
Changes in the Incidence of Invasive Pneumococcal Disease in Calgary, Canada, during the SARS-CoV-2 Pandemic 2020–2022

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Laboratory Methods
2.2. Incidence and Incidence Rate Ratios
2.3. Interrupted Time Series Analysis
3. Results
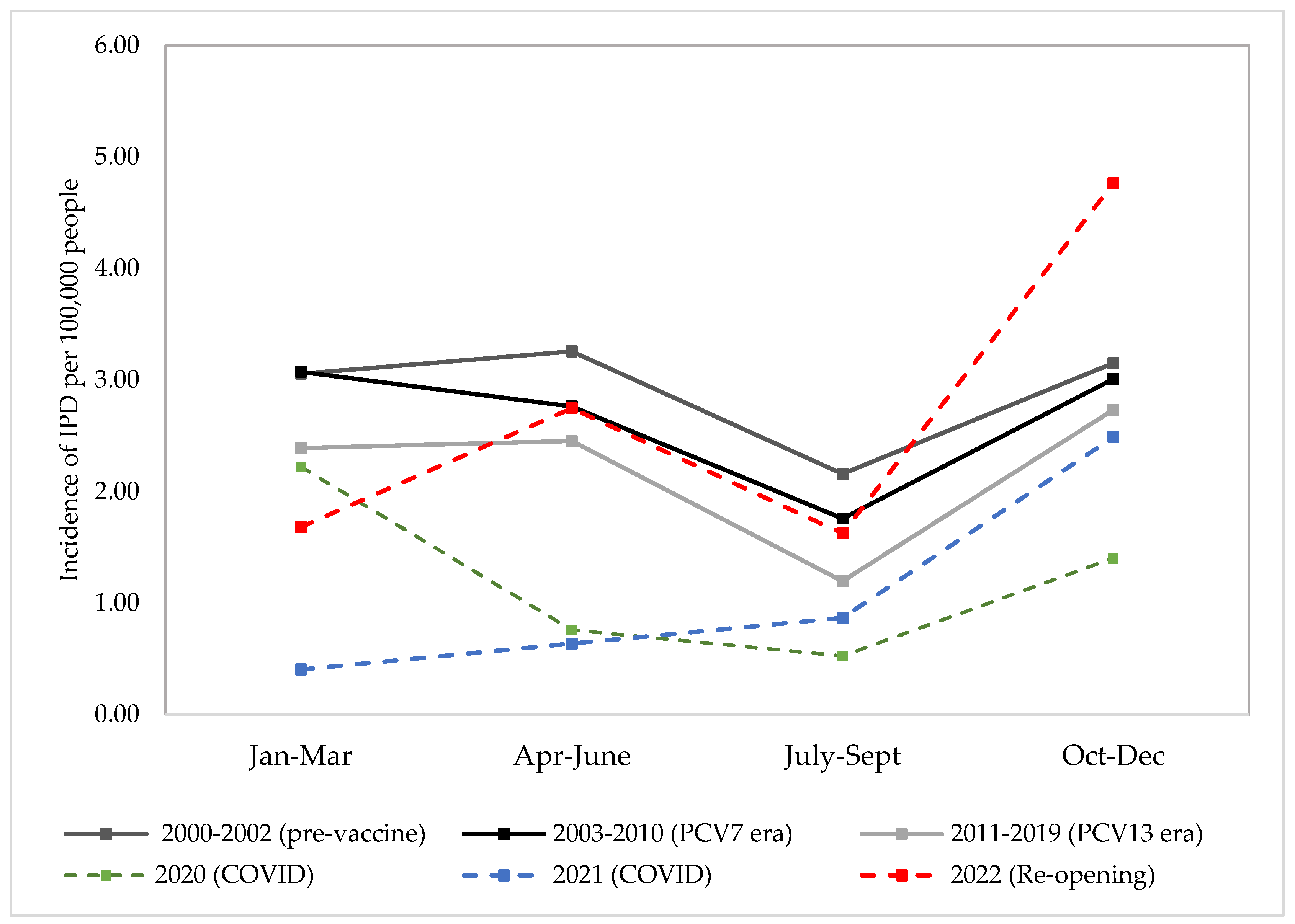
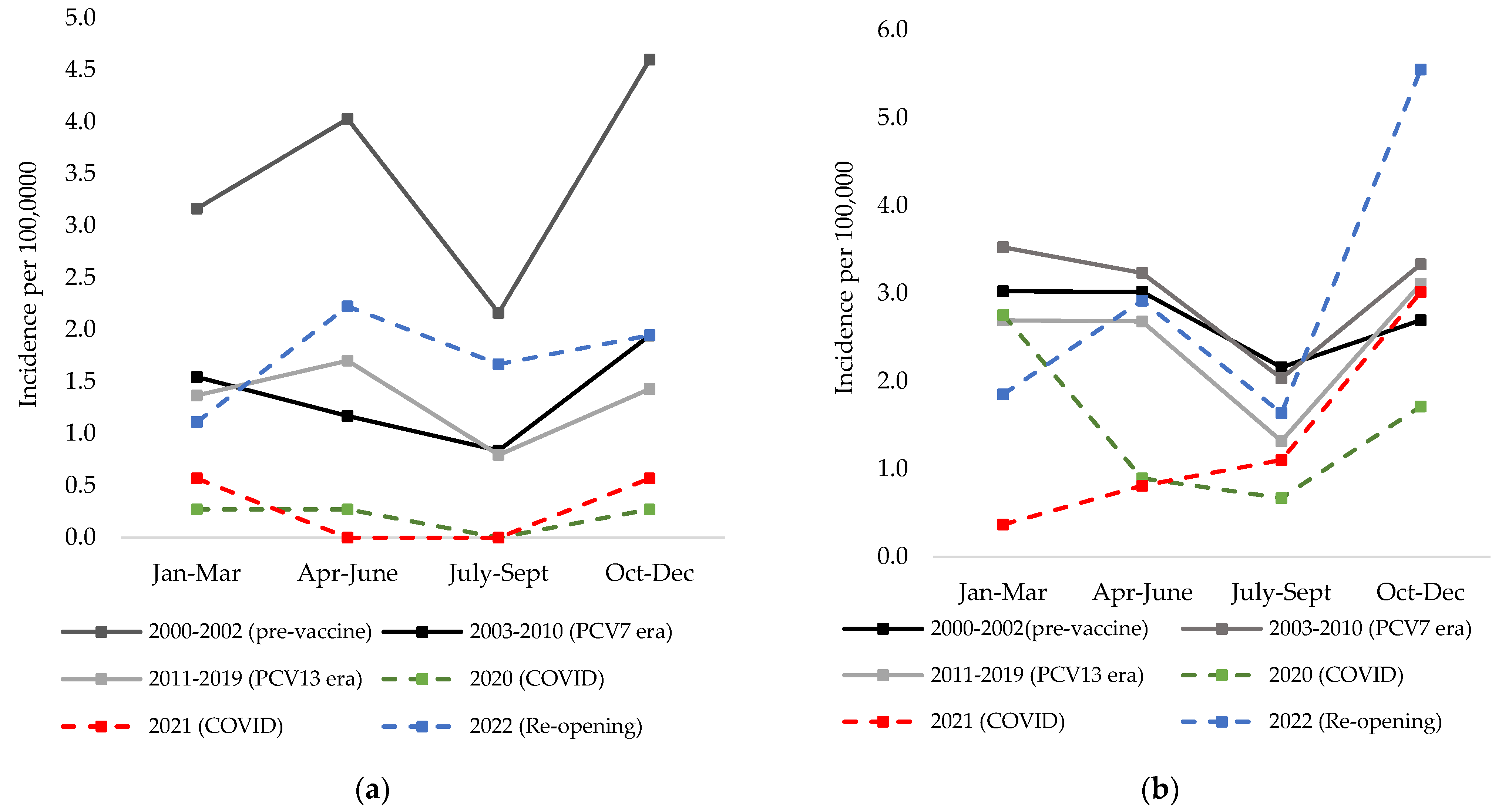
3.1. IPD Incidence in Calgary
3.1.1. Incidence Rate Ratios Comparing Pre-Pandemic (2019) and Early Pandemic Periods (2020/2021)
3.1.2. Incidence Rate Ratios Comparing Pre-Pandemic (2019) and Pre-PCV7 Periods to Later Pandemic Period (2022)
3.2. 2022 Serotypes Causing IPD in Calgary
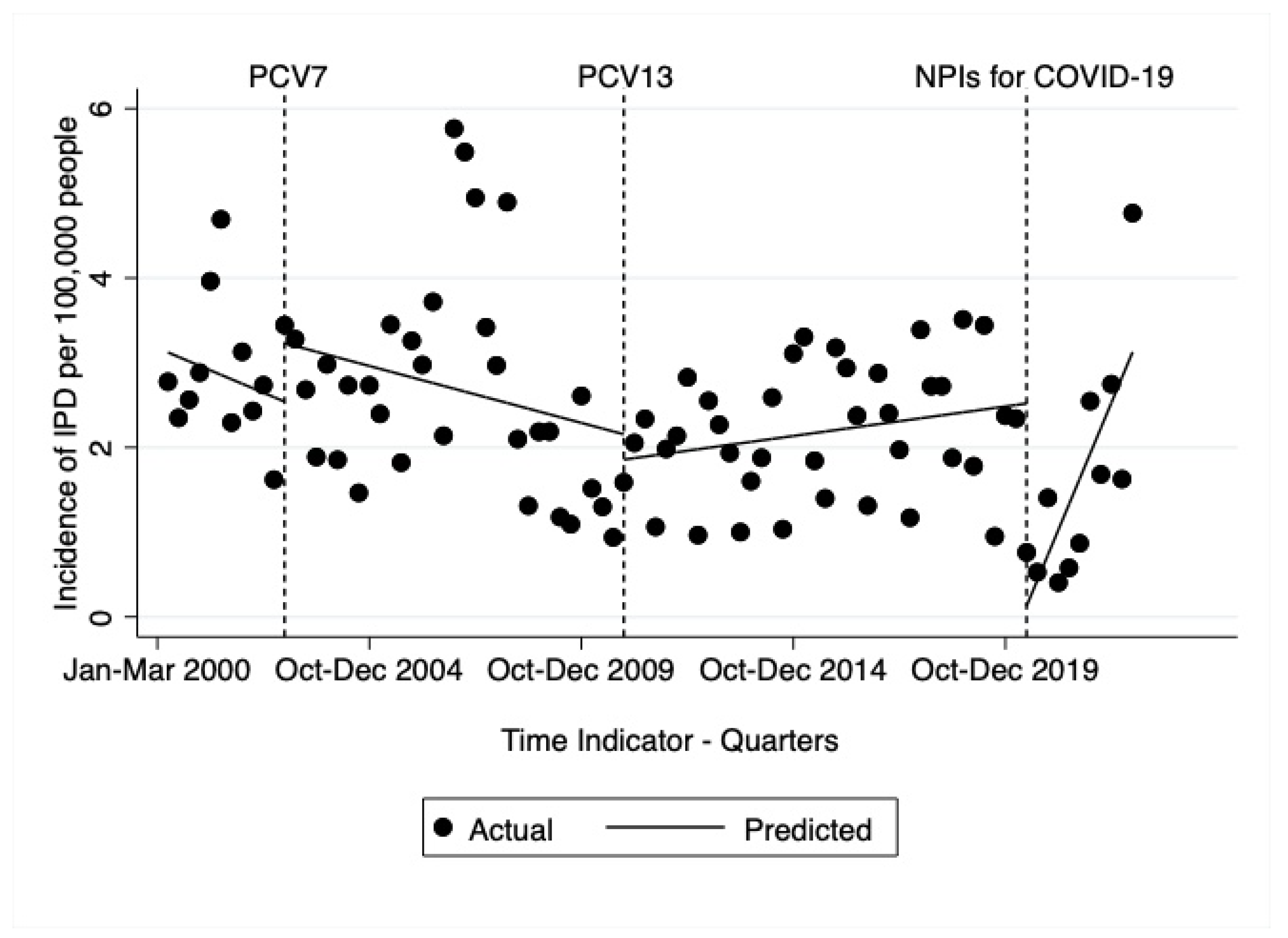
3.3. Interrupted Time Series Analysis 2000–2022
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 9 February 2021).
- Mulcahy, K. Students Are Expected to Stay Home: Alberta Schools, Daycares to Close over COVID-19. CTV News Edmonton. 2020. Available online: https://edmonton.ctvnews.ca/students-are-expected-to-stay-home-alberta-schools-daycares-to-close-over-covid-19-1.4853911 (accessed on 14 March 2023).
- Bank of Canada. COVID-19 Stringiny Index. Available online: https://www.bankofcanada.ca/markets/market-operations-liquidity-provision/covid-19-actions-support-economy-financial-system/covid-19-stringency-index/ (accessed on 14 March 2023).
- Brueggemann, A.B.; Jansen van Rensburg, M.J.; Shaw, D.; McCarthy, N.D.; Jolley, K.A.; Maiden, M.C.J.; van der Linden, M.P.G.; Amin-Chowdhury, Z.; Bennett, D.E.; Borrow, R.; et al. Changes in the incidence of invasive disease due to Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis during the COVID-19 pandemic in 26 countries and territories in the Invasive Respiratory Infection Surveillance Initiative: A prospective analysis of surveillance data. Lancet Digit. Health 2021, 3, e360–e370. [Google Scholar] [CrossRef] [PubMed]
- Government of Alberta. Routine Immunization Schedule. Available online: https://www.alberta.ca/immunization-routine-schedule.aspx (accessed on 9 March 2021).
- Lemay, J.-A.; Ricketson, L.J.; Zwicker, L.; Kellner, J.D. Homelessness in Adults With Invasive Pneumococcal Disease in Calgary, Canada. Open Forum Infect. Dis. 2019, 6, ofz362. [Google Scholar] [CrossRef] [PubMed]
- Kellner, J.D.; Ricketson, L.J.; Demczuk, W.H.B.; Martin, I.; Tyrrell, G.J.; Vanderkooi, O.G.; Mulvey, M.R. Whole-Genome Analysis of Streptococcus pneumoniae Serotype 4 Causing Outbreak of Invasive Pneumococcal Disease, Alberta, Canada. Emerg. Infect. Dis. 2021, 27, 1867–1875. [Google Scholar] [CrossRef]
- Vanderkooi, O.G.; Church, D.L.; Macdonald, J.; Zucol, F.; Kellner, J.D. Community-Based Outbreaks in Vulnerable Populations of Invasive Infections Caused by Streptococcus pneumoniae Serotypes 5 and 8 in Calgary, Canada. PLoS ONE 2011, 6, e28547. [Google Scholar] [CrossRef] [PubMed]
- Ricketson, L.J.; Conradi, N.G.; Vanderkooi, O.G.; Kellner, J.D. Changes in the Nature and Severity of Invasive Pneumococcal Disease in Children, Before and After the 7-Valent and 13-Valent Pneumococcal Conjugate Vaccine Programs in Calgary, Canada. Pediatr. Infect. Dis. J. 2018, 37, 22–27. [Google Scholar] [CrossRef]
- Weinberger, D.M.; Grant, L.R.; Steiner, C.A.; Weatherholtz, R.; Santosham, M.; Viboud, C.; O’Brien, K.L. Seasonal Drivers of Pneumococcal Disease Incidence: Impact of Bacterial Carriage and Viral Activity. Clin. Infect. Dis. 2013, 58, 188–194. [Google Scholar] [CrossRef]
- Ricketson, L.J.; Kellner, J.D. Invasive Pneumococcal Disease in Calgary during the SARS-CoV-2 Pandemic. 2020. Available online: http://hdl.handle.net/1880/113465 (accessed on 13 May 2021).
- Kellner, J.D.; Vanderkooi, O.G.; MacDonald, J.; Church, D.L.; Tyrrell, G.J.; Scheifele, D.W. Changing epidemiology of invasive pneumococcal disease in Canada, 1998-2007: Update from the Calgary-area Streptococcus pneumoniae research (CASPER) study. Clin. Infect. Dis. 2009, 49, 205–212. [Google Scholar] [CrossRef]
- Austrian, R. The quellung reaction, a neglected microbiologic technique. Mt. Sinai J. Med. 1976, 43, 699–709. [Google Scholar]
- Clinical Laboratory and Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing; Twenty-fifth Informational Supplement. M100-S25. Zone Diameter and MIC Interpretive Standards for Streptococcus pneumoniae; Clinical Laboratory and Standards Institute: Wayne, NY, USA, 2015; pp. 96–99. [Google Scholar]
- Alberta Health. Alberta Interactive Health Data Application. Available online: http://www.ahw.gov.ab.ca/IHDA_Retrieval/ (accessed on 16 February 2021).
- Olsen, S.J.; Azziz-Baumgartner, E.; Budd, A.P.; Brammer, L.; Sullivan, S.; Pineda, R.F.; Cohen, C.; Fry, A.M. Decreased Influenza Activity During the COVID-19 Pandemic—United States, Australia, Chile, and South Africa, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1305–1309. [Google Scholar] [CrossRef]
- Chow, E.J.; Uyeki, T.M.; Chu, H.Y. The effects of the COVID-19 pandemic on community respiratory virus activity. Nat. Rev. Microbiol. 2023, 21, 195–210. [Google Scholar] [CrossRef]
- Pierce, A.; Haworth-Brockman, M.; Marin, D.; Rueda, Z.V.; Keynan, Y. Changes in the incidence of seasonal influenza in response to COVID-19 social distancing measures: An observational study based on Canada’s national influenza surveillance system. Can. J. Public Health 2021, 112, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Park, K.Y.; Seo, S.; Han, J.; Park, J.Y. Respiratory virus surveillance in Canada during the COVID-19 pandemic: An epidemiological analysis of the effectiveness of pandemic-related public health measures in reducing seasonal respiratory viruses test positivity. PLoS ONE 2021, 16, e0253451. [Google Scholar] [CrossRef] [PubMed]
- Amin-Chowdhury, Z.; Aiano, F.; Mensah, A.; Sheppard, C.L.; Litt, D.; Fry, N.K.; Andrews, N.; Ramsay, M.E.; Ladhani, S.N. Impact of the Coronavirus Disease 2019 (COVID-19) Pandemic on Invasive Pneumococcal Disease and Risk of Pneumococcal Coinfection With Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Prospective National Cohort Study, England. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 72, e65–e75. [Google Scholar] [CrossRef] [PubMed]
- Lim, R.H.; Chow, A.; Ho, H.J. Decline in pneumococcal disease incidence in the time of COVID-19 in Singapore. J. Infect. 2020, 81, e19–e21. [Google Scholar] [CrossRef] [PubMed]
- Juan, H.C.; Chao, C.M.; Lai, C.C.; Tang, H.J. Decline in invasive pneumococcal disease during COVID-19 pandemic in Taiwan. J. Infect. 2021, 82, 282–327. [Google Scholar] [CrossRef] [PubMed]
- Teng, J.L.L.; Fok, K.M.N.; Lin, K.P.K.; Chan, E.; Ma, Y.; Lau, S.K.P.; Woo, P.C.Y. Substantial Decline in Invasive Pneumococcal Disease During Coronavirus Disease 2019 Pandemic in Hong Kong. Clin. Infect. Dis. 2021, 74, 335–338. [Google Scholar] [CrossRef]
- Chan, K.-P.F.; Ma, T.-F.; Ip, M.S.-M.; Ho, P.-L. Invasive pneumococcal disease, pneumococcal pneumonia and all-cause pneumonia in Hong Kong during the COVID-19 pandemic compared with the preceding 5 years: A retrospective observational study. BMJ Open 2021, 11, e055575. [Google Scholar] [CrossRef]
- Janapatla, R.P.; Chen, C.-L.; Dudek, A.; Li, H.-C.; Yang, H.-P.; Su, L.-H.; Chiu, C.-H. Serotype transmission dynamics and reduced incidence of invasive pneumococcal disease caused by different serotypes after implementation of non-pharmaceutical interventions during COVID-19 pandemic. Eur. Respir. J. 2021, 58, 2100978. [Google Scholar] [CrossRef]
- Amarsy, R.; Fournier, S.; Trystram, D.; Monteil, C.; Raynaud, X.; Jarlier, V.; Robert, J. Decrease of hospital- and community-acquired bloodstream infections due to Streptococcus pneumoniae and Streptococcus pyogenes during the first year of the COVID-19 pandemic: A time-series analysis in Paris region. Am. J. Infect. Control 2023, 51, 475–477. [Google Scholar] [CrossRef]
- Ciruela, P.; Soldevila, N.; García-Garcia, J.J.; González-Peris, S.; Díaz-Conradi, A.; Redin, A.; Viñado, B.; Izquierdo, C.; Muñoz-Almagro, C.; Domínguez, A. Effect of COVID-19 Pandemic on Invasive Pneumococcal Disease in Children, Catalonia, Spain. Emerg. Infect. Dis. 2022, 28, 2321–2325. [Google Scholar] [CrossRef]
- Prasad, N.; Rhodes, J.; Deng, L.; McCarthy, N.L.; Moline, H.L.; Baggs, J.; Reddy, S.C.; Jernigan, J.A.; Havers, F.P.; Sosin, D.M.; et al. Changes in the Incidence of Invasive Bacterial Disease During the COVID-19 Pandemic in the United States, 2014–2020. J. Infect. Dis. 2023, 227, 907–916. [Google Scholar] [CrossRef]
- Sarmiento Clemente, A.; Kaplan, S.L.; Barson, W.J.; Lin, P.L.; Romero, J.R.; Bradley, J.S.; Tan, T.Q.; Pannaraj, P.S.; Givner, L.B.; Hultén, K.G. Decrease in Pediatric Invasive Pneumococcal Disease During the COVID-19 Pandemic. J. Pediatric Infect. Dis. Soc. 2022, 11, 426–428. [Google Scholar] [CrossRef]
- Steens, A.; Knol, M.J.; Freudenburg-de Graaf, W.; de Melker, H.E.; van der Ende, A.; van Sorge, N.M. Pathogen- and Type-Specific Changes in Invasive Bacterial Disease Epidemiology during the First Year of the COVID-19 Pandemic in The Netherlands. Microorganisms 2022, 10, 972. [Google Scholar] [CrossRef]
- Danino, D.; Ben-Shimol, S.; van der Beek, B.A.; Givon-Lavi, N.; Avni, Y.S.; Greenberg, D.; Weinberger, D.M.; Dagan, R. Decline in Pneumococcal Disease in Young Children During the Coronavirus Disease 2019 (COVID-19) Pandemic in Israel Associated With Suppression of Seasonal Respiratory Viruses, Despite Persistent Pneumococcal Carriage: A Prospective Cohort Study. Clin. Infect. Dis. 2021, 75, e1154–e1164. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.; Sweet, C. Cooperation between Viral and Bacterial Pathogens in Causing Human Respiratory Disease. In Polymicrobial Diseases; Wiley: Hoboken, NJ, USA, 2002; pp. 199–212. [Google Scholar]
- Morris, D.E.; Cleary, D.W.; Clarke, S.C. Secondary Bacterial Infections Associated with Influenza Pandemics. Front. Microbiol. 2017, 8, 1041. [Google Scholar] [CrossRef]
- Mirzaei, R.; Goodarzi, P.; Asadi, M.; Soltani, A.; Aljanabi, H.A.A.; Jeda, A.S.; Dashtbin, S.; Jalalifar, S.; Mohammadzadeh, R.; Teimoori, A. Bacterial co-infections with SARS-CoV-2. IUBMB Life 2020, 72, 2097–2111. [Google Scholar] [CrossRef] [PubMed]
- Rybak, A.; Levy, C.; Angoulvant, F.; Auvrignon, A.; Gembara, P.; Danis, K.; Vaux, S.; Levy-Bruhl, D.; van der Werf, S.; Béchet, S.; et al. Association of Nonpharmaceutical Interventions During the COVID-19 Pandemic With Invasive Pneumococcal Disease, Pneumococcal Carriage, and Respiratory Viral Infections Among Children in France. JAMA Netw. Open 2022, 5, e2218959. [Google Scholar] [CrossRef] [PubMed]
- Nourazari, S.; Davis, S.R.; Granovsky, R.; Austin, R.; Straff, D.J.; Joseph, J.W.; Sanchez, L.D. Decreased hospital admissions through emergency departments during the COVID-19 pandemic. Am. J. Emerg. Med. 2021, 42, 203–210. [Google Scholar] [CrossRef]
- Kirsten, K.T.D.; Bert, M.; Annelies, S.P.; Martijn, H.R.; Caroline, M.A.S.; Heiman, F.L.W.; Amelieke, J.H.C. The drop in reported invasive pneumococcal disease among adults during the first COVID-19 wave in the Netherlands explained. Int. J. Infect. Dis. 2021, 111, 196–203. [Google Scholar] [CrossRef]
- Lai, C.-C.; Wang, C.-Y.; Hsueh, P.-R. Co-infections among patients with COVID-19: The need for combination therapy with non-anti-SARS-CoV-2 agents? J. Microbiol. Immunol. Infect. 2020, 53, 505–512. [Google Scholar] [CrossRef]
- Rodriguez-Nava, G.; Yanez-Bello, M.A.; Trelles-Garcia, D.P.; Chung, C.W.; Egoryan, G.; Friedman, H.J. A Retrospective Study of Coinfection of SARS-CoV-2 and Streptococcus pneumoniae in 11 Hospitalized Patients with Severe COVID-19 Pneumonia at a Single Center. Med. Sci. Monit. 2020, 26, e928754. [Google Scholar] [CrossRef] [PubMed]
- Nieto-Moro, M.; Ecclesia, F.G.; Tomé-Masa, I.; De Lama Caro-Patón, G.; Leoz-Gordillo, I.; Cabrero-Hernández, M.; García-Salido, A. SARS-CoV-2 and Streptococcus pneumoniae coinfection as a cause of severe pneumonia in an infant. Pediatr. Pulmonol. 2020, 55, 2198–2200. [Google Scholar] [CrossRef]
- Anton-Vazquez, V.; Clivillé, R. Streptococcus pneumoniae coinfection in hospitalised patients with COVID-19. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1353–1355. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.D.; Fairfield, C.J.; Drake, T.M.; Turtle, L.; Seaton, R.A.; Wootton, D.G.; Sigfrid, L.; Harrison, E.M.; Docherty, A.B.; de Silva, T.I.; et al. Co-infections, secondary infections, and antimicrobial use in patients hospitalised with COVID-19 during the first pandemic wave from the ISARIC WHO CCP-UK study: A multicentre, prospective cohort study. Lancet Microbe 2021, 2, e354–e365. [Google Scholar] [CrossRef] [PubMed]
- Thelen, J.M.; Buenen, A.G.; van Apeldoorn, M.; Wertheim, H.F.; Hermans, M.H.A.; Wever, P.C. Community-acquired bacteraemia in COVID-19 in comparison to influenza A and influenza B: A retrospective cohort study. BMC Infect. Dis. 2021, 21, 199. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Ayad, S.; Alyacoub, R.; Gergis, K.; Grossman, D.; Salamera, J. Invasive pneumococcal disease in a patient with COVID-19: A case report. Cureus 2021, 13. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef]
- Westblade, L.F.; Simon, M.S.; Satlin, M.J. Bacterial Coinfections in Coronavirus Disease 2019. Trends Microbiol. 2021, 29, 930–941. [Google Scholar] [CrossRef]
- Public Health England. Pneumococcal: The Green Book, Chapter 25 (for Infants Born on or after 1 January 2020). Available online: https://www.gov.uk/government/publications/pneumococcal-the-green-book-chapter-25 (accessed on 9 March 2021).
- Perniciaro, S.; van der Linden, M.; Weinberger, D.M. Reemergence of Invasive Pneumococcal Disease in Germany During the Spring and Summer of 2021. Clin. Infect. Dis. 2022, 75, 1149–1153. [Google Scholar] [CrossRef]
- Bertran, M.; Amin-Chowdhury, Z.; Sheppard, C.L.; Eletu, S.; Zamarreño, D.V.; Ramsay, M.E.; Litt, D.; Fry, N.K.; Ladhani, S.N. Increased Incidence of Invasive Pneumococcal Disease among Children after COVID-19 Pandemic. England. Emerg. Infect. Dis. 2022, 28, 1669–1672. [Google Scholar] [CrossRef] [PubMed]
- Alberta Health Services. Alberta Health Services Respiratory Virus Surveillance. Available online: https://public.tableau.com/app/profile/surveillance.reporting.ahs/viz/AlbertaHealthServicesRespiratoryVirusSurveillance/Summary (accessed on 12 April 2023).
- Government of Alberta. Alberta Influenza Statistics. Available online: https://www.alberta.ca/stats/influenza/influenza-statistics.htm#geospatial (accessed on 12 April 2023).
- Ackerson, B.K.; Sy, L.S.; Glenn, S.C.; Qian, L.; Park, C.H.; Riewerts, R.J.; Jacobsen, S.J. Pediatric vaccination during the COVID-19 pandemic. Pediatrics 2021, 148, e2020047092. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, S.E.; Paudel, Y.R.; Kiely, M.; Rafferty, E.; Sadarangani, M.; Robinson, J.L.; Driedger, S.M.; Svenson, L.W. Impact of the COVID-19 pandemic on vaccine coverage for early childhood vaccines in Alberta, Canada: A population-based retrospective cohort study. BMJ Open 2022, 12, e055968. [Google Scholar] [CrossRef] [PubMed]
- Government of Canada. Public Health Level Recommendations on the Use of Pneumococcal Vaccines in Adults, Including the Use of 15-Valent and 20-Valent Conjugate Vaccines. Available online: https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/public-health-level-recommendations-use-pneumococcal-vaccines-adults-including-use-15-valent-20-valent-conjugate-vaccines.html (accessed on 14 April 2023).




{kind=link}
{kind=link}
{kind=link}
| 2019 | 2020 | 2021 | 2022 | |||||
|---|---|---|---|---|---|---|---|---|
| Serotype | Children | Adults | Children | Adults | Children | Adults | Children | Adults |
| 7-valent vaccine serotypes | ||||||||
| 4 | 0 | 4 | 0 | 5 | 0 | 11 | 0 | 49 |
| 6B | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 9V | 0 | 0 | 0 | 1 | 0 | 2 | 0 | 7 |
| 14 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 18C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 19F | 1 | 2 | 1 | 1 | 0 | 1 | 3 | 1 |
| 23F | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 10-valent vaccine serotypes | ||||||||
| 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 7F | 0 | 20 | 0 | 10 | 1 | 7 | 0 | 12 |
| 13-valent vaccine serotypes | ||||||||
| 3 | 2 | 18 | 0 | 8 | 0 | 8 | 2 | 22 |
| 6A | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| 19A | 0 | 2 | 0 | 1 | 0 | 0 | 0 | 7 |
| 15-valent vaccine serotypes | ||||||||
| 22F | 4 | 12 | 1 | 6 | 1 | 6 | 2 | 8 |
| 33F | 0 | 3 | 0 | 0 | 0 | 1 | 0 | 3 |
| 20-valent vaccine serotypes | ||||||||
| 8 | 1 | 2 | 0 | 2 | 0 | 4 | 1 | 5 |
| 10A | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 4 |
| 11A | 0 | 2 | 0 | 3 | 0 | 0 | 2 | 4 |
| 12F | 0 | 6 | 0 | 9 | 0 | 0 | 0 | 2 |
| 15B | 0 | 3 | 0 | 0 | 1 | 0 | 2 | 1 |
| 23-valent polysaccharide vaccine serotypes | ||||||||
| 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 9N | 1 | 8 | 0 | 12 | 0 | 9 | 0 | 11 |
| 17F | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 |
| 20 | 0 | 11 | 0 | 4 | 0 | 4 | 2 | 10 |
| Other serotypes | ||||||||
| 6C | 0 | 2 | 0 | 1 | 0 | 3 | 0 | 1 |
| 7C | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 |
| 13 | 0 | 2 | 0 | 0 | 0 | 1 | 0 | 1 |
| 15A | 0 | 4 | 0 | 2 | 0 | 2 | 0 | 2 |
| 15C | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 1 |
| 16F | 0 | 3 | 0 | 2 | 0 | 1 | 0 | 2 |
| 21 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| 23A | 2 | 4 | 0 | 4 | 0 | 2 | 0 | 0 |
| 23B | 3 | 2 | 0 | 0 | 0 | 2 | 0 | 4 |
| 28A | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 |
| 29 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| 31 | 0 | 7 | 0 | 3 | 1 | 3 | 0 | 1 |
| 34 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 |
| 35B | 0 | 4 | 1 | 1 | 0 | 1 | 2 | 0 |
| 35F | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 |
| 38 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 0 |
| Missing | 0 | 0 | 0 | 0 | 1 | 1 | 5 | 9 |
| Total | 14 | 131 | 4 | 78 | 5 | 70 | 26 | 172 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ricketson, L.J.; Kellner, J.D. Changes in the Incidence of Invasive Pneumococcal Disease in Calgary, Canada, during the SARS-CoV-2 Pandemic 2020–2022. Microorganisms 2023, 11, 1333. https://doi.org/10.3390/microorganisms11051333
Ricketson LJ, Kellner JD. Changes in the Incidence of Invasive Pneumococcal Disease in Calgary, Canada, during the SARS-CoV-2 Pandemic 2020–2022. Microorganisms. 2023; 11(5):1333. https://doi.org/10.3390/microorganisms11051333
Chicago/Turabian StyleRicketson, Leah J., and James D. Kellner. 2023. "Changes in the Incidence of Invasive Pneumococcal Disease in Calgary, Canada, during the SARS-CoV-2 Pandemic 2020–2022" Microorganisms 11, no. 5: 1333. https://doi.org/10.3390/microorganisms11051333