Detection of β-Lactamase-Producing Enterococcus faecalis and Vancomycin-Resistant Enterococcus faecium Isolates in Human Invasive Infections in the Public Hospital of Tandil, Argentina

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Epidemiological Background of the Strains Isolated from Human Invasive Infections in Hospital Ramón Santamarina (HRS).
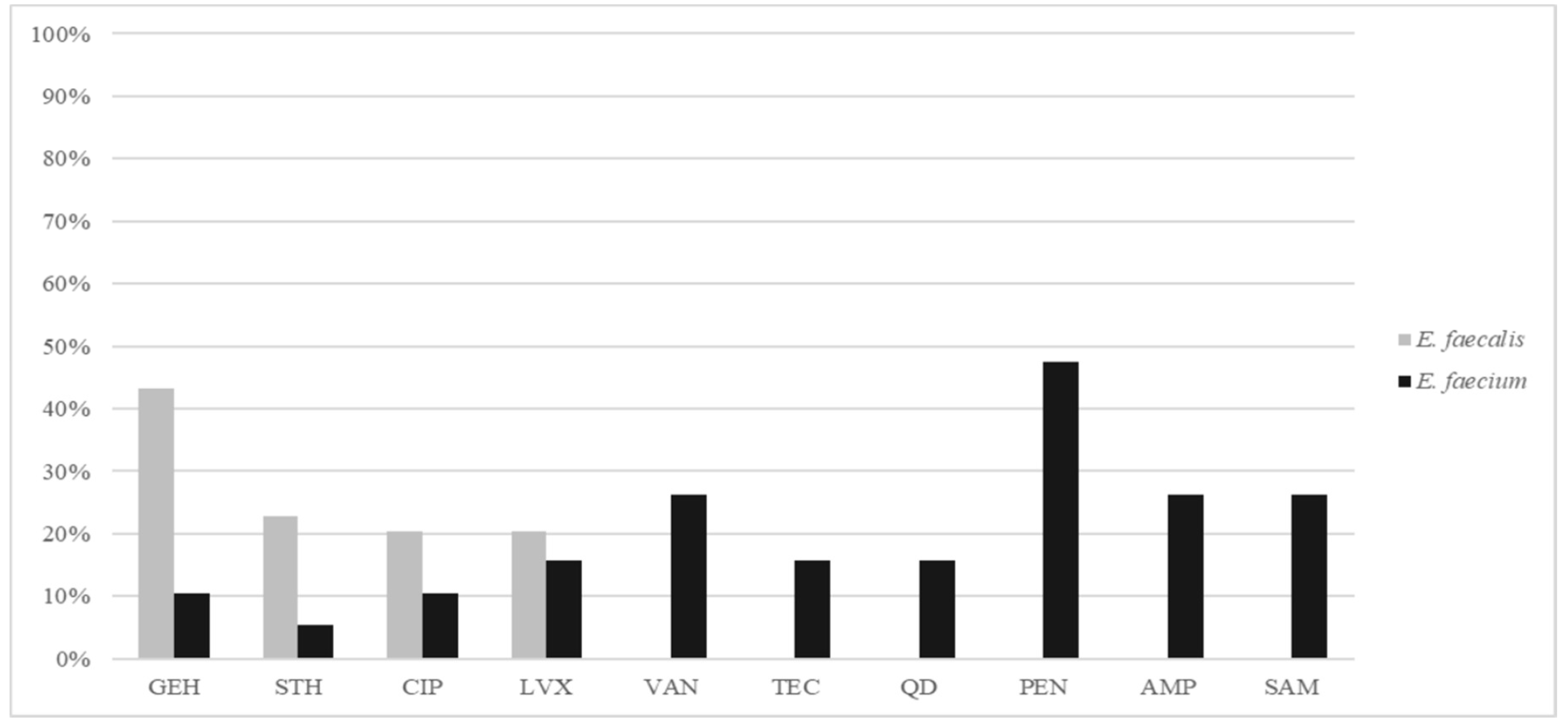
2.2. E. faecalis
2.3. E. faecium
3. Discussion
4. Materials and Methods
4.1. Epidemiological Data and Sampling of Enterococcus spp.
4.2. Ethical Approval
4.3. Antimicrobial Susceptibility
4.4. β-lactamase Production
4.5. Detection of van Genes
4.6. Clonal Relatedness
4.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Arias, C.A.; Murray, B.E. The rise of the Enterococcus: Beyond vancomycin resistance. Nat. Rev. Microbiol. 2012, 10, 266–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guzman Prieto, A.M.; van Schaik, W.; Rogers, M.R.C.; Coque, T.M.; Baquero, F.; Corander, J.; Willems, R.J.L. Global Emergence and Dissemination of Enterococci as Nosocomial Pathogens: Attack of the Clones? Front. Microbiol. 2016, 7, 788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werner, G.; Coque, T.M.; Hammerum, A.M.; Hope, R.; Hryniewicz, W.; Johnson, A.; Klare, I.; Kristinsson, K.G.; Leclercq, R.; Lester, C.H.; et al. Emergence and spread of vancomycin resistance among enterococci in Europe. Euro Surveill. 2008, 13, 19046. [Google Scholar]
- Togneri, A.; Corso, A.; González, J.; Lopardo, H.; Podestá, L.; Gagetti, P.; Peréz, M.; Rodríguez, V.; Rodríguez, M.; Ríos, L.; et al. Análisis clínico-epidemiológico de la portación intestinal de enterococos resistentes a vancomicina en una unidad de terapia intensiva. Rev. Argent. Microbiol. 2005, 37, 26–33. [Google Scholar]
- Lopardo, H.; Blanco, A.; Carbonaro, M.; Ruvinsky, S.; Andión, E.; Venuta, E.; Corso, A.; Gagetti, P.; Bologna, R. Impacto de 10 años de vigilancia de colonización con enterococos resistentes a vancomicina (ERV) en un hospital pediátrico de alta complejidad. Med. Infant. 2008, 1, 114–120. [Google Scholar]
- Murray, B.E.; Mederski-Samaroj, B. Transferable beta-lactamase. A new mechanism for in vitro penicillin resistance in Streptococcus faecalis. J. Clin. Investig. 1983, 72, 1168–1171. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Cormican, M.; Flamm, R.K.; Mendes, R.E.; Jones, R.N. Temporal and Geographic Variation in Antimicrobial Susceptibility and Resistance Patterns of Enterococci: Results from the SENTRY Antimicrobial Surveillance Program, 1997–2016. Open Forum Infect. Dis. 2019, 6, S54–S62. [Google Scholar] [CrossRef]
- Rice, L.B.; Carias, L.L.; Rudin, S.; Hutton, R.; Marshall, S.; Hassan, M.; Josseaume, N.; Dubost, L.; Marie, A.; Arthur, M. Role of class A penicillin-binding proteins in the expression of beta-lactam resistance in Enterococcus faecium. J. Bacteriol. 2009, 191, 3649–3656. [Google Scholar] [CrossRef] [Green Version]
- Novais, C.; Tedim, A.P.; Lanza, V.F.; Freitas, A.R.; Silveira, E.; Escada, R.; Roberts, A.P.; Al-Haroni, M.; Baquero, F.; Peixe, L.; et al. Co-diversification of Enterococcus faecium Core Genomes and PBP5: Evidences of pbp5 Horizontal Transfer. Front. Microbiol. 2016, 7, 1581. [Google Scholar] [CrossRef]
- Sarti, M.; Campanile, F.; Sabia, C.; Santagati, M.; Gargiulo, R.; Stefani, S. Polyclonal diffusion of beta-lactamase-producing Enterococcus faecium. J. Clin. Microbiol. 2012, 50, 169–172. [Google Scholar] [CrossRef] [Green Version]
- Murray, B.E. Beta-lactamase-producing enterococci. Antimicrob. Agents Chemother. 1992, 36, 2355–2359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodel-Christian, S.L.; Murray, B.E. Comparison of the gentamicin resistance transposon Tn5281 with regions encoding gentamicin resistance in Enterococcus faecalis isolates from diverse geographic locations. Antimicrob. Agents Chemother. 1992, 36, 2259–2264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conceição, N.; da Silva, L.E.P.; Darini, A.L.d.C.; Pitondo-Silva, A.; de Oliveira, A.G. Penicillin-resistant, ampicillin-susceptible Enterococcus faecalis of hospital origin: pbp4 gene polymorphism and genetic diversity. Infect. Genet. Evol. 2014, 28, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Marín, M.E.; Mera, J.R.; Arduino, R.C.; Correa, A.P.; Coque, T.M.; Stamboulian, D.; Murray, B.E. First report of vancomycin-resistant Enterococcus faecium isolated in Argentina. Clin. Infect. Dis. 1998, 26, 235–236. [Google Scholar] [CrossRef] [Green Version]
- Corso, A.C.; Gagetti, P.S.; Rodríguez, M.M.; Melano, R.G.; Ceriana, P.G.; Faccone, D.F.; Galas, M.F. Molecular epidemiology of vancomycin-resistant Enterococcus faecium in Argentina. Int. J. Infect. Dis. 2007, 11, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Faccone, D.; Abel, F.; Lopez Ruitti, P.; Gagetti, P.; Corso, A. Diseminación de Enterococcus faecium con resistencia a glicopeptidos (VREFM) del complejo clonal 17 en Argentina. In Proceedings of the XII Congreso Argentino de Microbiología, VI Congreso de la Sociedad Argentina de Bacteriología, Micología y Parasitología Clínica—SADEBAC, I Congreso de Microbiología Agrícola y Ambiental, Buenos Aires, Argentina, 17–20 Octubre 2010. [Google Scholar]
- Corso, A.; Faccone, D.; Gagetti, P.; Togneri, A.; Lopardo, H.; Melano, R.; Rodríguez, V.; Rodriguez, M.; Galas, M. First report of VanA Enterococcus gallinarum dissemination within an intensive care unit in Argentina. Int. J. Antimicrob. Agents 2005, 25, 51–56. [Google Scholar] [CrossRef]
- Tedim, A.P.; Ruiz-Garbajosa, P.; Corander, J.; Rodríguez, C.M.; Cantón, R.; Willems, R.J.; Baquero, F.; Coque, T.M. Population biology of intestinal Enterococcus isolates from hospitalized and nonhospitalized individuals in different age groups. Appl. Environ. Microbiol. 2015, 81, 1820–1831. [Google Scholar] [CrossRef] [Green Version]
- Tedim, A.P.; Ruíz-Garbajosa, P.; Rodríguez, M.C.; Rodríguez-Baños, M.; Lanza, V.F.; Derdoy, L.; Cárdenas Zurita, G.; Loza, E.; Cantón, R.; Baquero, F.; et al. Long-term clonal dynamics of Enterococcus faecium strains causing bloodstream infections (1995–2015) in Spain. J. Antimicrob. Chemother. 2017, 72, 48–55. [Google Scholar] [CrossRef]
- Baquero, F.; Coque, T.M. Multilevel population genetics in antibiotic resistance. FEMS Microbiol. Rev. 2011, 35, 705–706. [Google Scholar] [CrossRef] [Green Version]
- Instituto Nacional de Enfermedades Infecciosas. Protocolo De Trabajo Red WHONET Argentina; SERVICIO ANTIMICROBIANOS, Dpto. Bacteriología, Instituto Nacional de Enfermedades Infecciosas (INEI): Buenos Aires, Argentina, 2018. [Google Scholar]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Nallapareddy, S.R.; Duh, R.-W.; Singh, K.V.; Murray, B.E. Molecular typing of selected Enterococcus faecalis isolates: Pilot study using multilocus sequence typing and pulsed-field gel electrophoresis. J. Clin. Microbiol. 2002, 40, 868–876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayakawa, K.; Marchaim, D.; Vidaillac, C.; Lephart, P.; Pogue, J.M.; Sunkara, B.; Kotra, H.; Hasan, A.; Shango, M.; Yerramalla, Y.; et al. Growing prevalence of vancomycin-resistant Enterococcus faecalis in the region with the highest prevalence of vancomycin-resistant Staphylococcus aureus. Infect. Control Hosp. Epidemiol. 2011, 32, 922–924. [Google Scholar] [CrossRef] [PubMed]
- Gawryszewska, I.; Żabicka, D.; Bojarska, K.; Malinowska, K.; Hryniewicz, W.; Sadowy, E. Invasive enterococcal infections in Poland: The current epidemiological situation. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 847–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagetti, P.; Bonofiglio, L.; García Gabarrot, G.; Kaufman, S.; Mollerach, M.; Vigliarolo, L.; von Specht, M.; Toresani, I.; Lopardo, H.A. Resistance to β-lactams in enterococci. Rev. Argent. Microbiol. 2019, 51, 179–183. [Google Scholar] [CrossRef]
- Freitas, A.R.; Tedim, A.P.; Francia, M.V.; Jensen, L.B.; Novais, C.; Peixe, L.; Sánchez-Valenzuela, A.; Sundsfjord, A.; Hegstad, K.; Werner, G.; et al. Multilevel population genetic analysis of vanA and vanB Enterococcus faecium causing nosocomial outbreaks in 27 countries (1986–2012). J. Antimicrob. Chemother. 2016, 71, 3351–3366. [Google Scholar] [CrossRef] [Green Version]
- Pourcel, G.; Sparo, M.; Corso, A.; Delpech, G.; Gagetti, P.; de Luca, M.M.; Bernstein, J.; Schell, C.; Lissarrague, S.; Basualdo, J.A. Molecular Genetic Profiling of Clinical and Foodborne Strains of Enterococci with High Level Resistance to Gentamicin and Vancomycin. Clin. Microbiol. Open Access 2017, 6, 1000272. [Google Scholar] [CrossRef] [Green Version]
- Osuka, H.; Nakajima, J.; Oishi, T.; Funayama, Y.; Ebihara, T.; Ishikawa, H.; Saito, K.; Koganemaru, H.; Hitomi, S. High-level aminoglycoside resistance in Enterococcus faecalis and Enterococcus faecium causing invasive infection: Twelve-year surveillance in the Minami Ibaraki Area. J. Infect. Chemother. 2016, 22, 61–63. [Google Scholar] [CrossRef]
- Rice, L.B.; Hutton-Thomas, R.; Lakticova, V.; Helfand, M.S.; Donskey, C.J. Beta-lactam antibiotics and gastrointestinal colonization with vancomycin-resistant enterococci. J. Infect. Dis. 2004, 189, 1113–1118. [Google Scholar] [CrossRef] [Green Version]
- Facklam, R.R.; Collins, M.D. Identification of Enterococcus species isolated from human infections by a conventional test scheme. J. Clin. Microbiol. 1989, 27, 731–734. [Google Scholar] [CrossRef] [Green Version]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Twenty-Seventh Informational Supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2017; ISBN 1-56238-804-5. [Google Scholar]
- McBride, S.M.; Fischetti, V.A.; Leblanc, D.J.; Moellering, R.C.; Gilmore, M.S. Genetic diversity among Enterococcus faecalis. PLoS ONE 2007, 2, e582. [Google Scholar] [CrossRef]
- Aarestrup, F.M.; Agerso, Y.; Gerner-Smidt, P.; Madsen, M.; Jensen, L.B. Comparison of antimicrobial resistance phenotypes and resistance genes in Enterococcus faecalis and Enterococcus faecium from humans in the community, broilers, and pigs in Denmark. Diagn. Microbiol. Infect. Dis. 2000, 37, 127–137. [Google Scholar] [CrossRef]
- Depardieu, F.; Perichon, B.; Courvalin, P. Detection of the van alphabet and identification of enterococci and staphylococci at the species level by multiplex PCR. J. Clin. Microbiol. 2004, 42, 5857–5860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coque, T.M.; Willems, R.J.L.; Fortún, J.; Top, J.; Diz, S.; Loza, E.; Cantón, R.; Baquero, F. Population structure of Enterococcus faecium causing bacteremia in a Spanish university hospital: Setting the scene for a future increase in vancomycin resistance? Antimicrob. Agents Chemother. 2005, 49, 2693–2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tenover, F.C.; Arbeit, R.D.; Goering, R.V.; Mickelsen, P.A.; Murray, B.E.; Persing, D.H.; Swaminathan, B. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: Criteria for bacterial strain typing. J. Clin. Microbiol. 1995, 33, 2233–2239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Homan, W.L.; Tribe, D.; Poznanski, S.; Li, M.; Hogg, G.; Spalburg, E.; Van Embden, J.D.A.; Willems, R.J.L. Multilocus sequence typing scheme for Enterococcus faecium. J. Clin. Microbiol. 2002, 40, 1963–1971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz-Garbajosa, P.; Bonten, M.J.M.; Robinson, D.A.; Top, J.; Nallapareddy, S.R.; Torres, C.; Coque, T.M.; Cantón, R.; Baquero, F.; Murray, B.E.; et al. Multilocus sequence typing scheme for Enterococcus faecalis reveals hospital-adapted genetic complexes in a background of high rates of recombination. J. Clin. Microbiol. 2006, 44, 2220–2228. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Strain | Clinical Sample | Year | Antibiotic Susceptibility | PFGE-Type/ β-lactamase+ | ST | HRS Ward |
|---|---|---|---|---|---|---|
| C43-IR | Renal abscess | 2014 | GEH, PEN | EFC-2/bla+ | 9 | Surgery |
| C46-IR | Abdominal fluid | 2014 | GEH, PEN | EFC-2/bla+ | 9 | Surgery |
| C47-IRE1 | Abdominal fluid | 2014 | GEH, PEN | EFC-2/bla+ | 9 | Surgery |
| C50-IR | Blood | 2014 | GEH, PEN | EFC-2/bla+ | 9 | IM |
| C51-IRE1 | Peritoneal fluid | 2014 | GEH, PEN | EFC-2/bla+ | 9 | Surgery |
| C11-IR | Abdominal fluid | 2010 | GEH, STH, CIP, LVX | EFC-3 | 720 | Unknown |
| C13-IR | Blood | 2013 | STH, CIP, LVX | EFC-3 | 720 | Unknown |
| C22-IR | Blood | 2013 | GEN, STH, CIP, LVX | EFC-3 | 720 | Unknown |
| C33-IR | Abscess | 2013 | GEH, STH, CIP, LVX | EFC-3 | 720 | ER |
| C54-IR | Blood | 2014 | GEH | EFC-4 | 388 | Traumatology |
| C55-IR | Blood | 2014 | GEH | EFC-4 | 388 | ICU |
| C12-IRE1 | Blood | 2013 | - | EFC-5 | 604 | Unknown |
| C12-IRE1.1 | Blood | 2013 | - | EFC-5 | 604 | Unknown |
| C15-IR | Synovial fluid | 2013 | - | EFC-5 | 604 | Unknown |
| C5-IR | Liver abscess | 2010 | GEH | EFC-6 | ND | Unknown |
| C6-IR | Blood | 2013 | GEH, CIP, LVX | EFC-7 | 179 | Unknown |
| C7-IRE1 | Peritoneal fluid | 2010 | GEH | EFC-7 | 179 | Guard |
| C19-IR | Blood | 2013 | GEH | EFC-7 | 179 | Unknown |
| C28-IR | Blood | 2013 | GEH | EFC-7 | 179 | Unknown |
| C9-IR | Endometrial biopsy | 2013 | - | EFC-8 | ND | Unknown |
| C1-IR | Peritoneal fluid | 2010 | - | EFC-9 | ND | Unknown |
| C2-IR | Blood | 2013 | - | EFC-10 | ND | Unknown |
| C4-IR | Abdominal fluid | 2010 | GEH | EFC-11 | ND | Unknown |
| C37-IR | Blood | 2014 | - | EFC-12 | 236 | Traumatology |
| C49-IR | Blood | 2014 | - | E12 | 236 | ICU |
| C41-IR | Synovial fluid | 2014 | - | EFC-12.1 | 236 | Traumatology |
| C42-IR | Tissue abscess | 2014 | - | EFC-12.1 | 236 | ER |
| C8-IR | Subphrenic abscess | 2010 | - | EFC-13 | ND | Unknown |
| C10-IR | Blood | 2013 | - | EFC-14 | ND | Unknown |
| C14-IRE1 | Peritoneal fluid | 2010 | STH, CIP, LVX | EFC-15 | ND | IM |
| C29-IR | Liver abscess | 2010 | STH, CIP, LVX | EFC-16.1 | 281 | Unknown |
| C39-IR | Pericardial fluid | 2014 | - | EFC-16 | 281 | ICU |
| C44-IRE1 | Liver abscess | 2014 | - | EFC-16 | 281 | ICU |
| C52-IRE1 | Synovial fluid | 2014 | GEH, STH, CIP, LVX | EFC-16.1 | 281 | Traumatology |
| C23-IR | Peritoneal fluid | 2010 | - | EFC-17 | ND | Surgery |
| C24-IR | Tubo-ovarian abscess | 2013 | STH | EFC-18 | ND | Unknown |
| C27-IR | Synovial fluid | 2013 | GEH, STH, CIP, LVX, CHL | EFC-19 | ND | Traumatology |
| C25-IR | Blood | 2013 | - | EFC-20 | ND | Surgery |
| C26-IR | Blood | 2013 | - | EFC-21 | ND | Unknown |
| C20-IRE1 | Liver abscess | 2010 | - | EFC-22 | ND | Surgery |
| C21-IR | Synovial fluid | 2013 | GEH, STH | EFC-23 | ND | Traumatology |
| C17-IR | Synovial fluid | 2013 | - | EFC-24 | ND | Unknown |
| C18-IR | Abdominal fluid | 2010 | - | EFC-25 | ND | ER |
| C36-IR | Skin abscess | 2013 | - | EFC-26 | ND | Unknown |
| Strain | Clinical Sample | Year | Antibiotic Susceptibility | van Genotype | PFGE-Type | ST | BAPS | HRS Ward |
|---|---|---|---|---|---|---|---|---|
| C47-IRE2 | Abdominal fluid | 2014 | VAN, Q/D, PEN | vanB | EFM-1 | 25 | 2.3 | Surgery |
| C48-IR | Blood | 2014 | VAN, TEC, Q/D, PEN | vanA | EFM-1 | 25 | 2.3 | Surgery |
| C38-IR | Blood | 2014 | - | - | EFM-1 | 25 | 2.3 | Traumatology |
| C30-IR | Blood | 2013 | VAN | vanB | EFM-1 | 25 | 2.3 | ICU |
| C31-IR | Abdominal fluid | 2010 | LVX, PEN, AMP | - | EFM-2 | ND | ND | ER |
| C32-IR | Intravesicular fluid | 2010 | - | - | EFM-2.1 | ND | ND | Unknow |
| C34-IR | Sinovial fluid | 2013 | PEN | - | EFM-2 | ND | ND | Unknow |
| C45-IR | Blood | 2014 | PEN, SAM | - | EFM-3 | 18 | 3.3 | Traumatology |
| C52-IRE2 | Sinovial fluid | 2014 | PEN, AMP, SAM | - | EFM-3 | 18 | 3.3 | Traumatology |
| C16-IR | Blood | 2013 | PEN | - | EFM-4 | ND | ND | ICU |
| C20-IRE2 | Liver abscess | 2013 | - | - | EFM-4 | 52 | 7 | Surgery |
| C35-IR | Peritoneal fluid | 2010 | - | - | EFM-4 | 52 | 7 | ER |
| C3-IR | Blood | 2013 | - | - | EFM-5 | ND | ND | Unknow |
| C7-IRE2 | Peritoneal fluid | 2010 | GEH, Q/D | - | EFM-5 | ND | ND | ER |
| C14-IRE2 | Peritoneal fluid | 2010 | - | - | EFM-6 | ND | ND | IM |
| C53-IR | Abdominal abscess | 2014 | VAN, TEC, GEH, CIP, LVX, PEN, AMP, SAM | vanA | EFM-7 | 792 | 3.1 | ICU |
| C40-IR | Blood | 2014 | STH, PEN, AMP, SAM | - | EFM-8 | 19 | 7 | Traumatology |
| C44-IRE2 | Liver abscess | 2014 | VAN, TEC, LVX, CIP, PEN, AMP, SAM | vanA | EFM-9 | 792 | 3.1 | ICU |
| C51-IRE2 | Peritoneal fluid | 2014 | - | - | EFM-10 | ND | ND | Surgery |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schell, C.M.; Tedim, A.P.; Rodríguez-Baños, M.; Sparo, M.D.; Lissarrague, S.; Basualdo, J.A.; Coque, T.M. Detection of β-Lactamase-Producing Enterococcus faecalis and Vancomycin-Resistant Enterococcus faecium Isolates in Human Invasive Infections in the Public Hospital of Tandil, Argentina. Pathogens 2020, 9, 142. https://doi.org/10.3390/pathogens9020142
Schell CM, Tedim AP, Rodríguez-Baños M, Sparo MD, Lissarrague S, Basualdo JA, Coque TM. Detection of β-Lactamase-Producing Enterococcus faecalis and Vancomycin-Resistant Enterococcus faecium Isolates in Human Invasive Infections in the Public Hospital of Tandil, Argentina. Pathogens. 2020; 9(2):142. https://doi.org/10.3390/pathogens9020142
Chicago/Turabian StyleSchell, Celia M., Ana P. Tedim, Mercedes Rodríguez-Baños, Mónica D. Sparo, Sabina Lissarrague, Juan A. Basualdo, and Teresa M. Coque. 2020. "Detection of β-Lactamase-Producing Enterococcus faecalis and Vancomycin-Resistant Enterococcus faecium Isolates in Human Invasive Infections in the Public Hospital of Tandil, Argentina" Pathogens 9, no. 2: 142. https://doi.org/10.3390/pathogens9020142