
Analysis of Etiology of Community-Acquired and Nosocomial Urinary Tract Infections and Antibiotic Resistance of Isolated Strains: Results of a 3-Year Surveillance (2020–2022) at the Pediatric Teaching Hospital in Warsaw
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Microbiological Procedures
2.4. ESBL and Carbapenemase Detection
2.5. Statistical Analysis
3. Results
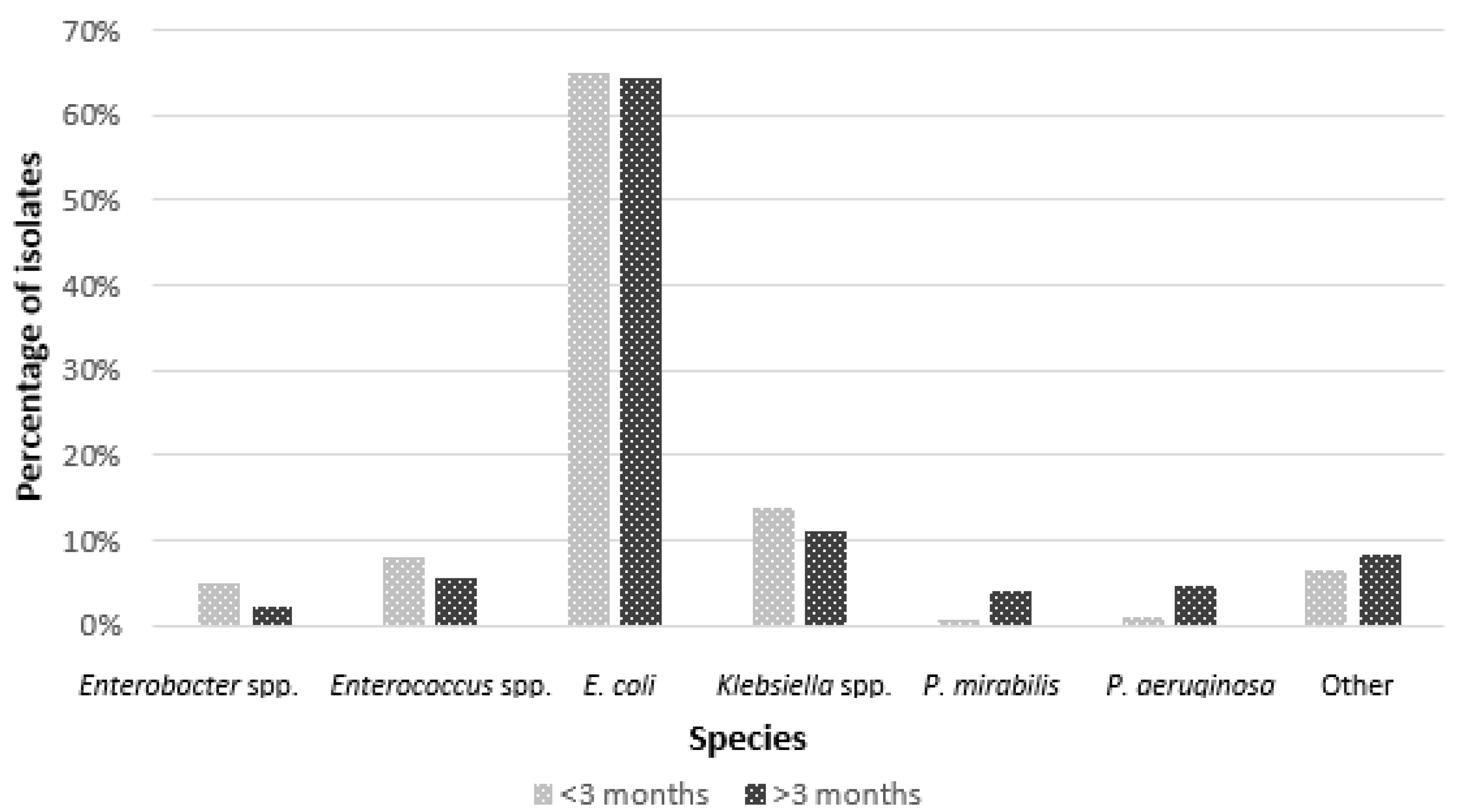
3.1. Etiology of UTI
3.2. Resistance Pattern of Uropathogens
3.2.1. Resistance to Beta-Lactams
3.2.2. Resistance to Other Classes of Antibiotics
3.2.3. Changes in Susceptibility in a Period of Three Years and the COVID-19 Pandemic in E. coli and Klebsiella spp.
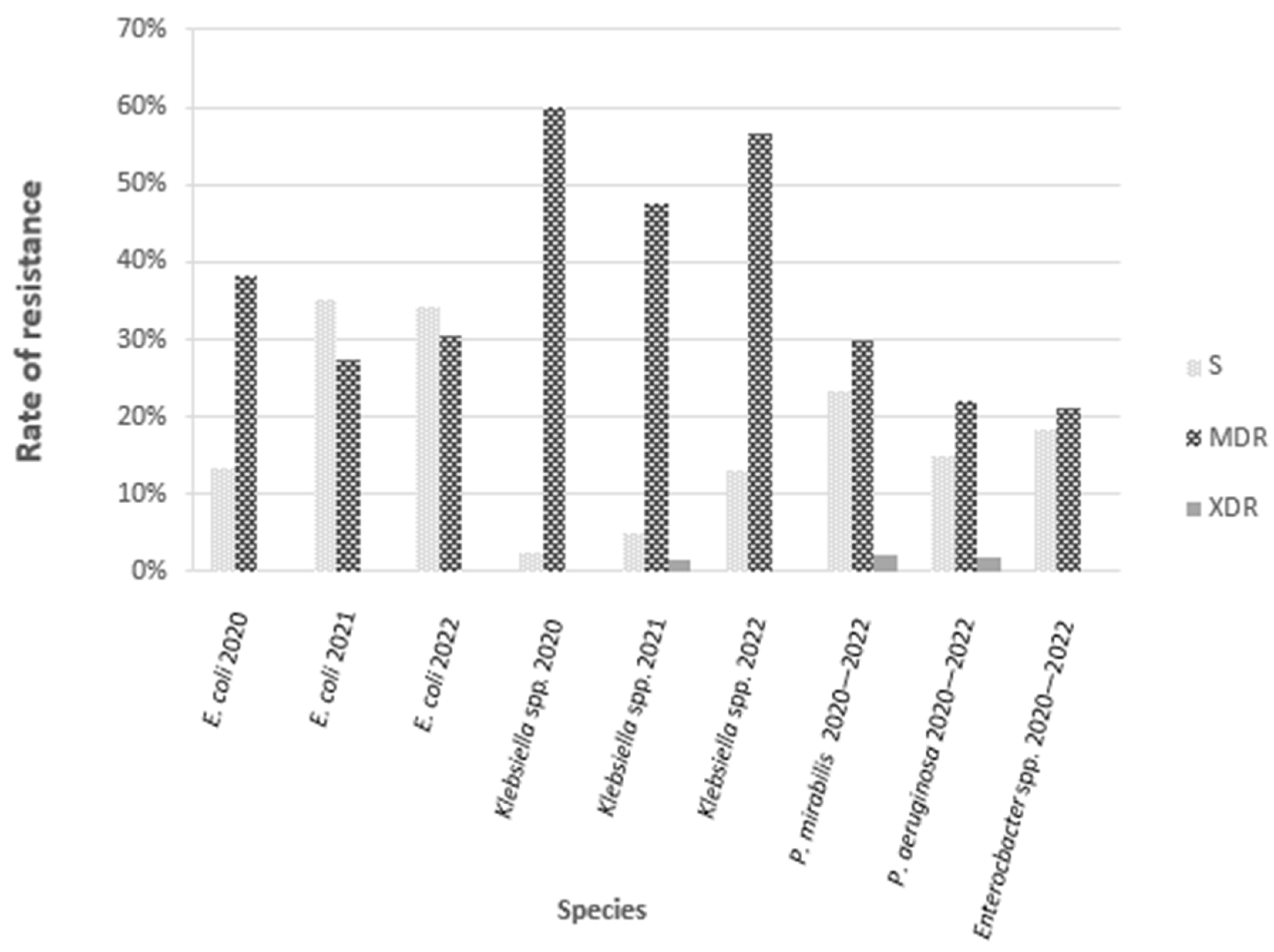
3.2.4. Resistance Profile—S, MDR, XDR, PDR
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| AMP | TZP | CFN | CROPO | CROX | CAZ | CTX | FEP | CFX | IMI | MEM | ETP | GM | AN | TOB | TMP | SXT | CIP | LEV | NF | FOS-IV | FOSPO | GMH | STR | VA | TEI | LZD | FLU | AMB | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| E. coli | 54.9 | 5.5 | 12.3 | 11.4 | 13.5 | 8.5 | 10.7 | 8.8 | 8.3 1 | 0 | 0 | 0 | 5.5 | 1.2 | 0.1 | 26.7 | 25.2 | 11.9 | — | 3.3 | 0 | 0.8 | — | — | — | — | — | — | |
| Klebsiella sp. | — | 34.2 | 32.3 | 34.8 | 42.2 | 31.1 | 31.1 | 29.8 | 27.3 1 | 0.6 | 0.6 | 0.6 | 17.4 | 6.8 | 0 | 48.4 | 40.4 | 31.1 | — | — | — | — | — | — | — | — | — | — | — |
| Proteus mirabilis | 44.7 | 0 | 8.5 | 6.4 | 6.4 | 4.3 | 6.4 | 6.4 | 2.11 | 0 | 0 | 0 | 8.5 | 0 | 0 | 51.1 | 40.4 | 29.8 | — | — | — | — | — | — | — | — | — | — | — |
| Enterobacter sp. | — | 0 | 0 | — | — | 31.6 | 31.6 | 21.1 | — | 0 | 0 | 10.5 | 5.3 | 0 | 0 | 15.8 | 13.2 | 2.6 | — | — | — | — | — | — | — | — | — | — | — |
| Ps. aeruginosa | — | 16.7 | — | — | — | 11.1 | — | 12.9 | — | 12.9 | 11.1 | — | 7.4 | 5.6 | 7.4 | — | — | 9.3 | — | — | — | — | — | — | — | — | — | — | — |
| E. faecalis | 0 | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | 4.6 | 4.6 | 1.5 | 0 | 1.5 | — | 15.4 | 18.5 | 0 | 0 | 0 | — | — |
| Candida sp. | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | — | 0 | 0 |
Appendix B
| Antibiotic | E. coli | Klebsiella spp. | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2020 | 2021 | 2022 | 2020 | 2021 | 2022 | |||||||
| No | % | No | % | No | % | No | % | No | % | No | % | |
| ampicillin | 178 | 58.17 | 162 | 51.27 | 153 | 55.43 | - | - | - | - | - | - |
| cefalexin | 48 | 15.69 | 36 | 11.39 | 26 | 9.42 | 12 | 30.00 | 15 | 25.42 | 25 | 40.32 |
| cefuroxime po | 46 | 15.03 | 24 | 7.59 | 32 | 11.59 | 17 | 42.50 | 11 | 18.64 | 28 | 45.16 |
| cefuroxime iv | 49 | 16.01 | 39 | 12.34 | 33 | 11.96 | 18 | 45.00 | 22 | 37.29 | 28 | 45.16 |
| cefotaxime | 49 | 16.01 | 25 | 7.91 | 22 | 7.97 | 12 | 30.00 | 14 | 23.73 | 24 | 38.71 |
| cefepime | 38 | 12.42 | 22 | 6.96 | 19 | 6.88 | 12 | 30.00 | 14 | 23.73 | 22 | 35.48 |
| cefixime | 4 | 1.31 | 29 | 9.18 | 20 | 7.25 | 1 | - | 12 | 20.34 | 21 | 33.87 |
| ceftazidime | 35 | 11.44 | 22 | 6.96 | 19 | 6.88 | 13 | 32.50 | 14 | 23.73 | 23 | 37.10 |
| piperacillin–tazobactam | 23 | 7.52 | 13 | 4.11 | 13 | 4.71 | 10 | 25.00 | 18 | 30.51 | 27 | 43.55 |
| imipenem | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 1 | 1.69 | 0 | 0.00 |
| meropenem | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 1 | 1.69 | 0 | 0.00 |
| ertapenem | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 1 | 1.69 | 0 | 0.00 |
| gentamycin | 22 | 7.19 | 13 | 4.11 | 14 | 5.07 | 6 | 15.00 | 12 | 20.34 | 10 | 16.13 |
| amikacin | 4 | 1.31 | 3 | 0.95 | 4 | 1.45 | 1 | 2.50 | 2 | 3.39 | 8 | 12.90 |
| tobramycin | 1 | 0.33 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| trimethoprim | 81 | 26.47 | 79 | 25.00 | 80 | 28.99 | 19 | 47.50 | 22 | 37.29 | 37 | 59.68 |
| Trimethoprim-sulfamethoxazole | 76 | 24.84 | 76 | 24.05 | 74 | 26.81 | 14 | 35.00 | 16 | 27.12 | 35 | 56.45 |
| ciprofloxacin | 35 | 11.44 | 46 | 14.56 | 26 | 9.42 | 14 | 35.00 | 17 | 28.81 | 19 | 30.65 |
| nitrofurantoin | 17 | 5.56 | 6 | 1.90 | 7 | 2.54 | - | - | - | - | - | - |
| fosfomycin iv | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | - | - | - | - | - | - |
| fosfomycin po | 1 | 0.33 | 2 | 0.63% | 4 | 1.45% | - | - | - | - | - | - |
References
- Shaikh, N.; Morone, N.E.; Bost, J.E.; Farrell, M.H. Prevalence of urinary tract infection in childhood: A meta-analysis. Pediatr. Infect. Dis. J. 2008, 27, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Salo, J.; Ikäheimo, R.; Tapiainen, T.; Uhari, M. Childhood urinary tract infections as a cause of chronic kidney disease. Pediatrics 2011, 128, 840–847. [Google Scholar] [CrossRef]
- Practice parameter: The diagnosis, treatment, and evaluation of the initial urinary tract infection in febrile infants and young children. American Academy of Pediatrics. Committee on Quality Improvement. Subcommittee on Urinary Tract Infection. Pediatrics 1999, 103, 843–852. [Google Scholar]
- Roberts, K.B. Urinary tract infection: Clinical practice guideline for diagnosing and managing the initial UTI in febrile infants and children 2 to 24 months. Pediatrics 2011, 128, 595–610. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, N.; Ewing, A.L.; Bhatnagar, S.; Hoberman, A. Risk of renal scarring in children with a first urinary tract infection: A systematic review. Pediatrics 2010, 126, 1084–1091. [Google Scholar] [CrossRef]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef]
- Kim, Y.H.; Yang, E.M.; Kim, C.J. Urinary tract infection caused by community-acquired extended-spectrum β-lactamase-producing bacteria in infants. J. Pediatr. 2017, 93, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Fan, N.C.; Chen, H.H.; Chen, C.L.; Ou, L.S.; Lin, T.Y.; Tsai, M.H.; Chiu, C.H. Rise of community-onset urinary tract infection caused by extended-spectrum β-lactamase-producing Escherichia coli in children. J. Microbiol. Immunol. Infect. 2014, 47, 399–405. [Google Scholar] [CrossRef]
- Stapleton, P.J.; Lundon, D.J.; McWade, R.; Scanlon, N.; Hannan, M.M.; O’Kelly, F.; Lynch, M. Antibiotic resistance patterns of Escherichia coli urinary isolates and comparison with antibiotic consumption data over 10 years, 2005–2014. Ir. J. Med. Sci. 2017, 186, 733–774. [Google Scholar] [CrossRef]
- Stefaniuk, E.; Bosacka, K.; Czajkowska, U.; Hryniewicz, W. Epidemiology of community-acquired urinary tract infections—Etiologic agents and their susceptibility to antibiotics. In Proceedings of the 25th ECCMID, Copenhagen, Denmark, 25–28 April 2015. [Google Scholar]
- Paterson, D.L.; Bonomo, R.A. Extended-spectrum beta-lactamases: A clinical update. Clin. Microbiol. Rev. 2005, 18, 657–686. [Google Scholar] [CrossRef]
- Paterson, D.L. Recommendation for treatment of severe infections caused by Enterobacteriaceae producing extended-spectrum b-lactamases (ESBLs). Clin. Microbiol. Infect. 2000, 6, 460–463. [Google Scholar] [CrossRef]
- MacVane, S.H.; Tuttle, L.O.; Nicolau, D.P. Impact of extended-spectrum beta-lactamase-producing organisms on clinical and economic outcomes in patients with urinary tract infection. J. Hosp. Med. 2014, 9, 232–238. [Google Scholar] [CrossRef]
- Blaschke, A.J.; Korgenski, E.K.; Daly, J.A.; LaFleur, B.; Pavia, A.T.; Byington, C.L. Extended-spectrum beta-lactamase-producing pathogens in a children’s hospital: A 5-year experience. Am. J. Infect. Control 2009, 37, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Logan, L.K.; Braykov, N.P.; Weinstein, R.A.; Laxminarayan, R. Extended-spectrum beta-lactamase-producing and third-generation cephalosporin-resistant Enterobacteriaceae in children: Trends in the United States, 1999–2011. J. Pediatr. Infect. Dis. Soc. 2014, 3, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pan drug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- EUCAST Guidelines for Detection of Resistance Mechanisms and Specific Resistances of Clinical and/or Epidemiological Importance; Version 2.0; European Committee on Antimicrobial Susceptibility Testing: Växjö, Sweden, 2017.
- Esposito, S.; Maglietta, G.; Di Costanzo, M.; Ceccoli, M.; Vergine, G.; La Scola, C.; Malaventura, C.; Falcioni, A.; Iacono, A.; Crisafi, A.; et al. The UTI-Ped-ER Study Group. Retrospective 8-Year Study on the Antibiotic Resistance of Uropathogens in Children Hospitalised for Urinary Tract Infection in the Emilia-Romagna Region, Italy. Antibiotics 2021, 10, 1207. [Google Scholar] [CrossRef]
- Stefaniuk, E.; Suchocka, U.; Bosacka, K.; Hryniewicz, W. Etiology and antibiotic susceptibility of bacterial pathogens responsible for community-acquired urinary tract infections in Poland. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1363–1369. [Google Scholar] [CrossRef]
- Kot, B.; Grużewska, A.; Szweda, P.; Wicha, J.; Parulska, U. Antibiotic Resistance of Uropathogens Isolated from Patients Hospitalized in District Hospital in Central Poland in 2020. Antibiotics 2021, 10, 447. [Google Scholar] [CrossRef]
- Clark, C.J.; Kennedy, W.A.; Shortliffe, L.D. Urinary tract infection in children: When to worry. Urol. Clin. N. Am. 2010, 37, 229–241. [Google Scholar] [CrossRef]
- Mahony, M.; McMullan, B.; Brown, J.; Kennedy, S.E. Multidrug-resistant organisms in urinary tract infections in children. Pediatr. Nephrol. 2020, 35, 1563–1573. [Google Scholar] [CrossRef]
- Miftode, I.L.; Pasare, M.A.; Miftode, R.S.; Nastase, E.; Plesca, C.E.; Lunca, C.; Miftode, E.G.; Timpau, A.S.; Iancu, L.S.; Dorneanu, O.S. What Doesn’t Kill Them Makes Them Stronger: The Impact of the Resistance Patterns of Urinary Enterobacterales Isolates in Patients from a Tertiary Hospital in Eastern Europe. Antibiotics 2022, 20, 548. [Google Scholar] [CrossRef] [PubMed]
- Farfour, E.; Dortet, L.; Guillard, T.; Chatelain, N.; Poisson, A.; Mizrahi, A.; Fournier, D.; Bonnin, R.A.; Degand, N.; Morand, P.; et al. On Behalf of The Gmc Study Group. Antimicrobial Resistance in Enterobacterales Recovered from Urinary Tract Infections in France. Pathogens 2022, 15, 356. [Google Scholar] [CrossRef] [PubMed]
- Bora, A.; Sanjana, R.; Jha, B.K.; Mahaseth, S.N.; Pokharel, K. Incidence of metallo-beta-lactamase producing clinical isolates of Escherichia coli and Klebsiella pneumoniae in central Nepal. BMC Res. Notes 2014, 7, 557. [Google Scholar] [CrossRef]
- Zalecenia Polskiego Towarzystwa Nefrologii Dziecięcej (PTNFD) Dotyczące Postępowania z Dzieckiem z Zakażeniem Układu Moczowego. Available online: https://ptnfd.org/site/resource/1323,zalecenia-zum_2021.pdf (accessed on 24 February 2023).
- Demir, M.; Kazanasmaz, H. Uropathogens, and antibiotic resistance in the community and hospital-induced urinary tract infected children. J. Glob. Antimicrob. Resist. 2020, 20, 68–73. [Google Scholar] [CrossRef] [PubMed]
- King, L.M.; Bartoces, M.; Fleming-Dutra, K.E.; Roberts, R.M.; Hicks, L.A. Changes in US Outpatient Antibiotic Prescriptions From 2011–2016. Clin. Infect. Dis. 2020, 70, 370–377. [Google Scholar] [CrossRef]
- Etminan, M.; Guo, M.Y.; Carleton, B. Oral Fluoroquinolone Prescribing to Children in the United States From 2006 to 2015. Pediatr. Infect. Dis. J. 2019, 38, 268–270. [Google Scholar] [CrossRef]
- Meesters, K.; Mauel, R.; Dhont, E.; Walle, J.V.; De Bruyne, P. Systemic fluoroquinolone prescriptions for hospitalized children in Belgium, results of a multicenter retrospective drug utilization study. BMC. Infect. Dis. 2018, 18, 89. [Google Scholar] [CrossRef]
- Bryce, A.; Hay, A.D.; Lane, I.F.; Thornton, H.V.; Wootton, M.; Costelloe, C. Global prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli and association with routine use of antibiotics in primary care: Systematic review and meta-analysis. BMJ 2016, 352, i939. [Google Scholar] [CrossRef]
- Raman, G.; McMullan, B.; Taylor, P.; Mallitt, K.A.; Kennedy, S.E. Multiresistant E. coli urine infections in children: A case-control study. Arch. Dis. Child. 2018, 103, 336–340. [Google Scholar] [CrossRef]
- Salmanov, A.G.; Vdovychenko, S.Y.; Litus, O.I.; Litus, V.I.; Bisyuk, Y.A.; Bondarenko, T.M.; Davtian, L.L.; Olifirova, T.F.; Leleka, M.V.; Kovalchuk, O.I.; et al. Prevalence of healthcare-associated infections and antimicrobial resistance of the responsible pathogens in Ukraine: Results of a multicenter study (2014–2016). Am. J. Infect. Control 2019, 47, 15–20. [Google Scholar] [CrossRef]
- Salmanov, A.G.; Vozianov, S.; Kryzhevsky, V.; Litus, O.; Drozdova, A.; Vlasenko, I. Prevalence of healthcare-associated infections and antimicrobial resistance in acute care hospitals in Kyiv, Ukraine. J. Hosp. Infect. 2019, 102, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial Resistance Surveillance in Europe. 2022. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/ECDC-WHO-AMR-report.pdf (accessed on 24 February 2023).
- Schultze, T.; Hogardt, M.; Velázquez, E.S.; Hack, D.; Besier, S.; Wichelhaus, T.A.; Rochwalsky, U.; Kempf, V.A.; Reinheimer, C. Molecular surveillance of multidrug-resistant Gram-negative bacteria in Ukrainian patients, Germany, March to June 2022. Euro. Surveill. 2023, 28, 2200850. [Google Scholar] [CrossRef] [PubMed]
- Kot, B.; Wicha, J.; Gruzewska, A.; Piechota, M.; Wolska, K.; Obrebska, M. Virulence factors, biofilm-forming ability, and antimicrobial resistance of urinary Escherichia coli strains isolated from hospitalized patients. Turk. J. Med. Sci. 2016, 46, 1908–1914. [Google Scholar] [CrossRef] [PubMed]
- Ciontea, A.S.; Cristea, D.; Andrei, M.M.; Popa, A.; Usein, C.R. In vitro antimicrobial resistance of urinary Escherichia coli isolates from outpatients collected in a laboratory during two years, 2015–2017. Roum. Arch. Microbiol. Immunol. 2018, 77, 28–32. [Google Scholar]
- Lavigne, J.-P.; Bruyère, F.; Bernard, L.; Combescure, C.; Ronco, E.; Lanotte, P.; Coloby, P.; Thibault, M.; Cariou, G.; Desplaces, N. Resistance and virulence potential of uropathogenic Escherichia coli strains isolated from patients hospitalized in urology departments: A French prospective multicentre study. J. Med. Microbiol. 2016, 65, 530–537. [Google Scholar] [CrossRef]


| Etiological Agent | 2020 | 2021 | 2022 | Total | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | % | |
| Escherichia coli | 306 | 70.0 | 316 | 65.2 | 276 | 58.6 | 64.5 |
| Klebsiella spp. (K. pneumoniae, K. oxytoca, K. variicola) | 40 | 9.2 | 59 | 12.2 | 62 | 13.2 | 11.6 |
| Enterococcus faecalis | 15 | 3.4 | 18 | 3.7 | 32 | 6.8 | 4.7 |
| Pseudomonas aeruginosa | 14 | 3.2 | 18 | 3.7 | 22 | 4.7 | 3.9 |
| Proteus mirabilis | 19 | 4.3 | 12 | 2.5 | 16 | 3.4 | 3.4 |
| Enterobacter spp. | 9 | 2.1 | 14 | 2.9 | 15 | 3.2 | 2.7 |
| Candida spp. | 10 | 2.3 | 12 | 2.5 | 8 | 1.7 | 2.2 |
| Enterococcus faecium | 2 | 0.5 | 3 | 0.6 | 14 | 3.0 | 1.4 |
| Citrobacter spp. | 3 | 0.7 | 5 | 1.0 | 3 | 0.6 | 0.8 |
| Serratia marcescens | 4 | 0.9 | 3 | 0.6 | 2 | 0.4 | 0.6 |
| Klebsiella aerogenes (Enterobacter aerogenes) | 3 | 0.7 | 4 | 0.8 | 1 | 0.2 | 0.6 |
| Staphylococcus saprophyticus | 0 | 0.0 | 4 | 0.8 | 3 | 0.6 | 0.5 |
| Streptococcus agalactiae | 0 | 0.0 | 3 | 0.6 | 4 | 0.8 | 0.5 |
| Morganella morganii | 2 | 0.5 | 2 | 0.4 | 1 | 0.2 | 0.4 |
| Corynebacterium spp. | 2 | 0.5 | 0 | 0.0 | 2 | 0.4 | 0.3 |
| Aerococcus urinae | 0 | 0.0 | 0 | 0.0 | 4 | 0.8 | 0.3 |
| Other | 8 | 1.8 | 12 | 2.5 | 6 | 1.3 | 1.9 |
| TOTAL | 437 | 485 | 471 | 1393 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wanke-Rytt, M.; Sobierajski, T.; Lachowicz, D.; Seliga-Gąsior, D.; Podsiadły, E. Analysis of Etiology of Community-Acquired and Nosocomial Urinary Tract Infections and Antibiotic Resistance of Isolated Strains: Results of a 3-Year Surveillance (2020–2022) at the Pediatric Teaching Hospital in Warsaw. Microorganisms 2023, 11, 1438. https://doi.org/10.3390/microorganisms11061438
Wanke-Rytt M, Sobierajski T, Lachowicz D, Seliga-Gąsior D, Podsiadły E. Analysis of Etiology of Community-Acquired and Nosocomial Urinary Tract Infections and Antibiotic Resistance of Isolated Strains: Results of a 3-Year Surveillance (2020–2022) at the Pediatric Teaching Hospital in Warsaw. Microorganisms. 2023; 11(6):1438. https://doi.org/10.3390/microorganisms11061438
Chicago/Turabian StyleWanke-Rytt, Monika, Tomasz Sobierajski, Dominika Lachowicz, Dominika Seliga-Gąsior, and Edyta Podsiadły. 2023. "Analysis of Etiology of Community-Acquired and Nosocomial Urinary Tract Infections and Antibiotic Resistance of Isolated Strains: Results of a 3-Year Surveillance (2020–2022) at the Pediatric Teaching Hospital in Warsaw" Microorganisms 11, no. 6: 1438. https://doi.org/10.3390/microorganisms11061438