
Adaptation of Brucella melitensis Antimicrobial Susceptibility Testing to the ISO 20776 Standard and Validation of the Method

 , , , , , , , , , ,
on behalf of the EMERGE AST Working Groupadd
Show full author list
, , , , , , , , , ,
on behalf of the EMERGE AST Working Groupadd
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Bacterial Strains and Culture Conditions
2.2. Culture Media
2.3. Correlation of the McFarland Standard and Bacterial Cell Counts
2.4. Broth Microdilution Method
2.5. Agar Dilution Method
2.6. Growth Curve Analysis
2.7. Interlaboratory Validation
2.8. Data Analysis
3. Results
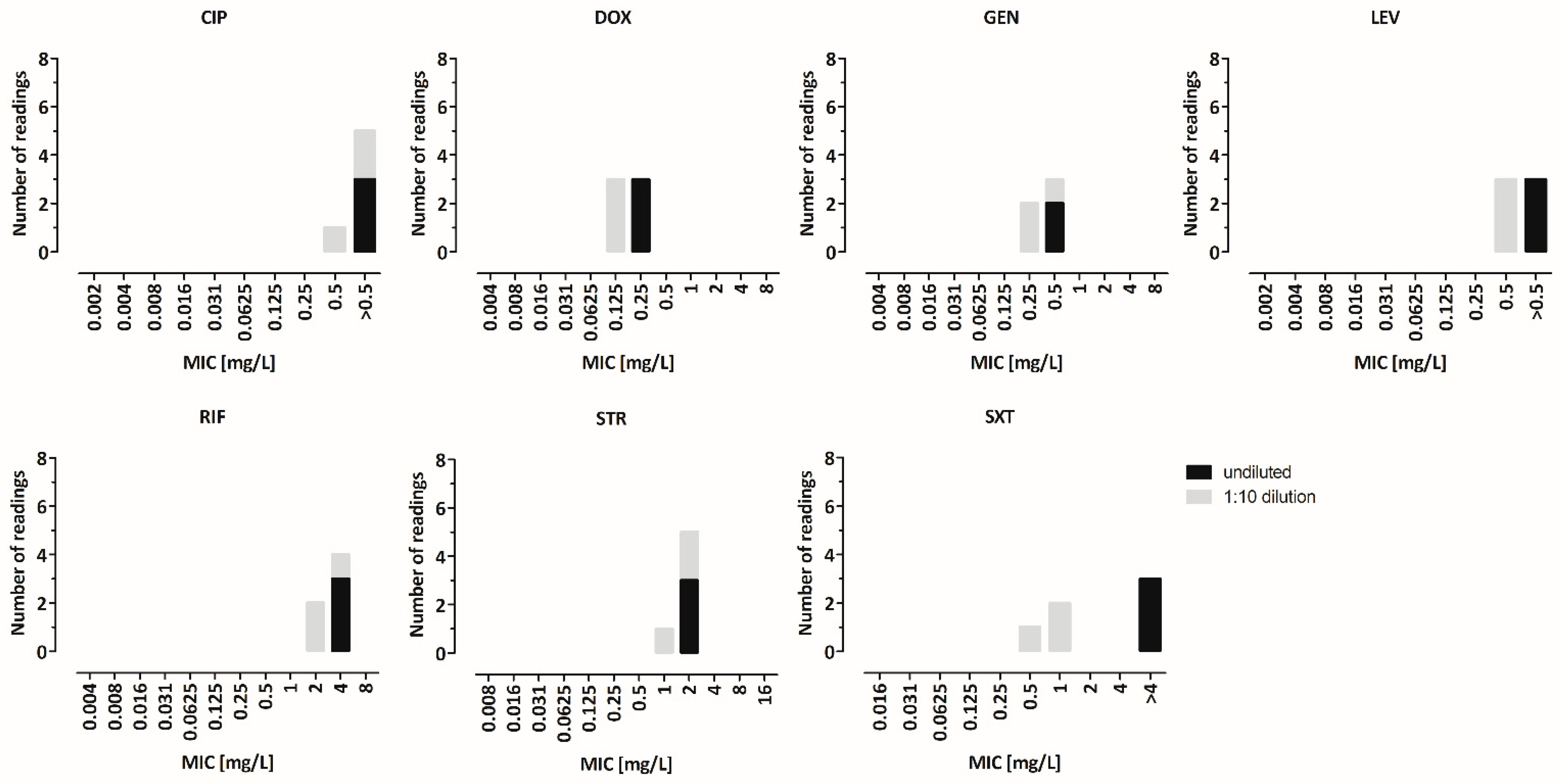
3.1. CFU of the Bacterial Inoculum and Its Impact on the MIC Endpoints
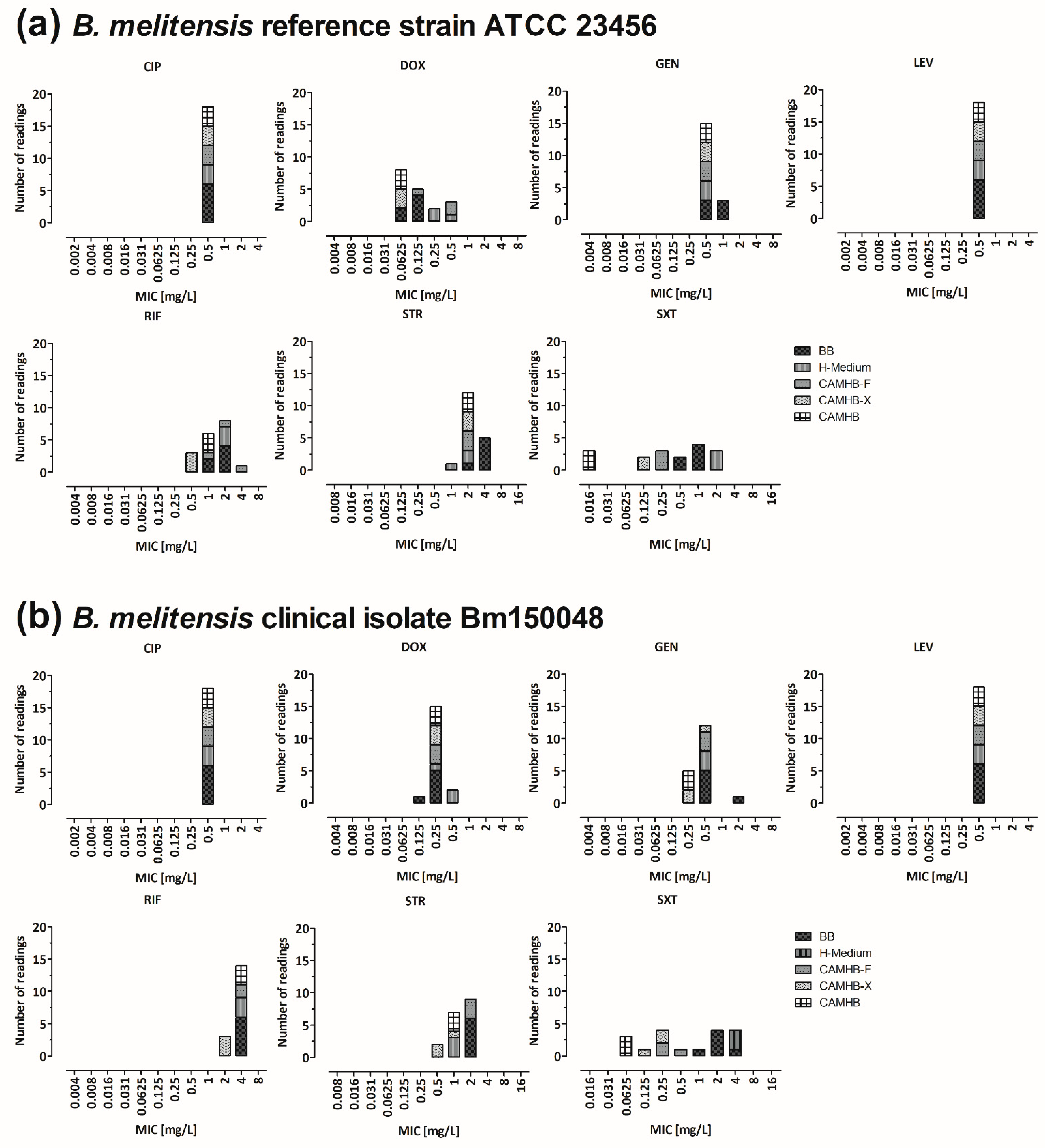
3.2. Comparison of the MICs in Different Culture Media
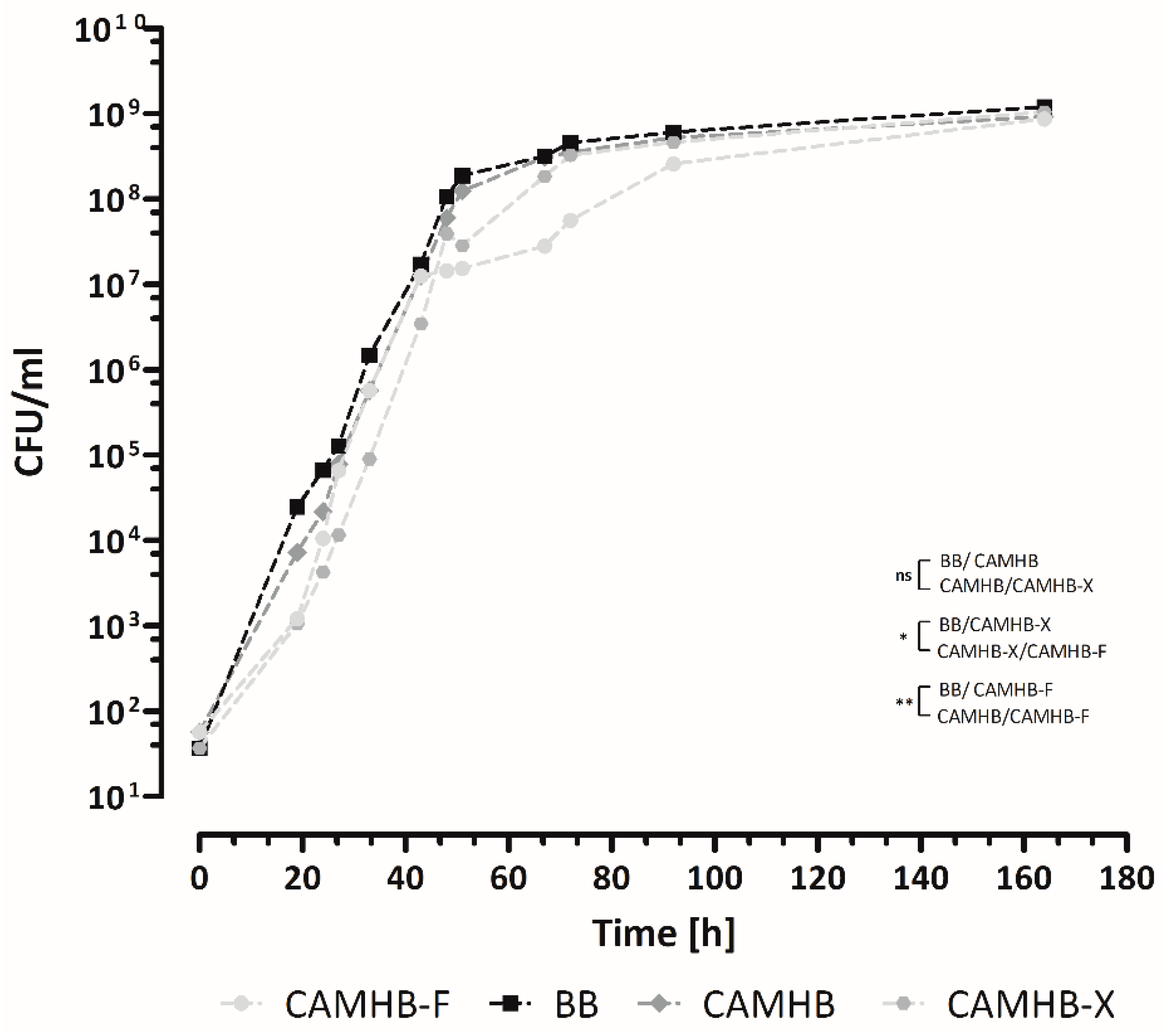
3.3. B. melitensis Growth Curves in Different Culture Media
3.4. Broth Microdilution vs. Agar Dilution with BB vs. CAMHB
3.5. Impact of the Incubation Time on the MIC Values
3.6. Impact of the Cultivation Atmosphere on the MIC Values
3.7. Interlaboratory Validation
3.8. Re-Evaluation with Clinical Isolates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seleem, M.N.; Boyle, S.M.; Sriranganathan, N. Brucellosis: A re-emerging zoonosis. Vet. Microbiol. 2010, 140, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Moreno, E. Retrospective and prospective perspectives on zoonotic brucellosis. Front. Microbiol. 2014, 5, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Centre for Disease Prevention and Control. Surveillance Atlas of Infectious Diseases. Available online: http://atlas.ecdc.europa.eu/public/index.aspx (accessed on 12 May 2022).
- European Food Safety Authority; European Centre for Disease Prevention and Control. The European Union One Health 2018 Zoonoses Report. EFSA J. 2019, 17, e05926. [Google Scholar] [CrossRef] [Green Version]
- European Food Safety Authority; European Centre for Disease Prevention and Control. The European Union One Health 2019 Zoonoses Report. EFSA J. 2021, 19, e06406. [Google Scholar] [CrossRef]
- Nenova, R.; Tomova, I.; Saparevska, R.; Kantardjiev, T. A new outbreak of brucellosis in Bulgaria detected in July 2015—Preliminary report. Euro Surveill. 2015, 20, 30031. [Google Scholar] [CrossRef] [Green Version]
- Karagiannis, I.; Mellou, K.; Gkolfinopoulou, K.; Dougas, G.; Theocharopoulos, G.; Vourvidis, D.; Ellinas, D.; Sotolidou, M.; Papadimitriou, T.; Vorou, R. Outbreak investigation of brucellosis in Thassos, Greece, 2008. Euro Surveill. 2012, 17, 20116. [Google Scholar] [CrossRef]
- Pelerito, A.; Cordeiro, R.; Matos, R.; Santos, M.A.; Soeiro, S.; Santos, J.; Manita, C.; Rio, C.; Santo, M.; Paixão, E.; et al. Human brucellosis in Portugal-Retrospective analysis of suspected clinical cases of infection from 2009 to 2016. PLoS ONE 2017, 12, e0179667. [Google Scholar] [CrossRef] [Green Version]
- Cama, B.A.V.; Ceccarelli, M.; Venanzi Rullo, E.; Ferraiolo, F.; Paolucci, I.A.; Maranto, D.; Mondello, P.; Lo Presti Costantino, M.R.; Marano, F.; D’Andrea, G.; et al. Outbreak of Brucella melitensis infection in Eastern Sicily: Risk factors, clinical characteristics and complication rate. New Microbiol. 2019, 42, 43–48. [Google Scholar]
- Dean, A.S.; Crump, L.; Greter, H.; Hattendorf, J.; Schelling, E.; Zinsstag, J. Clinical manifestations of human brucellosis: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2012, 6, e1929. [Google Scholar] [CrossRef] [Green Version]
- Franco, M.P.; Mulder, M.; Gilman, R.H.; Smits, H.L. Human brucellosis. Lancet Infect. Dis. 2007, 7, 775–786. [Google Scholar] [CrossRef]
- Bossi, P.; Tegnell, A.; Baka, A.; van Loock, F.; Hendriks, J.; Werner, A.; Maidhof, H.; Gouvras, G. Bichat guidelines for the clinical management of brucellosis and bioterrorism-related brucellosis. Euro Surveill. 2004, 9, E15–E16. [Google Scholar] [CrossRef] [PubMed]
- Solera, J.; Martínez-Alfaro, E.; Espinosa, A. Recognition and optimum treatment of brucellosis. Drugs 1997, 53, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Solera, J. Update on brucellosis: Therapeutic challenges. Int. J. Antimicrob. Agents 2010, 36 (Suppl. S1), S18–S20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosilkovski, M.; Keramat, F.; Arapović, J. The current therapeutical strategies in human brucellosis. Infection 2021, 49, 823–832. [Google Scholar] [CrossRef]
- Falagas, M.E.; Bliziotis, I.A. Quinolones for treatment of human brucellosis: Critical review of the evidence from microbiological and clinical studies. Antimicrob. Agents Chemother. 2006, 50, 22–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ariza, J.; Bosilkovski, M.; Cascio, A.; Colmenero, J.D.; Corbel, M.J.; Falagas, M.E.; Memish, Z.A.; Roushan, M.R.H.; Rubinstein, E.; Sipsas, N.V.; et al. Perspectives for the treatment of brucellosis in the 21st century: The Ioannina recommendations. PLoS Med. 2007, 4, e317. [Google Scholar] [CrossRef] [Green Version]
- Erdem, H.; Ulu-Kilic, A.; Kilic, S.; Karahocagil, M.; Shehata, G.; Eren-Tulek, N.; Yetkin, F.; Celen, M.K.; Ceran, N.; Gul, H.C.; et al. Efficacy and tolerability of antibiotic combinations in neurobrucellosis: Results of the Istanbul study. Antimicrob. Agents Chemother. 2012, 56, 1523–1528. [Google Scholar] [CrossRef] [Green Version]
- Pappas, G.; Akritidis, N.; Christou, L. Treatment of neurobrucellosis: What is known and what remains to be answered. Expert Rev. Anti-Infect. Ther. 2007, 5, 983–990. [Google Scholar] [CrossRef]
- Baron, E.J.; Miller, J.M. Bacterial and fungal infections among diagnostic laboratory workers: Evaluating the risks. Diagn. Microbiol. Infect. Dis. 2008, 60, 241–246. [Google Scholar] [CrossRef]
- Pike, R.M. Laboratory-associated infections: Incidence, fatalities, causes, and prevention. Annu. Rev. Microbiol. 1979, 33, 41–66. [Google Scholar] [CrossRef] [Green Version]
- Sayan, M.; Yumuk, Z.; Dündar, D.; Bilenoglu, O.; Erdenlig, S.; Yaşar, E.; Willke, A. Rifampicin resistance phenotyping of Brucella melitensis by rpoB gene analysis in clinical isolates. J. Chemother. 2008, 20, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Marianelli, C.; Ciuchini, F.; Tarantino, M.; Pasquali, P.; Adone, R. Genetic bases of the rifampin resistance phenotype in Brucella spp. J. Clin. Microbiol. 2004, 42, 5439–5443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Rautlin de la Roy, Y.M.; Grignon, B.; Grollier, G.; Coindreau, M.F.; Becq-Giraudon, B. Rifampicin resistance in a strain of Brucella melitensis after treatment with doxycycline and rifampicin. J. Antimicrob. Chemother. 1986, 18, 648–649. [Google Scholar] [CrossRef] [PubMed]
- Gerhardt, P. The nutrition of brucellae. Bacteriol. Rev. 1958, 22, 81–98. [Google Scholar] [CrossRef]
- Maves, R.C.; Castillo, R.; Guillen, A.; Espinosa, B.; Meza, R.; Espinoza, N.; Núñez, G.; Sánchez, L.; Chacaltana, J.; Cepeda, D.; et al. Antimicrobial susceptibility of Brucella melitensis isolates in Peru. Antimicrob. Agents Chemother. 2011, 55, 1279–1281. [Google Scholar] [CrossRef] [Green Version]
- Deshmukh, A.; Hagen, F.; Sharabasi, O.A.; Abraham, M.; Wilson, G.; Doiphode, S.; Maslamani, M.A.; Meis, J.F. In vitro antimicrobial susceptibility testing of human Brucella melitensis isolates from Qatar between 2014–2015. BMC Microbiol. 2015, 15, 121. [Google Scholar] [CrossRef] [Green Version]
- Gür, D.; Kocagöz, S.; Akova, M.; Unal, S. Comparison of E test to microdilution for determining in vitro activities of antibiotics against Brucella melitensis. Antimicrob. Agents Chemother. 1999, 43, 2337. [Google Scholar] [CrossRef] [Green Version]
- Akova, M.; Gür, D.; Livermore, D.M.; Kocagöz, T.; Akalin, H.E. In vitro activities of antibiotics alone and in combination against Brucella melitensis at neutral and acidic pHs. Antimicrob. Agents Chemother. 1999, 43, 1298–1300. [Google Scholar] [CrossRef] [Green Version]
- Rubinstein, E.; Lang, R.; Shasha, B.; Hagar, B.; Diamanstein, L.; Joseph, G.; Anderson, M.; Harrison, K. In vitro susceptibility of Brucella melitensis to antibiotics. Antimicrob. Agents Chemother. 1991, 35, 1925–1927. [Google Scholar] [CrossRef] [Green Version]
- Clinical and Laboratory Standards Institute. Methods for Antimicrobial Dilution and Disk Susceptibility Testing of Infrequently Isolated or Fastidious Bacteria, M45, 3rd ed.; CLSI Guideline M45; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2016. [Google Scholar]
- Georgi, E.; Walter, M.C.; Pfalzgraf, M.-T.; Northoff, B.H.; Holdt, L.M.; Scholz, H.C.; Zoeller, L.; Zange, S.; Antwerpen, M.H. Whole genome sequencing of Brucella melitensis isolated from 57 patients in Germany reveals high diversity in strains from Middle East. PLoS ONE 2017, 12, e0175425. [Google Scholar] [CrossRef] [Green Version]
- Johansen, T.B.; Scheffer, L.; Jensen, V.K.; Bohlin, J.; Feruglio, S.L. Whole-genome sequencing and antimicrobial resistance in Brucella melitensis from a Norwegian perspective. Sci. Rep. 2018, 8, 8538. [Google Scholar] [CrossRef] [PubMed]
- ISO 20776-1:2006; Clinical Laboratory Testing and In Vitro Diagnostic Test Systems—Susceptibility Testing of Infectious Agents and Evaluation of Performance of Antimicrobial Susceptibility Test Devices—Part 1: Reference Method for Testing the In Vitro Activity of Antimicrobial Agents against Rapidly Growing Aerobic Bacteria Involved in Infectious Diseases. International Organization for Standardization: Geneva, Switzerland, 2006.
- López-Goñi, I.; García-Yoldi, D.; Marín, C.M.; de Miguel, M.J.; Muñoz, P.M.; Blasco, J.M.; Jacques, I.; Grayon, M.; Cloeckaert, A.; Ferreira, A.C.; et al. Evaluation of a multiplex PCR assay (Bruce-ladder) for molecular typing of all Brucella species, including the vaccine strains. J. Clin. Microbiol. 2008, 46, 3484–3487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing. Media Preparation for EUCAST Disk Diffusion Testing and for Determination of MIC Values by the Broth Microdilution Method. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Disk_test_documents/2020_manuals/Media_preparation_v_6.0_EUCAST_AST (accessed on 12 May 2022).
- The European Committee on Antimicrobial Susceptibility Testing. Routine and Extended Internal Quality Control for MIC Determination and Disk Diffusion as Recommended by EUCAST. Version 10.0. 2020. Available online: http://www.eucast.org (accessed on 12 May 2022).
- European Committee for Antimicrobial Susceptibility Testing (EUCAST) of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID). EUCAST Definitive Document E.DEF 3.1, June 2000: Determination of minimum inhibitory concentrations (MICs) of antibacterial agents by agar dilution. Clin. Microbiol. Infect. 2000, 6, 509–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barry, A.L.; Fuchs, P.C.; Jones, R.N. Statistical criteria for selecting quality control limits for broth microdilution susceptibility tests with 39 different antimicrobial agents. Diagn. Microbiol. Infect. Dis. 1989, 12, 413–420. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing M100 S, 26th ed.; CLSI Guideline M45; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2016. [Google Scholar]
- Turkmani, A.; Ioannidis, A.; Christidou, A.; Psaroulaki, A.; Loukaides, F.; Tselentis, Y. In vitro susceptibilities of Brucella melitensis isolates to eleven antibiotics. Ann. Clin. Microbiol. Antimicrob. 2006, 5, 24. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Maksoud, M.; House, B.; Wasfy, M.; Abdel-Rahman, B.; Pimentel, G.; Roushdy, G.; Dueger, E. In vitro antibiotic susceptibility testing of Brucella isolates from Egypt between 1999 and 2007 and evidence of probable rifampin resistance. Ann. Clin. Microbiol. Antimicrob. 2012, 11, 24. [Google Scholar] [CrossRef] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 12.0. 2022. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_10.0_Breakpoint_Tables.pdf (accessed on 12 May 2022).
- Memish, Z.; Mah, M.W.; Al Mahmoud, S.; Al Shaalan, M.; Khan, M.Y. Brucella bacteraemia: Clinical and laboratory observations in 160 patients. J. Infect. 2000, 40, 59–63. [Google Scholar] [CrossRef]
- Stokes, A.; Lacey, R.W. Effect of thymidine on activity of trimethoprim and sulphamethoxazole. J. Clin. Pathol. 1978, 31, 165–171. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.D.; Traczewski, M.M. Broth microdilution susceptibility testing of Brucella species: Quality control limits for ten antimicrobial agents against three standard quality control strains. J. Clin. Microbiol. 2005, 43, 5804–5807. [Google Scholar] [CrossRef] [Green Version]
- Sutton, S. Measurement of microbial cells by optical density. J. Valid. Technol. 2011, 17, 46–49. [Google Scholar]
- Koch, A.L.; Gross, G.H. Growth conditions and rifampin susceptibility. Antimicrob. Agents Chemother. 1979, 15, 220–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lonsway, D.R.; Jevitt, L.A.; Uhl, J.R.; Cockerill, F.R.; Anderson, M.E.; Sullivan, M.M.; De, B.K.; Edwards, J.R.; Patel, J.B. Effect of carbon dioxide on broth microdilution susceptibility testing of Brucella spp. J. Clin. Microbiol. 2010, 48, 952–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Etayo, L.; de Miguel, M.J.; Conde-Álvarez, R.; Muñoz, P.M.; Khames, M.; Iriarte, M.; Moriyón, I.; Zúñiga-Ripa, A. The CO2-dependence of Brucella ovis and Brucella abortus biovars is caused by defective carbonic anhydrases. Vet. Res. 2018, 49, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing. EUCAST Reading Guide for Broth Microdilution. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/MIC_testing/Reading_guide_BMD_v_3.0_2021.pdf (accessed on 12 May 2022).
- Feary, D.J.; Hyatt, D.; Traub-Dargatz, J.; Roach, S.; Jones, R.L.; Wu, C.C.; Morley, P.S. Investigation of falsely reported resistance of Streptococcus equi subsp. zooepidemicus isolates from horses to trimethoprim-sulfamethoxazole. J. Vet. Diagn. Investig. 2005, 17, 483–486. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antimicrobial Substance | Medium | Mode (mg/L) |
|---|---|---|
| CIP | BB CAMHB | 0.5 0.5 |
| DOX | BB CAMHB | 0.0625 0.0625 |
| GEN | BB CAMHB | 0.25 0.125 |
| LEV | BB CAMHB | 0.5 0.5 |
| RIF | BB CAMHB | 1.0 1.0 |
| STR | BB CAMHB | 1.0 0.5 |
| SXT | BB CAMHB | 1.0 ≤0.016 |
| Cation-Adjusted Mueller–Hinton II Broth (CAMHB) | Brucella Broth (BB) | ||
|---|---|---|---|
| Pro | Con | Pro | Con |
| Growth after 96 h equal to BB | Method is currently not valid for B. melitensis | Tradition (established method) | High nutrient contents in BB lead to “false high” MIC values for trimethoprim–sulfamethoxazole |
| MIC values for trimethoprim–sulfamethoxazole are four log2 steps lower | Reading of plates is more difficult | Reading of plates easier → fewer and less discrepancies in interlaboratory validation trial | MIC values for rifampicin cluster around the applied breakpoint (S ≤ 1 mg/L) |
| Culture medium recommended by EUCAST | |||
| Already used in the laboratory for other bacteria | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tscherne, A.; Mantel, E.; Boskani, T.; Budniak, S.; Elschner, M.; Fasanella, A.; Feruglio, S.L.; Galante, D.; Giske, C.G.; Grunow, R.; et al. Adaptation of Brucella melitensis Antimicrobial Susceptibility Testing to the ISO 20776 Standard and Validation of the Method. Microorganisms 2022, 10, 1470. https://doi.org/10.3390/microorganisms10071470
Tscherne A, Mantel E, Boskani T, Budniak S, Elschner M, Fasanella A, Feruglio SL, Galante D, Giske CG, Grunow R, et al. Adaptation of Brucella melitensis Antimicrobial Susceptibility Testing to the ISO 20776 Standard and Validation of the Method. Microorganisms. 2022; 10(7):1470. https://doi.org/10.3390/microorganisms10071470
Chicago/Turabian StyleTscherne, Alina, Enrico Mantel, Talar Boskani, Sylwia Budniak, Mandy Elschner, Antonio Fasanella, Siri L. Feruglio, Domenico Galante, Christian G. Giske, Roland Grunow, and et al. 2022. "Adaptation of Brucella melitensis Antimicrobial Susceptibility Testing to the ISO 20776 Standard and Validation of the Method" Microorganisms 10, no. 7: 1470. https://doi.org/10.3390/microorganisms10071470