
Viral Etiological Agent(s) of Respiratory Tract Infections in Symptomatic Individuals during the Second Wave of COVID-19 Pandemic: A Single Drive-Thru Mobile Collection Site Study

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Specimen Collection
2.2. Nucleic Acids Isolation and RT-qPCR Tests
2.2.1. Detection of SARS-CoV-2
2.2.2. Differentiation of SARS-CoV-2 Variants
2.2.3. Identification of Other Respiratory Pathogens
2.3. Statistical Analysis
3. Results
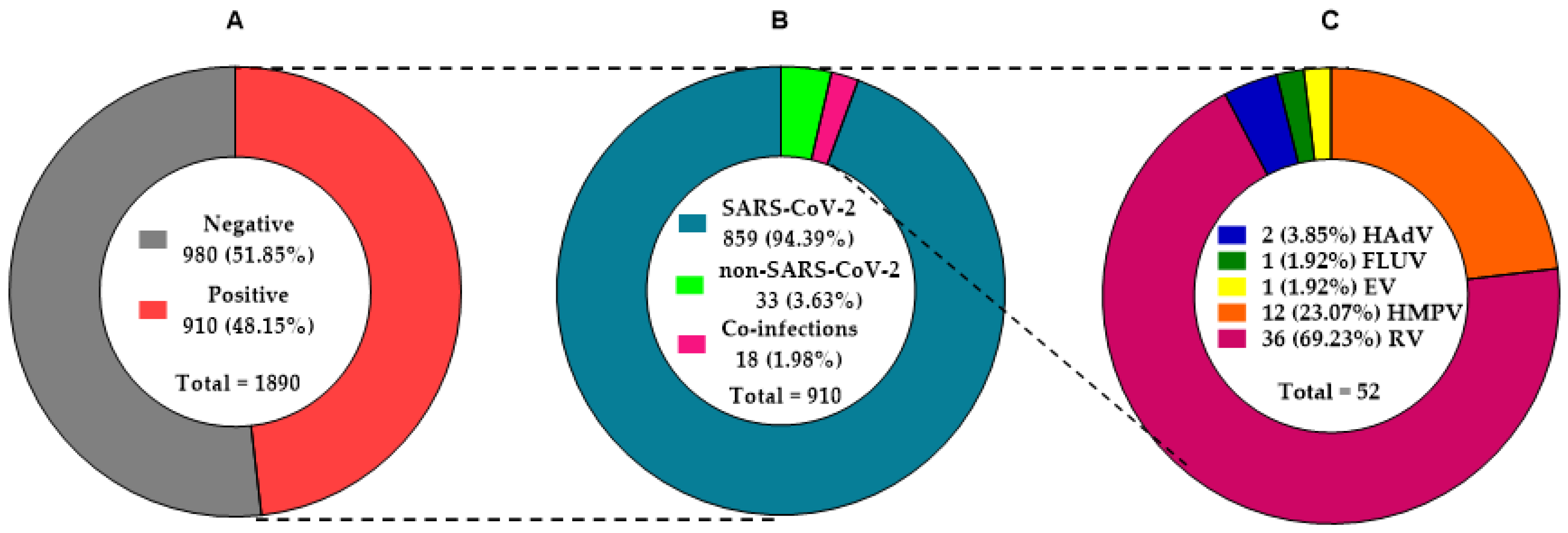
3.1. Study Specimen Characteristics
3.2. Distribution of SARS-CoV-2
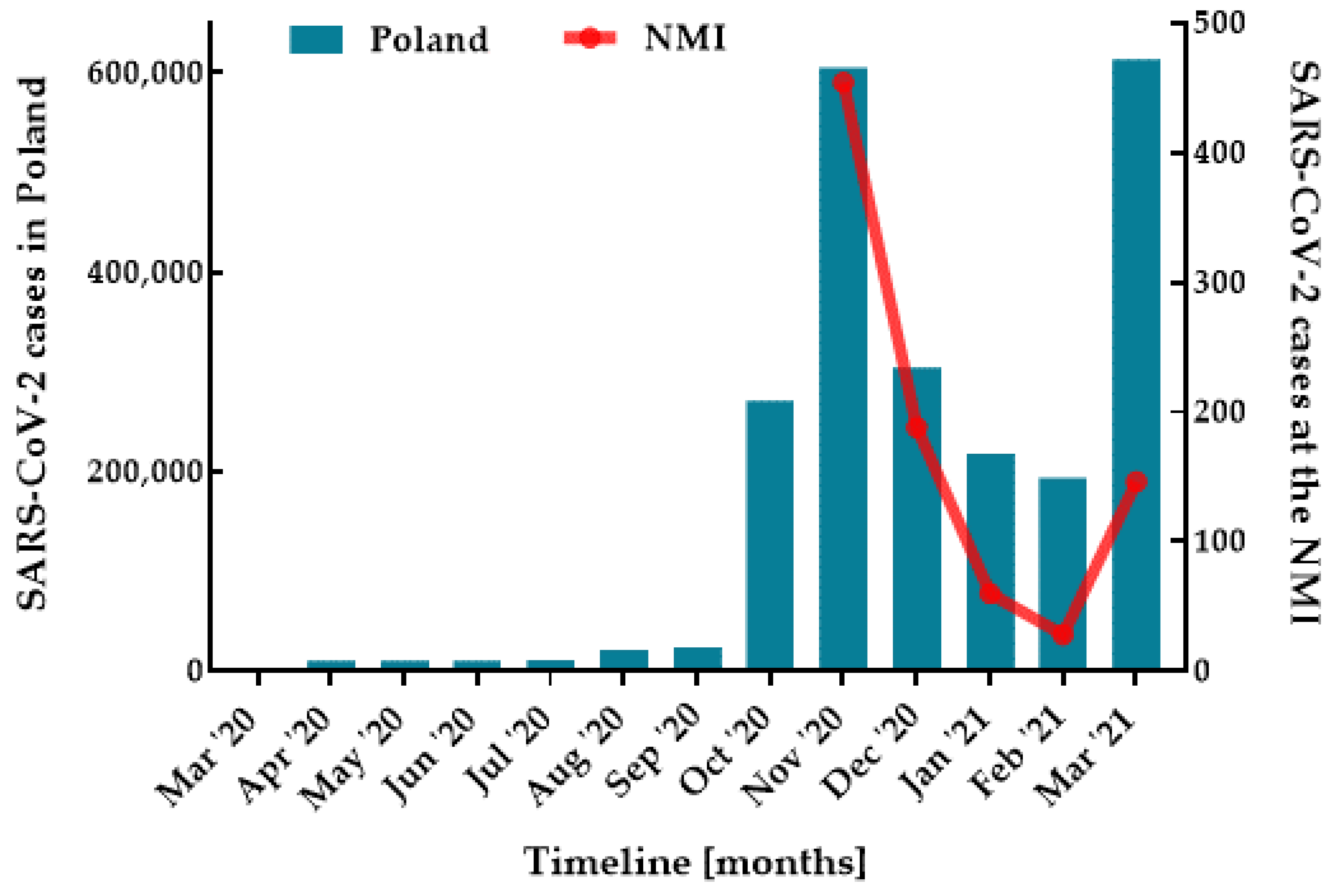
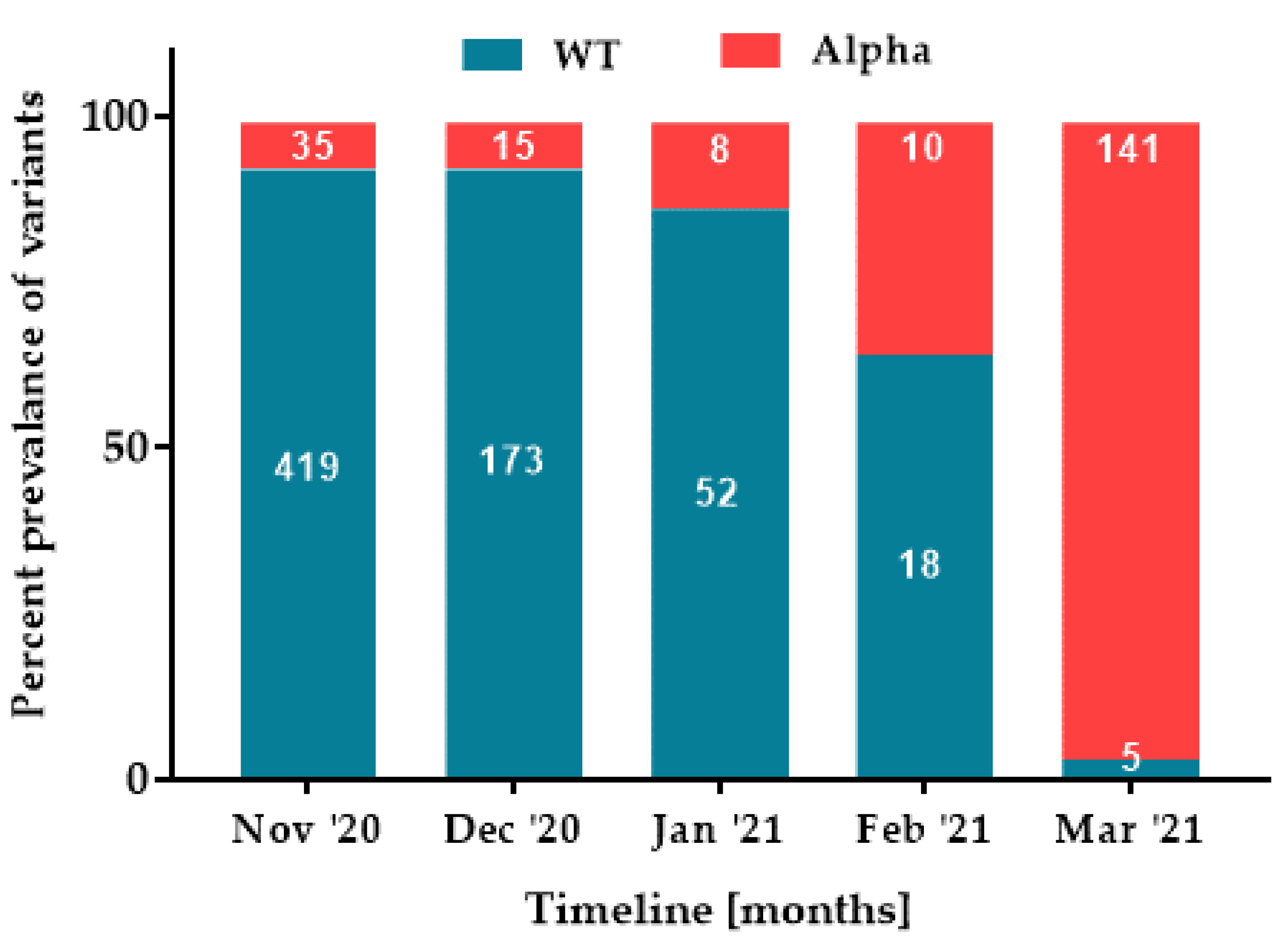
3.3. Changing Epidemiology of SARS-CoV-2
3.4. Distribution of Non-SARS-CoV-2 Respiratory Viruses
3.5. Co-Infection Rates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Forum of International Respiratory Societies. The Global Impact of Respiratory Disease. Third Edition. European Respiratory Society. 2021. Available online: https://www.firsnet.org/images/publications/FIRS_Master_09202021.pdf (accessed on 20 January 2022).
- World Health Organization. Infection Prevention and Control Measures for Acute Respiratory Infections in Healthcare Settings: An Update. Available online: https://www.who.int/publications/i/item/issn-1020-3397 (accessed on 20 January 2022).
- Mandell, L.A. Etiologies of Acute Respiratory Tract Infections. Clin. Infect. Dis. 2005, 41, 503–506. [Google Scholar] [CrossRef]
- Johnston, S.; Holgate, S. Epidemiology of viral respiratory tract infections. In Viral and Other Infections of the Human Respiratory Tract, 1st ed.; Myint, S., Taylor-Robinson, D., Eds.; Chapman & Hall: London, UK, 1996; pp. 1–28. [Google Scholar]
- Garaua, J.; Barryb, B.; Butzlerc, J.P.; Dagand, R.; Peltone, S.I. Upper respiratory tract infections: Etiology, current treatment, and experience with fluoroquinolones. Clin. Microbiol. Infect. 1998, 4, S51–S58. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Xiang, Z.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease 2019. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 20 January 2022).
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19−11-march-2020 (accessed on 20 January 2022).
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Huang, C.L.; Wang, Y.M.; Li, X.W.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 393, 1054–1062. [Google Scholar] [CrossRef]
- Komiazyk, M.; Aptowicz, A.; Ksiazek, I.; Sitkiewicz, I.; Baraniak, A. Asymptomatic carriage of severe acute respiratory syndrome coronavirus 2 by a pregnant woman and her newborn. Pol. Arch. Intern. Med. 2021, 131, 182–183. [Google Scholar] [CrossRef]
- Komiazyk, M.; Walory, J.; Gawor, J.; Ksiazek, I.; Gromadka, R.; Baraniak, A. Case Report of COVID-19 after full vaccination: Viral loads and anti-SARS-CoV-2 antibodies. Diagnostics 2021, 11, 1815. [Google Scholar] [CrossRef]
- Khodamoradi, Z.; Moghadami, M.; Lotfi, M. Co-infection of coronavirus disease 2019 and influenza A: A report from Iran. Arch. Iran Med. 2020, 23, 239–243. [Google Scholar] [CrossRef] [Green Version]
- Man-Ling, T.; Yue-Qiu, L.; Xiang, C.; Hui, L.; Zhong-Chun, J.; Dai-Li, G.; Xun, C.; Cai-Xi, T.; Zhi-Qin, X. Co-Infection with Common Respiratory Pathogens and SARS-CoV-2 in Patients with COVID-19 Pneumonia and Laboratory Biochemistry Findings: A Retrospective Cross-Sectional Study of 78 Patients from a Single Center in China. Med. Sci. Monit. 2021, 27, e929783. [Google Scholar]
- Scott, S.J.; Pfotenhauer, B.; Weiner, J.J.; Hilleshiem, J.; Khubbar, M.; Bhattacharyya, S. Respiratory Pathogen Coinfections in SARS-CoV-2-Positive Patients in Southeastern Wisconsin: A Retrospective Analysis. Microbiol. Spectr. 2021, 9, e0083121. [Google Scholar] [CrossRef] [PubMed]
- Peci, A.; Tran, V.; Guthrie, J.L.; Li, L.; Nelson, P.; Schwartz, K.L.; Eshaghi, A.; Buchan, S.A.; Gubbay, J.B. Prevalence of Co-Infections with Respiratory Viruses in Individuals Investigated for SARS-CoV-2 in Ontario, Canada. Viruses 2021, 13, 130. [Google Scholar] [CrossRef] [PubMed]
- Yanjun, S.; Zhenzhen, Z.; Rong, C.; Huiyu, Z.; Tangyuheng, L.; Minjin, W.; Xingbo, S.; Weimin, L.; Binwu, Y. Epidemiological surveillance of common respiratory viruses in patients with suspected COVID-19 in Southwest China. BMC Infect. Dis. 2020, 20, 688. [Google Scholar]
- Penela-Sánchez, D.; González-de-Audicana, J.; Armero, G.; Henares, D.; Esteva, C.; Fernández de-Sevilla, M.; Ricart, S.; Jordan, I.; Brotons, P.; Cabrerizo, M.; et al. Lower Respiratory Tract Infection and Genus Enterovirus in Children Requiring Intensive Care: Clinical Manifestations and Impact of Viral Co-Infections. Viruses 2021, 13, 2059. [Google Scholar] [CrossRef] [PubMed]
- Guan, Z.; Chen, C.; Li, Y.; Yan, D.; Zhang, X.; Jiang, D.; Yang, S.; Li, L. Impact of Coinfection With SARS-CoV-2 and Influenza on Disease Severity: A Systematic Review and Meta-Analysis. Front. Public Health 2021, 9, 773130. [Google Scholar] [CrossRef] [PubMed]
- Ginocchio, C.C.; McAdam, A.J. Current Best Practices for Respiratory Virus Testing. J. Clin. Microbiol. 2011, 49 (Suppl. 9), S44–S48. [Google Scholar] [CrossRef] [Green Version]
- Komiazyk, M.; Walory, J.; Kozinska, A.; Wasko, I.; Baraniak, A. Impact of the Nucleic Acid Extraction Method and the RT-qPCR Assay on SARS-CoV-2 Detection in Low-Viral Samples. Diagnostics 2021, 11, 2247. [Google Scholar] [CrossRef]
- Evans, L.K.; Shinagawa, A.; Sutton, S.; Calvo, L. COVID-19 Drive-Through Point of Screening and Testing (POST) System: A Safe, Efficient, and Adaptable Model for Nasopharyngeal Swab Collection. Disaster Med. Public Health Prep. 2020, 1–7. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 14 February 2022).
- Flynn, E.F.; Kuhn, E.; Shaik, M.; Tarr, E.; Scattolini, N.; Ballantine, A. Drive-Through COVID-19 Testing During the 2020 Pandemic: A safe, efficient, and scalable model for pediatric patients and healthcare workers. Acad. Pediatr. 2020, 20, 753–755. [Google Scholar] [CrossRef]
- Polish Government Newsletter. Available online: https://www.gov.pl/web/koronawirus/wykaz-zarazen-koronawirusem-sars-cov-2 (accessed on 14 February 2022).
- Choi, S.; Han, C.; Lee, J.; Kim, S.I.; Kim, I.B. Innovative screening tests for COVID-19 in South Korea. Clin. Exp. Emerg. Med. 2020, 7, 73–77. [Google Scholar] [CrossRef] [Green Version]
- Kwon, K.T.; Ko, J.H.; Shin, H.; Sung, M.; Kim, J.Y. Drive-through screening center for COVID-19: A safe and efficient screening system against massive community outbreak. J. Korean Med. Sci. 2020, 35, e123. [Google Scholar] [CrossRef] [PubMed]
- Fulawka, L.; Kuzan, A. COVID-19 Diagnostics Outside and Inside the National Health Service: A Single Institutional Experience. Diagnostics 2021, 11, 2044. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Public Health–National Institute of Hygiene, Poland. Epidemiological Reports: Information on Falling Ill with Infectious Diseases and Poisoning in Poland in 2020 Illnesses and Suspected Cases of Influenza in Poland. Available online: http://wwwold.pzh.gov.pl/oldpage/epimeld/2020/index_mp.html (accessed on 14 February 2022).
- National Institute of Public Health–National Institute of Hygiene, Poland. Epidemiological Reports: Information on Falling Ill with Infectious Diseases and Poisoning in Poland in 2021 Illnesses and Suspected Cases of Influenza in Poland. Available online: http://wwwold.pzh.gov.pl/oldpage/epimeld/2021/index_mp.html (accessed on 14 February 2022).
- Kuchar, E.; Załęski, A.; Wronowski, M.; Krankowska, D.; Podsiadły, E.; Brodaczewska, K.; Lewicka, A.; Lewicki, S.; Kieda, C.; Horban, A.; et al. Children were less frequently infected with SARS-CoV-2 than adults during 2020 COVID-19 pandemic in Warsaw, Poland. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Louca, S. SARS-CoV-2 infections in 165 countries over time. Int. J. Infect. Dis. 2021, 111, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Martín, U.; Bacigalupe, A.; Jiménez Carrillo, M. COVID-19 and gender: Certainties and uncertainties in monitoring the pandemic. Rev. Esp. Salud Publica 2021, 95, 33927179. [Google Scholar]
- Case, J.B.; Winkler, E.S.; Errico, J.M.; Diamond, M.S. On the road to ending the COVID-19 pandemic: Are we there yet? Virology 2021, 557, 70–85. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Garcia-Beltran, W.F.; Lam, E.C.; Denis, K.S.; Nitido, A.D.; Garcia, Z.H.; Hauser, B.M.; Feldman, J.; Pavlovic, M.N.; Gregory, D.J.; Poznansky, M.C.; et al. Multiple SARS-CoV-2 variants escape neutralization by vaccine-induced humoral immunity. Cell 2021, 184, 2372–2383. [Google Scholar] [CrossRef]
- World Health Organization. Tracking SARS-CoV-2 Variants as of 3 February 2022. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 14 February 2022).
- European Centre for Disease Prevention and Control. SARS-CoV-2 Variants of Concern as of 3 February 2022. Available online: https://www.ecdc.europa.eu/en/covid-19/variants-concern (accessed on 14 February 2022).
- Washington, N.L.; Gangavarapu, K.; Zeller, M.; Bolze, A.; Cirulli, E.T.; Schiabor Barrett, K.M.; Larsen, B.B.; Anderson, C.; White, S.; Cassens, T.; et al. Genomic epidemiology identifies emergence and rapid transmission of SARS-CoV-2 B.1.1.7 in the United States. MedRxiv 2021, 184, 2587–2594.e7. [Google Scholar]
- Map of SARS-CoV-2 Variants in Poland. Available online: https://dev.sarswpolsce.pl/vis/piechart_map (accessed on 28 February 2022).
- Chotpitayasunondh, T.; Kølsen Fischer, T.; Heraud, J.M.; Hurt, A.C.; Monto, A.S.; Osterhaus, A.; Shu, Y.; Tam, J.S. Influenza and COVID-19: What does co-existence mean? Influenza Other Respir. Viruses 2021, 15, 407–412. [Google Scholar] [CrossRef]
- Sharov, K.S. SARS-CoV-2-related pneumonia cases in pneumonia picture in Russia in March-May 2020: Secondary bacterial pneumonia and viral coinfections. J. Glob. Health 2020, 10, 020504. [Google Scholar] [CrossRef] [PubMed]
- Wee, L.E.; Ko, K.K.K.; Ho, W.Q.; Kwek, G.T.C.; Tan, T.T.; Wijaya, L. Community-acquired viral respiratory infections amongst hospitalized in patients during a COVID-19 outbreak in Singapore: Co-infection and clinical outcomes. J. Clin. Virol. 2020, 128, 104436. [Google Scholar] [CrossRef] [PubMed]
- Arruda, E.; Pitkaranta, A.; Witek, T.J., Jr.; Doyle, C.A.; Hayden, F.G. Frequency and natural history of rhinovirus infections in adults during autumn. J. Clin. Microbiol. 1997, 35, 2864–2868. [Google Scholar] [CrossRef] [Green Version]
- Linder, J.E.; Kraft, D.C.; Mohamed, Y.; Lu, Z.; Heil, L.; Tollefson, S.; Saville, B.R.; Wright, P.F.; Williams, J.V.; Miller, E.K. Human rhinovirus C: Age, season, and lower respiratory illness over the past 3 decades. J. Allergy Clin. Immunol. 2013, 131, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Schildgen, V.; van den Hoogen, B.; Fouchier, R.; Tripp, R.A.; Alvarez, R.; Manoha, C.; Williams, J.; Schildgen, O. Human Metapneumovirus: Lessons Learned over the First Decade. Clin. Microbiol. Rev. 2011, 24, 734–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malekifar, P.; Pakzad, R.; Shahbahrami, R.; Zandi, M.; Jafarpour, A.; Rezayat, S.A.; Akbarpour, S.; Shabestari, A.N.; Pakzad, I.; Hesari, E.; et al. Viral Coinfection among COVID-19 Patient Groups: An Update Systematic Review and Meta-Analysis. BioMed Res. Int. 2021, 2021, 5313832. [Google Scholar] [CrossRef]
- Alhumaid, S.; Al Mutair, A.; Al Alawi, Z.; Alshawi, A.M.; Alomran, S.A.; Almuhanna, M.S.; Almuslim, A.A.; Bu Shafia, A.H.; Alotaibi, A.M.; Ahmed, G.Y.; et al. Coinfections with Bacteria, Fungi, and Respiratory Viruses in Patients with SARS-CoV-2: A Systematic Review and Meta-Analysis. Pathogens 2021, 10, 809. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | No. of Samples (%) | No. of Negative Cases (%) | No. of Positive Cases (%) | SARS-CoV-2 Mono-Infection (%) | SARS-CoV-2 Co-Infection (%) | Non-SARS-CoV-2 Mono-Infection (%) | Non-SARS-CoV-2 Co-Infection (%) |
|---|---|---|---|---|---|---|---|
| Specimen collection | 1890 (100) | 980 (51.85) | 910 (48.15) | 859 (45.45) | 17 (0.9) | 33 (1.75) | 1 (0.05) |
| Female | 1041 (55.07) | 555 (53.31) | 486 (46.69) | 454 (43.61) | 12 (1.15) | 20 (1.92) | 0 (0.00) |
| Male | 849 (44.92) | 425 (50.06) | 424 (49.94) | 405 (47.70) | 5 (0.59) | 13 (1.53) | 1 (0.12) |
| Median age in years (range) | 51 (0–99) | ||||||
| 0–5 | 40 (2.12) | 29 (72.5) | 11 (27.5) | 7 (17.5) | 2 (5.0) | 2 (5.0) | 0 (0.0) |
| 6–18 | 63 (3.33) | 36 (57.14) | 27 (42.86) | 24 (38.10) | 1 (1.59) | 2 (3.17) | 0 (0.0) |
| 19–35 | 342 (18.09) | 167 (48.83) | 175 (51.17) | 164 (47.95) | 2 (0.58) | 9 (2.63) | 0 (0.0) |
| 36–64 | 1023 (54.13) | 505 (49.36) | 518 (50.64) | 491 (48.0) | 10 (0.98) | 17 (1.66) | 0 (0.0) |
| ≥65 | 422 (22.33) | 243 (57.58) | 179 (42.42) | 173 (41.0) | 2 (0.47) | 4 (0.95) | 1 (1.0) |
| Age Group | Mono-Infections, n (Female/Male) | Co-Infections, n (Female/Male) |
|---|---|---|
| RV | SARS-CoV-2 + RV | |
| Total | 22 (13/9) | 13 (9/4) |
| 0–5 | 2 (2/0) | 2 (0/2) |
| 6–18 | 2 (0/2) | 0 (0/0) |
| 19–35 | 6 (3/3) | 2 (2/0) |
| 36–64 | 11 (7/4) | 7 (6/1) |
| ≥65 | 1 (1/0) | 2 (1/1) |
| HAdV | SARS-CoV-2 + HAdV | |
| Total | 0 (0/0) | 2 (2/0) |
| 0–5 | 0 (0/0) | 0 (0/0) |
| 6–18 | 0 (0/0) | 1 (1/0) |
| 19–35 | 0 (0/0) | 0 (0/0) |
| 36–64 | 0 (0/0) | 1 (1/0) |
| ≥65 | 0 (0/0) | 0 (0/0) |
| HMPV | SARS-CoV-2 + HMPV | |
| Total | 10 (6/4) | 2 (1/1) |
| 0–5 | 0 (0/0) | 0 (0/0) |
| 6–18 | 0 (0/0) | 0 (0/0) |
| 19–35 | 3 (2/1) | 0 (0/0) |
| 36–64 | 5 (3/2) | 2 (1/1) |
| ≥65 | 2 (2/0) | 0 (0/0) |
| EV | RV + EV | |
| Total | 0 (0/0) | 1 (0/1) |
| ≥65 | 0 (0/0) | 1 (0/1) |
| FLUV | ||
| Total | 1 (1/0) | - |
| 36–64 | 1 (1/0) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kozinska, A.; Wegrzynska, K.; Komiazyk, M.; Walory, J.; Wasko, I.; Baraniak, A. Viral Etiological Agent(s) of Respiratory Tract Infections in Symptomatic Individuals during the Second Wave of COVID-19 Pandemic: A Single Drive-Thru Mobile Collection Site Study. Pathogens 2022, 11, 475. https://doi.org/10.3390/pathogens11040475
Kozinska A, Wegrzynska K, Komiazyk M, Walory J, Wasko I, Baraniak A. Viral Etiological Agent(s) of Respiratory Tract Infections in Symptomatic Individuals during the Second Wave of COVID-19 Pandemic: A Single Drive-Thru Mobile Collection Site Study. Pathogens. 2022; 11(4):475. https://doi.org/10.3390/pathogens11040475
Chicago/Turabian StyleKozinska, Aleksandra, Karolina Wegrzynska, Magdalena Komiazyk, Jaroslaw Walory, Izabela Wasko, and Anna Baraniak. 2022. "Viral Etiological Agent(s) of Respiratory Tract Infections in Symptomatic Individuals during the Second Wave of COVID-19 Pandemic: A Single Drive-Thru Mobile Collection Site Study" Pathogens 11, no. 4: 475. https://doi.org/10.3390/pathogens11040475