Hand Hygiene Behaviors in a Representative Sample of Polish Adolescents in Regions Stratified by COVID-19 Morbidity and by Confounding Variables (PLACE-19 Study): Is There Any Association?



Abstract
:1. Introduction
2. Materials and Methods
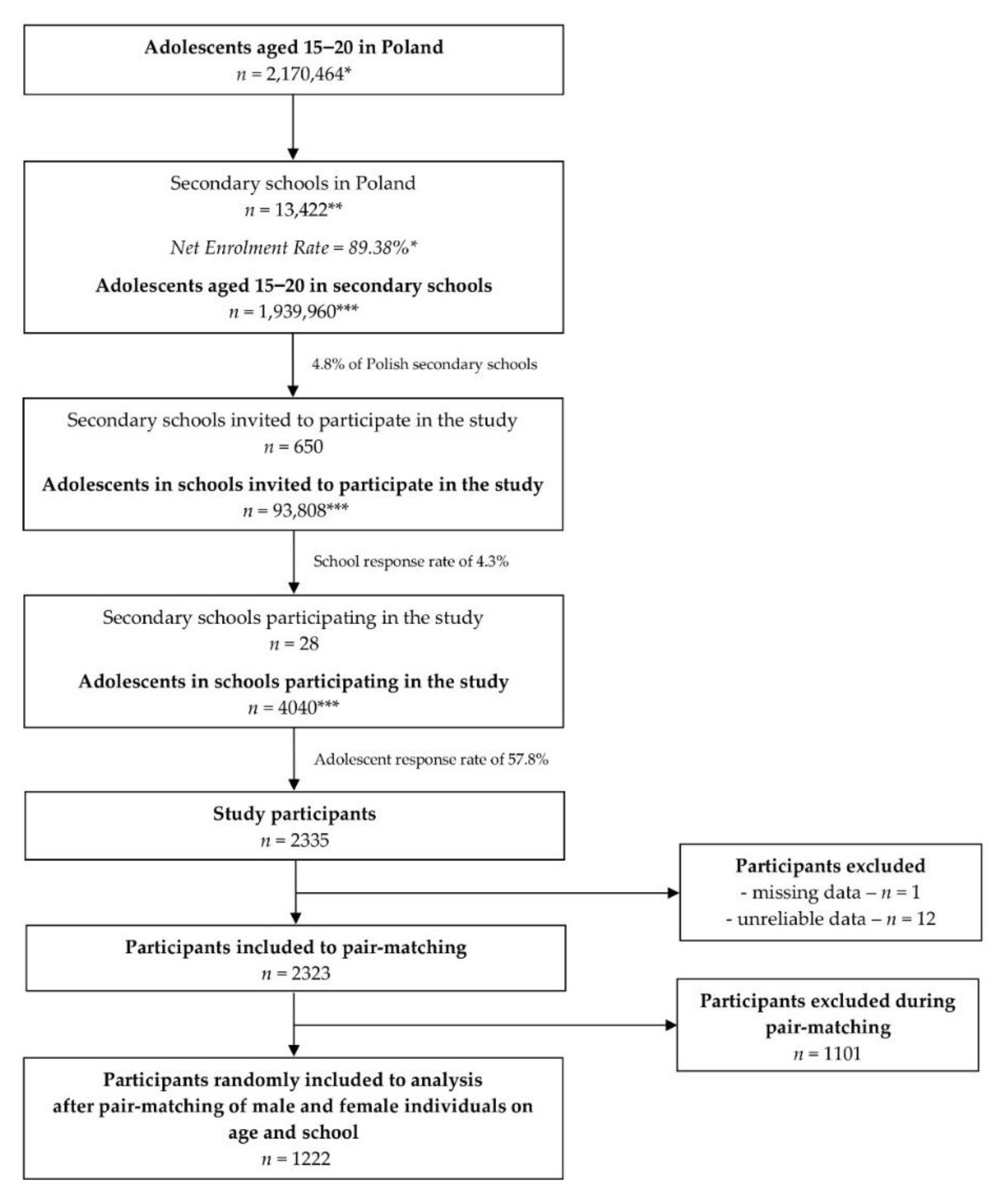
2.1. Study Population
- -
- first stage (conducted for all 16 voivodeships, which are basic administrative units in Poland and are further divided into counties, in the period of 31 March–14 April 2020)—random selection of five counties out of each of the voivodeship and five secondary schools out of each of the county, resulting in random selection of 400 secondary schools from Poland;
- -
- second stage (conducted for 10 voivodeships, in which after the first stage a total number of obtained answers was insufficient, in the period of 15 April–29 April 2020)—random selection of five counties out of each of the voivodeship and five secondary schools out of each of the county, resulting in random selection of 250 secondary schools from Poland.
2.2. Applied Questionnaire
2.3. Statistical Analysis
- -
- COVID-19 morbidity in the region, assessed based on the number of the COVID-19 cases in the voivodeships in Poland in April 2020 [41]—the voivodeships were divided into groups of low COVID-19 morbidity (10 voivodeships attributed to less than 30% of total number of COVID-19 cases in Poland) and high COVID-19 morbidity (six voivodeships attributed to more than 70% of total number of COVID-19 cases in Poland). The cumulative number of COVID-19 cases in each voivodeship classified as low COVID-19 morbidity was, in April 2020, lower than 150, 500, and 750 for the beginning, the middle, and end of the month, respectively [41];
- -
- status of the region, assessed based on the gross domestic product (GDP) in the voivodeship, while the data by the Eurostat were used [54]—the voivodeships were divided into groups of low GDP (13 voivodeships) and high GDP (3 voivodeships). The low GDP was interpreted as 24–73% in purchasing power standard and high GDP was interpreted as 73–624% in purchasing power standard [54];
- -
- environment (rural/urban), assessed based on the size of the town, as classified into groups of villages and small towns, medium cities, big cities—assessed based on the data of Polish Central Statistical Office [55]. The villages and small cities were defined as ones having < 20,000 inhabitants, medium cities—having 20,000–100,000 inhabitants, and big cities—having > 100,000 inhabitants [55].
3. Results
3.1. Analysis of Hand Hygiene Behaviors in a National Representative Sample of Polish Adolescents in Regions Stratified by COVID-19 Morbidity
3.2. Analysis of Hand Hygiene Behaviors in a National Representative Sample of Polish Adolescents in Regions Stratified by Gross Domestic Product (GDP)
3.3. Analysis of Hand Hygiene Behaviors in A National Representative Sample of Polish Adolescents in Regions Stratified by the Size of the Town
4. Discussion
4.1. Analysis of Hand Hygiene Behaviors in Regions Stratified by COVID-19 Morbidity
4.2. Analysis of Hand Hygiene Behaviors in Regions Stratified by Gross Domestic Product (GDP)
4.3. Analysis of Hand Hygiene Behaviors in Regions Stratified by the Size of the Town
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ali, I.; Alharbi, O.M. COVID-19: Disease, management, treatment, and social impact. Sci. Total Environ. 2020, 138861. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, S.M.; Yu, X.H.; Tang, S.L.; Tang, C.K. Coronavirus disease 2019 (COVID-19): Current status and future perspective. Int. J. Antimicrob. Agents 2020, 105951. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Statement on the second meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV). Available online: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 9 September 2020).
- World Health Organization (WHO). WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 9 September 2020).
- European Centre for Disease Prevention and Control. Transmission of COVID-19. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/transmission (accessed on 9 September 2020).
- Buonanno, G.; Morawska, L.; Stabile, L. Quantitative assessment of the risk of airborne transmission of SARS-CoV-2 infection: Prospective and retrospective applications. Environ. Int. 2020, 145, 106112. [Google Scholar] [CrossRef] [PubMed]
- Lotfi, M.; Hamblin, M.R.; Rezaei, N. COVID-19: Transmission, prevention, and potential therapeutic opportunities. Clin. Chim. Acta 2020, 508, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; on behalf of the COVID-19 Systematic Urgent Review Group Effort (SURGE) study authors. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Liang, M.; Gao, L.; Cheng, C.; Zhou, Q.; Uy, J.P.; Heiner, K.; Sun, C. Efficacy of face mask in preventing respiratory virus transmission: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 101751. [Google Scholar] [CrossRef]
- Morawska, L.; Tang, J.W.; Bahnfleth, W.; Bluyssen, P.M.; Boerstra, A.; Buonanno, G.; Cao, J.; Dancer, S.; Floto, A.; Franchimon, F.; et al. How can airborne transmission of COVID-19 indoors be minimised? Environ. Int. 2020, 142, 105832. [Google Scholar] [CrossRef]
- Buonanno, G.; Stabile, L.; Morawska, L. Estimation of airborne viral emission: Quanta emission rate of SARS-CoV-2 for infection risk assessment. Environ. Int. 2020, 141, 105794. [Google Scholar] [CrossRef]
- Morawska, L.; Milton, D.K. It Is Time to Address Airborne Transmission of Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2020, 6. [Google Scholar] [CrossRef]
- Alzyood, M.; Jackson, D.; Aveyard, H.; Brooke, J. COVID—19 reinforces the importance of hand washing. J. Clin. Nurs. 2020. [Google Scholar] [CrossRef]
- Cherrie, J.W.; Loh, M.; Aitken, R.J. Protecting healthcare workers from inhaled SARS-CoV-2 virus. Occup. Med. 2020, 70, 335–337. [Google Scholar] [CrossRef] [PubMed]
- Spinazzè, A.; Cattaneo, A.; Cavallo, D.M. COVID-19 outbreak in Italy: Protecting worker health and the response of the Italian Industrial Hygienists Association. Ann. Work Expo. Health 2020, 64, 559–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vishnevetsky, A.; Levy, M. Rethinking high-risk groups in COVID-19. Mult. Scler. Relat. Disord. 2020, 42. [Google Scholar] [CrossRef] [PubMed]
- Efuribe, C.; Barre-Hemingway, M.; Vaghefi, E.; Suleiman, A.B. Coping with the COVID-19 crisis: A call for youth engagement and the inclusion of young people in matters that affect their lives. J. Adolesc. Health 2020, 67, 16–17. [Google Scholar] [CrossRef]
- Mantovani, A.; Rinaldi, E.; Zusi, C.; Beatrice, G.; Saccomani, M.D.; Dalbeni, A. Coronavirus disease 2019 (COVID-19) in children and/or adolescents: A meta-analysis. Pediatr. Res. 2020, 17, 1–6. [Google Scholar] [CrossRef]
- Kar, S.K.; Verma, N.; Saxena, S.K. Coronavirus Infection Among Children and Adolescents. Coronavirus Dis. 2019 (COVID-19) 2020, 30, 71–79. [Google Scholar] [CrossRef]
- Park, Y.J.; Choe, Y.J.; Park, O.; Park, S.Y.; Kim, Y.M.; Kim, J.; Kweon, S.; Woo, Y.; Gwack, J.; Kim, S.S.; et al. Contact tracing during coronavirus disease outbreak, South Korea. Emerging Infect. Dis. 2020, 26, 2465–2468. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Save Lives: Clean Your Hands in the Context of COVID-19. Available online: https://www.who.int/infection-prevention/campaigns/clean-hands/WHO_HH-Community-Campaign_finalv3.pdf?ua=1 (accessed on 9 September 2020).
- Centers for Disease Control and Prevention (CDC). When and How to Wash Your Hands. Available online: https://www.cdc.gov/handwashing/when-how-handwashing.html (accessed on 9 September 2020).
- Chen, X.; Ran, L.; Liu, Q.; Hu, Q.; Du, X.; Tan, X. Hand Hygiene, Mask-Wearing Behaviors and Its Associated Factors during the COVID-19 Epidemic: A Cross-Sectional Study among Primary School Students in Wuhan, China. Int. J. Environ. Res. Public Health 2020, 17, 2893. [Google Scholar] [CrossRef]
- Ubheeram, J.; Biranjia-Hurdoyal, S.D. Effectiveness of hand hygiene education among a random sample of women from the community. J. Prev. Med. Hyg. 2017, 58, E53. [Google Scholar]
- Wong, J.S.W.; Lee, J.K.F. The common missed handwashing instances and areas after 15 years of hand-hygiene education. J. Environ. Public Health 2019, 8, 5928924. [Google Scholar] [CrossRef] [Green Version]
- Suen, L.K.; So, Z.Y.; Yeung, S.K.; Lo, K.Y.; Lam, S.C. Epidemiological investigation on hand hygiene knowledge and behaviour: A cross-sectional study on gender disparity. BMC Public Health 2019, 19, 401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, J.L.; Warren, C.A.; Perez, E.; Louis, R.I.; Phillips, S.; Wheeler, J.; Cole, M.; Misra, R. Gender and ethnic differences in hand hygiene practices among college students. Am. J. Infect. Control. 2008, 36, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Van de Mortel, T.; Bourke, R.; McLoughlin, J.; Nonu, M.; Reis, M. Gender influences handwashing rates in the critical care unit. Am. J. Infect. Control. 2001, 29, 395–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mariwah, S.; Hampshire, K.; Kasim, A. The impact of gender and physical environment on the handwashing behaviour of university students in Ghana. Trop. Med. Int. Health 2012, 17, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Dobe, M.; Mandal, R.N.; Jha, A. Social determinants of good hand-washing practice (GHP) among adolescents in a rural Indian community. Fam. Community Health 2013, 36, 172–177. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S. Oral and hand hygiene behaviour and risk factors among in-school adolescents in four Southeast Asian countries. Int. J. Environ. Res. Public Health 2014, 11, 2780–2792. [Google Scholar] [CrossRef] [Green Version]
- Qorbani, M.; Kelishadi, R.; Djalalinia, S.; Motlagh, M.E.; Kasaeian, A.; Ardalan, G.; Shafiee, G.; Safari, O.; Heshmat, R.; Mahdavi, S.B. Regional disparity in hygienic behaviors of Iranian children and adolescents: The CASPIAN-IV study. Med. J. Islam Repub. Iran. 2016, 30, 431. [Google Scholar]
- Taddese, A.A.; Dagnew, B.; Dagne, H.; Andualem, Z. Mother’s Handwashing Practices and Health Outcomes of Under-Five Children in Northwest Ethiopia. Pediatric Health Med. Ther. 2020, 11, 101. [Google Scholar] [CrossRef] [Green Version]
- To, K.G.; Lee, J.K.; Nam, Y.S.; Trinh, O.T.H.; Do, D.V. Hand washing behavior and associated factors in Vietnam based on the Multiple Indicator Cluster Survey, 2010–2011. Glob. Health Action 2016, 9, 29207. [Google Scholar] [CrossRef]
- Aiello, A.E.; Coulborn, R.M.; Perez, V.; Larson, E.L. Effect of hand hygiene on infectious disease risk in the community setting: A meta-analysis. Am. J. Public Health 2008, 98, 1372–1381. [Google Scholar] [CrossRef]
- Moore, L.D.; Robbins, G.; Quinn, J.; Arbogast, J.W. The Impact of COVID-19 Pandemic on Hand Hygiene Performance in Hospitals. Am. J. Infect. Control 2020. [Google Scholar] [CrossRef] [PubMed]
- Głąbska, D.; Skolmowska, D.; Guzek, D. Population-Based Study of the Influence of the COVID-19 Pandemic on Hand Hygiene Behaviors—Polish Adolescents’ COVID-19 Experience (PLACE-19) Study. Sustainability 2020, 12, 4930. [Google Scholar] [CrossRef]
- Guzek, D.; Skolmowska, D.; Głąbska, D. Analysis of Gender-Dependent Personal Protective Behaviors in a National Sample: Polish Adolescents’ COVID-19 Experience (PLACE-19) Study. Int. J. Environ. Res. Public Health 2020, 17, 5770. [Google Scholar] [CrossRef] [PubMed]
- Głąbska, D.; Skolmowska, D.; Guzek, D. Population-Based Study of the Changes in the Food Choice Determinants of Secondary School Students: Polish Adolescents’ COVID-19 Experience (PLACE-19) Study. Nutrients 2020, 12, 2640. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/?gclid=CjwKCAjwq_D7BRADEiwAVMDdHvneRLIPC03U3FJa-UNKxxjMd7TP28noIrDy_k9iqdH6_ns_ns6_ns_k9iqdH6_ns (accessed on 17 November 2020).
- Polish Ministry of Health. Available online: https://www.gov.pl/web/koronawirus/wykaz-zarazen-koronawirusem-sars-cov-2 (accessed on 15 May 2020).
- The Central Statistical Office in Poland. December 2019. Available online: https://bdl.stat.gov.pl/BDL/dane/podgrup/temat (accessed on 30 September 2020).
- Polish Ministry of National Education. Available online: https://www.gov.pl/web/edukacja/zawieszenie-zajec-w-szkolach (accessed on 28 September 2020).
- Mbroh, L.A. Assessing Knowledge, Attitude and Practices of Hand Hygiene among University Students. Master’s Thesis, Minnesota State University, Mankato, MN, USA, 24 June 2019. [Google Scholar]
- Sultana, M.; Mahumud, R.A.; Sarker, A.R.; Hossain, S.M. Hand hygiene knowledge and practice among university students: Evidence from Private Universities of Bangladesh. Risk Manag. Healthc. Policy 2016, 9, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Ergin, A.; Bostanci, M.; Onal, O.; Bozkurt, A.I.; Ergin, N. Evaluation of students’ social hand washing knowledge, practices, and skills in a university setting. Cent. Eur. J. Public Health 2011, 19, 222–226. [Google Scholar] [CrossRef] [Green Version]
- Tüzün, H.; Karakaya, K.; Deniz, E.B. Turkey Handwashing Survey: Suggestion for taking the ecological model into better consideration. Environ. Health Prev. Med. 2015, 20, 325–331. [Google Scholar] [CrossRef] [Green Version]
- Üner, S.; Sevencan, F.; Başaran, E.; Balcı, C.; Bilaloğlu, B. To determine some knowledge and attitudes related to the social hand washing of individuals who apply to a primary health center. TAF Prev. Med. Bull. 2009, 8, 207–216. [Google Scholar]
- World Health Organization (WHO). Hand Hygiene: Why, How & When? Available online: https://www.who.int/gpsc/5may/Hand_Hygiene_Why_How_and_When_Brochure.pdf (accessed on 28 September 2020).
- WHO Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge Clean Care Is Safer Care. World Health Organization: Geneva, Switzerland, 2009; II, CONSENSUS RECOMMENDATIONS. Available online: https://www.ncbi.nlm.nih.gov/books/NBK144035/ (accessed on 28 September 2020).
- Centers for Disease Control and Prevention (CDC). Handwashing: A Healthy Habit in the Kitchen. Available online: https://www.cdc.gov/handwashing/handwashing-kitchen.html (accessed on 28 September 2020).
- Centers for Disease Control and Prevention (CDC). Proper Hygiene When around Animals. Available online: https://www.cdc.gov/healthywater/hygiene/etiquette/around_animals.html (accessed on 28 September 2020).
- United Nations International Children’s Emergency Fund. Everything You Need to Know about Washing Your Hands to Protect against Coronavirus (COVID-19). Available online: https://www.unicef.org/coronavirus/everything-you-need-know-about-washing-your-hands-protect-against-coronavirus-covid-19 (accessed on 28 September 2020).
- Eurostat. GDP per Inhabitant in PPS (% of the EU-27 Average). Available online: https://ec.europa.eu/eurostat/web/regions/statistics-illustrated (accessed on 17 November 2020).
- The Central Statistical Office in Poland. Available online: https://stat.gov.pl/cps/rde/xbcr/gus/oz_miasta_w_liczbach_2009_notatka_infor.pdf (accessed on 17 November 2020).
- The Central Statistical Office in Poland. January 2019. Available online: https://stat.gov.pl/obszary-tematyczne/ludnosc/ludnosc/powierzchnia-i-ludnosc-w-przekroju-terytorialnym-w-2019-roku,7,16.html (accessed on 30 September 2020).
- Kadi, N.; Khelfaoui, M. Population density, a factor in the spread of COVID-19 in Algeria: Statistic study. Bull. Natl. Res. Cent. 2020, 44, 1–7. [Google Scholar] [CrossRef]
- Rocklöv, J.; Sjödin, H. High population densities catalyse the spread of COVID-19. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef]
- Apisarnthanarak, A.; Apisarnthanarak, P.; Siripraparat, C.; Saengaram, P.; Leeprechanon, N.; Weber, D.J. Impact of Anxiety and Fear for COVID-19 toward Infection Control Practices Among Thai Healthcare Workers. Infect. Control Hosp. Epidemiol. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Harper, C.A.; Satchell, L.P.; Fido, D.; Latzman, R.D. Functional fear predicts public health compliance in the COVID-19 pandemic. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef] [PubMed]
- Israel, S.; Harpaz, K.; Radvogin, E.; Schwartz, C.; Gross, I.; Mazeh, H.; Cohen, M.J.; Benenson, S. Dramatically improved hand hygiene performance rates at time of coronavirus pandemic. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, K.; Hirsch, M.S.; Bloom, A. Coronavirus Disease 2019 (COVID-19), UpToDate. 2020. Available online: https://www.uptodate.com/contents/coronavirus-disease-2019-covid-19-epidemiology-virology-and-prevention (accessed on 29 September 2020).
- Goumenou, M.; Sarigiannis, D.; Tsatsakis, A.; Anesti, O.; Docea, A.O.; Petrakis, D.; Tsoukalas, D.; Kostoff, R.; Rakitskii, V.; Spandidos, D.A.; et al. COVID-19 in Northern Italy: An integrative overview of factors possibly influencing the sharp increase of the outbreak. Mol. Med. Rep. 2020, 22, 20–32. [Google Scholar] [CrossRef]
- Eurostat. Population Structure and Ageing. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php/Population_structure_and_ageing#Median_age_is_highest_in_Italy (accessed on 29 September 2020).
- The Central Statistical Office in Poland. December 2019. Available online: https://stat.gov.pl/obszary-tematyczne/ludnosc/ludnosc/ludnosc-stan-i-struktura-ludnosci-oraz-ruch-naturalny-w-przekroju-terytorialnym-stan-w-dniu-31-12-2019,6,27.html (accessed on 30 September 2020).
- Suk, J.E.; Semenza, J.C. Future infectious disease threats to Europe. Am. J. Public Health 2011, 101, 2068–2079. [Google Scholar] [CrossRef]
- Rabbi, S.E.; Dey, N.C. Exploring the gap between hand washing knowledge and practices in Bangladesh: A cross-sectional comparative study. BMC Public Health 2013, 13, 89. [Google Scholar] [CrossRef] [Green Version]
- Luby, S.P.; Halder, A.K. Associations among handwashing indicators, wealth, and symptoms of childhood respiratory illness in urban Bangladesh. Trop. Med. Int. Health 2008, 13, 835–844. [Google Scholar] [CrossRef]
- You, H.; Wu, X.; Guo, X. Distribution of COVID-19 Morbidity Rate in Association with Social and Economic Factors in Wuhan, China: Implications for Urban Development. Int. J. Environ. Res. Public Health 2020, 17, 3417. [Google Scholar] [CrossRef]
- Takagi, H.; Kuno, T.; Yokoyama, Y.; Ueyama, H.; Matsushiro, T.; Hari, Y.; Ando, T. Meta-regression of COVID-19 prevalence/fatality on socioeconomic characteristics of data from top 50 US large cities. J. Med. Virol. 2020, 22. [Google Scholar] [CrossRef]
- Sarmadi, M.; Marufi, N.; Moghaddam, V.K. Association of COVID-19 global distribution and environmental and demographic factors: An updated three-month study. Environ. Res. 2020, 188, 109748. [Google Scholar] [CrossRef] [PubMed]
- Mane, A.B.; Reddy, N.S.; Reddy, P.; Chetana, K.V.; Srijith, S.N.; Sriniwas, T. Differences of Hand Hygiene and its Correlates among School going Children in Rural and Urban Area of Karnataka, India. Arch. Med. 2016, 8. [Google Scholar] [CrossRef]
- Khan, S.; Kumar, V.; Priya, N.; Yadav, S.S. Handwashing practices among the caregivers of under five children in rural and urban areas of Moradabad, India: A community based study. Int. J. Med. Sci. Public Health 2017, 6, 133–138. [Google Scholar] [CrossRef] [Green Version]
- Ranscombe, P. Rural areas at risk during COVID-19 pandemic. Lancet Infect. Dis. 2020, 20, 545. [Google Scholar] [CrossRef]
- Neiderud, C.J. How urbanization affects the epidemiology of emerging infectious diseases. Infect. Ecol. Epidemiol. 2015, 5, 27060. [Google Scholar] [CrossRef]


{kind=link}
| Voivodeship | 1st April | 8th April | 15th April | 22nd April | 29th April | |
|---|---|---|---|---|---|---|
| Voivodeships of low COVID-19 morbidity | Podlaskie | 44 | 149 | 259 | 333 | 367 |
| Lubusz | 47 | 66 | 79 | 84 | 87 | |
| Holy Cross | 55 | 127 | 170 | 242 | 266 | |
| Pomeranian | 56 | 143 | 179 | 227 | 422 | |
| Warmian-Masurian | 59 | 92 | 125 | 145 | 146 | |
| Opole | 73 | 116 | 219 | 316 | 386 | |
| Kuyavian-Pomeranian | 76 | 277 | 359 | 452 | 537 | |
| West Pomeranian | 76 | 165 | 217 | 284 | 380 | |
| Subcarpathian | 100 | 182 | 243 | 271 | 328 | |
| Lublin | 132 | 199 | 270 | 332 | 359 | |
| Voivodeships of high COVID-19 morbidity | Greater Poland | 158 | 394 | 785 | 1097 | 1399 |
| Lesser Poland | 209 | 398 | 561 | 726 | 863 | |
| Łódź | 221 | 400 | 572 | 750 | 904 | |
| Silesian | 272 | 644 | 988 | 1580 | 2080 | |
| Lower Silesian | 298 | 539 | 561 | 1136 | 1500 | |
| Masovian | 544 | 1314 | 1792 | 2059 | 2391 | |
| Total for Poland | 2420 | 5205 | 7582 | 10,034 | 12,415 | |
| Characteristics | Low COVID-19 Morbidity in Region | High COVID-19 Morbidity in Region | p | |
|---|---|---|---|---|
| Before meals | Always | 445 (72.2%) | 394 (65.0%) | 0.0196 |
| Sometimes | 156 (25.3%) | 189 (31.2%) | ||
| Never | 15 (2.4%) | 23 (3.8%) | ||
| After meals | Always | 185 (30.0%) | 164 (27.1%) | 0.0041 |
| Sometimes | 358 (58.1%) | 329 (54.3%) | ||
| Never | 73 (11.9%) | 113 (18.6%) | ||
| Before preparing meals | Always | 519 (84.3%) | 495 (81.7%) | 0.7453 |
| Sometimes | 48 (7.8%) | 51 (8.4%) | ||
| Never | 6 (1.0%) | 4 (0.7%) | ||
| Not applicable * | 43 (7.0%) | 56 (9.2%) | ||
| After preparing meals | Always | 432 (70.1%) | 374 (61.7%) | 0.0297 |
| Sometimes | 126 (20.5%) | 155 (25.6%) | ||
| Never | 17 (2.8%) | 21 (3.5%) | ||
| Not applicable * | 41 (6.7%) | 56 (9.2%) | ||
| Before using the restroom | Always | 107 (17.4%) | 68 (11.2%) | 0.0068 |
| Sometimes | 219 (35.6%) | 244 (40.3%) | ||
| Never | 290 (47.1%) | 294 (48.5%) | ||
| After using the restroom | Always | 593 (96.3%) | 571 (94.2%) | 0.0014 |
| Sometimes | 15 (2.4%) | 34 (5.6%) | ||
| Never | 8 (1.3%) | 1 (0.2%) | ||
| Before going to bed | Always | 265 (43.0%) | 256 (42.2%) | 0.7722 |
| Sometimes | 208 (33.8%) | 216 (35.6%) | ||
| Never | 143 (23.2%) | 134 (22.1%) | ||
| After waking up in the morning | Always | 272 (44.2%) | 265 (43.7%) | 0.2235 |
| Sometimes | 212 (34.4%) | 188 (31.0%) | ||
| Never | 132 (21.4%) | 153 (25.2%) | ||
| After combing their hair | Always | 158 (25.6%) | 115 (19.0%) | 0.0298 |
| Sometimes | 196 (31.8%) | 203 (33.5%) | ||
| Never | 205 (33.3%) | 220 (36.3%) | ||
| Not applicable * | 57 (9.3%) | 68 (11.2%) | ||
| Characteristics | Low COVID-19 Morbidity in Region | High COVID-19 Morbidity in Region | p | |
|---|---|---|---|---|
| After coming back home | Always | 536 (87.0%) | 538 (88.8%) | 0.5363 |
| Sometimes | 75 (12.2%) | 62 (10.2%) | ||
| Never | 5 (0.8%) | 6 (1.0%) | ||
| After using public transportation | Always | 473 (76.8%) | 470 (77.6%) | 0.8816 |
| Sometimes | 107 (17.4%) | 99 (16.3%) | ||
| Never | 36 (5.8%) | 37 (6.1%) | ||
| After money exchange | Always | 334 (54.2%) | 312 (51.5%) | 0.5120 |
| Sometimes | 171 (27.8%) | 186 (30.7%) | ||
| Never | 111 (18.0%) | 108 (17.8%) | ||
| When hands are visibly soiled | Always | 528 (85.7%) | 487 (80.4%) | 0.1236 |
| Sometimes | 66 (10.7%) | 84 (13.9%) | ||
| Never | 22 (3.6%) | 35 (5.8%) | ||
| After handshaking | Always | 297 (48.2%) | 248 (40.9%) | 0.0373 |
| Sometimes | 228 (37.0%) | 255 (42.1%) | ||
| Never | 91 (14.8%) | 103 (17.0%) | ||
| After touching animals | Always | 317 (51.5%) | 253 (41.7%) | 0.0007 |
| Sometimes | 160 (26%) | 181 (29.9%) | ||
| Never | 27 (4.4%) | 49 (8.1%) | ||
| Not applicable * | 112 (18.2%) | 123 (20.3%) | ||
| After handling animal waste | Always | 432 (70.1%) | 416 (68.6%) | 0.8981 |
| Sometimes | 39 (6.3%) | 39 (6.4%) | ||
| Never | 17 (2.8%) | 14 (2.3%) | ||
| Not applicable * | 128 (20.8%) | 137 (22.6%) | ||
| After handling animal food | Always | 336 (54.5%) | 305 (50.3%) | 0.3763 |
| Sometimes | 119 (19.3%) | 129 (21.3%) | ||
| Never | 37 (6.0%) | 42 (6.9%) | ||
| Not applicable * | 124 (20.1%) | 130 (21.5%) | ||
| After contacting babies | Always | 113 (18.3%) | 72 (11.9%) | 0.0278 |
| Sometimes | 101 (16.4%) | 98 (16.2%) | ||
| Never | 38 (6.2%) | 46 (7.6%) | ||
| Not applicable * | 364 (59.1%) | 390 (64.4%) | ||
| After changing diapers | Always | 160 (26.0%) | 101 (16.7%) | 0.2487 |
| Sometimes | 21 (3.4%) | 15 (2.5%) | ||
| Never | 9 (1.5%) | 12 (2.0%) | ||
| Not applicable * | 426 (69.2%) | 478 (78.9%) | ||
| Characteristics | Low COVID-19 Morbidity in Region | High COVID-19 Morbidity in Region | p | |
|---|---|---|---|---|
| After blowing nose | Always | 250 (40.6%) | 204 (33.7%) | 0.0435 |
| Sometimes | 260 (42.2%) | 285 (47.0%) | ||
| Never | 106 (17.2%) | 117 (19.3%) | ||
| After sneezing | Always | 280 (45.5%) | 245 (40.4%) | 0.1080 |
| Sometimes | 253 (41.1%) | 258 (42.6%) | ||
| Never | 83 (13.5%) | 103 (17.0%) | ||
| After coughing | Always | 257 (41.7%) | 222 (36.6%) | 0.1831 |
| Sometimes | 253 (41.1%) | 267 (44.1%) | ||
| Never | 106 (17.2%) | 117 (19.3%) | ||
| Before touching sick people | Always | 271 (44.0%) | 255 (42.1%) | 0.1074 |
| Sometimes | 202 (32.8%) | 179 (29.5%) | ||
| Never | 143 (23.2%) | 172 (28.4%) | ||
| After touching sick people | Always | 528 (85.7%) | 487 (80.4%) | 0.0351 |
| Sometimes | 66 (10.7%) | 84 (13.9%) | ||
| Never | 22 (3.6%) | 35 (5.8%) | ||
| After touching garbage | Always | 474 (76.9%) | 447 (73.8%) | 0.8142 |
| Sometimes | 81 (13.1%) | 80 (13.2%) | ||
| Never | 17 (2.8%) | 13 (2.1%) | ||
| Not applicable * | 44 (7.1%) | 66 (10.9%) | ||
| After cleaning their home | Always | 430 (69.8%) | 387 (63.9%) | 0.0234 |
| Sometimes | 148 (24.0%) | 181 (29.9%) | ||
| Never | 27 (4.4%) | 17 (2.8%) | ||
| Not applicable * | 11 (1.8%) | 21 (3.5%) | ||
| After washing dishes | Always | 392 (63.6%) | 356 (58.7%) | 0.0741 |
| Sometimes | 91 (14.8%) | 112 (18.5%) | ||
| Never | 49 (8.0%) | 61 (10.1%) | ||
| Not applicable * | 84 (13.6%) | 77 (12.7%) | ||
| After doing laundry | Always | 182 (29.5%) | 160 (26.4%) | 0.1720 |
| Sometimes | 176 (28.6%) | 150 (24.8%) | ||
| Never | 100 (16.2%) | 116 (19.1%) | ||
| Not applicable * | 158 (25.6%) | 180 (29.7%) | ||
| Characteristics | Low COVID-19 Morbidity in Region | High COVID-19 Morbidity in Region | p | |
|---|---|---|---|---|
| Folding sleeves | Always | 332 (53.9%) | 289 (47.7%) | 0.0667 |
| Sometimes | 116 (18.8%) | 133 (21.9%) | ||
| Never | 21 (3.4%) | 30 (5.0%) | ||
| Not applicable * | 147 (23.9%) | 154 (25.4%) | ||
| Removing watch and bracelets | Always | 92 (14.9%) | 68 (11.2%) | 0.0052 |
| Sometimes | 123 (20.0%) | 93 (15.3%) | ||
| Never | 45 (7.3%) | 68 (11.2%) | ||
| Not applicable * | 356 (57.8%) | 377 (62.2%) | ||
| Removing rings before or during handwashing | Always | 68 (11.0%) | 54 (8.9%) | 0.0318 |
| Sometimes | 48 (7.8%) | 33 (5.4%) | ||
| Never | 40 (6.5%) | 57 (9.4%) | ||
| Not applicable * | 460 (74.7%) | 462 (76.2%) | ||
| Using soap | Always | 580 (94.2%) | 566 (93.4%) | 0.7258 |
| Sometimes | 33 (5.4%) | 38 (6.3%) | ||
| Never | 3 (0.5%) | 2 (0.3%) | ||
| Using warm water | Always | 381 (61.9%) | 383 (63.2%) | 0.6845 |
| Sometimes | 222 (36.0%) | 207 (34.2%) | ||
| Never | 13 (2.1%) | 16 (2.6%) | ||
| Soaking hands before using soap | Always | 441 (71.6%) | 438 (72.3%) | 0.3727 |
| Sometimes | 102 (16.6%) | 110 (18.2%) | ||
| Never | 72 (11.7%) | 57 (9.4%) | ||
| Not applicable * | 1 (0.2%) | 1 (0.2%) | ||
| Careful making soap lather on whole hands | Always | 376 (61.0%) | 360 (59.4%) | 0.8098 |
| Sometimes | 214 (34.7%) | 216 (35.6%) | ||
| Never | 26 (4.3%) | 29 (4.8%) | ||
| Not applicable * | 0 (0%) | 1 (0.2%) | ||
| Turning the faucet off with hand | Always | 314 (51.0%) | 302 (49.8%) | 0.7012 |
| Sometimes | 170 (27.6%) | 162 (26.7%) | ||
| Never | 132 (21.4%) | 142 (23.4%) | ||
| Drying hands with towel | Always | 523 (84.9%) | 466 (76.9%) | 0.0031 |
| Sometimes | 77 (12.5%) | 122 (20.1%) | ||
| Never | 16 (2.6%) | 18 (2.9%) | ||
| Characteristics | Low GDP in Region | High GDP in Region | p | |
|---|---|---|---|---|
| Before meals | Always | 650 (67.9%) | 189 (71.3%) | 0.1949 |
| Sometimes | 273 (28.5%) | 72 (27.2%) | ||
| Never | 34 (3.6%) | 4 (1.5%) | ||
| After meals | Always | 264 (27.6%) | 85 (32.1%) | 0.2452 |
| Sometimes | 541 (56.5%) | 146 (55.1%) | ||
| Never | 152 (15.9%) | 34 (12.8%) | ||
| Before preparing meals | Always | 802 (83.8%) | 212 (80.0%) | 0.1935 |
| Sometimes | 78 (8.2%) | 21 (7.9%) | ||
| Never | 8 (0.8%) | 2 (0.8%) | ||
| Not applicable * | 69 (7.2%) | 30 (11.3%) | ||
| After preparing meals | Always | 642 (67.1%) | 164 (61.9%) | 0.4502 |
| Sometimes | 216 (22.6%) | 65 (24.5%) | ||
| Never | 32 (3.3%) | 6 (2.3%) | ||
| Not applicable * | 67 (7.0%) | 30 (11.3%) | ||
| Before using the restroom | Always | 136 (14.2%) | 39 (14.7%) | 0.0355 |
| Sometimes | 346 (36.1%) | 117 (44.2%) | ||
| Never | 475 (48.7%) | 109 (41.1%) | ||
| After using the restroom | Always | 910 (95.1%) | 254 (95.8%) | 0.2834 |
| Sometimes | 38 (4.0%) | 11 (4.2%) | ||
| Never | 9 (0.9%) | 0 (0.0%) | ||
| Before going to bed | Always | 408 (42.6%) | 113 (42.6%) | 0.6373 |
| Sometimes | 327 (34.2%) | 97 (36.6%) | ||
| Never | 222 (23.2%) | 55 (20.8%) | ||
| After waking up in the morning | Always | 406 (42.4%) | 131 (49.4%) | 0.1249 |
| Sometimes | 321 (33.6%) | 79 (29.8%) | ||
| Never | 230 (24.0%) | 55 (20.8%) | ||
| After combing their hair | Always | 208 (21.8%) | 65 (24.5%) | 0.4800 |
| Sometimes | 311 (32.5%) | 88 (33.2%) | ||
| Never | 340 (35.5%) | 85 (32.1%) | ||
| Not applicable * | 98 (10.2%) | 27 (10.2%) | ||
| Characteristics | Low GDP in Region | High GDP in Region | p | |
|---|---|---|---|---|
| After coming back home | Always | 837 (87.5%) | 237 (89.5%) | 0.5361 |
| Sometimes | 112 (11.7%) | 25 (9.4%) | ||
| Never | 8 (0.8%) | 3 (1.1%) | ||
| After using public transportation | Always | 737 (77.0%) | 206 (77.7%) | 0.6774 |
| Sometimes | 165 (17.2%) | 41 (15.5%) | ||
| Never | 55 (5.8%) | 18 (6.8%) | ||
| After money exchange | Always | 521 (54.5%) | 125 (47.2%) | 0.1092 |
| Sometimes | 271 (28.3%) | 86 (32.4%) | ||
| Never | 165 (17.2%) | 54 (20.4%) | ||
| When hands are visibly soiled | Always | 931 (97.3%) | 249 (94.0%) | 0.0314 |
| Sometimes | 19 (2.0%) | 12 (4.5%) | ||
| Never | 7 (0.7%) | 4 (1.5%) | ||
| After handshaking | Always | 426 (44.5%) | 119 (44.9%) | 0.9656 |
| Sometimes | 380 (39.7%) | 103 (38.9%) | ||
| Never | 151 (15.8%) | 43 (16.2%) | ||
| After touching animals | Always | 452 (47.3%) | 118 (44.5%) | 0.1397 |
| Sometimes | 264 (27.6%) | 77 (29.1%) | ||
| Never | 52 (5.4%) | 24 (9.1%) | ||
| Not applicable * | 189 (19.7%) | 46 (17.3%) | ||
| After handling animal waste | Always | 660 (69.0%) | 188 (70.9%) | 0.9319 |
| Sometimes | 61 (6.4%) | 17 (6.4%) | ||
| Never | 25 (2.6%) | 6 (2.3%) | ||
| Not applicable * | 211 (22.0%) | 54 (20.4%) | ||
| After handling animal food | Always | 510 (53.3%) | 131 (49.4%) | 0.1299 |
| Sometimes | 181 (18.9%) | 67 (25.3%) | ||
| Never | 61 (6.4%) | 18 (6.8%) | ||
| Not applicable * | 205 (21.4%) | 49 (18.5%) | ||
| After contacting babies | Always | 155 (16.2%) | 30 (11.3%) | 0.2844 |
| Sometimes | 154 (16.1%) | 45 (17.0%) | ||
| Never | 68 (7.1%) | 16 (6.0%) | ||
| Not applicable * | 580 (60.6%) | 174 (65.7%) | ||
| After changing diapers | Always | 209 (21.8%) | 52 (19.6%) | 0.2475 |
| Sometimes | 32 (3.3%) | 4 (1.5%) | ||
| Never | 19 (2.0%) | 2 (0.8%) | ||
| Not applicable * | 697 (72.9%) | 207 (78.1%) | ||
| Characteristics | Low GDP in Region | High GDP in Region | p | |
|---|---|---|---|---|
| After blowing nose | Always | 346 (36.1%) | 108 (40.8%) | 0.3505 |
| Sometimes | 436 (45.6%) | 109 (41.1%) | ||
| Never | 175 (18.3%) | 48 (18.1%) | ||
| After sneezing | Always | 405 (42.3%) | 120 (45.3%) | 0.1555 |
| Sometimes | 413 (43.2%) | 98 (37.0%) | ||
| Never | 139 (14.5%) | 47 (17.7%) | ||
| After coughing | Always | 370 (38.7%) | 109 (41.1%) | 0.7012 |
| Sometimes | 413 (43.1%) | 107 (40.4%) | ||
| Never | 174 (18.2%) | 49 (18.5%) | ||
| Before touching sick people | Always | 416 (43.5%) | 110 (41.5%) | 0.6335 |
| Sometimes | 292 (30.5%) | 89 (33.6%) | ||
| Never | 249 (26.0%) | 66 (24.9%) | ||
| After touching sick people | Always | 811 (84.7%) | 204 (77.0%) | 0.0106 |
| Sometimes | 107 (11.2%) | 43 (16.2%) | ||
| Never | 39 (4.1%) | 18 (6.8%) | ||
| After touching garbage | Always | 719 (75.1%) | 202 (76.3%) | 0.8704 |
| Sometimes | 130 (13.6%) | 31 (11.7%) | ||
| Never | 23 (2.4%) | 7 (2.6%) | ||
| Not applicable * | 85 (8.9%) | 25 (9.4%) | ||
| After cleaning their home | Always | 656 (68.5%) | 161 (60.8%) | 0.0485 |
| Sometimes | 243 (25.4%) | 86 (32.4%) | ||
| Never | 36 (3.8%) | 8 (3.0%) | ||
| Not applicable * | 22 (2.3%) | 10 (3.8%) | ||
| After washing dishes | Always | 591 (61.8%) | 157 (59.2%) | 0.8068 |
| Sometimes | 157 (16.4%) | 46 (17.4%) | ||
| Never | 87 (9.1%) | 23 (8.7%) | ||
| Not applicable * | 122 (12.7%) | 39 (14.7%) | ||
| After doing laundry | Always | 267 (27.9%) | 75 (28.3%) | 0.8065 |
| Sometimes | 260 (27.2%) | 66 (24.9%) | ||
| Never | 173 (18.1%) | 43 (16.2%) | ||
| Not applicable * | 257 (26.8%) | 81 (30.6%) | ||
| Characteristics | Villages and Small Towns | Medium Cities | Big Cities | p | |
|---|---|---|---|---|---|
| Before meals | Always | 172 (78.9%) | 393 (68%) | 274 (64.3%) | 0.0027 |
| Sometimes | 44 (20.2%) | 167 (28.9%) | 134 (31.5%) | ||
| Never | 2 (0.9%) | 18 (3.1%) | 18 (4.2%) | ||
| After meals | Always | 78 (35.8%) | 169 (29.2%) | 102 (23.9%) | 0.0020 |
| Sometimes | 122 (56.0%) | 318 (55.0%) | 247 (58.0%) | ||
| Never | 18 (8.3%) | 91 (15.7%) | 77 (18.1%) | ||
| Before preparing meals | Always | 189 (86.7%) | 476 (82.4%) | 349 (81.9%) | 0.7148 |
| Sometimes | 14 (6.4%) | 46 (8%) | 39 (9.2%) | ||
| Never | 1 (0.5%) | 5 (0.9%) | 4 (0.9%) | ||
| Not applicable * | 14 (6.4%) | 51 (8.8%) | 34 (8.0%) | ||
| After preparing meals | Always | 160 (73.4%) | 366 (63.3%) | 280 (65.7%) | 0.0524 |
| Sometimes | 43 (19.7%) | 144 (24.9%) | 94 (22.1%) | ||
| Never | 2 (0.9%) | 18 (3.1%) | 18 (4.2%) | ||
| Not applicable * | 13 (6.0%) | 50 (8.7%) | 34 (8.0%) | ||
| Before using the restroom | Always | 55 (25.2%) | 74 (12.8%) | 46 (10.8%) | 0.0000 |
| Sometimes | 79 (36.2%) | 232 (40.1%) | 152 (35.7%) | ||
| Never | 84 (38.5%) | 272 (47.1%) | 228 (53.5%) | ||
| After using the restroom | Always | 210 (96.3%) | 542 (93.8%) | 412 (96.7%) | 0.2063 |
| Sometimes | 6 (2.8%) | 31 (5.4%) | 12 (2.8%) | ||
| Never | 2 (0.9%) | 5 (0.9%) | 2 (0.5%) | ||
| Before going to bed | Always | 101 (46.3%) | 234 (40.5%) | 186 (43.7%) | 0.1478 |
| Sometimes | 80 (36.7%) | 208 (36.0%) | 136 (31.9%) | ||
| Never | 37 (17.0%) | 136 (23.5%) | 104 (24.4%) | ||
| After waking up in the morning | Always | 111 (50.9%) | 245 (42.4%) | 181 (42.5%) | 0.0430 |
| Sometimes | 73 (33.5%) | 190 (32.9%) | 137 (32.2%) | ||
| Never | 34 (15.6%) | 143 (24.7%) | 108 (25.4%) | ||
| After combing their hair | Always | 79 (36.2%) | 127 (22%) | 67 (15.7%) | 0.0000 |
| Sometimes | 60 (27.5%) | 212 (36.7%) | 127 (29.8%) | ||
| Never | 61 (28%) | 183 (31.7%) | 181 (42.5%) | ||
| Not applicable * | 18 (8.3%) | 56 (9.7%) | 51 (12.0%) | ||
| Characteristics | Villages and Small Towns | Medium Cities | Big Cities | p | |
|---|---|---|---|---|---|
| After coming back home | Always | 191 (87.6%) | 506 (87.5%) | 377 (88.5%) | 0.5086 |
| Sometimes | 24 (11%) | 65 (11.2%) | 48 (11.3%) | ||
| Never | 3 (1.4%) | 7 (1.2%) | 1 (0.2%) | ||
| After using public transportation | Always | 167 (76.6%) | 443 (76.6%) | 333 (78.2%) | 0.6704 |
| Sometimes | 34 (15.6%) | 100 (17.3%) | 72 (16.9%) | ||
| Never | 17 (7.8%) | 35 (6.1%) | 21 (4.9%) | ||
| After money exchange | Always | 131 (60.1%) | 294 (50.9%) | 221 (51.9%) | 0.0839 |
| Sometimes | 47 (21.6%) | 178 (30.8%) | 132 (31.0%) | ||
| Never | 40 (18.3%) | 106 (18.3%) | 73 (17.1%) | ||
| When hands are visibly soiled | Always | 213 (97.7%) | 552 (95.5%) | 415 (97.4%) | 0.0536 |
| Sometimes | 4 (1.8%) | 22 (3.8%) | 5 (1.2%) | ||
| Never | 1 (0.5%) | 4 (0.7%) | 6 (1.4%) | ||
| After handshaking | Always | 121 (55.5%) | 237 (41.0%) | 187 (43.9%) | 0.0004 |
| Sometimes | 67 (30.7%) | 258 (44.6%) | 158 (37.1%) | ||
| Never | 30 (13.8%) | 83 (14.4%) | 81 (19.0%) | ||
| After touching animals | Always | 143 (65.6%) | 271 (46.9%) | 156 (36.6%) | 0.0000 |
| Sometimes | 39 (17.9%) | 167 (28.9%) | 135 (31.7%) | ||
| Never | 7 (3.2%) | 40 (6.9%) | 29 (6.8%) | ||
| Not applicable * | 29 (13.3%) | 100 (17.3%) | 106 (24.9%) | ||
| After handling animal waste | Always | 172 (78.9%) | 403 (69.7%) | 273 (64.1%) | 0.6382 |
| Sometimes | 12 (5.5%) | 42 (7.3%) | 24 (5.6%) | ||
| Never | 4 (1.8%) | 17 (2.9%) | 10 (2.3%) | ||
| Not applicable * | 30 (13.8%) | 116 (20.1%) | 119 (27.9%) | ||
| After handling animal food | Always | 144 (66.1%) | 296 (51.2%) | 201 (47.2%) | 0.0015 |
| Sometimes | 38 (17.4%) | 136 (23.5%) | 74 (17.4%) | ||
| Never | 7 (3.2%) | 36 (6.2%) | 36 (8.5%) | ||
| Not applicable * | 29 (13.3%) | 110 (19%) | 115 (27.0%) | ||
| After contacting babies | Always | 55 (25.2%) | 87 (15.1%) | 43 (10.1%) | 0.2107 |
| Sometimes | 40 (18.3%) | 103 (17.8%) | 56 (13.1%) | ||
| Never | 17 (7.8%) | 45 (7.8%) | 22 (5.2%) | ||
| Not applicable * | 106 (48.6%) | 343 (59.3%) | 305 (71.6%) | ||
| After changing diapers | Always | 79 (36.2%) | 116 (20.1%) | 66 (15.5%) | 0.1877 |
| Sometimes | 10 (4.6%) | 22 (3.8%) | 4 (0.9%) | ||
| Never | 4 (1.8%) | 10 (1.7%) | 7 (1.6%) | ||
| Not applicable * | 125 (57.3%) | 430 (74.4%) | 349 (81.9%) | ||
| Characteristics | Villages and Small Towns | Medium Cities | Big Cities | p | |
|---|---|---|---|---|---|
| After blowing nose | Always | 112 (51.4%) | 209 (36.2%) | 133 (31.2%) | 0.0000 |
| Sometimes | 77 (35.3%) | 264 (45.7%) | 204 (47.9%) | ||
| Never | 29 (13.3%) | 105 (18.2%) | 89 (20.9%) | ||
| After sneezing | Always | 122 (56.0%) | 246 (42.6%) | 157 (36.9%) | 0.0001 |
| Sometimes | 70 (32.1%) | 253 (43.8%) | 188 (44.1%) | ||
| Never | 26 (11.9%) | 79 (13.7%) | 81 (19.0%) | ||
| After coughing | Always | 110 (50.5%) | 230 (39.8%) | 139 (32.6%) | 0.0001 |
| Sometimes | 78 (35.8%) | 253 (43.8%) | 189 (44.4%) | ||
| Never | 30 (13.8%) | 95 (16.4%) | 98 (23.0%) | ||
| Before touching sick people | Always | 108 (49.5%) | 251 (43.4%) | 167 (39.2%) | 0.0260 |
| Sometimes | 71 (32.6%) | 171 (29.6%) | 139 (32.6%) | ||
| Never | 39 (17.9%) | 156 (27.0%) | 120 (28.2%) | ||
| After touching sick people | Always | 193 (88.5%) | 472 (81.7%) | 350 (82.2%) | 0.0876 |
| Sometimes | 15 (6.9%) | 76 (13.1%) | 59 (13.8%) | ||
| Never | 10 (4.6%) | 30 (5.2%) | 17 (4.0%) | ||
| After touching garbage | Always | 178 (81.7%) | 440 (76.1%) | 303 (71.1%) | 0.3727 |
| Sometimes | 25 (11.5%) | 70 (12.1%) | 66 (15.5%) | ||
| Never | 6 (2.8%) | 14 (2.4%) | 10 (2.3%) | ||
| Not applicable * | 9 (4.1%) | 54 (9.3%) | 47 (11.0%) | ||
| After cleaning their home | Always | 160 (73.4%) | 380 (65.7%) | 277 (65.0%) | 0.0582 |
| Sometimes | 42 (19.3%) | 166 (28.7%) | 121 (28.4%) | ||
| Never | 11 (5%) | 18 (3.1%) | 15 (3.5%) | ||
| Not applicable * | 5 (2.3%) | 14 (2.4%) | 13 (3.1%) | ||
| After washing dishes | Always | 142 (65.1%) | 344 (59.5%) | 262 (61.5%) | 0.1896 |
| Sometimes | 36 (16.5%) | 110 (19%) | 57 (13.4%) | ||
| Never | 16 (7.3%) | 58 (10%) | 36 (8.5%) | ||
| Not applicable * | 24 (11%) | 66 (11.4%) | 71 (16.7%) | ||
| After doing laundry | Always | 84 (38.5%) | 158 (27.3%) | 100 (23.5%) | 0.0531 |
| Sometimes | 59 (27.1%) | 168 (29.1%) | 99 (23.2%) | ||
| Never | 32 (14.7%) | 110 (19.0%) | 74 (17.4%) | ||
| 43 (19.7%) | 142 (24.6%) | 153 (35.9%) | |||
| Characteristics | Villages and Small Towns | Medium Cities | Big Cities | p | |
|---|---|---|---|---|---|
| Folding sleeves | Always | 130 (59.6%) | 307 (53.1%) | 184 (43.2%) | 0.0063 |
| Sometimes | 38 (17.4%) | 112 (19.4%) | 99 (23.2%) | ||
| Never | 4 (1.8%) | 25 (4.3%) | 22 (5.2%) | ||
| Not applicable * | 46 (21.1%) | 134 (23.2%) | 121 (28.4%) | ||
| Removing watch and bracelets | Always | 41 (18.8%) | 79 (13.7%) | 40 (9.4%) | 0.0218 |
| Sometimes | 48 (22%) | 94 (16.3%) | 74 (17.4%) | ||
| Never | 13 (6%) | 60 (10.4%) | 40 (9.4%) | ||
| Not applicable * | 116 (53.2%) | 345 (59.7%) | 272 (63.8%) | ||
| Removing rings before or during handwashing | Always | 23 (10.6%) | 60 (10.4%) | 39 (9.2%) | 0.0854 |
| Sometimes | 23 (10.6%) | 39 (6.7%) | 19 (4.5%) | ||
| Never | 12 (5.5%) | 56 (9.7%) | 29 (6.8%) | ||
| Not applicable * | 160 (73.4%) | 423 (73.2%) | 339 (79.6%) | ||
| Using soap | Always | 206 (94.5%) | 541 (93.6%) | 399 (93.7%) | 0.3960 |
| Sometimes | 10 (4.6%) | 34 (5.9%) | 27 (6.3%) | ||
| Never | 2 (0.9%) | 3 (0.5%) | 0 (0%) | ||
| Using warm water | Always | 140 (58.1%) | 371 (58.2%) | 253 (54.4%) | 0.4848 |
| Sometimes | 74 (30.7%) | 195 (30.6%) | 160 (34.4%) | ||
| Never | 4 (1.7%) | 12 (1.9%) | 13 (2.8%) | ||
| Soaking hands before using soap | Always | 153 (70.2%) | 408 (70.6%) | 318 (74.6%) | 0.1480 |
| Sometimes | 34 (15.6%) | 104 (18%) | 74 (17.4%) | ||
| Never | 31 (14.2%) | 64 (11.1%) | 34 (8.0%) | ||
| Not applicable * | 0 (0%) | 2 (0.3%) | 0 (0%) | ||
| Careful making soap lather on whole hands | Always | 138 (63.3%) | 334 (57.8%) | 264 (62%) | 0.3941 |
| Sometimes | 74 (33.9%) | 213 (36.9%) | 143 (33.6%) | ||
| Never | 6 (2.8%) | 30 (5.2%) | 19 (4.5%) | ||
| Not applicable * | 0 (0%) | 1 (0.2%) | 0 (0%) | ||
| Turning the faucet off with hand | Always | 114 (52.3%) | 301 (52.1%) | 201 (47.2%) | 0.1880 |
| Sometimes | 55 (25.2%) | 143 (24.7%) | 134 (31.4%) | ||
| Never | 49 (22.5%) | 134 (23.2%) | 91 (21.4%) | ||
| Drying hands with towel | Always | 180 (82.6%) | 477 (82.5%) | 332 (77.9%) | 0.2588 |
| Sometimes | 31 (14.2%) | 86 (14.9%) | 82 (19.2%) | ||
| Never | 7 (3.2%) | 15 (2.6%) | 12 (2.8%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skolmowska, D.; Głąbska, D.; Guzek, D. Hand Hygiene Behaviors in a Representative Sample of Polish Adolescents in Regions Stratified by COVID-19 Morbidity and by Confounding Variables (PLACE-19 Study): Is There Any Association? Pathogens 2020, 9, 1011. https://doi.org/10.3390/pathogens9121011
Skolmowska D, Głąbska D, Guzek D. Hand Hygiene Behaviors in a Representative Sample of Polish Adolescents in Regions Stratified by COVID-19 Morbidity and by Confounding Variables (PLACE-19 Study): Is There Any Association? Pathogens. 2020; 9(12):1011. https://doi.org/10.3390/pathogens9121011
Chicago/Turabian StyleSkolmowska, Dominika, Dominika Głąbska, and Dominika Guzek. 2020. "Hand Hygiene Behaviors in a Representative Sample of Polish Adolescents in Regions Stratified by COVID-19 Morbidity and by Confounding Variables (PLACE-19 Study): Is There Any Association?" Pathogens 9, no. 12: 1011. https://doi.org/10.3390/pathogens9121011