
A Regional Analysis of the Progress of Current Dog-Mediated Rabies Control and Prevention

Abstract
:1. Introduction
2. Results
2.1. Descriptive Analysis toward Zero by 30 Targets
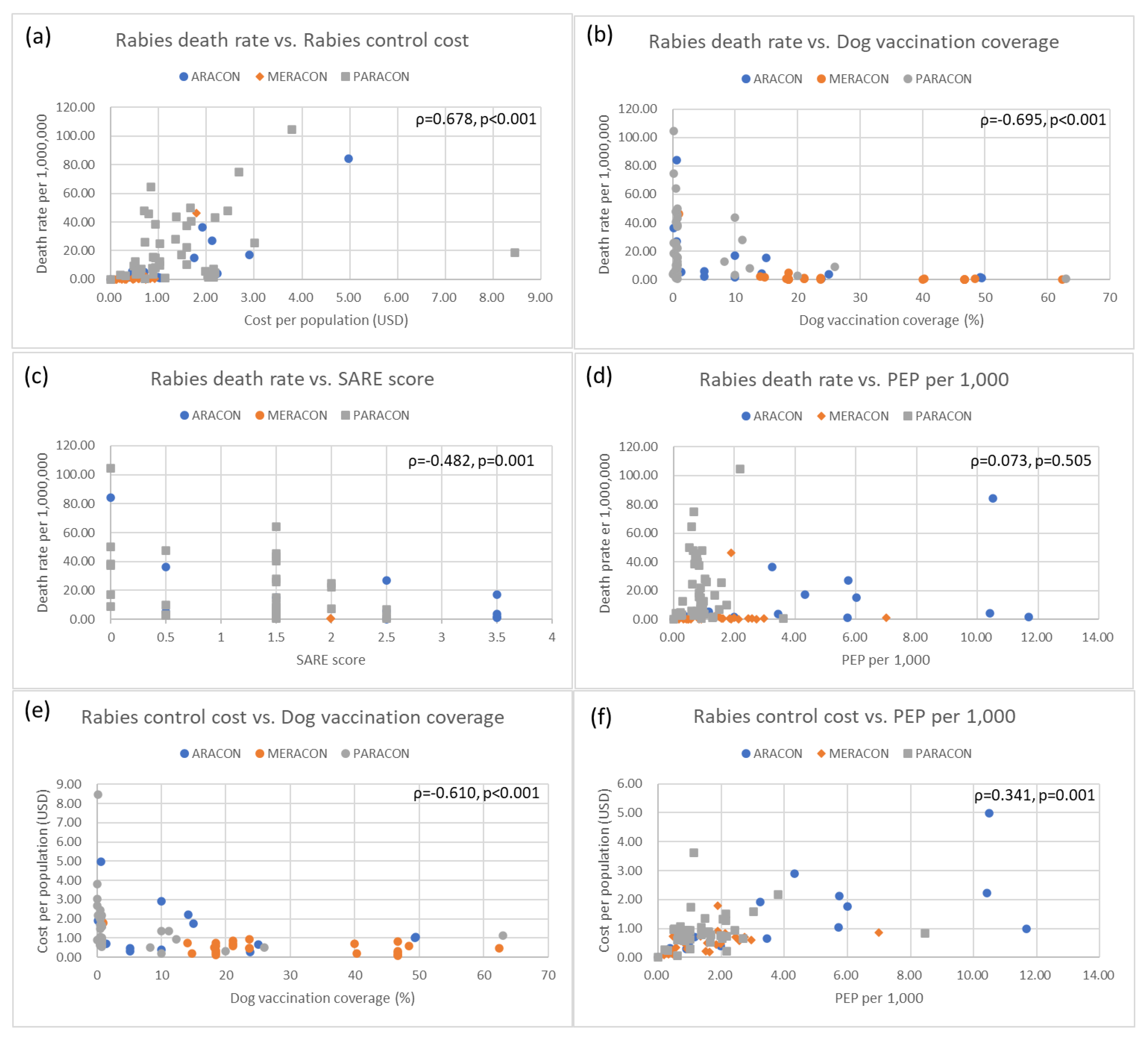
2.2. Correlational Analysis among Indicators of Rabies Prevention and Control
3. Discussion
4. Materials and Methods
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Expert Consultation on Rabies; Third Report (WHO Technical Report Series, No. 1012); World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Hampson, K.; Coudeville, L.; Lembo, T.; Sambo, M.; Kieffer, A.; Attlan, M.; Barrat, J.; Blanton, J.D.; Briggs, D.J.; Cleaveland, S.; et al. Estimating the global burden of endemic canine rabies. PLoS Negl. Trop. Dis. 2015, 9, e0003709. [Google Scholar] [CrossRef]
- World Health Organization; Food and Agriculture Organization of the United Nations; World Organisation for Animal Health; Global Alliance for Rabies Control Partners for Rabies Prevention. Zero by 30: The Global Strategic Plan to End Human Deaths from Dog-Mediated Rabies by 2030; World Health Organization, Food and Agriculture Organization of the United Nations, World Organisation for Animal Health: Geneva, Switzerland, 2018. [Google Scholar]
- Kanda, K.; Obayashi, Y.; Jayasinghe, A.; de S. Gunawardena, G.S.P.; Delpitiya, N.Y.; Priyadarshani, N.G.W.; Gamage, C.D.; Arai, A.; Tamashiro, H. Outcomes of a school-based intervention on rabies prevention among school children in rural Sri Lanka. Int. Health 2015, 7, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Matibag, G.C.; Ohbayashi, Y.; Kanda, K.; Yamashina, H.; Bandula Kumara, W.R.; Gamini Perera, I.N.; Niranjala De Silva, D.D.; Gunawardena, G.S.P.D.S.; Jayasinghe, A.; Ditangco, R.A.; et al. A pilot study on the usefulness of information and education campaign materials in enhancing the knowledge, attitude and practice on rabies in rural Sri Lanka. J. Infect. Dev. Ctries. 2009, 3, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Rouse, J.; Godbole, M.; Wells, H.L.; Boppana, S.; Schwebel, D.C. Systematic Review: Interventions to Educate Children About Dog Safety and Prevent Pediatric Dog-Bite Injuries: A Meta-Analytic Review. J. Pediatr. Psychol. 2017, 42, 779–791. [Google Scholar] [CrossRef] [PubMed]
- Duperrex, O.; Blackhall, K.; Burri, M.; Jeannot, E. Education of children and adolescents for the prevention of dog bite injuries. Cochrane Database Syst. Rev. 2009, CD004726. [Google Scholar] [CrossRef]
- Amparo, A.C.B.; Mendoza, E.C.B.; Licuan, D.A.; Valenzuela, L.M.; Madalipay, J.D.; Jayme, S.I.; Taylor, L.H. Impact of Integrating Rabies Education Into the Curriculum of Public Elementary Schools in Ilocos Norte, Philippines on Rabies Knowledge, and Animal Bite Incidence. Front. Public Health 2019, 7, 119. [Google Scholar] [CrossRef] [PubMed]
- World Organisation for Animal Health; World Health Organization; Food and Agriculture Organization of the United Nations. Rabies: Rationale for Investing in the Global Elimination of Dog-Mediated Human Rabies; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Cleaveland, S.; Kaare, M.; Tiringa, P.; Mlengeya, T.; Barrat, J. A dog rabies vaccination campaign in rural Africa: Impact on the incidence of dog rabies and human dog-bite injuries. Vaccine 2003, 21, 1965–1973. [Google Scholar] [CrossRef]
- Coleman, P.G.; Dye, C. Immunization coverage required to prevent outbreaks of dog rabies. Vaccine 1996, 14, 185–186. [Google Scholar] [CrossRef]
- Davlin, S.L.; Vonville, H.M. Canine rabies vaccination and domestic dog population characteristics in the developing world: A systematic review. Vaccine 2012, 30, 3492–3502. [Google Scholar] [CrossRef]
- Harischandra, P.A.L.; Gunesekera, A.; Janakan, N.; Gongal, G.; Abela-Ridder, B. Sri Lanka takes action towards a target of zero rabies death by 2020. WHO South East Asia J. Public Health 2016, 5, 113–116. [Google Scholar] [CrossRef] [Green Version]
- Darkaoui, S.; Cliquet, F.; Wasniewski, M.; Robardet, E.; Aboulfidaa, N.; Bouslikhane, M.; Fassi-Fihri, O. A Century Spent Combating Rabies in Morocco (1911-2015): How Much Longer? Front. Vet. Sci. 2017, 4, 78. [Google Scholar] [CrossRef]
- Nguyen, H.T.T.; Afriyie, D.O.; Tran, C.H.; Dang, A.D.; Tran, D.N.; Dang, T.Q.; Otsu, S.; Urabe, M.I.; Pham, T.N.; Nguyen, H.T.; et al. Progress towards rabies control and elimination in Vietnam. Rev. Sci. Tech. 2019, 38, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Rana, M.S.; Islam, M.K.; Chowdhury, S.; Haider, N.; Kafi, M.A.H.; Ullah, S.M.; Shah, M.R.A.; Jahan, A.A.; Mursalin, H.S.; et al. Trends and clinico-epidemiological features of human rabies cases in Bangladesh 2006–2018. Sci. Rep. 2020, 10, 2410. [Google Scholar] [CrossRef] [PubMed]
- Nihal, P.D.B.; Dangolla, A.; Hettiarachchi, R.; Abeynayake, P.; Stephen, C. Surveillance Opportunities and the Need for Intersectoral Collaboration on Rabies in Sri Lanka. J. Vet. Med. 2019, 2019, 7808517. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.H.; Knopf, L. Surveillance of Human Rabies by National Authorities—A Global Survey. Zoonoses Public Health 2015, 62, 543–552. [Google Scholar] [CrossRef]
- Banyard, A.C.; Horton, D.L.; Freuling, C.; Müller, T.; Fooks, A.R. Control and prevention of canine rabies: The need for building laboratory-based surveillance capacity. Antivir. Res. 2013, 98, 357–364. [Google Scholar] [CrossRef]
- Kanda, K.; Jayasinghe, A.; Jayasinghe, C.; Yoshida, T. Public health implication towards rabies elimination in Sri Lanka: A systematic review. Acta Trop. 2021, 223, 106080. [Google Scholar] [CrossRef]
- Thomas, L.F.; Rushton, J.; Bukachi, S.A.; Falzon, L.C.; Howland, O.; Fèvre, E.M. Cross-Sectoral Zoonotic Disease Surveillance in Western Kenya: Identifying Drivers and Barriers Within a Resource Constrained Setting. Front. Vet. Sci. 2021, 8, 658454. [Google Scholar] [CrossRef]
- Fooks, A.R.; Banyard, A.C.; Horton, D.L.; Johnson, N.; McElhinney, L.M.; Jackson, A.C. Current status of rabies and prospects for elimination. Lancet 2014, 384, 1389–1399. [Google Scholar] [CrossRef]
- Scott, T.P.; Coetzer, A.; de Balogh, K.; Wright, N.; Nel, L.H. The Pan-African Rabies Control Network (PARACON): A unified approach to eliminating canine rabies in Africa. Antivir. Res. 2015, 124, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Coetzer, A.; Scott, T.P.; Amparo, A.C.; Jayme, S.; Nel, L.H. Formation of the Asian Rabies Control Network (ARACON): A common approach towards a global good. Antivir. Res. 2018, 157, 134–139. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Expert Consultation on Rabies: Second Report; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Knobel, D.L.; Cleaveland, S.; Coleman, P.G.; Fèvre, E.M.; Meltzer, M.I.; Miranda, M.E.; Shaw, A.; Zinsstag, J.; Meslin, F.X. Re-evaluating the burden of rabies in Africa and Asia. Bull. World Health Organ. 2005, 83, 360–368. [Google Scholar] [PubMed]
- US Centers for Disease Control and Prevention. Is Rabies in Your State? Available online: https://www.cdc.gov/rabies/location/usa/surveillance/ (accessed on 9 April 2021).
- Vigilato, M.A.; Clavijo, A.; Knobl, T.; Silva, H.M.; Cosivi, O.; Schneider, M.C.; Leanes, L.F.; Belotto, A.J.; Espinal, M.A. Progress towards eliminating canine rabies: Policies and perspectives from Latin America and the Caribbean. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2013, 368, 20120143. [Google Scholar] [CrossRef] [PubMed]
- Ueki, H. Tokyo Rabies Epidemic Journal (Reprint Edition); Jiku Publishers: Tokyo, Japan, 2007; ISBN 978-4-88267-041-4. (In Japanese) [Google Scholar]
- Ministry of Health, Labour and Welfare of Japan [MHLW]. Rabies. Available online: https://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou10/ (accessed on 14 September 2021). (In Japanese).
- MHLW. Annual Trend of the Number of Registered and Vaccinated Dogs in 1955–2019. Available online: https://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou10/02.html (accessed on 14 September 2021). (In Japanese).
- Velasco-Villa, A.; Escobar, L.E.; Sanchez, A.; Shi, M.; Streicker, D.G.; Gallardo-Romero, N.F.; Vargas-Pino, F.; Gutierrez-Cedillo, V.; Damon, I.; Emerson, G. Successful strategies implemented towards the elimination of canine rabies in the Western Hemisphere. Antivir. Res. 2017, 143, 1–12. [Google Scholar] [CrossRef]
- Global Alliance for Rabies Control. Stepwise Approach towards Rabies Elimination (SARE). Available online: https://rabiesalliance.org/tools/planning-tools/sare (accessed on 20 August 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ARACON (n = 15) | MERACON (n = 25) | PARACON (n=48) | TOTAL (n = 88) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Intervention: | |||||||||
| Death rate per 1,000,000 | 13.7 | (0–4.2) | 2.5 | (0–46.5) | 21.5 | (0.5–104.7) | 14.5 | (0–04.7) | <0.001 |
| Dog vaccination coverage (%) | 15.0 | (0.2–49.5) | 29.1 | (1–62.4) | 4.1 | (0.1–63.0) | 13.3 | (0.1–63.0) | <0.001 |
| Cost per population (USD) | 1.4 | (0–5.0) | 0.5 | (0–1.8) | 1.5 | (0–8.5) | 1.2 | (0–8.5) | <0.001 |
| PEP per 1000 | 4.4 | (0–11.7) | 1.6 | (0–7.0) | 0.9 | (0–3.6) | 1.7 | (0–1.7) | 0.001 |
| Policies: | |||||||||
| Top five priority diseases (%) | 12 | (80.0%) | 1 | (4.0%) | 16 | (33.3%) | 29 | (33.0%) | <0.001 |
| Notifiable in human (%) | 10 | (66.7%) | 3 | (12.0%) | 32 | (66.7%) | 45 | (51.1%) | <0.001 |
| Notifiable in animals (%) | 14 | (93.3%) | 3 | (12.0%) | 33 | (68.8%) | 50 | (56.8%) | <0.001 |
| National strategy | |||||||||
| Available (%) | 9 | (60.0%) | 0 | (0.0%) | 7 | (14.6%) | 16 | (18.2%) | <0.001 |
| Being developed (%) | 4 | (26.7%) | 2 | (8.0%) | 11 | (22.9%) | 17 | (19.3%) | |
| One Health working group or Rabies task force (%) | 9 | (60.0%) | 3 | (12.0%) | 22 | (45.8%) | 34 | (38.6%) | 0.003 |
| Stepwise Approach towards Rabies Elimination (SARE) Score | 2.1 | (0–3.5) | 1.8 | (1.5–2.0) | 1.2 | (0–2.5) | 1.5 | (0–3.5) | 0.043 |
| Death Rate Per 1,000,000 | Dog Vaccination Coverage | Cost Per Population | PEP Per 1000 | |||||
|---|---|---|---|---|---|---|---|---|
| Number | p-Value | Number | p-Value | Number | p-Value | Number | p-Value | |
| Disease priority | ||||||||
| Yes | 12.165 | 0.015 | 11.782 | 0.001 | 1.015 | 0.015 | 2.345 | 0.299 |
| No | 45.686 | 0.395 | 2.478 | 3.180 | ||||
| Notifiable in human | ||||||||
| Yes | 16.940 | 0.856 | 9.624 | 0.241 | 1.106 | 0.121 | 1.734 | 0.645 |
| No | 21.310 | 3.237 | 1.960 | 3.172 | ||||
| Notifiable in animals | ||||||||
| Yes | 18.079 | 0.586 | 9.055 | 0.427 | 1.222 | 0.882 | 1.999 | 0.092 |
| No | 4.913 | 0.650 | 1.303 | 0.409 | ||||
| National strategy | ||||||||
| Available/Being developed | 17.987 | 0.953 | 10.981 | 0.526 | 1.374 | 0.284 | 2.941 | <0.001 |
| No | 16.116 | 4.982 | 1.028 | 0.689 | ||||
| One Health | ||||||||
| Yes | 14.495 | 0.273 | 9.770 | 0.198 | 1.171 | 0.846 | 1.635 | 0.705 |
| No | 23.486 | 6.720 | 1.332 | 2.519 | ||||
| SARE score | ||||||||
| Less than 2.0 | 22.943 | 0.013 | 6.135 | 0.194 | 1.325 | 0.488 | 2.143 | 0.165 |
| 2.0 and above | 8.045 | 15.249 | 1.128 | 2.253 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanda, K.; Jayasinghe, A.; Jayasinghe, C.; Yoshida, T. A Regional Analysis of the Progress of Current Dog-Mediated Rabies Control and Prevention. Pathogens 2022, 11, 1130. https://doi.org/10.3390/pathogens11101130
Kanda K, Jayasinghe A, Jayasinghe C, Yoshida T. A Regional Analysis of the Progress of Current Dog-Mediated Rabies Control and Prevention. Pathogens. 2022; 11(10):1130. https://doi.org/10.3390/pathogens11101130
Chicago/Turabian StyleKanda, Koji, Ananda Jayasinghe, Chandrika Jayasinghe, and Takahiko Yoshida. 2022. "A Regional Analysis of the Progress of Current Dog-Mediated Rabies Control and Prevention" Pathogens 11, no. 10: 1130. https://doi.org/10.3390/pathogens11101130