
Screening for Vaginal and Endocervical Infections in the First Trimester of Pregnancy? A Study That Ignites an Old Debate



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Procedures
- -
- Normal or usual flora: Nugent score between 0 and 3 and no other pathogen isolated in the cultures;
- -
- Intermediate flora: Nugent score between 4 and 6 and no other pathogen isolated in the cultures;
- -
- Abnormal flora: Nugent score between 7 and 10 (and therefore diagnosis of bacterial vaginosis), or if another pathogen was isolated in the cultures.
- ○
- Bacterial vaginosis: 2% vaginal clindamycin (5 g) every 24 h for 6 nights;
- ○
- Ureaplasma/Mycoplasma *: Azithromycin 1 g oral weekly for 2 weeks;
- ○
- Candida spp.: Clotrimazole vaginal ovules 100 mg every 24 h for 6 nights;
- ○
- Neisseria gonorrhoeae *: a single dose of Ceftriaxone 250 mg intramuscular;
- ○
- Trichomonas vaginalis *: vaginal metronidazole 500 mg for 7 nights.
2.3. Outcomes
- Gestational age, signs or symptoms at the time of sample collection (leukorrhea, erythema, bad odor, itching), vaginal discomfort with sample collection (referred by the patient from 1 to 5);
- Antecedents of interest: maternal age, active smoking habit (and number of cigarettes per day), the antecedent of conization and obstetric history;
- Adverse obstetric events in previous pregnancies: late miscarriage; threatened preterm labor (TPL), determined as cervical changes caused by regular uterine contractions occurring before 35 weeks and which required hospitalization and administration of tocolytic therapy; preterm premature rupture of membranes (PPROM); preterm delivery (PTB); or chorioamnionitis;
- Current pregnancy data: cervical length at the 20-week scan, urine culture results, Group B Streptococcus culture result, the episodes of symptomatic vaginal infections during pregnancy, the need for fetal lung maduration, and adverse obstetric events (described above);
- Delivery data: mode of delivery (and its reason in the case of cesarean section or instrumental delivery), gestational age at the time of delivery, intrapartum fever, postpartum endometritis;
- Newborn data: Apgar score, type of newborn resuscitation if needed, blood cord pH at birth, birth weight and neonatal morbidity or adverse neonatal events (admission in neonatal unit, admission to NICU, mechanical ventilation, respiratory distress, interventricular hemorrhage or retinopathy).
2.4. Statistical Analysis
3. Results
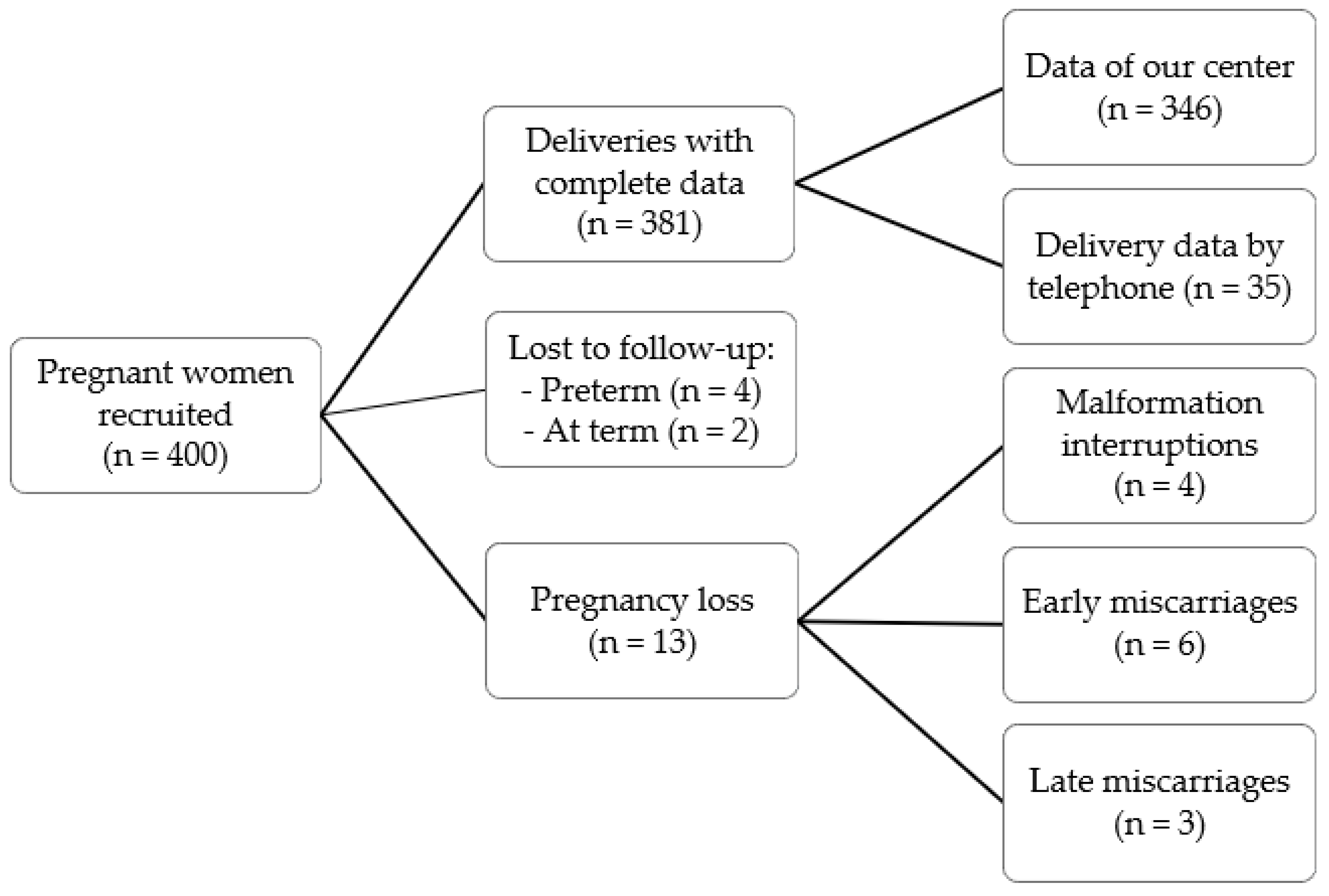
3.1. Recruitment
3.2. The Results of the Analyzed Smears of the Study Population (n = 400)
3.3. Comparative Analysis
3.3.1. Signs and/or Symptoms at the Time of Sample Collection
3.3.2. Adverse Events in Previous Pregnancies
3.3.3. Adverse Events in Current Pregnancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- da Fonseca, E.B.; Damião, R.; Moreira, D.A. Preterm birth prevention. Best Pract. Res. Clin. Obstet. Gynaecol. 2020, 69, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Walani, S.R. Global burden of preterm birth. Int. J. Gynaecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef] [PubMed]
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.B.; Narwal, R.; Adler, A.; Vera Garcia, C.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frey, H.A.; Klebanoff, M.A. The epidemiology, etiology, and costs of preterm birth. Semin. Fetal Neonatal Med. 2016, 21, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Dey, S.K.; Fisher, S.J. Preterm labor: One syndrome, many causes. Science 2014, 345, 760–765. [Google Scholar] [CrossRef] [Green Version]
- Hillier, S.L.; Nugent, R.P.; Eschenbach, D.A.; Krohn, M.A.; Gibbs, R.S.; Martin, D.H.; Cotch, M.F.; Edelman, R.; Pastorek, J.G., 2nd; Rao, A.V.; et al. Association between bacterial vaginosis and preterm delivery of a low-birth-weight infant. The Vaginal Infections and Prematurity Study Group. N. Engl. J. Med. 1995, 333, 1737–1742. [Google Scholar] [CrossRef] [PubMed]
- Kiss, H.; Petricevic, L.; Husslein, P. Prospective randomised controlled trial of an infection screening programme to reduce the rate of preterm delivery. BMJ 2004, 329, 371. [Google Scholar] [CrossRef] [Green Version]
- Leitich, H.; Kiss, H. Asymptomatic bacterial vaginosis and intermediate flora as risk factors for adverse pregnancy outcome. Best Pract. Res. Clin. Obstet. Gynaecol. 2007, 21, 375–390. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G.; Van Calsteren, K.; Bellen, G.; Reybrouck, R.; Van den Bosch, T.; Riphagen, I.; Van Lierde, S. Predictive value for preterm birth of abnormal vaginal flora, bacterial vaginosis and aerobic vaginitis during the first trimester of pregnancy. BJOG 2009, 116, 1315–1324. [Google Scholar] [CrossRef] [PubMed]
- Farr, A.; Kiss, H.; Hagmann, M.; Machal, S.; Holzer, I.; Kueronya, V.; Husslein, P.W.; Petricevic, L. Role of Lactobacillus Species in the Intermediate Vaginal Flora in Early Pregnancy: A Retrospective Cohort Study. PLoS ONE 2015, 10, e0144181. [Google Scholar] [CrossRef]
- Murtha, A.P.; Edwards, J.M. The role of Mycoplasma and Ureaplasma in adverse pregnancy outcomes. Obstet. Gynecol. Clin. N. Am. 2014, 41, 615–627. [Google Scholar] [CrossRef] [PubMed]
- Capoccia, R.; Greub, G.; Baud, D. Ureaplasma urealyticum, Mycoplasma hominis and adverse pregnancy outcomes. Curr. Opin. Infect. Dis. 2013, 26, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Kwak, D.W.; Hwang, H.S.; Kwon, J.Y.; Park, Y.W.; Kim, Y.H. Co-infection with vaginal Ureaplasma urealyticum and Mycoplasma hominis increases adverse pregnancy outcomes in patients with preterm labor or preterm premature rupture of membranes. J. Matern. Fetal Neonatal Med. 2014, 27, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Farr, A.; Kiss, H.; Holzer, I.; Husslein, P.; Hagmann, M.; Petricevic, L. Effect of asymptomatic vaginal colonization with Candida albicans on pregnancy outcome. Acta Obstet. Gynecol. Scand. 2015, 94, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Vouga, M.; Greub, G.; Prod’hom, G.; Durussel, C.; Roth-Kleiner, M.; Vasilevsky, S.; Baud, D. Treatment of genital mycoplasma in colonized pregnant women in late pregnancy is associated with a lower rate of premature labour and neonatal complications. Clin. Microbiol. Infect. 2014, 20, 1074–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subtil, D.; Brabant, G.; Tilloy, E.; Devos, P.; Canis, F.; Fruchart, A.; Bissinger, M.C.; Dugimont, J.C.; Nolf, C.; Hacot, C.; et al. Early clindamycin for bacterial vaginosis in pregnancy (PREMEVA): A multicentre, double-blind, randomised controlled trial. Lancet 2018, 392, 2171–2179. [Google Scholar] [CrossRef] [PubMed]
- Brocklehurst, P.; Gordon, A.; Heatley, E.; Milan, S.J. Antibiotics for treating bacterial vaginosis in pregnancy. Cochrane Database Syst. Rev. 2013, CD000262. [Google Scholar] [CrossRef] [Green Version]
- Shimaoka, M.; Yo, Y.; Doh, K.; Kotani, Y.; Suzuki, A.; Tsuji, I.; Mandai, M.; Matsumura, N. Association between preterm delivery and bacterial vaginosis with or without treatment. Sci. Rep. 2019, 9, 509. [Google Scholar] [CrossRef]
- Rebouças, K.F.; Eleutério, J., Jr.; Peixoto, R.C.; Costa, A.P.F.; Cobucci, R.N.; Gonçalves, A.K. Treatment of bacterial vaginosis before 28 weeks of pregnancy to reduce the incidence of preterm labor. Int. J. Gynaecol. Obstet. 2019, 146, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Peelen, M.J.; Luef, B.M.; Lamont, R.F.; de Milliano, I.; Jensen, J.S.; Limpens, J.; Hajenius, P.J.; Jørgensen, J.S.; Menon, R.; PREBIC Biomarker Working Group 2014–2018. The influence of the vaginal microbiota on preterm birth: A systematic review and recommendations for a minimum dataset for future research. Placenta 2019, 79, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGregor, J.A.; French, J.I. Bacterial vaginosis in pregnancy. Obstet. Gynecol. Surv. 2000, 55 (Suppl. S1), 1–19. [Google Scholar] [CrossRef] [PubMed]
- Aguin, T.J.; Sobel, J.D. Vulvovaginal candidiasis in pregnancy. Curr. Infect. Dis. Rep. 2015, 17, 462. [Google Scholar] [CrossRef] [PubMed]
- Nugent, R.P.; Krohn, M.A.; Hillier, S.L. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J. Clin. Microbiol. 1991, 29, 297–301. [Google Scholar] [CrossRef] [Green Version]
- Shore García, L.; Isenberg, H.D. American Society for Microbiology. In Clinical Microbiology Procedures Handbook, 3rd ed.; ASM Press: Washington, DC, USA, 2010. [Google Scholar]
- Vázquez, F.; Aznar, J.; Blanco, M.A.; Lepe, J.A.; Otero, L.; Vázquez, F. Diagnóstico microbiológico de las infecciones de transmisión sexual y otras infecciones genitales. In Procedimientos en Microbiología Clínica nº 24, 2nd ed.; SEIMC: Madrid, Spain, 2007. [Google Scholar]
- Workowski, K.A.; Bolan, G.A.; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm. Rep. 2015, 64, 1–137. [Google Scholar]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 48. [Google Scholar] [CrossRef]
- Lamont, R.F.; Nhan-Chang, C.L.; Sobel, J.D.; Workowski, K.; Conde-Agudelo, A.; Romero, R. Treatment of abnormal vaginal flora in early pregnancy with clindamycin for the prevention of spontaneous preterm birth: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2011, 205, 177–190. [Google Scholar] [CrossRef] [Green Version]
- Donadono, V.; Saccone, G.; Maruotti, G.M.; Berghella, V.; Migliorini, S.; Esposito, G.; Sirico, A.; Tagliaferri, S.; Ward, A.; Mazzarelli, L.L.; et al. Incidence of toxoplasmosis in pregnancy in Campania: A population-based study on screening, treatment, and outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 240, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Billette De Villemeur, A.; Tattevin, P.; Salmi, L.R.; French Haut Conseil de la santé publique Working Group. Hygiene promotion might be better than serological screening to deal with Cytomegalovirus infection during pregnancy: A methodological appraisal and decision analysis. BMC Infect. Dis. 2020, 20, 418. [Google Scholar] [CrossRef]
- Wingert, A.; Pillay, J.; Sebastianski, M.; Gates, M.; Featherstone, R.; Shave, K.; Vandermeer, B.; Hartling, L. Asymptomatic bacteriuria in pregnancy: Systematic reviews of screening and treatment effectiveness and patient preferences. BMJ Open 2019, 9, e021347. [Google Scholar] [CrossRef] [Green Version]
- Haahr, T.; Ersbøll, A.S.; Karlsen, M.A.; Svare, J.; Sneider, K.; Hee, L.; Weile, L.K.; Ziobrowska-Bech, A.; Østergaard, C.; Jensen, J.S.; et al. Treatment of bacterial vaginosis in pregnancy in order to reduce the risk of spontaneous preterm delivery-a clinical recommendation. Acta Obstet. Gynecol. Scand. 2016, 95, 850–860. [Google Scholar] [CrossRef] [PubMed]
- Lamont, R.F.; Keelan, J.A.; Larsson, P.G.; Jørgensen, J.S. The treatment of bacterial vaginosis in pregnancy with clindamycin to reduce the risk of infection-related preterm birth: A response to the Danish Society of Obstetrics and Gynecology guideline group’s clinical recommendations. Acta Obstet. Gynecol. Scand. 2017, 96, 139–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redelinghuys, M.J.; Geldenhuys, J.; Jung, H.; Kock, M.M. Bacterial Vaginosis: Current Diagnostic Avenues and Future Opportunities. Front. Cell Infect. Microbiol. 2020, 10, 354. [Google Scholar] [CrossRef] [PubMed]
- Masson, L.; Barnabas, S.; Deese, J.; Lennard, K.; Dabee, S.; Gamieldien, H.; Jaumdally, S.Z.; Williamson, A.L.; Little, F.; Van Damme, L.; et al. Inflammatory cytokine biomarkers of asymptomatic sexually transmitted infections and vaginal dysbiosis: A multicentre validation study. Sex. Transm. Infect. 2019, 95, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Foessleitner, P.; Kiss, H.; Deinsberger, J.; Ott, J.; Zierhut, L.; Rosta, K.; Falcone, V.; Farr, A. Screening Pregnant Women for Bacterial Vaginosis Using a Point-of-Care Test: A Prospective Validation Study. J. Clin. Med. 2021, 10, 2275. [Google Scholar] [CrossRef] [PubMed]
- Hoyme, U.B.; Hesse, M. Reduced incidence of early preterm birth in the State of Thuringia following an intravaginal pH-self-monitoring screening program. Arch. Gynecol. Obstet. 2020, 302, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Kiss, H.; Pichler, E.; Petricevic, L.; Husslein, P. Cost effectiveness of a screen-and-treat program for asymptomatic vaginal infections in pregnancy: Towards a significant reduction in the costs of prematurity. Eur. J. Obstet. Gynecol. Reprod. Biol. 2006, 127, 198–203. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Flora | Category | Number of Patients (%) | Total Percentage of Type of Flora | |
|---|---|---|---|---|
| Normal | 291 (72.8) | 72.8 | ||
| Intermediate | 9 (2.2) | 2.2 | ||
| Abnormal | Ureaplasma urealyticum | Total: Isolated Associated with others 2 | 49 (12.3) 28 21 | 25.0 |
| Candida spp. | Total: Isolated Asociated with UU 3 | 47 (11.8) 37 10 | ||
| Bacterial Vaginosis 1 | Total: Isolated Asociated with UU 3 | 20 (5.0) 12 8 | ||
| Mycoplasma hominis | Total: Isolated Asociated with UU 3 | 5 (1.2) 1 4 | ||
| Trichomonas vaginalis | Total: Isolated Asociated with UU 3 | 3 (0.8) 1 2 | ||
| Signs and/or Symptoms a | Normal Flora n = 268 | Intermediate Flora n = 8 | Abnormal Flora n = 90 | p-Value 3 Groups | p-Value 2 Groups b | OR (95%CI) 2 Groups b |
|---|---|---|---|---|---|---|
| No Signs or Symptoms | 257 (95.9) | 7 (87.5) | 74 (82.2) | <0.001 * | <0.001 * | 5.05 (2.25–11.32) |
| Signs or Symptoms | 11 (4.1) | 1 (12.5) | 16 (17.8) |
| Previous Obstetric Adverse Event a | Normal Flora n = 158 | Intermediate Flora n = 7 | Abnormal Flora n = 54 | p-Value 3 Groups | p-Value 2 Groups b | OR (95% CI) 2 Groups b |
|---|---|---|---|---|---|---|
| Yes | 17 (10.8) | 0 (0.0) | 12 (22.2) | 0.058 | 0.034 * | 2.37 (1.05–5.33) |
| No | 141 (89.2) | 7 (100.0) | 42 (77.8) |
| Adverse Event | Normal Flora n = 283 | Intermediate Flora n = 9 | Abnormal Flora n = 98 | p-Value 3 Groups | p-Value 2 Groups a |
|---|---|---|---|---|---|
| Late Miscarriage | 1 (0.4) | 0/9 (0.0) | 2 (2.0) | 0.248 | 0.164 |
| Chorioamnionitis | 4 (1.4) | 0/9 (0.0) | 2 (2.0) | 0.847 | 0.650 |
| TPL | 6/279 (2.2) | 0/9 (0.0) | 2/95 (2.1) | 0.906 | 1.000 |
| PPROM | 3/279 (1.1) | 0/9 (0.0) | 5/95 (5.3) | 0.043 * | 0.028 * |
| Preterm Delivery | 17/279 (6.1) | 0/9 (0.0) | 6/95 (6.3) | 0.743 | 0.938 |
| Birth Weight | Normal Flora n = 277 | Intermediate Flora n = 9 | Abnormal Flora n = 93 | p-Value 3 Groups | p-Value 2 Groups a |
|---|---|---|---|---|---|
| Weight in grams (median, IQR) | 3266 (2980–3588) | 3110 (3060–3578) | 3288 (3056–3674) | 0.318 | 0.144 |
| Weight < 2500 g | 15 (5.4) | 0 (0.0) | 2 (2.2) | 0.339 | 0.259 |
| Neonatal Morbidity | |||||
| Admission in neonatal unit | 17 (6.1) | 1 (11.1) | 4 (4.2) | 0.621 | 0.491 |
| Admission to NICU | 8 (2.9) | 0 (0.0) | 0 (0.0) | 0.218 | 0.211 |
| Mechanical ventilation | 1 (0.4) | 0 (0.0) | 1 (1.1) | 0.703 | 0.444 |
| Respiratory distress | 10 (3.6) | 0 (0.0) | 3 (3.2) | 0.834 | 1.000 |
| Interventricular hemorrhage | 1 (0.4) | 0 (0.0) | 0 (0.0) | 0.830 | 1.000 |
| Retinopathy | 1 (0.4) | 0 (0.0) | 0 (0.0) | 0.830 | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toboso Silgo, L.; Cruz-Melguizo, S.; de la Cruz Conty, M.L.; Encinas Pardilla, M.B.; Muñoz Algarra, M.; Nieto Jiménez, Y.; Arranz Friediger, A.; Martínez-Pérez, Ó. Screening for Vaginal and Endocervical Infections in the First Trimester of Pregnancy? A Study That Ignites an Old Debate. Pathogens 2021, 10, 1610. https://doi.org/10.3390/pathogens10121610
Toboso Silgo L, Cruz-Melguizo S, de la Cruz Conty ML, Encinas Pardilla MB, Muñoz Algarra M, Nieto Jiménez Y, Arranz Friediger A, Martínez-Pérez Ó. Screening for Vaginal and Endocervical Infections in the First Trimester of Pregnancy? A Study That Ignites an Old Debate. Pathogens. 2021; 10(12):1610. https://doi.org/10.3390/pathogens10121610
Chicago/Turabian StyleToboso Silgo, Leonie, Sara Cruz-Melguizo, María Luisa de la Cruz Conty, María Begoña Encinas Pardilla, María Muñoz Algarra, Yolanda Nieto Jiménez, Alexandra Arranz Friediger, and Óscar Martínez-Pérez. 2021. "Screening for Vaginal and Endocervical Infections in the First Trimester of Pregnancy? A Study That Ignites an Old Debate" Pathogens 10, no. 12: 1610. https://doi.org/10.3390/pathogens10121610