
Surveillance of SARS-CoV-2 in Sewage Treatment Plants between January 2020 and July 2021 in Taiwan

Abstract
:1. Introduction
2. Results
3. Discussion
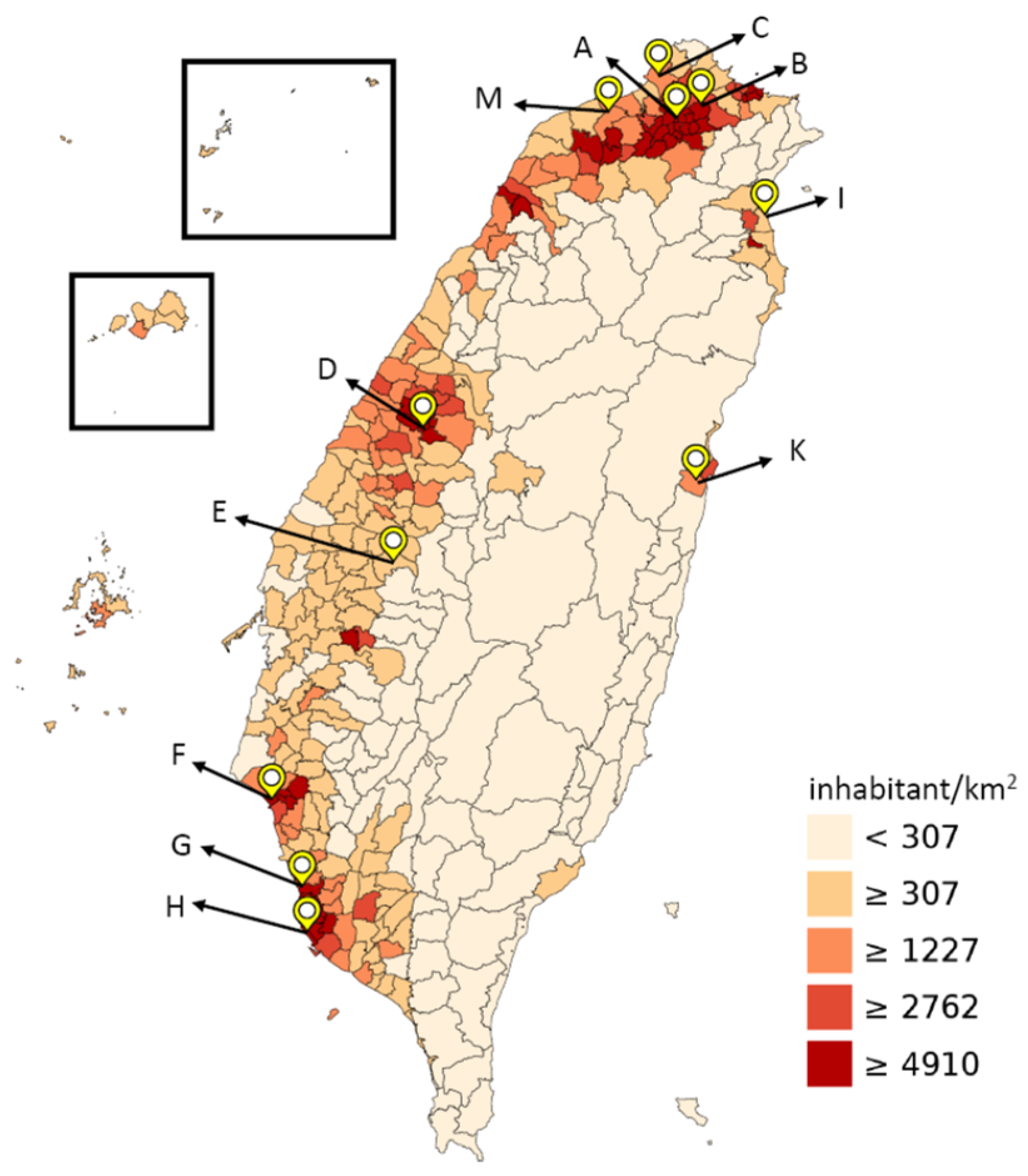
3.1. The Relationship between Sewage Treatment Plants and Population Density
3.2. The Frequency of Sampling and Detection from Sewage Treatment Plants
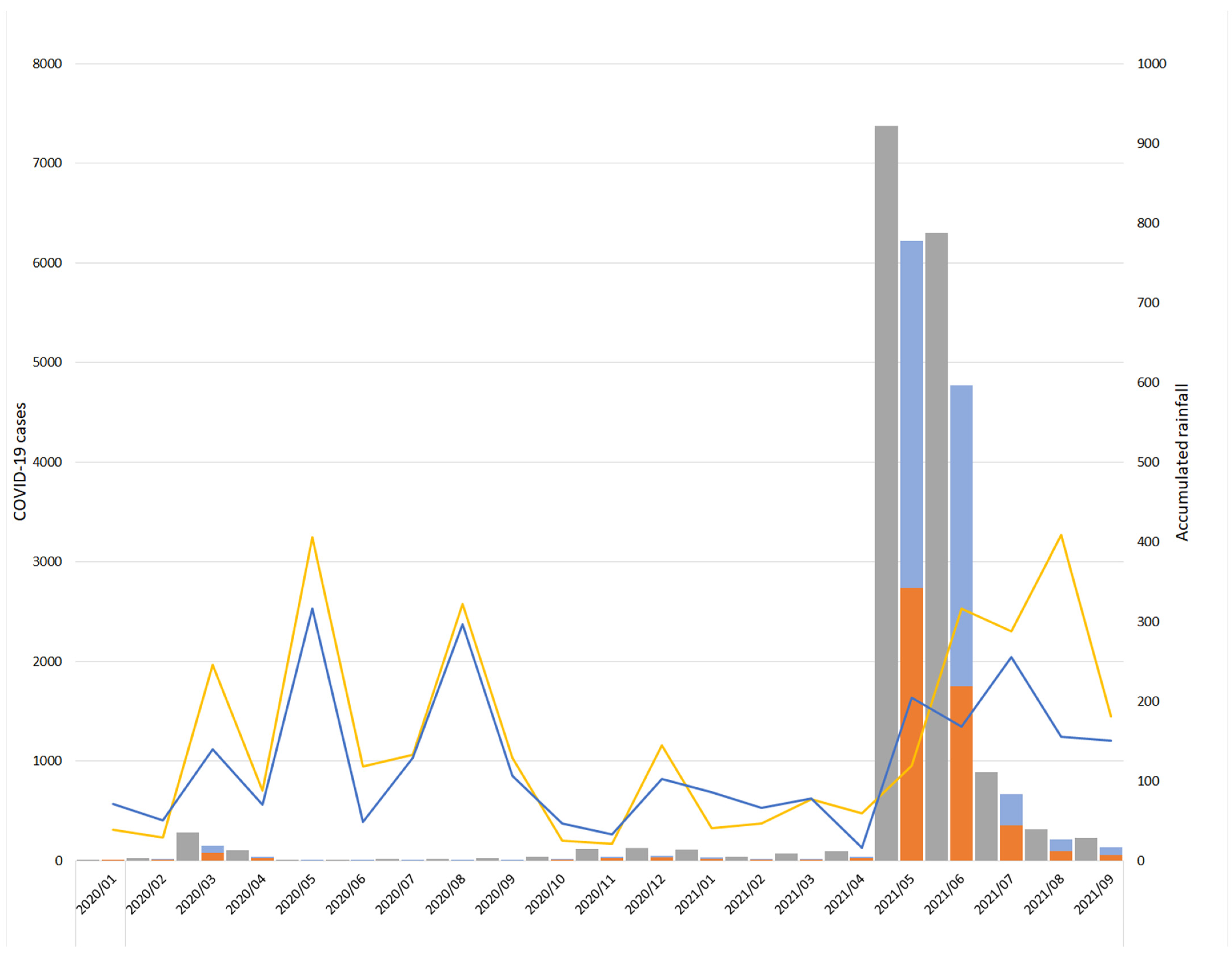
3.3. The Impact of Rainfall
3.4. Environmental SARS-CoV-2 Recovery
3.5. Detection Method
4. Materials and Methods
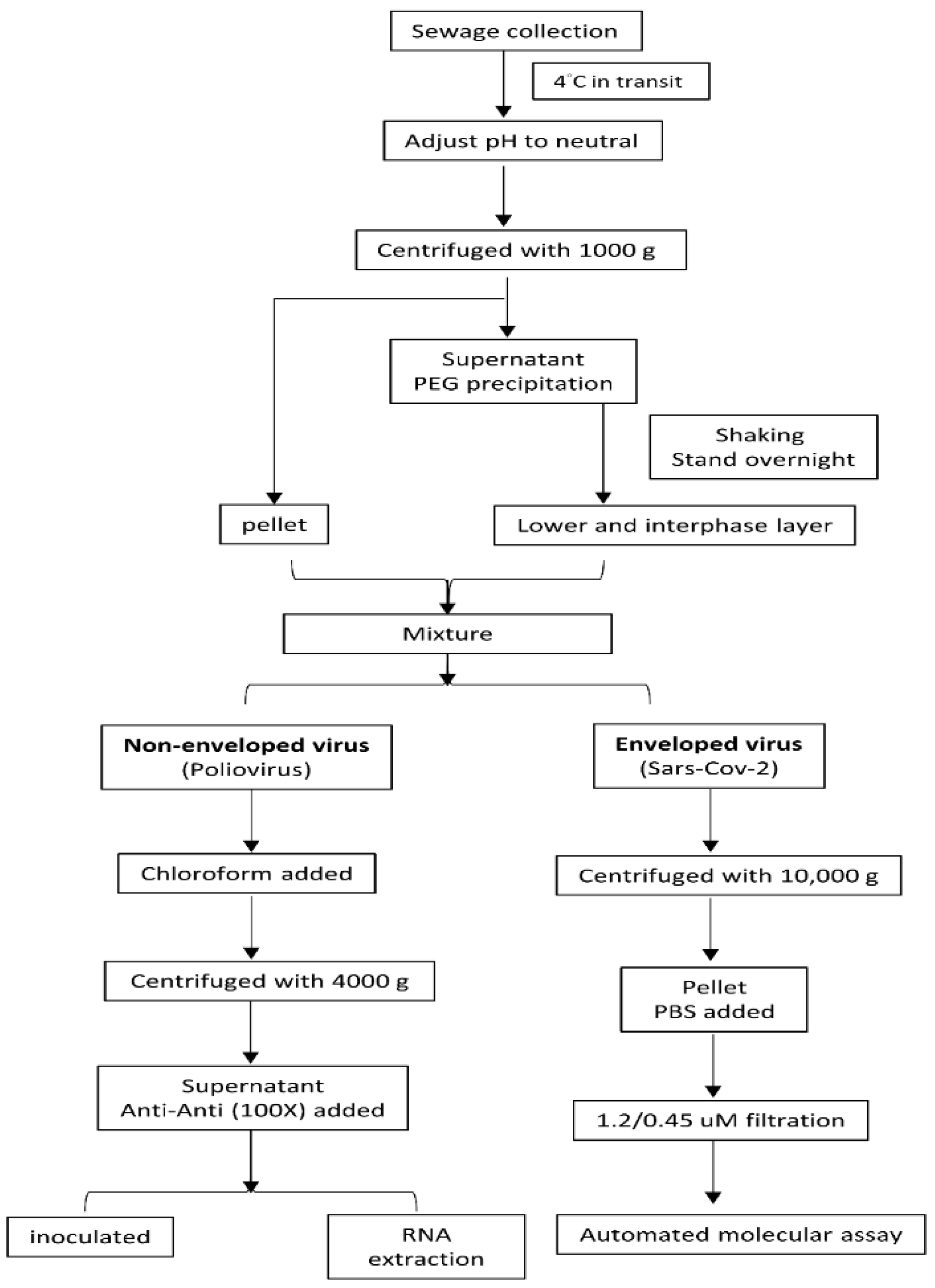
4.1. Sewage Collection
4.2. Concentration of Sewage Specimens
4.3. Routine Polio Surveillance System for Inoculation and Immunofluorescent Staining (IFA)
4.4. Routine Polio Surveillance System for RNA/DNA Extraction
4.5. Routine Polio Surveillance System for Molecular Analysis
4.6. SARS-CoV-2 Molecular Assay
4.6.1. SARS-CoV-2 In-House Real-Time PCR Assay
4.6.2. Automatic Extraction and Molecular Detection Assay for SARS-CoV-2
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Taiwan Centers of Disease Control. Available online: https://sites.google.com/cdc.gov.tw/2019ncov/global (accessed on 24 September 2021).
- Adhikari, S.P.; Meng, S.; Wu, Y.J.; Mao, Y.P.; Ye, R.X.; Wang, Q.Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef] [Green Version]
- Cheng, P.K.; Wong, D.A.; Tong, L.K.; Ip, S.M.; Lo, A.C.; Lau, C.S.; Yeung, E.Y.; Lim, W.W. Viral shedding patterns of coronavirus in patients with probable severe acute respiratory syndrome. Lancet 2004, 363, 1699–1700. [Google Scholar] [CrossRef] [Green Version]
- Lin, G.T.; Zhang, Y.H.; Xiao, M.F.; Wei, Y.; Chen, J.N.; Lin, D.J.; Wang, J.C.; Lin, Q.Y.; Lei, Z.X.; Zeng, Z.Q.; et al. Epidemiological investigation of a COVID-19 family cluster outbreak transmitted by a 3-month-old infant. Health Inf. Sci. Syst. 2021, 9, 6. [Google Scholar] [CrossRef] [PubMed]
- Holm-Jacobsen, J.N.; Vonasek, J.H.; Hagstrøm, S.; Donneborg, M.L.; Sørensen, S. Prolonged rectal shedding of SARS-CoV-2 in a 22-day-old-neonate: A case report. BMC Pediatr. 2021, 21, 506. [Google Scholar] [CrossRef]
- World Health Organization; United Nations Children’s Fund (UNICEF). Water, Sanitation, Hygiene, and Waste Management for the Covid-19 Virus: Interim Guidance; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Cheung, K.S.; Hung, I.F.N.; Chan, P.P.Y.; Lung, K.C.; Tso, E.; Liu, R.; Ng, Y.Y.; Chu, M.Y.; Chung, T.W.H.; Tam, A.R.; et al. Gastrointestinal manifestations of SARS-CoV-2 infection and virus load in fecal samples from a Hong Kong cohort: Systematic review and meta-analysis. Gastroenterology 2020, 159, 81–95. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, L.; Deng, Q.; Zhang, G.; Wu, K.; Ni, L.; Yang, Y.; Liu, B.; Wang, W.; Wei, C.; et al. The presence of SARS-CoV-2 RNA in the feces of COVID-19 patients. J. Med. Virol. 2020, 92, 833–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, I.L.; Lio, C.F.; Cheong, H.H.; Lei, C.I.; Cheong, T.H.; Zhong, X.; Tian, Y.; Sin, N.N. Evaluation of SARS-CoV-2 RNA shedding in clinical specimens and clinical characteristics of 10 patients with COVID-19 in Macau. Int. J. Biol. Sci. 2020, 16, 1698–1707. [Google Scholar] [CrossRef] [Green Version]
- Han, M.S.; Seong, M.W.; Heo, E.Y.; Park, J.H.; Kim, N.; Shin, S.; Cho, S.I.; Park, S.S.; Choi, E.H. Sequential analysis of viral load in a neonate and her mother infected with severe acute respiratory syndrome coronavirus 2. Clin. Infect. Dis. 2020, 71, 2236–2239. [Google Scholar] [CrossRef] [Green Version]
- Lescure, F.X.; Bouadma, L.; Nguyen, D.; Parisey, M.; Wicky, P.H.; Behillil, S.; Gaymard, A.; Bouscambert-Duchamp, M.; Donati, F.; Le Hingrat, Q.; et al. Clinical and virological data of the first cases of COVID-19 in Europe: A case series. Lancet Infect. Dis. 2020, 20, 697–706. [Google Scholar] [CrossRef] [Green Version]
- Chin, A.W.H.; Chu, J.T.S.; Perera, M.R.A.; Hui, K.P.Y.; Yen, H.L.; Chan, M.C.W.; Peiris, M.; Poon, L.L.M. Stability of SARS-CoV-2 in different environmental conditions. Lancet Microbe 2020, 1, e10. [Google Scholar] [CrossRef]
- Lim, M.C.; Wang, Y.F.; Huang, S.W.; Yang, J.Y.; Wang, J.R. High incidence of mammalian orthoreovirus identified by environmental surveillance in Taiwan. PLoS ONE 2015, 10, e0142745. [Google Scholar] [CrossRef]
- Hovi, T.; Shulman, L.M.; van der Avoort, H.; Deshpande, J.; Roivainen, M.; EM, D.E.G. Role of environmental poliovirus surveillance in global polio eradication and beyond. Epidemiol. Infect. 2012, 140, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.C.; Chiang, P.H.; Liao, Y.H.; Huang, L.C.; Hsieh, Y.J.; Chiu, C.M.; Lo, Y.C.; Yang, C.H.; Yang, J.Y. Outbreak of hepatitis A virus infection in Taiwan, June 2015 to September 2017. Eurosurveillance 2019, 24, 1800133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.; Gwee, S.X.W.; Ng, J.Q.X.; Lau, N.; Koh, J.; Pang, J. Wastewater surveillance to infer COVID-19 transmission: A systematic review. Sci. Total Environ. 2022, 804, 150060. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for Environmental Surveillance of Poliovirus Circulation; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- World Health Organization. Global Antimicrobial Resistance Surveillance System (GLASS). Available online: https://www.who.int/initiatives/glass (accessed on 2 September 2021).
- Medema, G.; Heijnen, L.; Elsinga, G.; Italiaander, R.; Brouwer, A. Presence of SARS-coronavirus-2 RNA in sewage and correlation with reported COVID-19 prevalence in the early stage of the epidemic in The Netherlands. Environ. Sci. Technol. Lett. 2020, 7, 511–516. [Google Scholar] [CrossRef]
- Ahmed, W.; Bertsch, P.M.; Bivins, A.; Bibby, K.; Farkas, K.; Gathercole, A.; Haramoto, E.; Gyawali, P.; Korajkic, A.; McMinn, B.R.; et al. Comparison of virus concentration methods for the RT-qPCR-based recovery of murine hepatitis virus, a surrogate for SARS-CoV-2 from untreated wastewater. Sci. Total Environ. 2020, 739, 139960. [Google Scholar] [CrossRef]
- Matsuura, K.; Ishikura, M.; Nakayama, T.; Hasegawa, S.; Morita, O.; Katori, K.; Uetake, H. Ecological studies on reovirus pollution of rivers in Toyama Prefecture. II. Molecular epidemiological study of reoviruses isolated from river water. Microbiol. Immunol. 1993, 37, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Dahling, D.R.; Safferman, R.S.; Wright, B.A. Isolation of enterovirus and reovirus from sewage and treated effluents in selected Puerto Rican communities. Appl. Environ. Microbiol. 1989, 55, 503–506. [Google Scholar] [CrossRef] [Green Version]
- Sharif, S.; Ikram, A.; Khurshid, A.; Salman, M.; Mehmood, N.; Arshad, Y.; Ahmed, J.; Safdar, R.M.; Rehman, L.; Mujtaba, G.; et al. Detection of SARs-CoV-2 in wastewater using the existing environmental surveillance network: A potential supplementary system for monitoring COVID-19 transmission. PLoS ONE 2021, 16, e0249568. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, G.; Iaconelli, M.; Mancini, P.; Bonanno Ferraro, G.; Veneri, C.; Bonadonna, L.; Lucentini, L.; Suffredini, E. First detection of SARS-CoV-2 in untreated wastewaters in Italy. Sci. Total Environ. 2020, 736, 139652. [Google Scholar] [CrossRef] [PubMed]
- Randazzo, W.; Truchado, P.; Cuevas-Ferrando, E.; Simón, P.; Allende, A.; Sánchez, G. SARS-CoV-2 RNA in wastewater anticipated COVID-19 occurrence in a low prevalence area. Water Res. 2020, 181, 115942. [Google Scholar] [CrossRef] [PubMed]
- Dutch Water Sector. Sewer Surveillance Part of Dutch National Covid-19 Dashboard. Available online: https://www.dutchwatersector.com/news/sewer-surveillance-part-of-dutch-national-covid-19-dashboard (accessed on 23 June 2020).
- Sewage Systems Office, Public Works Department, Taipei City Government. Available online: https://www.sso.gov.taipei/News_Content.aspx?n=6696E836C64AD074&s=ED9639F27BDEDFE9 (accessed on 2 September 2021).
- Water Resources Department, New Taipei City Government. Available online: https://data.gov.tw/dataset/123054 (accessed on 2 September 2021).
- Haramoto, E.; Malla, B.; Thakali, O.; Kitajima, M. First environmental surveillance for the presence of SARS-CoV-2 RNA in wastewater and river water in Japan. Sci. Total Environ. 2020, 737, 140405. [Google Scholar] [CrossRef]
- You, H.L.; Lin, M.C.; Lee, C.H. Comparison of the Roche cobas 6800 SARS-CoV-2 test and the Taiwan CDC protocol for the molecular diagnosis of COVID-19. Biomed. J. 2021, 44, 101–104. [Google Scholar] [CrossRef]
- Chen, C.M.; Jyan, H.W.; Chien, S.C.; Jen, H.H.; Hsu, C.Y.; Lee, P.C.; Lee, C.F.; Yang, Y.T.; Chen, M.Y.; Chen, L.S.; et al. Containing COVID-19 among 627,386 persons in contact with the diamond princess cruise ship passengers who disembarked in Taiwan: Big data analytics. J. Med. Internet Res. 2020, 22, e19540. [Google Scholar] [CrossRef]
- WHO. Status of Environmental Surveillance for SARS-CoV-2 Virus: Scientific Brief; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Jones, T.H.; Johns, M.W. Improved detection of F-specific RNA coliphages in fecal material by extraction and polyethylene glycol precipitation. Appl. Environ. Microbiol. 2009, 75, 6142–6146. [Google Scholar] [CrossRef] [Green Version]
- Deboosere, N.; Horm, S.V.; Pinon, A.; Gachet, J.; Coldefy, C.; Buchy, P.; Vialette, M. Development and validation of a concentration method for the detection of influenza a viruses from large volumes of surface water. Appl. Environ. Microbiol. 2011, 77, 3802–3808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honjo, M.N.; Minamoto, T.; Matsui, K.; Uchii, K.; Yamanaka, H.; Suzuki, A.A.; Kohmatsu, Y.; Iida, T.; Kawabata, Z. Quantification of cyprinid herpesvirus 3 in environmental water by using an external standard virus. Appl. Environ. Microbiol. 2010, 76, 161–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hata, A.; Hara-Yamamura, H.; Meuchi, Y.; Imai, S.; Honda, R. Detection of SARS-CoV-2 in wastewater in Japan during a COVID-19 outbreak. Sci. Total Environ. 2021, 758, 143578. [Google Scholar] [CrossRef] [PubMed]
- Nix, W.A.; Oberste, M.S.; Pallansch, M.A. Sensitive, seminested PCR amplification of VP1 sequences for direct identification of all enterovirus serotypes from original clinical specimens. J. Clin. Microbiol. 2006, 44, 2698–2704. [Google Scholar] [CrossRef] [Green Version]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [Green Version]
- FDA. Xpert Xpress SARS-CoV-2 Instructions for Use April 2020. Available online: https://www.fda.gov/media/136314/download (accessed on 24 September 2021).




{kind=link}
{kind=link}
{kind=link}
| Year | 2020 | 2021 | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Month | Jan | Feb | Mar | Apr | May | Jun | Jul | Aug | Sep | Oct | Nov | Dec | Jan | Feb | Mar | Apr | May | Jun | Jul |
| Total specimens tested | 11 | 22 | 22 | 22 | 22 | 22 | 22 | 22 | 22 | 22 | 22 | 22 | 23 | 11 | 22 | 22 | 22 | 22 | 22 |
| Poliovirus | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| EV * | 1 | 5 | 2 | 3 | 3 | 0 | 0 | 1 | 0 | 2 | 0 | 0 | 1 | 0 | 2 | 1 | 0 | 0 | 0 |
| CVA * | 1 | 3 | 1 | 0 | 1 | 0 | 0 | 4 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| CVB * | 3 | 3 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Echo * | 0 | 2 | 2 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| HRV * | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| AdV * | 7 | 6 | 5 | 3 | 0 | 1 | 0 | 3 | 8 | 2 | 0 | 2 | 0 | 0 | 6 | 4 | 4 | 0 | 0 |
| MRV * | 10 | 18 | 19 | 8 | 6 | 17 | 19 | 17 | 12 | 16 | 5 | 7 | 13 | 9 | 9 | 11 | 14 | 10 | 16 |
| SARS-CoV-2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, W.-L.; Fann, W.-B.; Shen, R.-J.; Chu, Y.; Yang, J.-Y. Surveillance of SARS-CoV-2 in Sewage Treatment Plants between January 2020 and July 2021 in Taiwan. Pathogens 2021, 10, 1611. https://doi.org/10.3390/pathogens10121611
Huang W-L, Fann W-B, Shen R-J, Chu Y, Yang J-Y. Surveillance of SARS-CoV-2 in Sewage Treatment Plants between January 2020 and July 2021 in Taiwan. Pathogens. 2021; 10(12):1611. https://doi.org/10.3390/pathogens10121611
Chicago/Turabian StyleHuang, Wei-Lun, Wen-Bin Fann, Rong-Jun Shen, Yi Chu, and Jyh-Yuan Yang. 2021. "Surveillance of SARS-CoV-2 in Sewage Treatment Plants between January 2020 and July 2021 in Taiwan" Pathogens 10, no. 12: 1611. https://doi.org/10.3390/pathogens10121611