
Global-, Regional-, and National-Level Impacts of the COVID-19 Pandemic on Tuberculosis Diagnoses, 2020–2021
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Statistical Analysis
3. Result
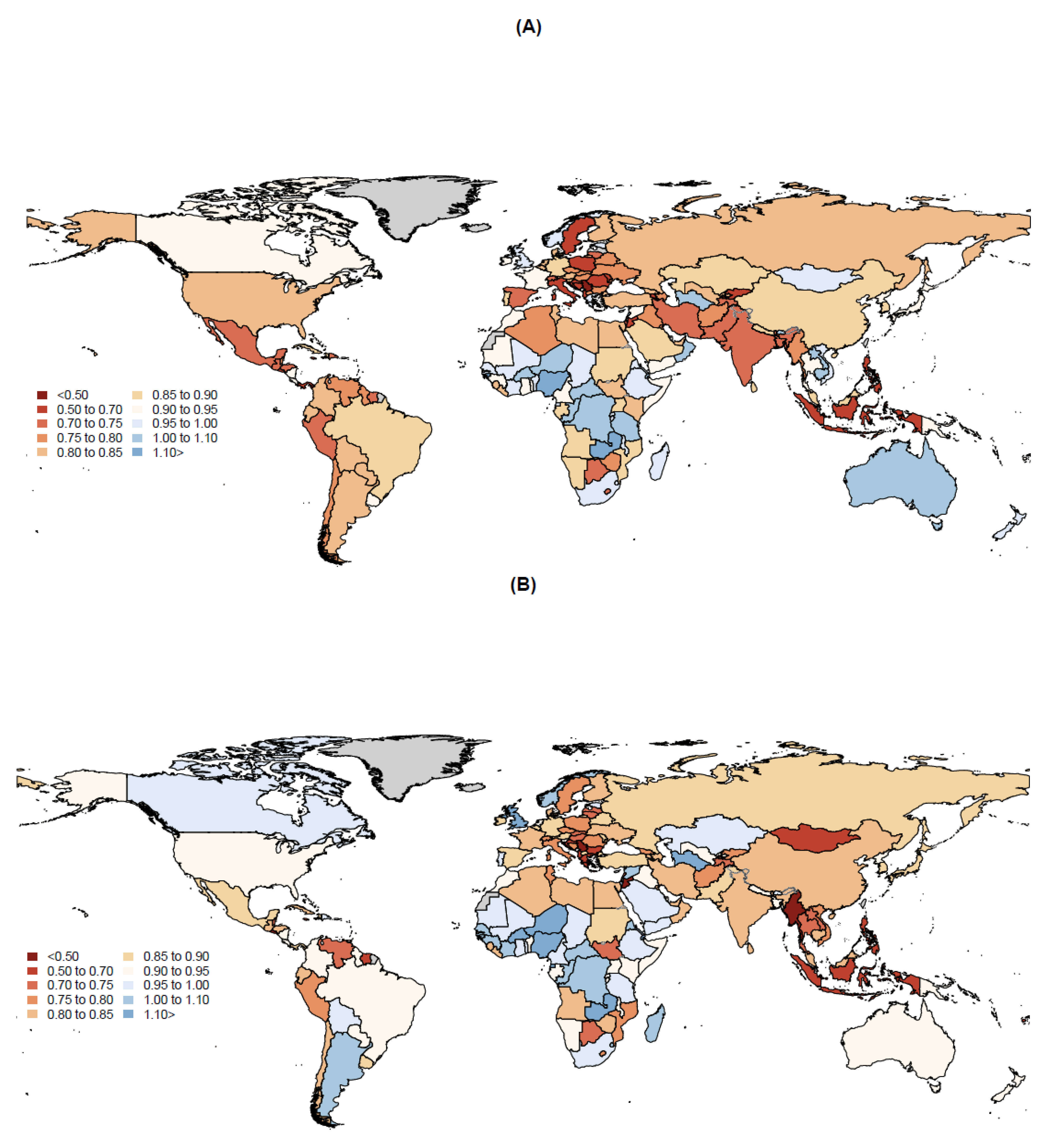
3.1. Impact of the COVID-19 Pandemic on TB Diagnoses in 2020
3.2. Impact of the COVID-19 Pandemic on TB Diagnoses in 2021
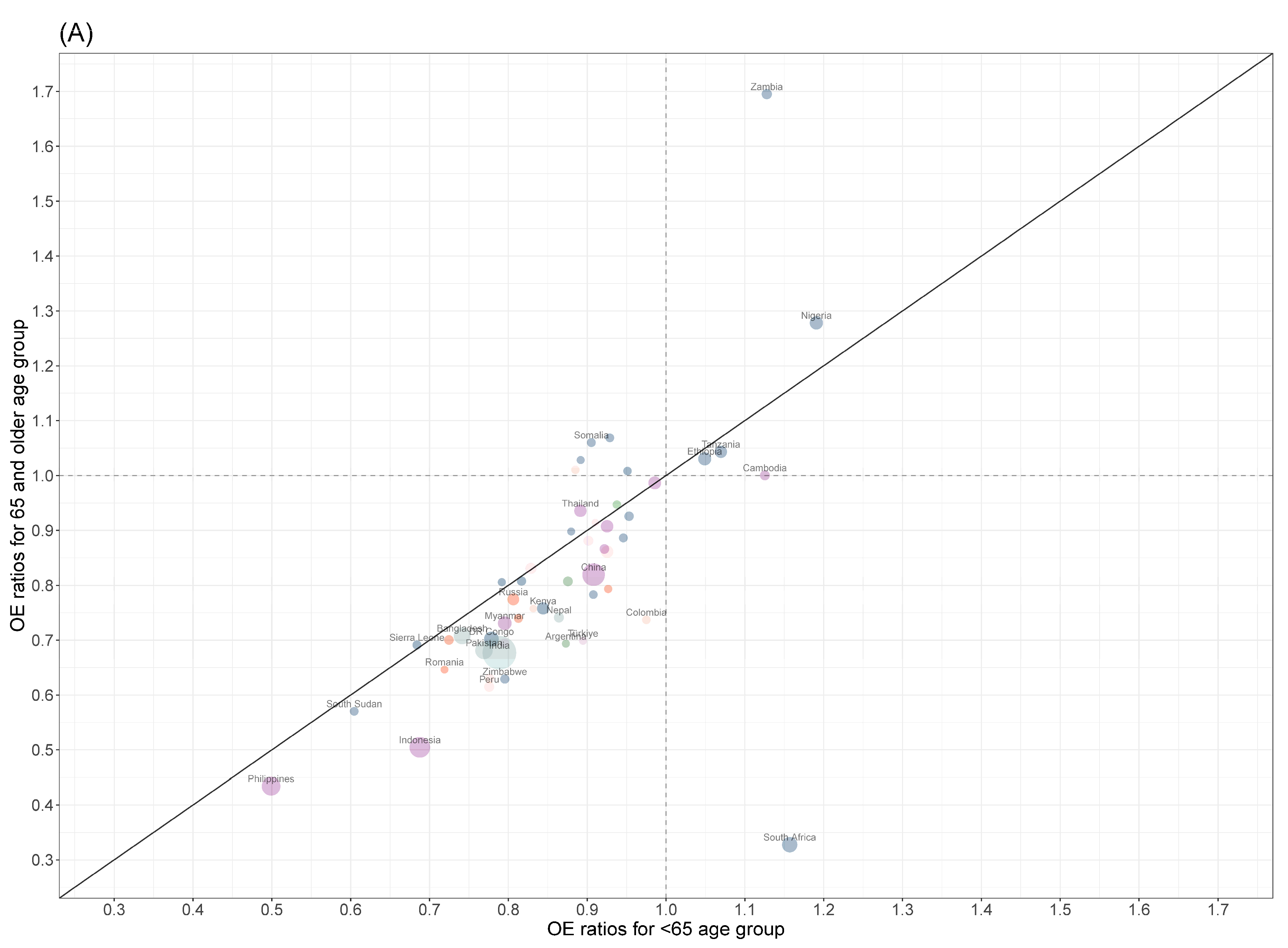
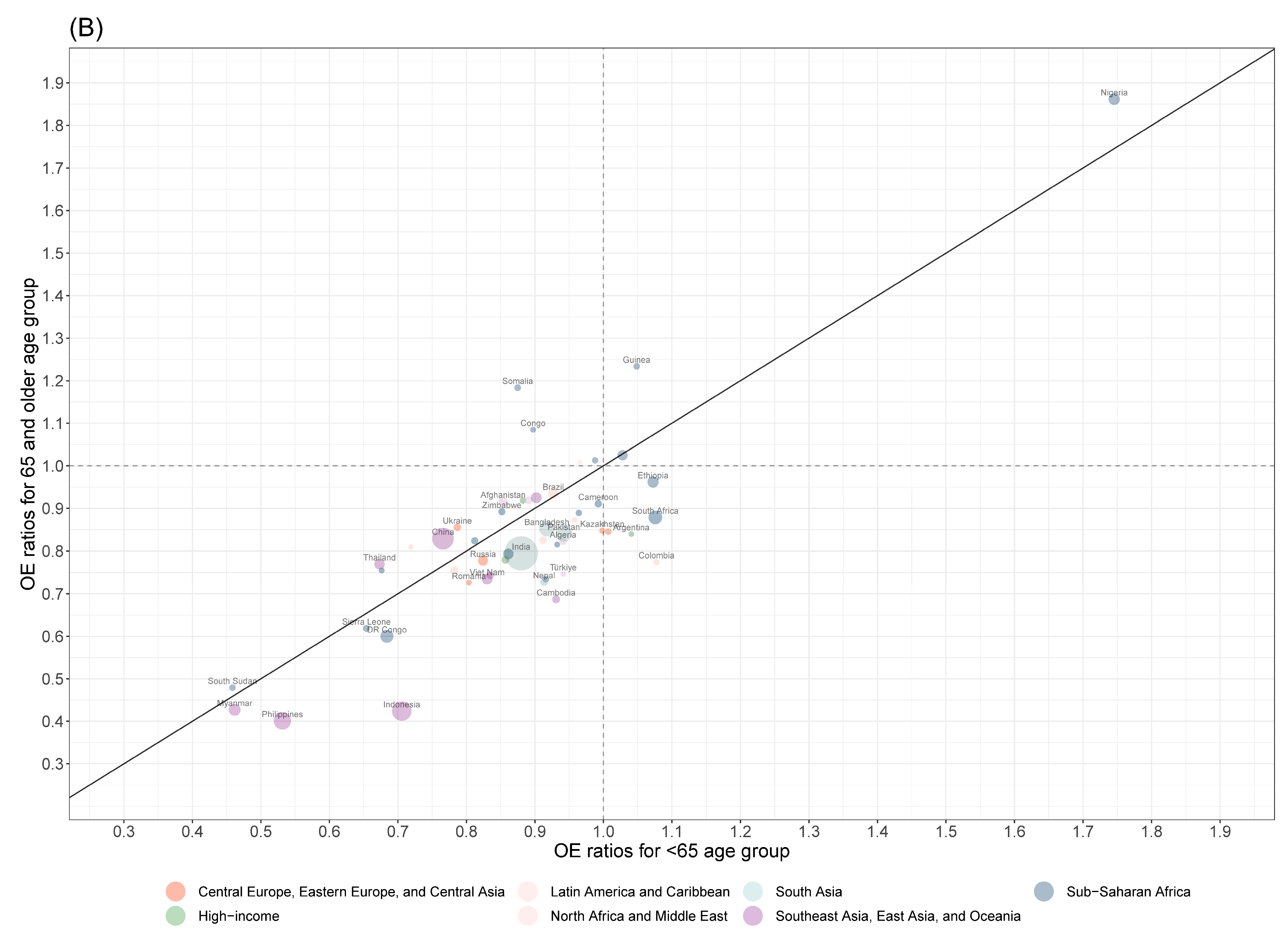
3.3. Age-Specific Impact of the COVID-19 Pandemic on TB Diagnoses
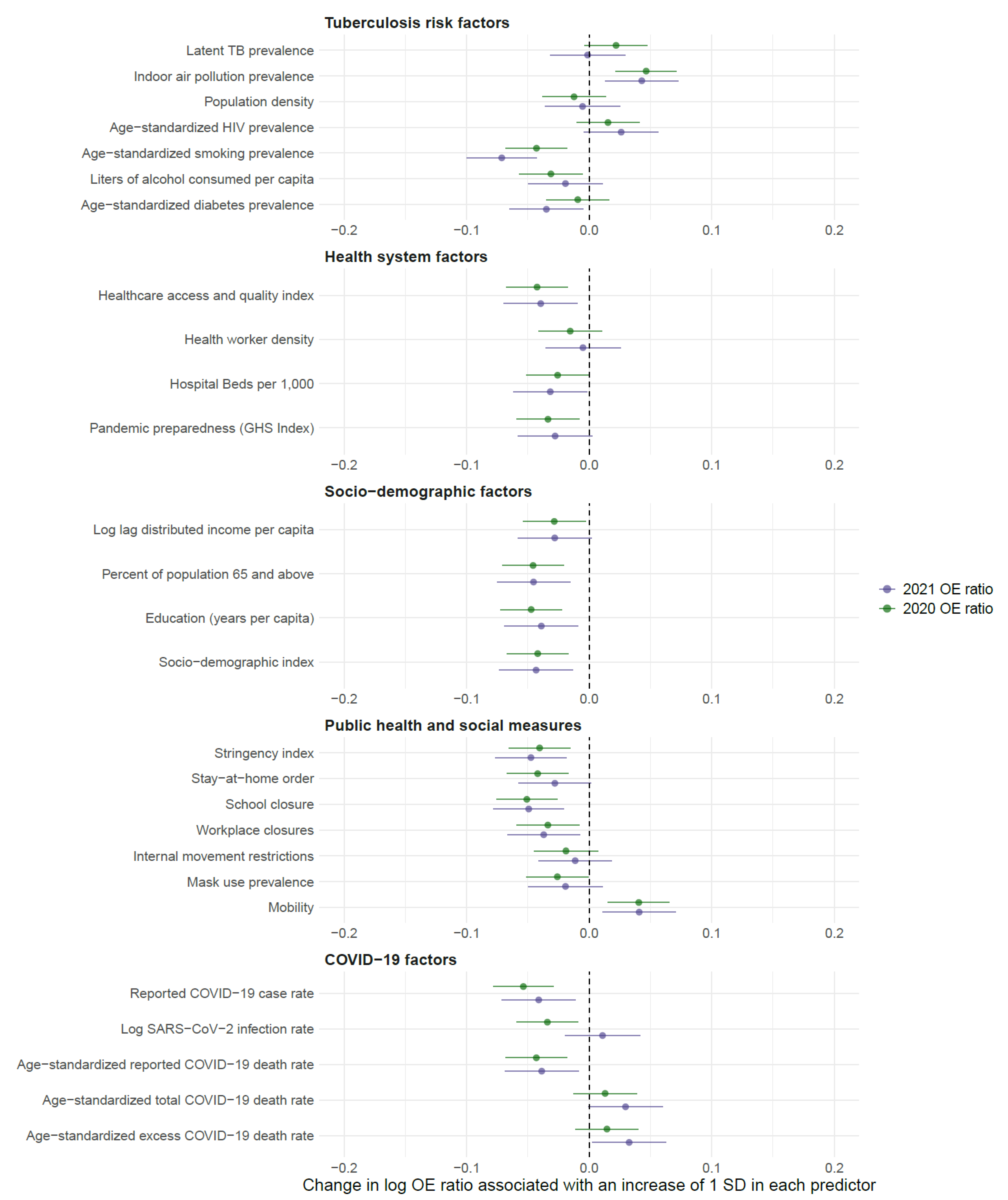
3.4. Predictors of COVID-19 Impact on TB Diagnoses
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ledesma, J.R.; Ma, J.; Vongpradith, A.; Maddison, E.R.; Novotney, A.; Biehl, M.H.; LeGrand, K.E.; Ross, J.M.; Jahagirdar, D.; Bryazka, D.; et al. Global, regional, and national sex differences in the global burden of tuberculosis by HIV status, 1990–2019: Results from the Global Burden of Disease Study 2019. Lancet Infect Dis. 2022, 22, 222–241. [Google Scholar]
- Kyu, H.H.; Maddison, E.R.; Henry, N.J.; Ledesma, J.R.; Wiens, K.E.; Reiner, R.; Biehl, M.H.; Shields, C.; Osgood-Zimmerman, A.; Ross, J.M.; et al. Global, regional, and national burden of tuberculosis, 1990–2016: Results from the Global Burden of Diseases, Injuries, and Risk Factors 2016 Study. Lancet Infect. Dis. 2018, 18, 1329–1349. Available online: https://linkinghub.elsevier.com/retrieve/pii/S147330991830625X (accessed on 12 June 2023).
- Ma, J.; Vongpradith, A.; Ledesma, J.R.; Novotney, A.; Yi, S.; Lim, K.; Hay, S.I.; Murray, C.J.L.; Kyu, H.H. Progress towards the 2020 milestones of the end TB strategy in Cambodia: Estimates of age and sex specific TB incidence and mortality from the Global Burden of Disease Study 2019. BMC Infect. Dis. 2022, 22, 904. [Google Scholar]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Zhong, N.S. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [PubMed]
- Carenzo, L.; Costantini, E.; Greco, M.; Barra, F.L.; Rendiniello, V.; Mainetti, M.; Bui, R.; Zanella, A.; Grasselli, G.; Lagioia, M.; et al. Hospital surge capacity in a tertiary emergency referral centre during the COVID-19 outbreak in Italy. Anaesthesia 2020, 75, 928–934. [Google Scholar] [CrossRef] [PubMed]
- Rehfuess, E.A.; Movsisyan, A.; Pfadenhauer, L.M.; Burns, J.; Ludolph, R.; Michie, S.; Strahwald, B. Public health and social measures during health emergencies such as the COVID-19 pandemic: An initial framework to conceptualize and classify measures. Influenza Other Respir. Viruses 2023, 17, e13110. [Google Scholar]
- Moynihan, R.; Sanders, S.; Michaleff, Z.A.; Scott, A.M.; Clark, J.; To, E.J.; Jones, M.; Kitchener, E.; Fox, M.; Johansson, M.; et al. Impact of COVID-19 pandemic on utilisation of healthcare services: A systematic review. BMJ Open 2021, 11, e045343. [Google Scholar]
- KC, A.; Gurung, R.; Kinney, M.V.; Sunny, A.K.; Moinuddin, M.; Basnet, O.; Paudel, P.; Bhattarai, P.; Subedi, K.; Shrestha, M.P.; et al. Effect of the COVID-19 pandemic response on intrapartum care, stillbirth, and neonatal mortality outcomes in Nepal: A prospective observational study. Lancet Glob. Health 2020, 8, e1273–e1281. [Google Scholar] [CrossRef]
- Causey, K.; Fullman, N.; Sorensen, R.J.D.; Galles, N.C.; Zheng, P.; Aravkin, A.; Danovaro-Holliday, M.C.; Martinez-Piedra, R.; Sodha, S.V.; Velandia-González, M.P.; et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: A modelling study. Lancet 2021, 398, 522–534. [Google Scholar] [CrossRef]
- Magnani, C.; Azzolina, D.; Gallo, E.; Ferrante, D.; Gregori, D. How Large Was the Mortality Increase Directly and Indirectly Caused by the COVID-19 Epidemic? An Analysis on All-Causes Mortality Data in Italy. Int. J. Environ. Res. Public Health 2020, 17, 3452. [Google Scholar]
- Dahal, S.; Banda, J.M.; Bento, A.I.; Mizumoto, K.; Chowell, G. Characterizing all-cause excess mortality patterns during COVID-19 pandemic in Mexico. BMC Infect. Dis. 2021, 21, 432. [Google Scholar]
- Sabbatini, A.K.; Robicsek, A.; Chiu, S.; Gluckman, T.J. Excess Mortality Among Patients Hospitalized During the COVID-19 Pandemic. J. Hosp. Med. 2021, 16, 596–602. [Google Scholar] [PubMed]
- McQuaid, C.F.; Vassall, A.; Cohen, T.; Fiekert, K.; COVID/TB Modelling Working Group; White, R.G. The impact of COVID-19 on TB: A review of the data. Int. J. Tuberc. Lung Dis. 2021, 25, 436–446. [Google Scholar] [PubMed]
- Schiza, V.; Kruse, M.; Xiao, Y.; Kar, S.; Lovejoy, K.; Wrighton-Smith, P.; Tattersall, A. Impact of the COVID-19 pandemic on TB infection testing. Int. J. Tuberc. Lung Dis. 2022, 26, 174–176. [Google Scholar]
- Rosser, J.I.; Phiri, C.; Bramante, J.T.; Fwoloshi, S.; Kankasa, C.; Lungu, P.; Chanda, R.; Chipimo, P.; Mulenga, L.; Claassen, C.W.; et al. Impact of the COVID-19 Pandemic on Tuberculosis Testing and Treatment at a Tertiary Hospital in Zambia. Am. J. Trop. Med. Hyg. 2023, 108, 911–915. [Google Scholar] [CrossRef]
- Di Gennaro, F.; Gualano, G.; Timelli, L.; Vittozzi, P.; Di Bari, V.; Libertone, R.; Cerva, C.; Pinnarelli, L.; Nisii, C.; Ianniello, S.; et al. Increase in Tuberculosis Diagnostic Delay during First Wave of the COVID-19 Pandemic: Data from an Italian Infectious Disease Referral Hospital. Antibiotics 2021, 10, 272. [Google Scholar]
- Migliori, G.B.; Thong, P.M.; Alffenaar, J.W.; Denholm, J.; Tadolini, M.; Alyaquobi, F.; Blanc, F.-X.; Buonsenso, D.; Cho, J.-G.; Codecasa, L.R.; et al. Gauging the impact of the COVID-19 pandemic on tuberculosis services: A global study. Eur. Respir. J. 2021, 58, 2101786. [Google Scholar]
- Coutinho, I.; Alves, L.C.; Werneck, G.L.; Trajman, A. The impact of the COVID-19 pandemic in tuberculosis preventive treatment in Brazil: A retrospective cohort study using secondary data. Lancet Reg. Health-Am. 2023, 19, 100444. [Google Scholar]
- Geric, C.; Saroufim, M.; Landsman, D.; Richard, J.; Benedetti, A.; Batt, J.; Brode, S.K.; Ahmad Khan, F. Impact of COVID-19 on Tuberculosis Prevention and Treatment in Canada: A Multicenter Analysis of 10,833 Patients. J. Infect. Dis. 2022, 225, 1317–1320. [Google Scholar] [CrossRef]
- Arega, B.; Negesso, A.; Taye, B.; Weldeyohhans, G.; Bewket, B.; Negussie, T.; Teshome, A.; Endazenew, G. Impact of COVID-19 pandemic on TB prevention and care in Addis Ababa, Ethiopia: A retrospective database study. BMJ Open 2022, 12, e053290. [Google Scholar] [CrossRef]
- Magro, P.; Formenti, B.; Marchese, V.; Gulletta, M.; Tomasoni, L.R.; Caligaris, S.; Castelli, F.; Matteelli, A. Impact of the SARS-CoV-2 epidemic on tuberculosis treatment outcome in Northern Italy. Eur. Respir. J. 2020, 56, 2002665. [Google Scholar] [CrossRef] [PubMed]
- Chilot, D.; Woldeamanuel, Y.; Manyazewal, T. Real-Time Impact of COVID-19 on Clinical Care and Treatment of Patients with Tuberculosis: A Multicenter Cross-Sectional Study in Addis Ababa, Ethiopia. Ann. Glob. Health 2021, 87, 109. [Google Scholar] [PubMed]
- Jackson, P.D.; Muyanja, S.Z.; Sekitoleko, I.; Bbuye, M.; Helwig, M.; Padalkar, R.; Hammad, M.; Hopkinson, D.; Siddharthan, T. Risk factors for disruptions in tuberculosis care in Uganda during the COVID-19 pandemic. PLoS Glob. Public Health 2023, 3, e0001573. [Google Scholar]
- Soko, R.N.; Burke, R.M.; Feasey, H.R.A.; Sibande, W.; Nliwasa, M.; Henrion, M.Y.R.; Khundi, M.; Dodd, P.J.; Ku, C.C.; Kawalazira, G.; et al. Effects of Coronavirus Disease Pandemic on Tuberculosis Notifications, Malawi. Emerg. Infect. Dis. 2021, 27, 1831–1839. [Google Scholar]
- Kwak, N.; Hwang, S.S.; Yim, J.J. Effect of COVID-19 on Tuberculosis Notification, South Korea. Emerg. Infect. Dis. 2020, 26, 2506–2508. [Google Scholar] [PubMed]
- Muñiz-Salazar, R.; Le, T.; Cuevas-Mota, J.; González-Fagoaga, J.E.; Zapata-Garibay, R.; Ruiz-Tamayo, P.S.; Robles-Flores, J.; Garfein, R.S. Impact of COVID-19 on tuberculosis detection and treatment in Baja California, México. Front. Public Health 2022, 10, 921596. [Google Scholar]
- Arentz, M.; Ma, J.; Zheng, P.; Vos, T.; Murray, C.J.L.; Kyu, H.H. The impact of the COVID-19 pandemic and associated suppression measures on the burden of tuberculosis in India. BMC Infect. Dis. 2022, 22, 92. [Google Scholar]
- Kiarie, H.; Temmerman, M.; Nyamai, M.; Liku, N.; Thuo, W.; Oramisi, V.; Nyaga, L.; Karimi, J.; Wamalwa, P.; Gatheca, G.; et al. The COVID-19 pandemic and disruptions to essential health services in Kenya: A retrospective time-series analysis. Lancet Glob. Health 2022, 10, e1257–e1267. [Google Scholar]
- Manhiça, I.; Augusto, O.; Sherr, K.; Cowan, J.; Cuco, R.M.; Agostinho, S.; Macuacua, B.C.; Ramiro, I.; Carimo, N.; Matsinhe, M.B.; et al. COVID-19-related healthcare impacts: An uncontrolled, segmented time-series analysis of tuberculosis diagnosis services in Mozambique, 2017–2020. BMJ Glob Health 2022, 7, e007878. [Google Scholar]
- McQuaid, C.F.; Henrion, M.Y.R.; Burke, R.M.; MacPherson, P.; Nzawa-Soko, R.; Horton, K.C. Inequalities in the impact of COVID-19-associated disruptions on tuberculosis diagnosis by age and sex in 45 high TB burden countries. BMC Med. 2022, 20, 432. [Google Scholar]
- Jeong, Y.; Min, J. Impact of COVID-19 Pandemic on Tuberculosis Preventive Services and Their Post-Pandemic Recovery Strategies: A Rapid Review of Literature. J. Korean Med. Sci. 2023, 38, e43. [Google Scholar] [CrossRef] [PubMed]
- Lestari, T.; Kamaludin; Lowbridge, C.; Kenangalem, E.; Poespoprodjo, J.R.; Graham, S.M.; Ralph, A.P. Impacts of tuberculosis services strengthening and the COVID-19 pandemic on case detection and treatment outcomes in Mimika District, Papua, Indonesia: 2014–2021. PLoS Global Public Health 2022, 2, e0001114. [Google Scholar] [CrossRef] [PubMed]
- Migliori, G.B.; Thong, P.M.; Akkerman, O.; Alffenaar, J.W.; Álvarez-Navascués, F.; Assao-Neino, M.M.; Bernard, P.V.; Biala, J.S.; Blanc, F.-X.; Bogorodskaya, E.M.; et al. Worldwide Effects of Coronavirus Disease Pandemic on Tuberculosis Services, January–April 2020. Emerg. Infect. Dis. 2020, 26, 2709–2712. [Google Scholar] [CrossRef] [PubMed]
- Barber, R.M.; Sorensen, R.J.D.; Pigott, D.M.; Bisignano, C.; Carter, A.; Amlag, J.O.; Collins, J.K.; Abbafati, C.; Adolph, C.; Allorant, A.; et al. Estimating global, regional, and national daily and cumulative infections with SARS-CoV-2 through Nov 14, 2021: A statistical analysis. Lancet 2022, 399, 2351–2380. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- COVID-19 Forecasting Team. Variation in the COVID-19 infection-fatality ratio by age, time, and geography during the pre-vaccine era: A systematic analysis. Lancet 2022, 399, 1469–1488. [Google Scholar] [CrossRef]
- Wang, Q.; Guo, S.; Wei, X.; Dong, Q.; Xu, N.; Li, H.; Zhao, J.; Sun, Q. Global prevalence, treatment and outcome of tuberculosis and COVID-19 coinfection: A systematic review and meta-analysis (from November 2019 to March 2021). BMJ Open 2022, 12, e059396. [Google Scholar] [CrossRef]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0140673620309259 (accessed on 13 June 2023). [CrossRef]
- Murray, C.J.L.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0140673620307522 (accessed on 13 June 2023). [CrossRef]
- Wang, H.; Paulson, K.R.; Pease, S.A.; Watson, S.; Comfort, H.; Zheng, P.; Aravkin, A.Y.; Bisignano, C.; Barber, R.M.; Alam, T.; et al. Estimating excess mortality due to the COVID-19 pandemic: A systematic analysis of COVID-19-related mortality, 2020–2021. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. Available online: http://www.nature.com/articles/s41562-021-01079-8 (accessed on 13 June 2023). [CrossRef] [PubMed]
- Wu, C.F.J.; Deng, L.Y. Estimation of Variance of the Ratio Estimator: An Empirical Study. In Scientific Inference, Data Analysis, and Robustness; Elsevier: Amsterdam, The Netherlands, 1983; pp. 245–277. [Google Scholar]
- Tibshirani, R. The LASSO method for variable selection in the Cox model. Stat. Med. 1997, 16, 385–395. [Google Scholar] [CrossRef]
- Owen, A.B.; Prieur, C. On Shapley Value for Measuring Importance of Dependent Inputs. SIAM/ASA J. Uncertain. Quantif. 2017, 5, 986–1002. [Google Scholar] [CrossRef]
- Li, H.; Ling, F.; Zhang, S.; Liu, Y.; Wang, C.; Lin, H.; Sun, J.; Wu, Y. Comparison of 19 major infectious diseases during COVID-19 epidemic and previous years in Zhejiang, implications for prevention measures. BMC Infect. Dis. 2022, 22, 296. [Google Scholar] [CrossRef] [PubMed]
- Amar, S.; Avni, Y.S.; O’Rourke, N.; Michael, T. Prevalence of Common Infectious Diseases After COVID-19 Vaccination and Easing of Pandemic Restrictions in Israel. JAMA Netw. Open. 2022, 5, e2146175. [Google Scholar] [CrossRef]
- Feng, L.; Zhang, T.; Wang, Q.; Xie, Y.; Peng, Z.; Zheng, J.; Qin, Y.; Zhang, M.; Lai, S.; Wang, D.; et al. Impact of COVID-19 outbreaks and interventions on influenza in China and the United States. Nat. Commun. 2021, 12, 3249. [Google Scholar] [CrossRef]
- Dharmadhikari, A.S.; Mphahlele, M.; Stoltz, A.; Venter, K.; Mathebula, R.; Masotla, T.; Lubbe, W.; Pagano, M.; First, M.; Jensen, P.A.; et al. Surgical Face Masks Worn by Patients with Multidrug-Resistant Tuberculosis. Am. J. Respir. Crit. Care Med. 2012, 185, 1104–1109. [Google Scholar] [CrossRef]
- Verver, S.; Warren, R.M.; Munch, Z.; Richardson, M.; van der Spuy, G.D.; Borgdorff, M.W.; Behr, M.A.; Beyers, N.; van Helden, P.D. Proportion of tuberculosis transmission that takes place in households in a high-incidence area. Lancet 2004, 363, 212–214. [Google Scholar] [CrossRef]
- Martinez, L.; Shen, Y.; Mupere, E.; Kizza, A.; Hill, P.C.; Whalen, C.C. Transmission of Mycobacterium Tuberculosis in Households and the Community: A Systematic Review and Meta-Analysis. Am. J. Epidemiol. 2017, 185, 1327–1339. [Google Scholar] [CrossRef]
- Martinez, L.; Lo, N.C.; Cords, O.; Hill, P.C.; Khan, P.; Hatherill, M.; Mandalakas, A.; Kay, A.; Croda, J.; Horsburgh, C.R.; et al. Paediatric tuberculosis transmission outside the household: Challenging historical paradigms to inform future public health strategies. Lancet Respir. Med. 2019, 7, 544–552. [Google Scholar] [CrossRef]
- Alene, K.A.; Wangdi, K.; Clements, A.C.A. Impact of the COVID-19 pandemic on tuberculosis control: An overview. Trop. Med. Infect. Dis. 2020, 5, 123. Available online: https://www.mdpi.com/2414-6366/5/3/123 (accessed on 16 June 2023). [CrossRef] [PubMed]
- Tuberculosis and COVID-19 co-infection: Description of the global cohort. Eur. Respir. J. 2022, 59, 2102538. [CrossRef]
- Easton, A.V.; Salerno, M.M.; Trieu, L.; Humphrey, E.; Kaba, F.; Macaraig, M.; Dworkin, F.; Nilsen, D.M.; Burzynski, J. Cohort study of the mortality among patients in New York City with tuberculosis and COVID-19, March 2020 to June 2022. PLoS Global. Public Health 2023, 3, e0001758. [Google Scholar] [CrossRef] [PubMed]
- Péterfi, A.; Mészáros, Á.; Szarvas, Z.; Pénzes, M.; Fekete, M.; Fehér, Á.; Lehoczki, A.; Csípő, T.; Fazekas-Pongor, V. Comorbidities and increased mortality of COVID-19 among the elderly: A systematic review. Physiol. Int. 2022, 109, 163–176. [Google Scholar] [CrossRef] [PubMed]
- Indian Council of Medical Research. National Tuberculosis Prevalence Survey in India, 2019–2021; Indian Council of Medical Research: New Delhi, India, 2022. [Google Scholar]
- Sabet, N.; Omar, T.; Milovanovic, M.; Magajane, T.; Mosala, M.; Moloantoa, T.; Kato-Kalule, N.; Semedo, L.V.; Swanepoel, F.; Wallis, C.; et al. Undiagnosed Pulmonary Tuberculosis (TB) and Coronavirus Disease 2019 (COVID-19) in Adults Dying at Home in a High-TB-Burden Setting, Before and During Pandemic COVID-19: An Autopsy Study. Clin. Infect. Dis. 2023, 77, ciad212. [Google Scholar] [CrossRef] [PubMed]
- Lewnard, J.A.; Kang, G.; Laxminarayan, R. Attributed causes of excess mortality during the COVID-19 pandemic in a south Indian city. Nat. Commun. 2023, 14, 3563. [Google Scholar] [CrossRef]
- Lin, E.C.; Tu, H.P.; Hong, C.H. Limited effect of reducing pulmonary tuberculosis incidence amid mandatory facial masking for COVID-19. Respir Res. 2023, 24, 54. [Google Scholar] [CrossRef]
- Bardhan, M.; Hasan, M.M.; Ray, I.; Sarkar, A.; Chahal, P.; Rackimuthu, S.; Essar, M.Y. Tuberculosis amidst COVID-19 pandemic in India: Unspoken challenges and the way forward. Trop. Med. Health 2021, 49, 84. [Google Scholar] [CrossRef]
- Winardi, W.; Wahyuni, H.; Hidayat, M.; Wirawan, A.; Uddin, M.N.; Yusup, M. Challenges on tuberculosis care in health care facilities during COVID-19 pandemic: Indonesian perspective. Narra J. 2022, 2, e80. [Google Scholar] [CrossRef]
- Xia, Y.; Huang, F.; Chen, H.; Wang, N.; Du, X.; Chen, W.; Li, T.; Huan, S.; Sun, M.; Liu, J.; et al. The Impact of COVID-19 on Tuberculosis Patients’ Behavior of Seeking Medical Care—China, 2020. China CDC Wkly 2021, 3, 553–556. [Google Scholar] [CrossRef]
- Amit, A.M.; Pepito, V.C.; Dayrit, M. Early response to COVID-19 in the Philippines. West. Pac. Surveill. Response J. 2021, 12, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.Y.; Islam, T.; Xu, C.; Chinnayah, T.; Garfin, A.M.C.; Rahevar, K.; Raviglione, M. The impact of COVID-19 and the restoration of tuberculosis services in the Western Pacific Region. Eur. Respir. J. 2020, 56, 2003054. [Google Scholar] [CrossRef]
- Lungu, P.; Kerkhoff, A.; Muyoyeta, M.; Kasapo, C.; Nyangu, S.; Kagujje, M.; Chimzizi, R.; Nyimbili, S.; Khunga, M.; Kasese-Chanda, N.; et al. Interrupted time-series analysis of active case-finding for tuberculosis during the COVID-19 pandemic, Zambia. Bull. World Health Organ. 2022, 100, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Oga-Omenka, C.; Sassi, A.; Vasquez, N.A.; Baruwa, E.; Rosapep, L.; Daniels, B.; Olusola-Faleye, B.; Huria, L.; Adamu, A.; Johns, B.; et al. Tuberculosis service disruptions and adaptations during the first year of the COVID-19 pandemic in the private health sector of two urban settings in Nigeria—A mixed methods study. PLoS Glob. Public Health 2023, 3, e0001618. [Google Scholar] [CrossRef]
- Klinton, J.S.; Heitkamp, P.; Rashid, A.; Faleye, B.O.; Win Htat, H.; Hussain, H.; Syed, I.; Farough, K.; Mortera, L.; Moh Lwin, M.; et al. One year of COVID-19 and its impact on private provider engagement for TB: A rapid assessment of intermediary NGOs in seven high TB burden countries. J. Clin. Tuberc. Other Mycobact. Dis. 2021, 25, 100277. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Location | Year | Observed TB Notifications | Expected TB Notifications | Difference in Observed to Expected TB Notifications | |||
|---|---|---|---|---|---|---|---|
| Cases | Rate per 100,000 Population | Cases | Rate per 100,000 Population | Number | Ratio | ||
| Global | 2020 | 5,830,000 | 74.5 | 7,380,000 (7,090,000, 7,680,000) | 94.4 (90.6, 98.2) | −1,550,000 (−1,850,000, −1,260,000) | 0.79 (0.75, 0.83) |
| 2021 | 6,430,000 | 81.5 | 7,710,000 (7,330,000, 8,100,000) | 97.7 (92.8, 102.6) | −1,280,000 (−1,670,000, −897,000) | 0.83 (0.79, 0.88) | |
| Southeast Asia, East Asia, and Oceania | 2020 | 1,740,000 | 80.2 | 2,350,000 (2,240,000, 2,450,000) | 107.8 (103.0, 112.7) | −601,000 (−706,000, −496,000) | 0.74 (0.70, 0.78) |
| 2021 | 1,730,000 | 79.2 | 2,450,000 (2,310,000, 2,590,000) | 112.2 (105.7, 118.6) | −721,000 (−863,000, −580,000) | 0.71 (0.66, 0.75) | |
| Central Europe, Eastern Europe, and Central Asia | 2020 | 136,000 | 32.4 | 170,000 (165,000, 174,000) | 40.6 (39.5, 41.6) | −34,200 (−38,600, −29,800) | 0.80 (0.78, 0.82) |
| 2021 | 136,000 | 32.5 | 160,000 (155,000, 165,000) | 38.3 (37.1, 39.5) | −24,100 (−29,000, −19,100) | 0.85 (0.82, 0.88) | |
| High-income | 2020 | 84,600 | 7.8 | 98,200 (96,600, 99,700) | 9.0 (8.9, 9.2) | −13,600 (−15,200, −11,900) | 0.86 (0.85, 0.88) |
| 2021 | 85,900 | 7.9 | 95,100 (93,200, 96,900) | 8.7 (8.5, 8.9) | −9140 (−11,000, −7230) | 0.90 (0.88, 0.92) | |
| Latin America and the Caribbean | 2020 | 177,000 | 30.0 | 217,000 (212,000, 222,000) | 36.8 (36.0, 37.6) | −40,000 (−45,000, −35,000) | 0.82 (0.80, 0.84) |
| 2021 | 191,000 | 32.1 | 221,000 (215,000, 227,000) | 37.1 (36.1, 38.2) | −29,900 (−36,000, −23,700) | 0.86 (0.84, 0.89) | |
| North Africa and the Middle East | 2020 | 158,000 | 25.6 | 192,000 (187,000, 197,000) | 31.2 (30.4, 32.0) | −34,100 (−39,000, −29,100) | 0.82 (0.80, 0.85) |
| 2021 | 167,000 | 26.9 | 197,000 (191,000, 204,000) | 31.7 (30.7, 32.7) | −29,900 (−36,200, −23,600) | 0.85 (0.82, 0.88) | |
| South Asia | 2020 | 2,160,000 | 118.2 | 2,950,000 (2,670,000, 3,220,000) | 161.3 (146.3, 176.3) | −787,000 (−1,060,000, −513,000) | 0.73 (0.65, 0.81) |
| 2021 | 2,640,000 | 143.0 | 3,130,000 (2,780,000, 3,490,000) | 169.7 (150.5, 189.0) | −493,000 (−849,000, −138,000) | 0.84 (0.74, 0.95) | |
| Sub-Saharan Africa | 2020 | 1,370,000 | 123.9 | 1,410,000 (1,380,000, 1,450,000) | 127.8 (124.8, 130.8) | −43,900 (−77,200, −10,600) | 0.97 (0.95, 0.99) |
| 2021 | 1,480,000 | 130.6 | 1,450,000 (1,410,000, 1,500,000) | 128.3 (124.6, 131.9) | 26,100 (−15,500, 67,700) | 1.02 (0.99, 1.05) | |
| Coefficient (95% CI) | Standardized Coefficient (95% CI) | Variation in OE Ratio Explained by Each Factor | |||
|---|---|---|---|---|---|
| 2020 Model | Age-standardized smoking prevalence (per 5%) | 0.973 (0.957, 0.990) | −0.044 (−0.072, −0.016) | 16.4% | |
| Education (2 years per capita) | 0.986 (0.964, 1.009) | −0.020 (−0.053, 0.012) | 9.6% | ||
| Percent of population 65 and above (per 5%) | 0.971 (0.944, 0.999) | −0.038 (−0.074, −0.002) | 12.0% | ||
| Stay-at-home order (per 30 days in place) | 0.993 (0.985, 1.000) | −0.025 (−0.051, 0.002) | 12.3% | ||
| School closure (per 30 days in place) | 0.988 (0.977, 0.998) | −0.033 (−0.061, −0.006) | 17.6% | ||
| Reported COVID-19 case rate (per 1000) | 1.001 (0.999, 1.003) | 0.016 (−0.018, 0.051) | 9.0% | ||
| Log SARS-CoV-2 infection rate (per 25%) | 0.991 (0.987, 0.996) | −0.052 (−0.080, −0.025) | 16.6% | ||
| Age-standardized reported COVID-19 death rate (per 1000) | 0.984 (0.947, 1.022) | −0.011 (−0.037, 0.015) | 6.5% | ||
| Model characteristics | R2 | 0.288 | |||
| AIC | −614.373 | ||||
| 2021 Model | Age-standardized smoking prevalence (per 5%) | 0.957 (0.940, 0.974) | −0.071 (−0.100, −0.043) | ||
| Model characteristics | R2 | 0.121 | |||
| AIC | −565.799 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ledesma, J.R.; Basting, A.; Chu, H.T.; Ma, J.; Zhang, M.; Vongpradith, A.; Novotney, A.; Dalos, J.; Zheng, P.; Murray, C.J.L.; et al. Global-, Regional-, and National-Level Impacts of the COVID-19 Pandemic on Tuberculosis Diagnoses, 2020–2021. Microorganisms 2023, 11, 2191. https://doi.org/10.3390/microorganisms11092191
Ledesma JR, Basting A, Chu HT, Ma J, Zhang M, Vongpradith A, Novotney A, Dalos J, Zheng P, Murray CJL, et al. Global-, Regional-, and National-Level Impacts of the COVID-19 Pandemic on Tuberculosis Diagnoses, 2020–2021. Microorganisms. 2023; 11(9):2191. https://doi.org/10.3390/microorganisms11092191
Chicago/Turabian StyleLedesma, Jorge R., Ann Basting, Huong T. Chu, Jianing Ma, Meixin Zhang, Avina Vongpradith, Amanda Novotney, Jeremy Dalos, Peng Zheng, Christopher J. L. Murray, and et al. 2023. "Global-, Regional-, and National-Level Impacts of the COVID-19 Pandemic on Tuberculosis Diagnoses, 2020–2021" Microorganisms 11, no. 9: 2191. https://doi.org/10.3390/microorganisms11092191