
Cost-Effectiveness of Short Course of Ceftazidime/Avibactam for K. pneumoniae-KPC Bloodstream Infections in Italy
 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Methods
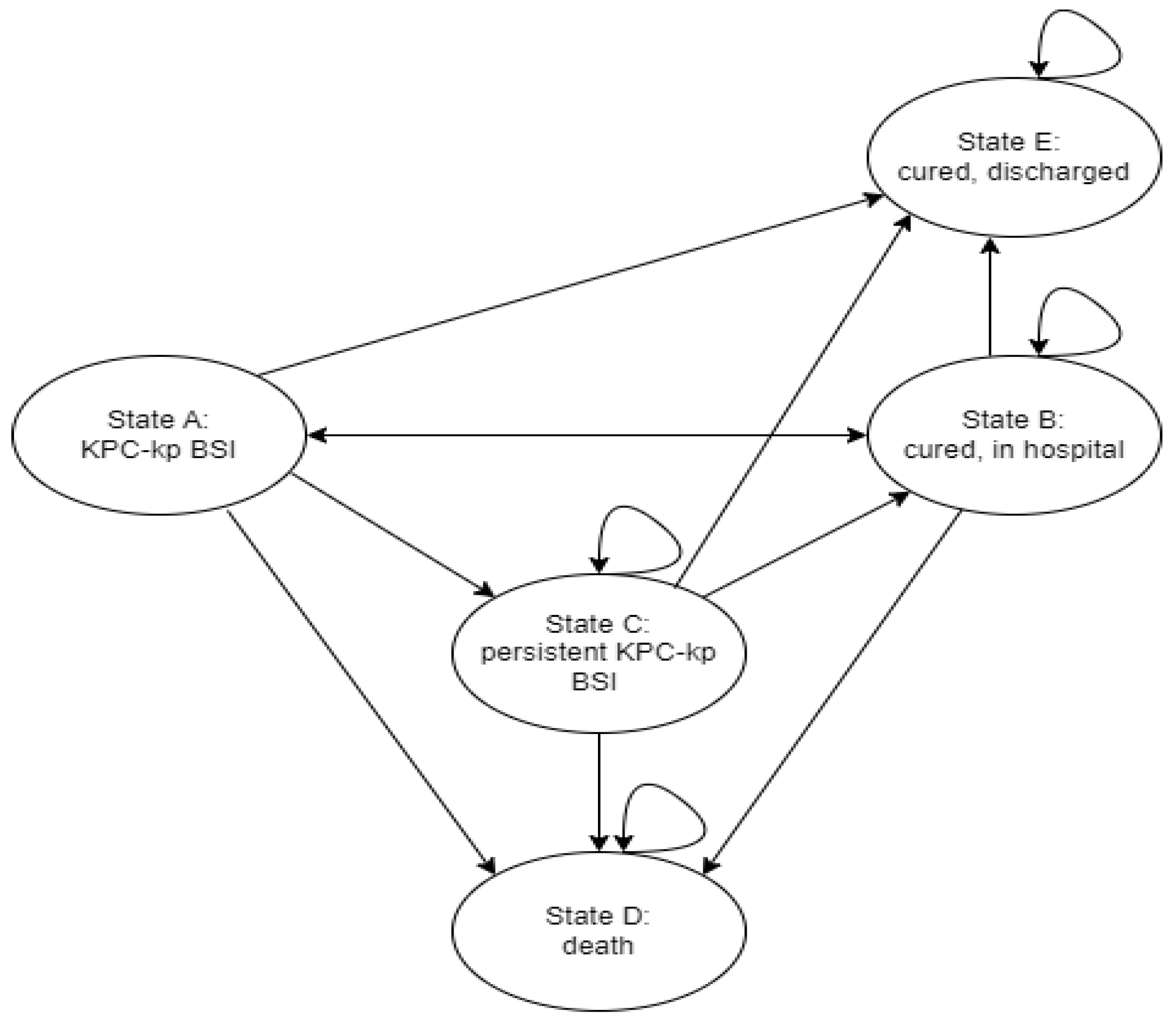
2.1. Model Design
2.2. Input Parameters
2.3. Cost-Utility Analysis
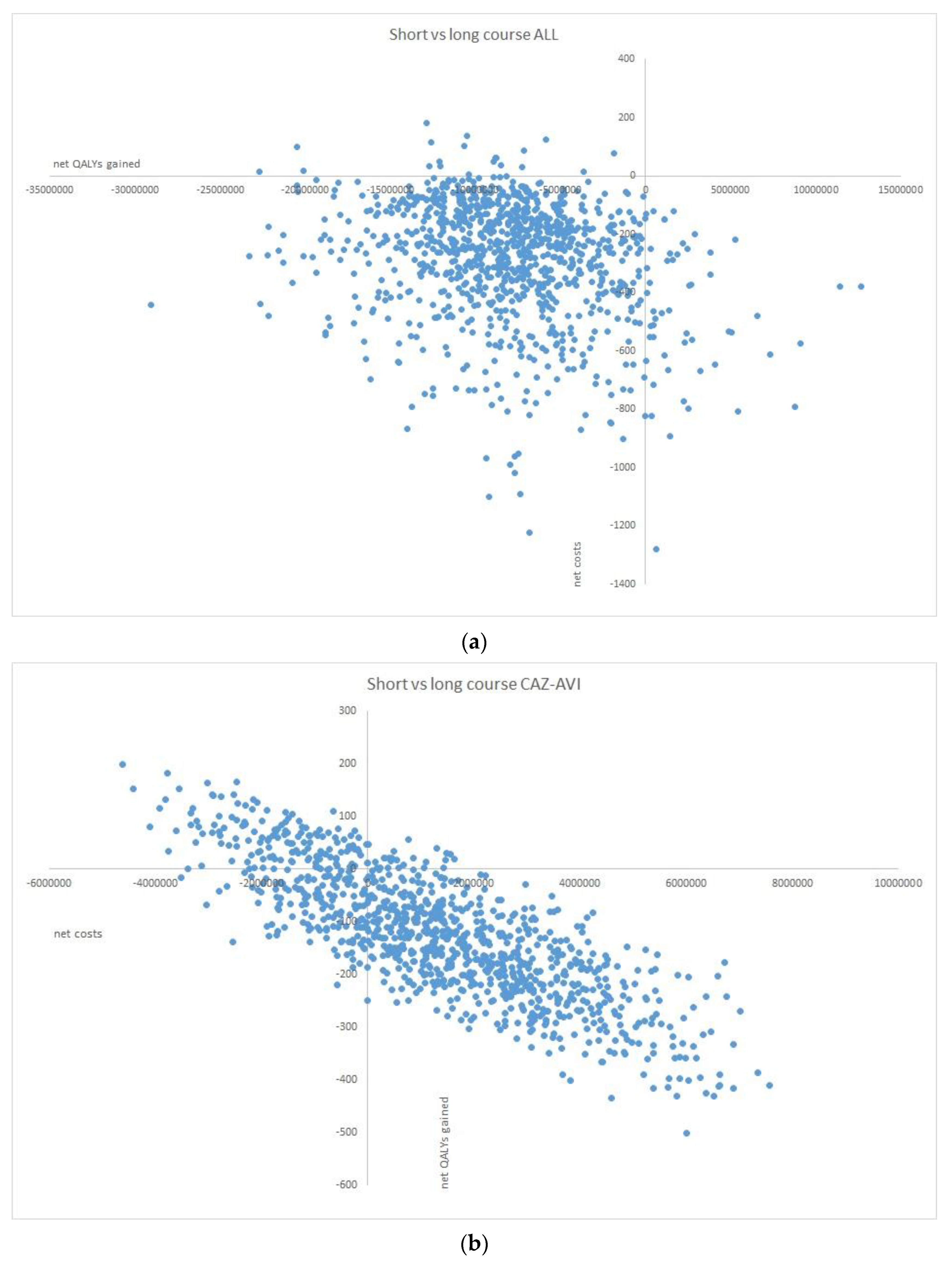
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Guidry, C.A.; Sawyer, R.G. Short-Course Antimicrobial Therapy for Intraabdominal Infection. N. Engl. J. Med. 2015, 373, 1578. [Google Scholar] [CrossRef] [PubMed]
- Pugh, R.; Grant, C.; Cooke, R.P.; Dempsey, G. Short-course versus prolonged-course antibiotic therapy for hospital-acquired pneumonia in critically ill adults. Cochrane Database Syst. Rev. 2015, 2015, CD007577. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Imaeda, T.; Nakada, T.A.; Oami, T.; Abe, T.; Yamao, Y.; Nakagawa, S.; Ogura, H.; Shime, N.; Matsushima, A.; et al. Short-versus long-course antibiotic therapy for sepsis: A post hoc analysis of the nationwide cohort study. J. Intensive Care 2022, 10, 49. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.; Montero-Mateos, E.; Praena-Segovia, J.; León-Jiménez, E.; Natera, C.; López-Cortés, L.E.; Valiente, L.; Rosso-Fernández, C.M.; Herrero, M.; Aller-García, A.I.; et al. Seven-versus 14-day course of antibiotics for the treatment of bloodstream infections by Enterobacterales: A randomized, controlled trial. Clin. Microbiol. Infect. 2022, 28, 550–557. [Google Scholar] [CrossRef]
- Yahav, D.; Franceschini, E.; Koppel, F.; Turjeman, A.; Babich, T.; Bitterman, R.; Neuberger, A.; Ghanem-Zoubi, N.; Santoro, A.; Eliakim-Raz, N.; et al. Seven Versus 14 Days of Antibiotic Therapy for Uncomplicated Gram-negative Bacteremia: A Noninferiority Randomized Controlled Trial. Clin. Infect. Dis. 2019, 69, 1091–1098. [Google Scholar] [CrossRef]
- von Dach, E.; Albrich, W.C.; Brunel, A.S.; Prendki, V.; Cuvelier, C.; Flury, D.; Gayet-Ageron, A.; Huttner, B.; Kohler, P.; Lemmenmeier, E.; et al. Effect of C-Reactive Protein–Guided Antibiotic Treatment Duration, 7-Day Treatment, or 14-Day Treatment on 30-Day Clinical Failure Rate in Patients With Uncomplicated Gram-Negative Bacteremia: A Randomized Clinical Trial. JAMA 2020, 323, 2160–2169. [Google Scholar] [CrossRef]
- Turjeman, A.; von Dach, E.; Molina, J.; Franceschini, E.; Koppel, F.; Yelin, D.; Dishon-Benattar, Y.; Mussini, C.; Rodríguez-Baño, J.; Cisneros, J.M.; et al. Duration of antibiotic treatment for Gram-negative bacteremia—Systematic review and individual participant data (IPD) meta-analysis. EClinicalMedicine 2022, 55, 101750. [Google Scholar] [CrossRef]
- Ruiz-Ruigómez, M.; Fernández-Ruiz, M.; San-Juan, R.; López-Medrano, F.; Orellana, M.Á.; Corbella, L.; Rodríguez-Goncer, I.; Hernández Jiménez, P.; Aguado, J.M. Impact of duration of antibiotic therapy in central venous catheter-related blood-stream infection due to Gram-negative bacilli. J. Antimicrob. Chemother. 2020, 75, 3049–3055. [Google Scholar] [CrossRef]
- Rodríguez-Baño, J.; Gutiérrez-Gutiérrez, B.; Machuca, I.; Pascual, A. Treatment of Infections Caused by Extended-Spectrum-Beta-Lactamase-, AmpC-, and Carbapenemase-Producing Enterobacteriaceae. Clin. Microbiol. Rev. 2018, 31, e00079-17. [Google Scholar] [CrossRef]
- van Duin, D.; Bonomo, R.A. Ceftazidime/Avibactam and Ceftolozane/Tazobactam: Second-generation β-Lactam/β-Lactamase Inhibitor Combinations. Clin. Infect. Dis. 2016, 63, 234–241. [Google Scholar] [CrossRef]
- Wagenlehner, F.M.; Sobel, J.D.; Newell, P.; Armstrong, J.; Huang, X.; Stone, G.G.; Yates, K.; Gasink, L.B. Ceftazidime-avibactam versus doripenem for the treatment of complicated urinary tract infections, including acute pyelonephritis: RECAPTURE, a phase 3 randomized trial program. Clin. Infect. Dis. 2016, 63, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Shields, R.K.; Nguyen, M.H.; Chen, L.; Press, E.G.; Potoski, B.A.; Marini, R.V.; Doi, Y.; Kreiswirth, B.N.; Clancy, C.J. Ceftazidime-avibactam is superior to other treatment regimens against carbapenem-resistant Klebsiella pneumoniae bacteremia. Antimicrob. Agents Chemother. 2017, 61, 8. [Google Scholar] [CrossRef] [PubMed]
- Van Duin, D.; Lok, J.J.; Earley, M.; Cober, E.; Richter, S.S.; Perez, F.; Salata, R.A.; Kalayjian, R.C.; Watkins, R.R.; Doi, Y.; et al. Antibacterial Resistance Leadership Group. Colistin versus ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae. Clin. Infect. Dis. 2018, 66, 163–171. [Google Scholar] [CrossRef]
- Jorgensen, S.C.; Trinh, T.D.; Zasowski, E.J.; Lagnf, A.M.; Bhatia, S.; Melvin, S.M.; Steed, M.E.; Simon, S.P.; Estrada, S.J.; Morrisette, T.; et al. Real-world experience with ceftazidime-avibactam for multidrug-resistant gram-negative bacterial infections. Open Forum Infect. Dis. 2019, 6, ofz522. [Google Scholar] [CrossRef]
- Tumbarello, M.; Trecarichi, E.M.; Corona, A.; De Rosa, F.G.; Bassetti, M.; Mussini, C.; Menichetti, F.; Viscoli, C.; Campoli, C.; Venditti, M.; et al. Efficacy of ceftazidime-avibactam salvage therapy in patients with infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae. Clin. Infect. Dis. 2019, 68, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Tsolaki, V.; Mantzarlis, K.; Mpakalis, A.; Malli, E.; Tsimpoukas, F.; Tsirogianni, A.; Papagiannitsis, C.; Zygoulis, P.; Papadonta, M.E.; Petinaki, E.; et al. Ceftazidime-avibactam to treat life-threatening infections by carbapenem-resistant pathogens in critically ill mechanically ventilated patients. Antimicrob. Agents Chemother. 2020, 64, e02320-19. [Google Scholar] [CrossRef]
- Corcione, S.; De Benedetto, I.; Shbaklo, N.; Ranzani, F.; Mornese Pinna, S.; Castiglione, A.; Scabini, S.; Bianco, G.; Cavallo, R.; Mirabella, S.; et al. Ten Years of KPC-Kp Bloodstream Infections Experience: Impact of Early Appropriate Empirical Therapy on Mortality. Biomedicines 2022, 10, 3268. [Google Scholar] [CrossRef] [PubMed]
- Tichy, E.; Torres, A.; Bassetti, M.; Kongnakorn, T.; Di Virgilio, R.; Irani, P.; Charbonneau, C. Cost-effectiveness Comparison of Ceftazidime/Avibactam Versus Meropenem in the Empirical Treatment of Hospital-acquired Pneumonia, Including Ventilator-associated Pneumonia, in Italy. Clin. Ther. 2020, 42, 802–817. [Google Scholar] [CrossRef]
- Torres, A.; Zhong, N.; Pachl, J.; Timsit, J.F.; Kollef, M.; Chen, Z.; Song, J.; Taylor, D.; Laud, P.J.; Stone, G.G.; et al. Ceftazidime-avibactam versus meropenem in nosocomial pneumonia, including ventilator-associated pneumonia (REPROVE): A randomised, double-blind, phase 3 non-inferiority trial. Lancet Infect. Dis. 2018, 18, 285–295. [Google Scholar] [CrossRef]
- Mazuski, J.E.; Gasink, L.B.; Armstrong, J.; Broadhurst, H.; Stone, G.G.; Rank, D.; Llorens, L.; Newell, P.; Pachl, J. Efficacy and safety of ceftazidime-avibactam plus metronidazole versus meropenem in the treatment of complicated intra-abdominal infection: Results from a randomized, controlled, double-blind, phase 3 program. Clin. Infect. Dis. 2016, 62, 1380–1389. [Google Scholar] [CrossRef]
- Kongnakorn, T.; Eckmann, C.; Bassetti, M.; Tichy, E.; Di Virgilio, R.; Baillon-Plot, N.; Charbonneau, C. Cost-effectiveness analysis comparing ceftazidime/avibactam (CAZ/AVI) as empirical treatment comparing to ceftolozane/tazobactam and to meropenem for complicated intra-abdominal infection (cIAI). Antimicrob. Resist. Infect. Control 2019, 8, 204. [Google Scholar] [CrossRef] [PubMed]
- Messori, A.; Trippoli, S. Estimation of Value-Based Price for Five High-Technology Medical Devices Approved by a Regional Health Technology Assessment Committee in Italy. Cureus 2022, 14, e24695. [Google Scholar] [CrossRef] [PubMed]
- Mosley, J.F., II; Smith, L.L.; Parke, C.K.; Brown, J.A.; Wilson, A.L.; Gibbs, L.V. 2016. Ceftazidime-avibactam (Avycaz): For the treatment of complicated intraabdominal and urinary tract infections. Pharm. Ther. 2016, 41, 479–483. [Google Scholar] [CrossRef]
- Simon, M.S.; Sfeir, M.M.; Calfee, D.P.; Satlin, M.J. Cost-effectiveness of ceftazidime-avibactam for treatment of carbapenem-resistant Enterobacteriaceae bacteremia and pneumonia. Antimicrob. Agents Chemother. 2019, 63, e00897-19. [Google Scholar] [CrossRef] [PubMed]
- Guh, A.Y.; Bulens, S.N.; Mu, Y.; Jacob, J.T.; Reno, J.; Scott, J.; Wilson, L.E.; Vaeth, E.; Lynfield, R.; Shaw, K.M.; et al. Epidemiology of Carbapenem-Resistant Enterobacteriaceae in 7 US Communities, 2012–2013. JAMA 2015, 314, 1479–1487. [Google Scholar] [CrossRef]
- Messina, J.A.; Cober, E.; Richter, S.S.; Perez, F.; Salata, R.A.; Kalayjian, R.C.; Watkins, R.R.; Scalera, N.M.; Doi, Y.; Kaye, K.S.; et al. Hospital Readmissions in Patients With Carbapenem-Resistant Klebsiella pneumoniae. Infect. Control Hosp. Epidemiol. 2016, 37, 281–288. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe/European Centre for Disease Prevention and Control. Antimicrobial Resistance Surveillance in Europe 2022–2020 Data; WHO Regional Office for Europe: Copenhagen, Denmark, 2022. [Google Scholar]
- Koukoubani, T.; Makris, D.; Daniil, Z.; Paraforou, T.; Tsolaki, V.; Zakynthinos, E.; Papanikolaou, J. The role of antimicrobial resistance on long-term mortality and quality of life in critically ill patients: A prospective longitudinal 2-year study. Health Qual. Life Outcomes 2021, 19, 72. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Short Course (<7 Days) | Long Course (≥7 Days) Old Appropriate Treatment | Long Course (≥7 Days) CAZ/AVI | |||||
|---|---|---|---|---|---|---|---|
| Transition | Probability description | Literature estimates | Point estimate of probability (estimated SD) | Literature estimates | Point estimate of probability (estimated SD) | Literature estimates | Point estimate of probability (estimated SD) |
| P(A to C) | Probability of persistent KPC-Kp BSI (microbiological failure) | 8/110 [4] 3/169 [6] | 0.039 (0.05) | 12/122 [4] 2/165 [6] 1/31 [19] | 0.047 (0.05) | 0/14 [19] | 0 (0.05) |
| P(A to D) | Probability of death due to primary KPC-Kp BSI | * | 4/31 [19] | 0.129 (0.05) | 2/14 [19] | 0.143 (0.05) | |
| P(A to E) | Probability of cure and discharge within one month after primary KPC-Kp BSI | * | 2/31 [19] | 0.065 (0.05) | 1/14 [19] | 0.071 (0.05) | |
| P(A to B) | Probability of cure without discharge within one month after primary KPC-Kp BSI | Mathematical extrapolation: 1–P(A to C)–P(A to D)–P(A to E) | |||||
| P(B to A) | Probability of relapse after microbiological cure | 7/108 [4] 1/169 [6] 8/306 [5] | 0.027 (0.02) | 6/121 [4] 2/165 [6] 8/298 [5] 3/31 [19] | 0.031 (0.02) | 1/14 [19] | 0.071 (0.02) |
| P(B to D) | Probability of death (in hospital) after cure | * | 0/31 [19] | 0 (0.05) | 0/14 [19] | 0 (0.05) | |
| P(B to E) | Probability of being discharged after 1 month following microbiological cure | * | 1/Median LOS in months: 3.0 (IQR 2.54–4.49) [19] | 0.333 (0.223–0.393) | 1/Median LOS in months: 2.93 (IQR 2.37–3.07) [19] | 0.341 (0.326–0.423) | |
| P(B to B) | Probability of remaining in hospital after cure | Mathematical extrapolation: 1–P(B to A)–P(B to D)–P(B to E) | |||||
| P(C to C) | Probability of persistent KPC-Kp BSI (microbiological failure) over 1 month | * | 0/5 [19] | 0 (0.05) | * | ||
| P(C to D) | Probability of death due to persistent KPC-Kp BSI over 1 month | * | 1/5 [19] | 0.2 (0.05) | * | ||
| P(C to E) | Probability of cure and discharge within one month after persistent KPC-Kp BSI | * | 1/5 [6] | 0.2 (0.05) | * | ||
| P(C to B) | Probability of cure without discharge within one month after persistent KPC-Kp BSI | Mathematical extrapolation: 1–P(C to C)–P(C to D)–P(C to E) | |||||
| Health State | Old Appropriate Treatment Model * | CAZ/AVI Model | |
|---|---|---|---|
| Short Course * | Long Course ** | ||
| A | 21,619.36 (19,721.52–23,513.52) | 22,831.48 (20,933.64–24,725.64) | 23,524.12 (21,626.28–25,418.28) |
| B | 23,308.57 (21,408.96–25,200.96) | 23,308.57 (21,408.96–25,200.96) | 23,308.57 (21,408.96–25,200.96) |
| C | 29,448 (27,552–31,344) | 30,660.12 (28,764.12–32,556.12) | 31,352.76 (29,456.76–33,248.76) |
| Old Appropriate Treatment Model | CAZ/AVI Model | |||||
|---|---|---|---|---|---|---|
| Short Course (<7 Days) | Long Course (≥7 Days) | Delta | Short Course (<7 Days) | Long Course (≥7 Days) | Delta | |
| Costs per patient, € | 78,121.88 | 82,940.49 | −4818.60 | 79,459.61 | 78,161.71 | 1297.9 |
| QALYs per patient | 1.9 | 2 | −0.10 | 1.9 | 1.86 | 0.04 |
| ICER | 49,959.59 | 32,317.82 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Benedetto, I.; Shbaklo, N.; Vicentini, C.; Zotti, C.M.; De Rosa, F.G.; Corcione, S. Cost-Effectiveness of Short Course of Ceftazidime/Avibactam for K. pneumoniae-KPC Bloodstream Infections in Italy. Microorganisms 2023, 11, 1102. https://doi.org/10.3390/microorganisms11051102
De Benedetto I, Shbaklo N, Vicentini C, Zotti CM, De Rosa FG, Corcione S. Cost-Effectiveness of Short Course of Ceftazidime/Avibactam for K. pneumoniae-KPC Bloodstream Infections in Italy. Microorganisms. 2023; 11(5):1102. https://doi.org/10.3390/microorganisms11051102
Chicago/Turabian StyleDe Benedetto, Ilaria, Nour Shbaklo, Costanza Vicentini, Carla Maria Zotti, Francesco Giuseppe De Rosa, and Silvia Corcione. 2023. "Cost-Effectiveness of Short Course of Ceftazidime/Avibactam for K. pneumoniae-KPC Bloodstream Infections in Italy" Microorganisms 11, no. 5: 1102. https://doi.org/10.3390/microorganisms11051102