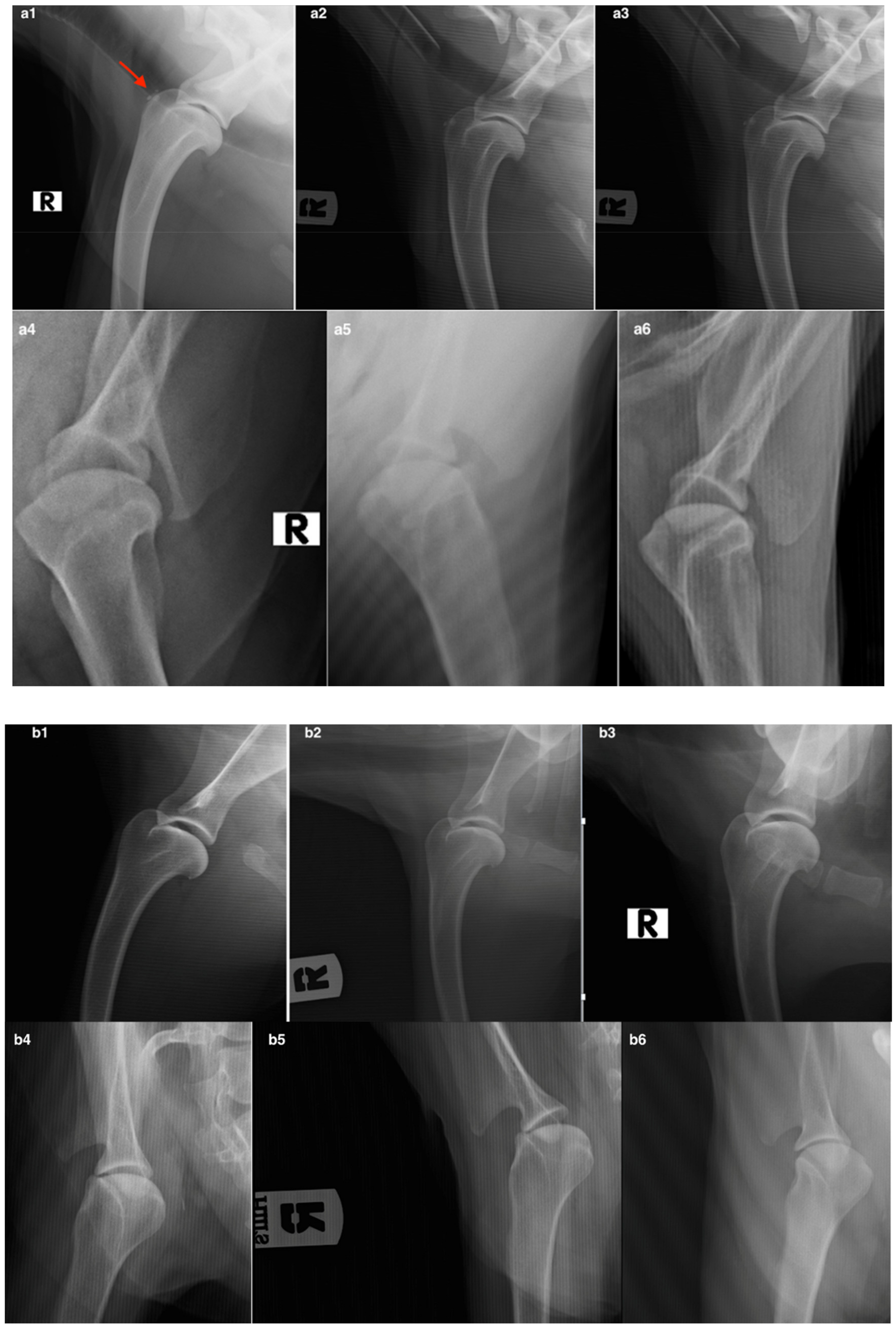
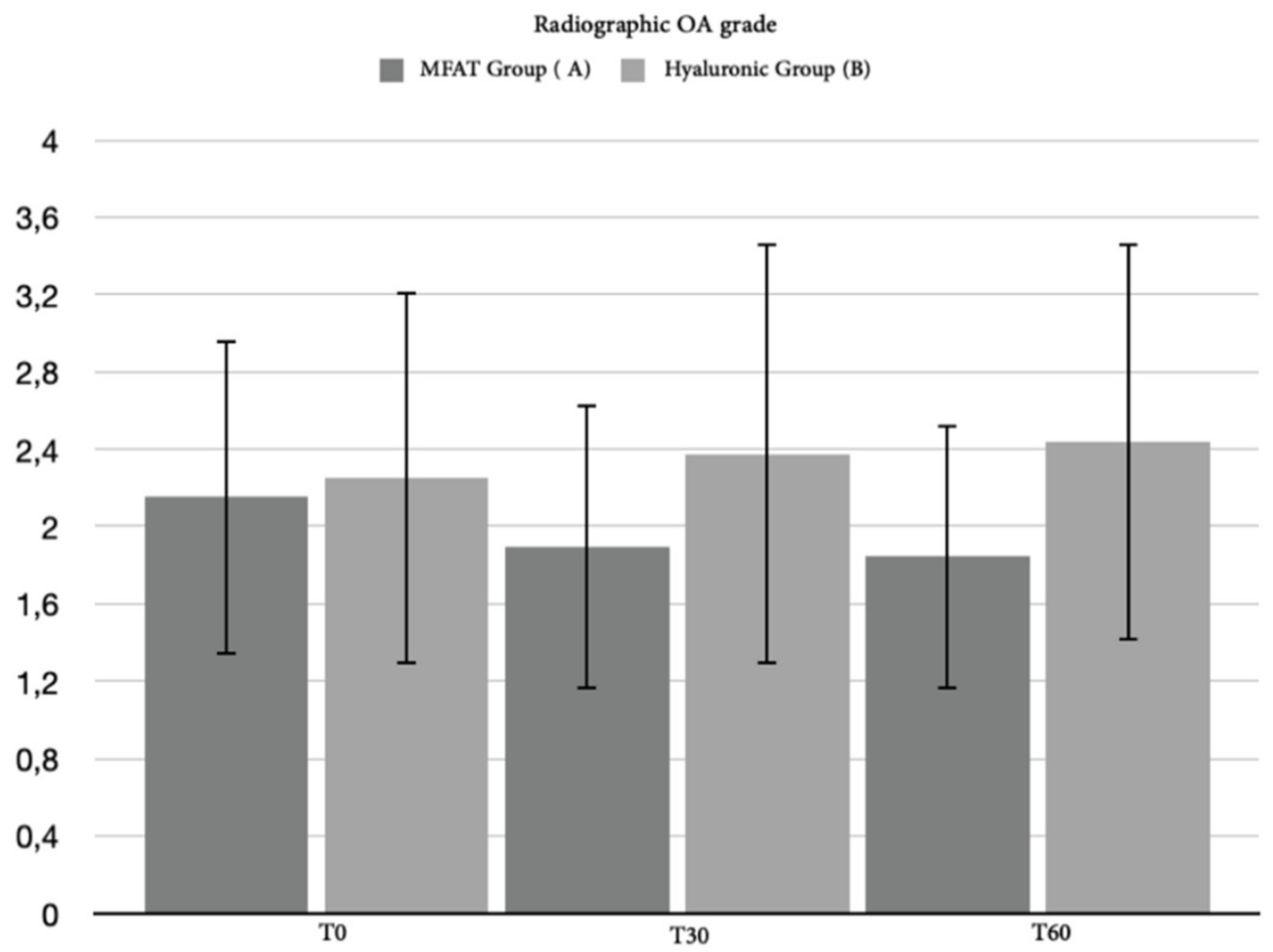
3.2.3. Radiographic Assessment
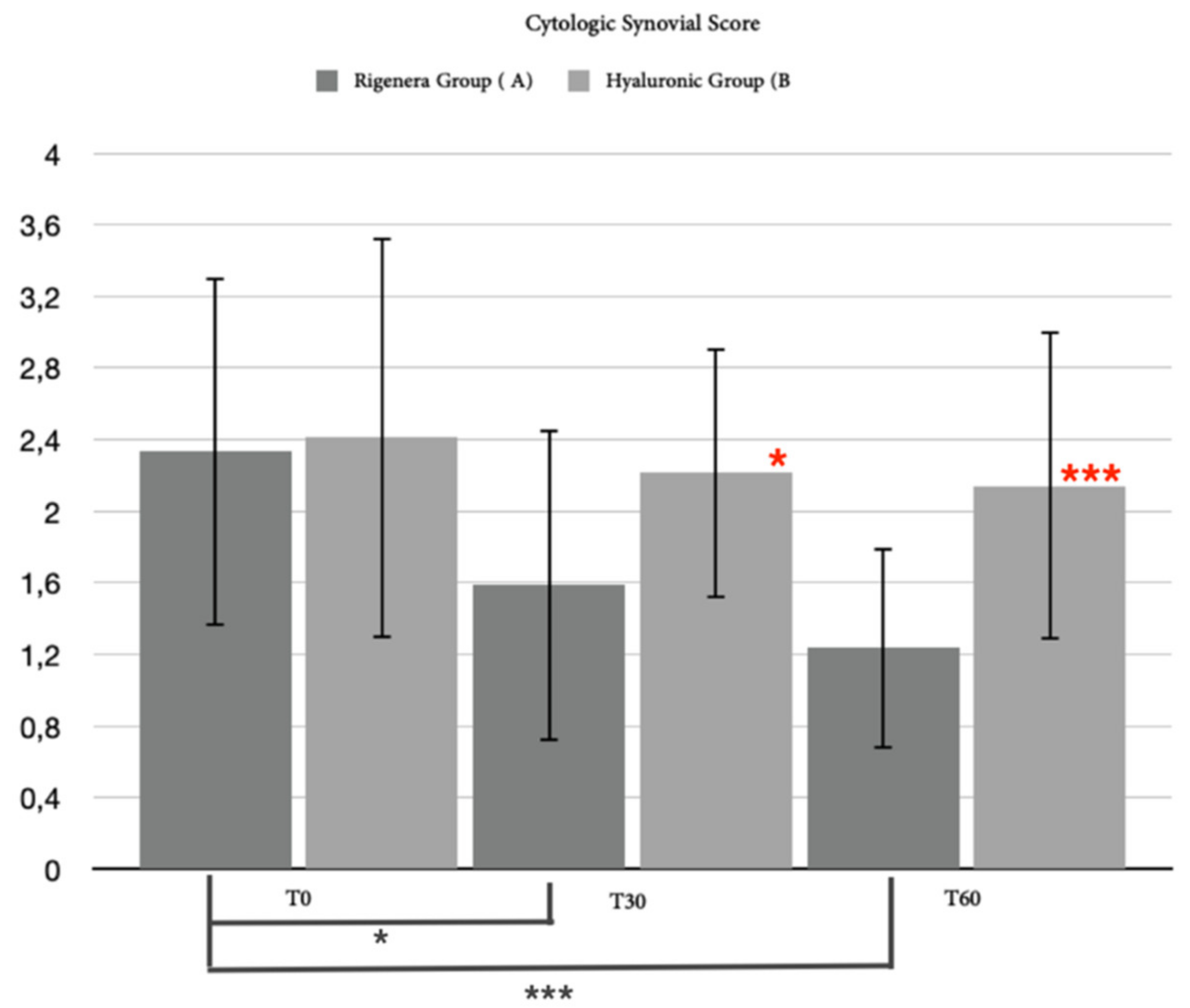
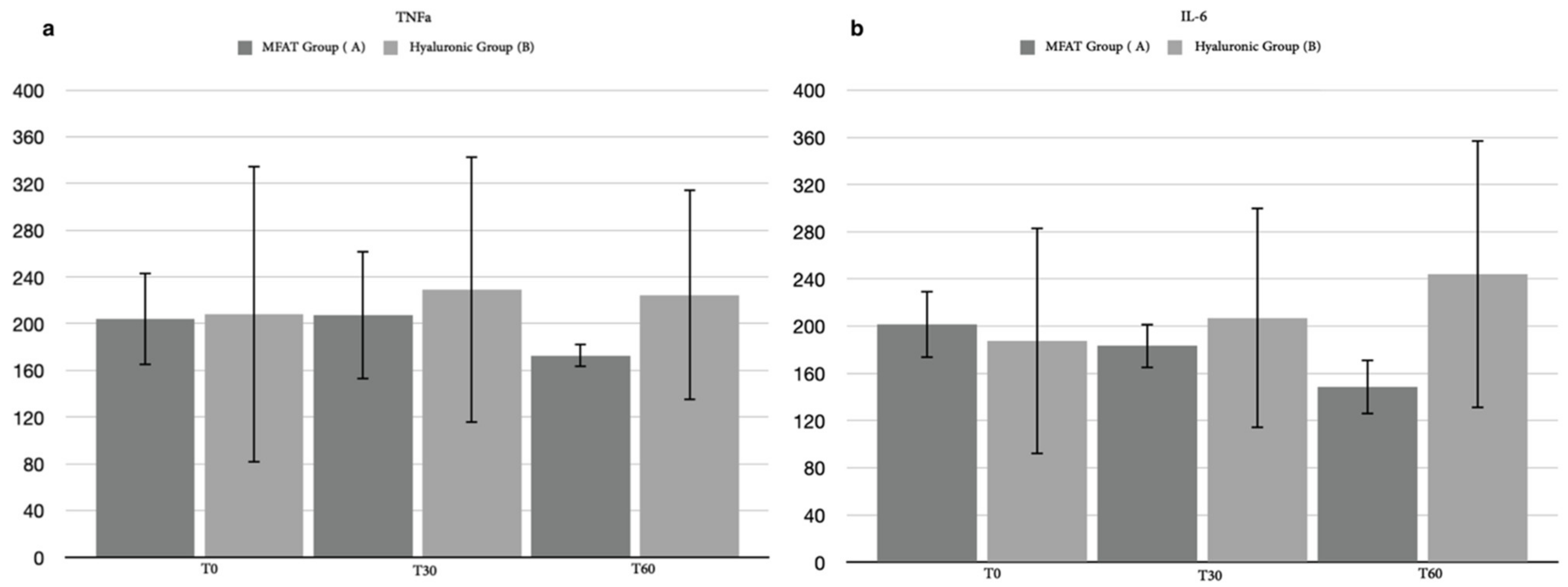
3.2.4. Synovial Assessment
3.3. Long-Term Outcome
3.3.1. Clinical Examination
3.3.2. Canine Brief Pain Inventory Index
3.3.3. Excluded Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smith, G.K.; Paster, E.R.; Powers, M.Y.; Lawler, D.F.; Biery, D.N.; Shofer, F.S.; McKelvie, P.J.; Kealy, R.D. Lifelong diet restriction and radiographic evidence of osteoarthritis of the hip joint in dogs. J. Am. Vet. Med. Assoc. 2006, 229, 690–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, M.R.; Lee, H.B.; Kim, M.S.; Kim, N.S. Surgical model of osteoarthritis secondary to medial patellar luxation in dogs. Vet. Med. 2011, 56, 123–130. [Google Scholar] [CrossRef] [Green Version]
- McCoy, A.M. Animal Models of Osteoarthritis: Comparisons and Key Considerations. Vet. Pathol. 2015, 52, 803–818. [Google Scholar] [CrossRef] [PubMed]
- Murphy, L.; Helmick, C.G. The impact of osteoarthritis in the United States: A population-health perspective: A population- based review of the fourth most common cause of hospitalization in U.S. adults. Orthop. Nurs. 2012, 31, 85–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aragon, C.L.; Hofmeister, E.H.; Budsberg, S.C. Systematic review of clinical trials of treatments for osteoarthritis in dogs. J. Am. Vet. Med. Assoc. 2007, 230, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Gregory, M.H.; Capito, N.; Kuroki, K.; Stoker, A.M.; Cook, J.L.; Sherman, S.L. A review of translational animal models for knee osteoarthritis. Arthritis 2012, 2012, 764621. [Google Scholar] [CrossRef] [PubMed]
- Meeson, R.L.; Todhunter, R.J.; Blunn, G.; Nuki, G.; Pitsillides, A.A. Spontaneous dog osteoarthritis—A One Medicine vision. Nat. Rev. Rheumatol. 2019, 15, 273–287. [Google Scholar] [CrossRef]
- Rychel, J.K. Diagnosis and treatment of osteoarthritis. Top. Companion Anim. Med. 2010, 25, 20–25. [Google Scholar] [CrossRef]
- Lachiewicz, P.F.; Soileau, E.S. Fifteen-year survival and osteolysis associated with a modular posterior stabilized knee replace-ment. A concise follow-up of a previous report. J. Bone Jt. Surg. Am. 2009, 91, 1419–1423. [Google Scholar] [CrossRef]
- Zhang, W.; Ouyang, H.; Dess, C.R.; Xu, J. Current research on pharmacologic and regenerative therapies for osteoarthritis. Bone Res. 2016, 4, 15040. [Google Scholar] [CrossRef]
- Lee, M.I.; Kim, J.H.; Kwak, H.H.; Woo, H.M.; Han, J.H.; Yayon, A.; Jung, Y.C.; Cho, J.M.; Kang, B.J. A placebo-controlled study comparing the efficacy of intra-articular injections of hyaluronic acid and a novel hyaluronic acid-platelet-rich plasma conjugate in a caninemodel of osteoarthritis. J. Orthop. Surg. Res. 2019, 14, 314. [Google Scholar] [CrossRef]
- Voga, M.; Adamic, N.; Vengust, M.; Majdic, G. Stem Cells in Veterinary Medicine-Current State and Treatment Options. Front. Vet. Sci. 2020, 7, 278. [Google Scholar] [CrossRef]
- Lodi, D.; Iannitti, T.; Palmieri, B. Stem cells in clinical practice: Applications and warnings. J. Exp. Clin. Cancer Res. 2011, 30, 9. [Google Scholar] [CrossRef] [Green Version]
- Senesi, L.; De Francesco, F.; Farinelli, L.; Manzotti, S.; Gagliardi, G.; Papalia, G.F.; Riccio, M.; Gigante, A. Mechanical and Enzymatic procedures to isolate the stromal vascular fraction from adipose tissue: Preliminary results. Front. Cell Dev. Biol. 2019, 7, 88. [Google Scholar] [CrossRef]
- Friedenstein, A.J.; Piatetzky-Shapiro, I.I.; Petrakova, K.V. Osteogenesis in transplants of bone marrow cells. J. Embryol. Exp. Morphol. 1966, 16, 381–390. [Google Scholar] [CrossRef]
- Pittenger, M.F.; Mackay, A.M.; Beck, S.C.; Jaiswal, R.K.; Douglas, R.; Mosca, J.D.; Moorman, M.A.; Simonetti, D.W.; Craig, S.; Marshak, D.R. Multilineage potential of adult human mesenchymal stem cells. Science 1999, 284, 143–147. [Google Scholar] [CrossRef] [Green Version]
- Zuk, P.A.; Zhu, M.; Mizuno, H.; Huang, J.; Futrell, J.W.; Katz, A.J.; Benhaim, P.; Lorenz, H.P.; Hedrick, M.H. Multilineage cells from human adipose tissue: Implications for cell-based therapies. Tissue Eng. 2001, 7, 211–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bieback, K.; Kern, S.; Kluter, H.; Eichler, H. Critical parameters for the isolation of mesenchymal stem cells from umbilical cord blood. Stem Cells 2004, 22, 625–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erices, A.; Conget, P.; Minguell, J.J. Mesenchymal progenitor cells in human umbilical cord blood. Br. J. Haematol. 2000, 109, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, H.S.; Bicknese, A.R.; Chien, S.N.; Bogucki, B.D.; Quinn, C.O.; Wall, D.A. Multilineage differentiation activity by cells isolated from umbilical cord blood: Expression of bone, fat, and neural markers. Biol. Blood Marrow Transpl. 2001, 7, 581–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kogler, G.; Sensken, S.; Airey, J.A.; Trapp, T.; Muschen, M.; Feldhahn, N.; Liedtke, S.; Sorg, R.V.; Fischer, J.; Rosenbaum, C. A new human somatic stem cell from placental cord blood with intrinsic pluripotent differentiation potential. J. Exp. Med. 2004, 200, 123–135. [Google Scholar] [CrossRef] [Green Version]
- Zvaifler, N.J.; Marinova-Mutafchieva, L.; Adams, G.; Edwards, C.J.; Moss, J.; Burger, J.A.; Maini, R.N. Mesenchymal precursor cells in the blood of normal individuals. Arthritis Res. Ther. 2000, 2, 477–488. [Google Scholar] [CrossRef] [Green Version]
- Kuznetsov, S.A.; Mankani, M.H.; Gronthos, S.; Satomura, K.; Bianco, P.; Robey, P.G. Circulating skeletal stem cells. J. Cell Biol. 2001, 153, 1133–1140. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Vaessen, B.; Lenvik, T.; Blackstad, M.; Reyes, M.; Verfaillie, C.M. Multipotent progenitor cells can be isolated from postnatal murine bone marrow, muscle, and brain. Exp. Hematol. 2002, 30, 896–904. [Google Scholar] [CrossRef]
- Marshall, C.D.; Brett, E.A.; Moore, A.L.; Wan, D.C.; Longaker, M.T. In Vitro and In Vivo Osteogenic Differentiation of Human Adipose-Derived Stromal Cells; Bone Morphogenetic Proteins; Humana Press: New York, NY, USA, 2019; Volume 1891, pp. 9–18. [Google Scholar] [CrossRef]
- Wagner, W.; Wein, F.; Seckinger, A.; Frankhauser, M.; Wirkner, U.; Krause, U.; Blake, J.; Schwager, C.; Eckstein, V.; Ansorge, W.; et al. Comparative characteristics of mesenchymal stem cells from human bone marrow, adipose tissue, and umbilical cord blood. Exp. Hematol. 2005, 33, 1402–1416. [Google Scholar] [CrossRef]
- De Francesco, F.; Ricci, G.; D’Andrea, F.; Nicoletti, G.F.; Ferraro, G.A. Human adipose stem cells: From bench to bedside. Tissue Eng Part B Rev. 2015, 21, 572–584. [Google Scholar] [CrossRef] [Green Version]
- Bora, P.; Majumdar, A.S. Adipose tissue-derived stromal vascular fraction in regenerative medicine: A brief review on biology and translation. Stem Cell Res. Ther. 2017, 8, 1–10. [Google Scholar] [CrossRef]
- Aronowitz, J.A.; Lockhart, R.A.; Hakakian, C.S. Mechanical versus enzymatic isolation of stromal vascular fraction cells from adipose tissue. SpringerPlus 2015, 4, 713. [Google Scholar] [CrossRef] [Green Version]
- Vinatier, C.; Guicheux, J. Cartilage tissue engineering: From biomaterials and stem cells to osteoarthritis treatments. Ann. Phys. Rehabil. Med. 2016, 59, 139–144. [Google Scholar] [CrossRef]
- Zimmerlin, L.; Donnenberg, V.S.; Rubin, J.P.; Donnenberg, A.D. Mesenchymal markers on human adipose stem/progenitor cells. Cytom. Part A 2013, 83, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Bourin, P.; Bunnell, B.A.; Casteilla, L.; Dominici, M.; Kats, A.J.; March, K.L.; Redl, H.; Rubin, J.P.; Yoshimura, K.; Gimble, M.J. Stromal cells from the adipose tissue-derived stromal vascular fraction and culture expanded adipose tissue-derived stromal/stem cells: A joint statement of the International Federation of Adipose Therapeutics (IFATS) and Science and International Society fro Cellular Therapy (ISCT). Cytotherapy 2013, 15, 641–648. [Google Scholar] [CrossRef] [Green Version]
- Hurley, E.T.; Yasui, Y.; Gianakos, A.L.; Seow, D.; Shimozono, Y.; Kerkhoffs, G.; Kennedy, J.G. Limited evidence for adipose-derived stem cell therapy on the treatment of osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3499–3507. [Google Scholar] [CrossRef]
- Zeira, O.; Scaccia, S.; Pettinari, L.; Ghezzi, E.; Asiag, N.; Martinelli, L.; Zahirpour, D.; Dumas, M.P.; Konar, M.; Lupi, D.M.; et al. Intra-articular administration of autologous micro-fragmented adipose tissue in dogs with spontaneous osteoarthritis: Safety, feasibility, and clinical outcomes. Stem Cells Transl. Med. 2018, 7, 819–828. [Google Scholar] [CrossRef] [Green Version]
- Purpura, V.; Bondioli, E.; Graziano, A.; Trovato, L.; Melandri, D.; Ghetti, M.; Marchesini, A.; Cusella De Angelis, M.G.; Benedetti, L.; Ceccarelli, G.; et al. Tissue Characterization after a new disaggregation method for skin micro-grafts generation. J. Vis. Exp. 2016, 4, e53579. [Google Scholar] [CrossRef] [Green Version]
- Svolacchia, F.; De Francesco, F.; Trovato, L.; Graziano, A.; Ferraro, G.A. An innovative regenerative treatment of scars with dermal micrografts. J. Cosmet. Dermatol. 2016, 15, 245–253. [Google Scholar] [CrossRef]
- Tremolada, C.; Colombo, V.; Ventura, C. Adipose Tissue and Mesenchymal Stem Cells: State of the Art and Lipogems® Technology Development. Curr. Stem Cell Rep. 2016, 2, 304–312. [Google Scholar] [CrossRef] [Green Version]
- Mudumbai, C.S.; Pershing, S.; Bowe, T.; Kamal, R.N.; Sears, E.D.; Finlay, A.K.; Eisenberg, D.; Hawn, M.T.; Weng, Y.; Trickey, A.W.; et al. Development and validation of a predictive model for American Society of Anesthesiologist Physical Status. BMC Health Serv. Res. 2019, 19, 859. [Google Scholar] [CrossRef] [Green Version]
- Kohn, M.D.; Sassoon, A.A.; Fernando, N.D. Classification in brief: Kellgren-Lawrence classification of osteoarthritis. Clin. Orthop. Relat. Res. 2016, 474, 1886–1893. [Google Scholar] [CrossRef] [Green Version]
- Brown, D.C.; Boston, R.C.; Coyne, J.C.; Farrar, J.T. Ability of the Canine Brief Pain Inventory to detect response to treatment in dogs with osteoarthritis. J. Am. Vet. Med. Assoc. 2008, 233, 1278. [Google Scholar] [CrossRef] [Green Version]
- Vasseur, P.B.; Johnson, A.L.; Budsberg, S.C.; Lincoln, J.D.; Toombs, J.P.; Whitehair, J.G.; Lentz, E.L. Rabdomized, controlled trial of the efficacy of carprofen, a nonsteroidal anti-inflammatory drug, in the treatment of osteoarthritis in dogs. J. Am. Vet. Med. Assoc. 1995, 206, 807. [Google Scholar]
- Hudson, J.T.; Slater, M.R.; Taylor, L.; Scott, H.M.; Kerwin, S.C. Assessing repeatability and validity of a visual analogue scale questionnaire for use in assessing pain and lameness in dogs. Am. J. Vet. Res. 2004, 65, 1634. [Google Scholar] [CrossRef] [PubMed]
- Haraden, C.A.; Huebner, J.L.; Hsueh, M.; Li, Y.J.; Kraus, V.B. Synovial fluid biomarkers associated with osteoarthritis severity reflect macrophage and neutrophil related inflammation. Arthritis Res. Ther. 2019, 21, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Udomsinprasert, W.; Jinawath, A.; Teerawattanapong, N.; Honsawek, S. Interleukin-34 overexpression mediated through tumor necrosis factor-alpha reflect severity of synovitis in knee osteoarthritis. Sci. Rep. 2020, 10, 7987. [Google Scholar] [CrossRef] [PubMed]
- Watkins, A.; Fasanello, D.; Stefanovki, D.; Schurer, S.; Caracappa, K.; D’Agostino, A.; Costello, E.; Free, H.; Rollins, A.; Read, C.; et al. Investigation of synovial fluid lubricants and inflammatory cytokines in the horse: A comparison of recombinant equina interleukin 1 beta- induced synovitis and joint lavage models. BMC Vet. Res. 2021, 17, 189. [Google Scholar] [CrossRef]
- Proschowsky, H.F.; Rugbjerg, H.; Ersboll, A.K. Mortality of purebred and mixed-breed dogs in Denmark. Prev. Vet. Med. 2003, 58, 63–74. [Google Scholar] [CrossRef]
- Malm, S.; Fikse, F.; Egenvall, A.; Bonnett, B.N.; Gunnarsson, L.; Hedhammar, A.; Strandberg, E. Association between radiographic assessment of hip status and subsequent incidence of veterinary care and mortality related to hip dysplasia in insured Swedish dogs. Prev. Vet. Med. 2010, 93, 222–232. [Google Scholar] [CrossRef]
- Grassel, S.; Muschter, D. Recent advances in the treatment of osteoarthritis. F1000 Res. 2020, 9, 325. [Google Scholar] [CrossRef]
- Belshaw, Z.; Dean, R.; Asher, L. Could it be osteoarthritis? How dog owners and veterinary surgeons describe identifying canine osteoarthritis in a general practice setting. Prev. Vet. Med. 2020, 185, 105198. [Google Scholar] [CrossRef]
- Malfait, A.M.; Little, C.B. On the predictive utility of animal models of osteoarthritis. Arthritis Res. Ther. 2015, 17, 225. [Google Scholar] [CrossRef] [Green Version]
- Haas, E.M.; Volkmer, E.; Giunta, R.E. Pilot study on the effects and benefits of autologous fat grafting in osteoarthritis of the CMC- 1 joint compared to intraarticular cortisone injection: Results after 3 months. Handchir. Mikrochir. Plast. Chir. 2017, 49, 288–296. [Google Scholar] [CrossRef]
- Kemper, R.; Wirth, J.; Baur, E.M. Arthroscopic synovectomy combined with autologous fat grafting in early stages of CMC osteoarthritis of the thumb. J. Wrist Surg. 2018, 7, 165–171. [Google Scholar] [CrossRef]
- Herold, C.; Rennekampff, H.O.; Groddeck, R.; Allert, S. Autologous fat transfer for thumb carpometacarpal joint osteoarthritis: A prospective study. Plast. Reconstr. Surg. 2017, 140, 327–335. [Google Scholar] [CrossRef]
- Bohr, S.; Rennekampff, H.O.; Pallua, N. Cell-enriched lipoaspirate arthroplasty: A novel approach to first carpometacarpal joint arthritis. Hand Surg. 2015, 20, 479–481. [Google Scholar] [CrossRef]
- Erne, H.C.; Cerny, M.K.; Ehrl, D.; Bauer, A.T.; Schmauss, V.; Moog, P.; Broer, P.N.; Loew, S.; Schmauss, D. Autologous fat injection versus Lundborg resection arthroplasty for the treatment of trape- ziometacarpal joint osteoarthritis. Plast. Reconstr. Surg. 2018, 141, 119–124. [Google Scholar] [CrossRef]
- Cattaneo, G.; De Caro, A.; Napoli, F.; Chiapale, D.; Trada, P.; Camera, A. Micro-fragmented adipose tissue injection associated with arthroscopic procedures in patients with symptomatic knee osteoarthritis. BMC Musculoskelet. Disord. 2018, 19, 176. [Google Scholar] [CrossRef]
- Si, Z.; Wang, X.; Sun, C.; Kang, Y.; Xu, J.; Wang, X.; Hui, Y. Adipose-derived stem cells: Sources, potency, and implications for regenerative therapies. Biomed. Pharm. 2019, 114, 108765. [Google Scholar] [CrossRef]
- Vezzani, B.; Shaw, I.; Lesme, H.; Yong, L.; Khan, N.; Tremolada, C.; Peault, B. Higher Pericyte Content and Secretory Activity of Microfragmented Human Adipose Tissue Compared to Enzymatically Derived Stromal Vascular Fraction. Stem Cells Transl. 2018, 7, 876–886. [Google Scholar] [CrossRef] [Green Version]
- Van den Brink, S.C.; Sage, F.; Vértesy, Á.; Spanjaard, B.; Peterson-Maduro, J.; Baron, C.S.; Robin, C.; van Oudenaarden, A. Single-cell sequencing reveals dissociation induced gene expression in tissue subpopulations. Nat. Methods 2017, 14, 935–936. [Google Scholar] [CrossRef]
- Garcia-Contreras, M.; Messaggio, F.; Jimenez, O.; Mendez, A. Differences in exosome content of human adipose tissue pro- cessed by non-enzymatic and enzymatic methods. CellR4 2015, 3, 1423. [Google Scholar]
- Quintero, E.C.; Escriva Machado, J.F.; Damian Robles, R.A. Meek micrografting history, indications, technique, physiology and experience: A review article. J. Wound Care. 2018, 27, 12–18. [Google Scholar] [CrossRef]
- De Francesco, F.; Mannucci, S.; Conti, G.; Dai Prè, E.; Sbarbati, A.; Riccio, M. A Non-Enzymatic Method to Obtain a Fat Tissue Derivative Highly Enriched in Adipose Stem Cells (ASCs) from Human Lipoaspirates: Preliminary Results. Int. J. Mol. Sci. 2018, 19, 2061. [Google Scholar] [CrossRef] [Green Version]
- Dai Prè, E.; Busato, A.; Mannucci, S.; Vurro, F.; De Francesco, F.; Riccio, V.; Solito, S.; Biswas, R.; Bernardi, P.; Riccio, M.; et al. In Vitro Characterization of Adipose Stem Cells Non-Enzymatically Extracted from the Thigh and Abdomen. Int. J. Mol. Sci. 2020, 21, 3081. [Google Scholar] [CrossRef]
- Palumbo Piccionello, A.; Riccio, V.; Senesi, L.; Volta, A.; Pennasilico, L.; Botto, R.; Tambella, A.M.; Galosi, L.; Marini, C.; Vullo, C.; et al. Adipose micro-grafts enhance tendinopathy healing in ovine model: An in vivo experimental perspective study. STEM Cells Transl. Med. 2021, 10, 1544–1560. [Google Scholar] [CrossRef]
- Pennasilico, L.; Di Bella, C.; Botto, R.; Murgia, E.; Riccio, V.; Palumbo Piccionello, A. Use of micro-grafts in a chronic infected open wound after limb amputation in a cat. Czech. Acad. Agric. Sci. 2021, 10, 448–455. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Gentile, P.; Marcarelli, M.; Balli, M.; Ronzoni, F.L.; Benedetti, L.; De Angelis, M.G.C. In vitro and in vivo studies of alar-nasal catilage using autologous micro-grafts: The use of the Rigenera® protocol in the treatment of an osteochondral lesion of the nose. Pharmaceuticals 2017, 10, 53. [Google Scholar] [CrossRef] [Green Version]
- Riccio, M.; Marchesini, A.; Zingaretti, N.; Carella, S.; Senesi, L.; Onesti, M.G.; Parodi, P.C.; Ribuffo, D.; Vaienti, L.; De Francesco, F.A. Multicentre study: The use of micrografts in the reconstruction of full-thickness posttraumatic skin defects of the limbs—A whole innovative concept in regenerative surgery. Stem Cells 2019, 2019, 5043518. [Google Scholar] [CrossRef]
- Astarita, C.; Arora, C.L.; Trovato, L. Tissue regeneration: An overview from stell cells to micrografts. J. Int. Med. Res. 2020, 48, 300060520914794. [Google Scholar] [CrossRef]
- Gentile, P.; Scioli, M.G.; Bielli, A.; Orlandi, A.; Cervelli, V. Reconstruction of aler nasal cartilage defects using a tissue engineering technique based on a combined use of autologous chondrocyte micrografts and platelet-rich plasma: Preliminary clinical and instrumental evaluation. Plast. Reconstr. Surg. Glob. Open 2016, 4, e1027. [Google Scholar] [CrossRef]
- Miotti, G.; Zingaretti, N.; Guarneri, F.; Manfrè, V.; Erricchetti, E.; Stinco, G.; Parodi, P.C. Autologous micrografts and methotrexate in plantar erosive lichen planus: Healing and pain control. A case report. Plast. Surg. Hand Surg. 2020, 7, 134–138. [Google Scholar] [CrossRef]
- Gentile, P.; Scioli, M.G.; Bielli, A.; De Angelis, B.; De Sio, C.; De Fazio, D.; Ceccarelli, G.; Trivisonno, A.; Orlandi, A.; Cervelli, V.; et al. Platelet-rich plasma and micrografts enriched with autologous human follicle mesenchymal stem cells improve hair regrowth in androgenetic alopecia. Biomolecular pathway analysis and clinical evaluation. Biomedicines 2019, 7, 27. [Google Scholar] [CrossRef] [Green Version]
- Marcarelli, M.; Zappia, M.; Risollio, L.; Baroni, C.; Astarita, C.; Trovato, L.; Graziano, A. Cartilage micrografts as a novel non-invasive and non-arthroscopic autograft procedure fro knee chondropathy: Three-year follow-up study. J. Clin. Med. 2021, 10, 322. [Google Scholar] [CrossRef] [PubMed]
- Abu-Ghname, A.; Perdanasari, A.T.; Reece, E.M. Principles and applications of fat grafting in plastic surgery. Semin. Plast. Surg. 2019, 33, 147–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Francesco, F.; Gravina, P.; Busato, A.; Farinelli, L.; Soranzo, C.; Vidal, L.; Zingaretti, N.; Zavan, B.; Sbarbati, A.; Riccio, M.; et al. Stem cells in autologous microfragmented apidose tissue: Current perspectives in osteoarthritis disease. Int. J. Mol. Sci. 2021, 22, 10197. [Google Scholar] [CrossRef] [PubMed]
- Brunelli, G.; Motroni, A.; Graziano, A.; D’Aquino, R.; Zollini, I.; Carinci, F. Sinus lift tissue engineering using autologous pulp micro-grafts: A casa report of bone density evaluation. J. Indian Soc. Periodontol. 2013, 17, 644–647. [Google Scholar] [CrossRef]
- Marcarelli, M.; Trovato, L.; Novarese, E.; Riccio, M.; Graziano, A. Rigenera protocol in the treatment of surgical wound dehiscence. Int. Wuond J. 2017, 14, 277–281. [Google Scholar] [CrossRef]
- De Francesco, F.; Riccio, V.; Busato, A.; Di Bella, C.; Serri, E.; Sbarbati, A.; Zavan, B.; Riccio, M.; Piccionello, A.P. In vitro characterization of canine microfragmented adipose tissue non-enzymatically extracted from the thigh and lumbar. Animals 2021, 11, 3231. [Google Scholar] [CrossRef]
- Carapeba, G.O.L.; Cavaleti, P.; Nicácio, G.M.; Brinholi, B. Intra-articular hyaluronic acid compared to traditional conservative treatment in dogs with osteoarthritis associated with hip dysplasia. Evid. Based Complement. Alternat. Med. 2016, 2016, 2076921. [Google Scholar] [CrossRef] [Green Version]
- Hellström, L.E.; Carlsson, C.; Boucher, J.F.; Michanek, P. Intra-articular injections with high molecular weight sodium hyaluronate as a therapy for canine arthritis. Vet. Rec. 2003, 153, 89–90. [Google Scholar] [CrossRef]
- Lattimer, J.C.; Selting, K.A.; Lunceford, J.M.; Holland, J.R.; Simon, J.; Stevenson, N.R.; Doerr, C.A. Intraarticular injection of a Tin-117 m radiosynoviorthesis agent in normal canine elbows causes no adverse effects. Vet. Radiol. Ultrasound 2019, 60, 567–574. [Google Scholar] [CrossRef]
- Pavarotti, G.S.; Hivernaud, V.; Brincin, M.; Roche, R.; Barreau, P.; Festy, F.; Gauthier, O. Evaluation of a Single Intra-Articular Injection of Autologous Adipose Tissue for the Treatment of Osteoarthritis: A Prospective Clinical Study in Dogs. Vet. Comp. Orthop. Traumatol. 2020, 33, 258–266. [Google Scholar] [CrossRef]
- Russo, A.; Condello, V.; Madonna, V.; Guerriero, M.; Zorzi, C. Autologous and micro-fragmented adipose tissue for the treatment of diffuse degenerative knee osteoarthtritis. J. Exp. Orthop. 2017, 4, 33. [Google Scholar] [CrossRef]
- Hudetz, D.; Boric, I.; Rod, E.; Jelec, Z.; Radic, A.; Vrdoljak, T.; Skelin, A.; Lauc, G.; Trbojevic-Akmacic, I.; Plecko, M.; et al. The effect of intra-articular injection of autologous microfragmented fat tissue on proteoglycan synthesis in patients with knee osteoarthritis. Genes 2017, 8, 270. [Google Scholar] [CrossRef] [Green Version]
- Yokota, N.; Yamakawa, M.; Shirata, T.; Kimura, T.; Kaneshima, H. Clinical results following intra-articular injection of adipose-derived stomal vascular fraction cells in patients with osteoarthritis of the knee. Regen. Ther. 2017, 6, 108–122. [Google Scholar] [CrossRef]
- Munana, K.; Zhang, D.; Patterson, E.E. Placebo effect in canine epilepsy trials. J. Vet. Intern. Med. 2010, 24, 166–170. [Google Scholar] [CrossRef]
- Conzemius, M.G.; Evans, R.B. Caregiver placebo effect for dogs with lameness from osteoarthritis. J. Am. Vet. Med. Assoc. 2012, 241, 1314–1319. [Google Scholar] [CrossRef]
- Kim, S.H.; Djaja, Y.P.; Park, Y.B.; Park, J.G.; Ko, Y.B.; Ha, C.W. Intra-articular Injection of Culture-Expanded Mesenchymal Stem Cells Without Adjuvant Surgery in Knee Osteoarthritis: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2020, 48, 2839–2849. [Google Scholar] [CrossRef]
- German, A.J.; Hervera, A.; Hunter, L.; Holden, S.L.; Morris, P.J.; Biourge, V.; Trayhurn, P. Improvement in insulin resistance and reduction in plasma inflammatory adipokines after weight loss in obese dogs. Domest. Anim. Endocrinol. 2009, 37, 214. [Google Scholar] [CrossRef]
- Eisele, I.; Wood, I.S.; German, A.J.; Hunter, L.; Trayhurn, P. Adipokine gene expression in dog adipose tissues and dog white adipocytes differentiated in primary culture. Horm. Metab. Res. 2005, 37, 474–481. [Google Scholar] [CrossRef]
- Trayhurn, P.; Wood, I.S. Adipokines: Inflammation and the pleiotropic role of white adipose tissue. Br. J. Nutr. 2004, 92, 347–355. [Google Scholar] [CrossRef] [Green Version]
- Muir, P.; Hans, E.C.; Racette, M.; Volstad, N.; Sample, S.J.; Heaton, C.; Holzman, G.; Schaefer, S.L.; Bloom, D.D.; Bleedorn, J.A.; et al. Autologous Bone Marrow-Derived Mesenchymal Stem Cells Modulate Molecular Markers of Inflammation in Dogs with Cruciate Ligament Rupture. PLoS ONE 2016, 11, e0159095. [Google Scholar] [CrossRef] [Green Version]
- Allen, P.I.; Conzemius, M.G.; Evans, R.B.; Kiefer, K. Correlation between synovial fluid cytokine concentrations and limb function in normal dogs and in dogs with lameness from spontaneous osteoarthritis. Vet. Surg. 2019, 48, 770–779. [Google Scholar] [CrossRef]
- Kleine, S.A.; Gogal, R.M.; George, C.; Thaliath, M.; Budsberg, S.C. Elevated Synovial Fluid Concentration of Monocyte Chemoattractant Protein-1 and Interleukin-8 in Dogs with Osteoarthritis of the Stifle. Vet. Comp. Orthop. Traumatol. 2020, 33, 147–150. [Google Scholar] [CrossRef]
- Kleine, S.A.; Gogal, R.M.; Krunkosky, T.M.; Sanderson, S.L.; George, C.; Norton, M.; Budsberg, S.C. Resistin concentrations in serum and stifle synovial fluid from normal and cruciate deficient dogs with osteoarthritis. Vet. Surg. 2020, 49, 1164–1173. [Google Scholar] [CrossRef]
- Sun, M.; He, Y.; Zhou, P.; Gao, J.; Lu, F. Adipose extracellular matrix/stromal vascular fraction gel secretes angiogenic factors and enhances skin would healing in a murine model. Biomed. Res. Int. 2017, 2017, 1–11. [Google Scholar] [CrossRef]
- Casadei, A.; Epis, R.; Ferroni, L.; Tocco, I.; Gardin, C.; Bressan, E.; Sivolella, S.; Vindigni, V.; Pinton, P.; Mucci, G.; et al. Adipose tissue regeneration: A state of the art. J. Biomed. Biotechnol. 2012, 2012, 462543. [Google Scholar] [CrossRef]
- Tremolada, C.; Ricordi, C.; Caplan, A.I.; Ventura, C. Mesenchymal Stem Cells in Lipogems, a Reverse Story: From Clinical Practice to Basic Science. Methods Mol. Biol. 2016, 1416, 109–122. [Google Scholar] [CrossRef]
- Elahi, F.M.; Farwell, D.G.; Nolta, J.A.; Anderson, J.D. Concise Review: Preclinical Translation of Exosomes Derived from Mesenchymal Stem/Stromal Cells. Stem Cells 2019, 38, 15–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bondeson, J. Activated synovial macrophages as targets for osteoarthritis drug therapy. Curr. Drug. Targets 2010, 11, 576. [Google Scholar] [CrossRef]
- Bondeson, J.; Lauder, S. Osteoarthritis synovial macrophages regulate the production of proinflammatory cytokines and matrix metalloproteinases via interleukin-1 and tumor necrosis factor alpha. Arthritis Rheum. 2004, 50, S279. [Google Scholar]
- Lust, G.; Summers, B.A. Early, asymptomatic stage of degenerative joint disease in canine hip joints. Am. J. Vet. Res. 1981, 42, 1849–1855. [Google Scholar]
- Pelletier, J.P.; Martel-Pelletier, J.; Ghandur-Mnaymneh, L.; Howell, D.S.; Woessner Jr, J.F. Role of synovial membrane inflammation in cartilage matrix breakdown in the Pond–Nuki dog model of osteoarthritis. Arthritis Rheumatol. 1985, 28, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Brandt, K.D.; Myers, S.L.; Burr, D.; Albrecht, M. Osteoarthritic changes in canine articular cartilage, subchondral bone, and synovium fifty- four months after transection of the anterior cruciate ligament. Arthritis Rheum. 1991, 34, 1560. [Google Scholar] [CrossRef] [PubMed]
- Hewicker-Trautwein, M.; Carter, S.D.; Bennett, D.; Kelly, D.F. Immunocytochemical demonstration of lymphocyte subsets and MHC class II antigen expression in synovial membranes from dogs with rheumatoid arthritis and degenerative joint disease. Vet. Immunol. Immunopathol. 1999, 67, 341. [Google Scholar] [CrossRef]
- Lemburg, A.K.; Meyer-Lindenberg, A.; Hewicker-Trautwein, M. Immunohistochemical characterization of inflammatory cell populations and adhesion molecule expression in synovial membranes from dogs with spontaneous cranial cruciate ligament rupture. Vet. Immunol. Immunopathol. 2004, 97, 231. [Google Scholar] [CrossRef]
- Sasaki, A.; Mizuno, M.; Ozeki, N.; Katano, H.; Otabe, K.; Tsuji, K.; Koga, H.; Mochizuki, M.; Sekiya, I. Canine mesenchymal stem cells from synovium have a higher chondrogenic potential than those from infrapatellar fat pad, adipose tissue, and bone marrow. PLoS ONE 2018, 13, e0202922. [Google Scholar] [CrossRef] [Green Version]
- Gruen, M.E.; Myers, J.A.E.; Lascelles, B.D.X. Efficacy and Safety of an Anti-nerve Growth Factor Antibody (Frunevetmab) for the Treatment of Degenerative Joint Disease-Associated Chronic Pain in Cats: A Multisite Pilot Field Study. Front. Vet. Sci. 2021, 8, 610028. [Google Scholar] [CrossRef]
- Wise, B.L.; Seidel, M.F.; Lane, N.E. The evolution of nerve growth factor inhibition in clinical medicine. Nat. Rev. Rheumatol. 2021, 17, 34–46. [Google Scholar] [CrossRef]
- Tazawa, R.; Kenmoku, T.; Uchida, K.; Arendt-Nielsen, L.; Nagura, N.; Nakawaki, M.; Matsumoto, T.; Inoue, G.; Takeuchi, H.; Jimbo, T. Increased nerve growth factor expression in the synovial tissues of patients with rotator cuff tears. Mol. Pain 2021, 17, 17448069211021252. [Google Scholar] [CrossRef]
- Kendall, A.; Nyström, S.; Ekman, S.; Hultén, L.M.; Lindahl, A.; Hansson, E.; Skiöldebrand, E. Nerve growth factor in the equine joint. Vet. J. 2021, 267, 105579. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trial Procedure | T0 (Start Trial) | T1 (30 Days) | T2 (60 Days) | T3 (180 Days) |
|---|---|---|---|---|
| Canine Brief Pain Inventory | X | X | X | X |
| Specialistic clinician assessment | X | X | X | X |
| Radiographic examination | X | X | X | |
| Synovial fluid examination | X | X | X | |
| Synovial Assay Test | X | X | X | |
| Intra-articular injection control group | X | |||
| Intra-articular injection study group | X |
| Walk/Trot | Clinical Signs |
|---|---|
| I | No lameness noted at a work or trot |
| II | No lameness at a walk, mild lameness at a trot |
| III | Mild lameness at a walk, significant lameness at a trot |
| IV | Significant lameness at a walk, non-weight-bearing at trot |
| V | Non-weight-bearing lameness at a walk and a trot |
| Standing | |
| I II III IV V | Normal weight-bearing at a stance Mild decrease in weight-bearing at a stance Significant decrease in weight-bearing at a stance Occasional toe-touching at a stance Holds limb off the ground at a stance |
| Contralateral LIMB | |
| I II III IV V | Readily accepts contralateral limb being held up and bears full weight on affected limb Offers resistance to elevation of contralateral limb but bears full weight on affected limb for more than 1 minute after contralateral limb is elevated Offers moderate resistance to elevation of contralateral limb and replaces it after 30 s Offers resistance to elevation of contralateral limb and replaces it after 10 s Refuses to raise contralateral limb |
| Pain on Palpation | |
| I II III IV V | No sign of pain during palpation of affected joint/bone Sign of mild pain during palpation of affected joint/bone; dog turns head in recognition Sign of moderate pain during palpation of affected joint/bone; dog pulls limb away Sign of severe pain during palpation of affected joint/bone; dog vocalizes or becomes aggressive Dog will not allow examiner to palpate joint |
| Radiographic Sign | 0 | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|
| Osteophytes | Absence | <1 mm | 1–2 mm | 2–3 mm | >3 mm |
| Bone sclerosis | Absence | Localized | Pervasive | ||
| Joint narrowing and/or incongruence | Absence | Mild <25% | Moderate 25–50% | Serious >50% | Joint deformity |
| Capsular ectasia | Absence | Evident | |||
| Final Score | 0 | 1–3 | 4–6 | 7–9 | >10 |
| Oa Grade | 0 | 1 | 2 | 3 | 4 |
| Cytologic Sign | 1 | 2 | 3 | |
|---|---|---|---|---|
| Inflammatory cells | Absence | Average prevalence | High prevalence | |
| Synovial cells | Absence | Average prevalence | High prevalence | |
| Cartilage fragments | Absence | Average prevalence | High prevalence | |
| Blood contamination | Absence | Average prevalence | High prevalence | |
| Matrix | Absence | Average prevalence | High prevalence | |
| Final Score | 1–2 | 3–5 | 6–9 | >10 |
| Synovial Score of OA | 1 Paraphysiological synovial fluid | 2 Mild inflammation of the synovial fluid | 3 Medium inflammation of the synovial fluid | 4 Severe inflammation of the synovial fluid |
| Patient | QuickCalcks (Random Generator) | Bread | Weight (kg) | Sex | Age | BCS | Joint Affected by OA |
|---|---|---|---|---|---|---|---|
| 1 | A | Mixed breed | 17 | F/OE | 7 | 7 | Left shoulder |
| 2 | B | Pit bull | 27 | M | 4 | 5 | Right shoulder |
| 3 | A | Mixed breed | 21 | F/OE | 6 | 8 | Right shoulder |
| 4 | B | Mixed breed | 18 | M/N | 13 | 6 | Left elbow |
| 5 | A | Armstaff | 25 | F/OE | 6 | 5 | Left stifle |
| 6 | B | Maremma shepherd | 47 | M | 6 | 7 | Right tarsus |
| 7 | A | Mixed breed | 31 | F/OE | 5 | 8 | Right stifle |
| 8 | B | German sheperd | 32 | F | 10 | 5 | Left elbow |
| 9 | A | Labrador retriever | 41 | F | 7 | 8 | Right shoulder |
| 10 | B | Mixed breed | 26 | M | 11 | 3 | Left stifle |
| 11 | A | Mixed breed | 10 | M | 12 | 8 | Right hip |
| 12 | B | Labrador retriever | 39 | M | 12 | 8 | Right shoulder |
| 13 | B | Mixed breed | 15 | F/OE | 10 | 5 | Left stifle |
| 14 | B | Golden retriever | 36 | F/OE | 3 | 6 | Left hip |
| 15 | A | Mixed breed | 12 | F | 7 | 8 | Left hip |
| 16 | B | Golden retriever | 40 | M | 5 | 7 | Right hip |
| 17 | B | Labrador retriever | 36 | F | 8 | 8 | Right shoulder |
| 18 | B | Mixed breed | 27 | F | 7 | 6 | Right stifle |
| 19 | A | Chow-Chow | 31 | F/OE | 9 | 8 | Right elbow |
| 20 | A | Samoyed | 37 | M | 10 | 8 | Left elbow |
| 21 | B | Mixed breed | 31 | M | 10 | 6 | Right stifle |
| 22 | A | Labrador retriever | 41 | M/N | 12 | 8 | Left stifle |
| 23 | B | Parson terrier | 9 | F/OE | 7 | 7 | Left stifle |
| 24 | B | Golden retriever | 27 | F | 5 | 5 | Right elbow |
| 25 | A | Labrador retriever | 38 | F/OE | 5 | 6 | Left elbow |
| 26 | A | Mixed breed | 33 | M | 6 | 6 | Left elbow |
| 27 | A | Fox terrier | 10 | M | 8 | 6 | Right shoulder |
| 28 | B | Labrador retriever | 25 | M | 7 | 3 | Right elbow |
| 29 | B | Mixed breed | 35 | F/OE | 11 | 3 | Right shoulder |
| 30 | A | Duchshound | 7 | F/OE | 8 | 6 | Left shoulder |
| 31 | A | Mixed breed | 31 | F | 9 | 3 | Right elbow |
| 32 | A | Mixed breed | 35 | M | 7 | 3 | Left elbow |
| 33 | B | Boxer | 27 | F | 8 | 3 | Left hip |
| 34 | B | Australian shepherd | 18 | M/N | 7 | 3 | Right shoulder |
| 35 | A | Dalmatian | 23 | F | 5 | 3 | Right shoulder |
| 36 | A | German shepherd | 24 | F/OE | 9 | 2 | Right hip |
| 37 | B | Maremma shepherd | 42 | M | 8 | 5 | Left shoulder |
| 38 | A | Border collie | 15 | F | 4 | 2 | Left hip |
| 39 | B | Mixed breed | 25 | F/OE | 8 | 3 | Left stifle |
| 40 | A | Mixed breed | 40 | F/OE | 8 | 3 | Right shoulder |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Botto, R.; Riccio, V.; Galosi, L.; Rossi, G.; Vincenzetti, S.; Tambella, A.M.; De Francesco, F.; Pennasilico, L.; Riccio, M.; Salvaggio, A.; et al. Effects of Intra-Articular Autologous Adipose Micrograft for the Treatment of Osteoarthritis in Dogs: A Prospective, Randomized, Controlled Study. Animals 2022, 12, 1844. https://doi.org/10.3390/ani12141844
Botto R, Riccio V, Galosi L, Rossi G, Vincenzetti S, Tambella AM, De Francesco F, Pennasilico L, Riccio M, Salvaggio A, et al. Effects of Intra-Articular Autologous Adipose Micrograft for the Treatment of Osteoarthritis in Dogs: A Prospective, Randomized, Controlled Study. Animals. 2022; 12(14):1844. https://doi.org/10.3390/ani12141844
Chicago/Turabian StyleBotto, Riccardo, Valentina Riccio, Livio Galosi, Giacomo Rossi, Silvia Vincenzetti, Adolfo Maria Tambella, Francesco De Francesco, Luca Pennasilico, Michele Riccio, Alberto Salvaggio, and et al. 2022. "Effects of Intra-Articular Autologous Adipose Micrograft for the Treatment of Osteoarthritis in Dogs: A Prospective, Randomized, Controlled Study" Animals 12, no. 14: 1844. https://doi.org/10.3390/ani12141844