
Direct Viral RNA Detection of SARS-CoV-2 and DENV in Inactivated Samples by Real-Time RT-qPCR: Implications for Diagnosis in Resource Limited Settings with Flavivirus Co-Circulation

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Cell Lines
2.3. Viruses
2.4. DENV-2 Serum Samples and COVID-19 Nasopharyngeal Swab Samples
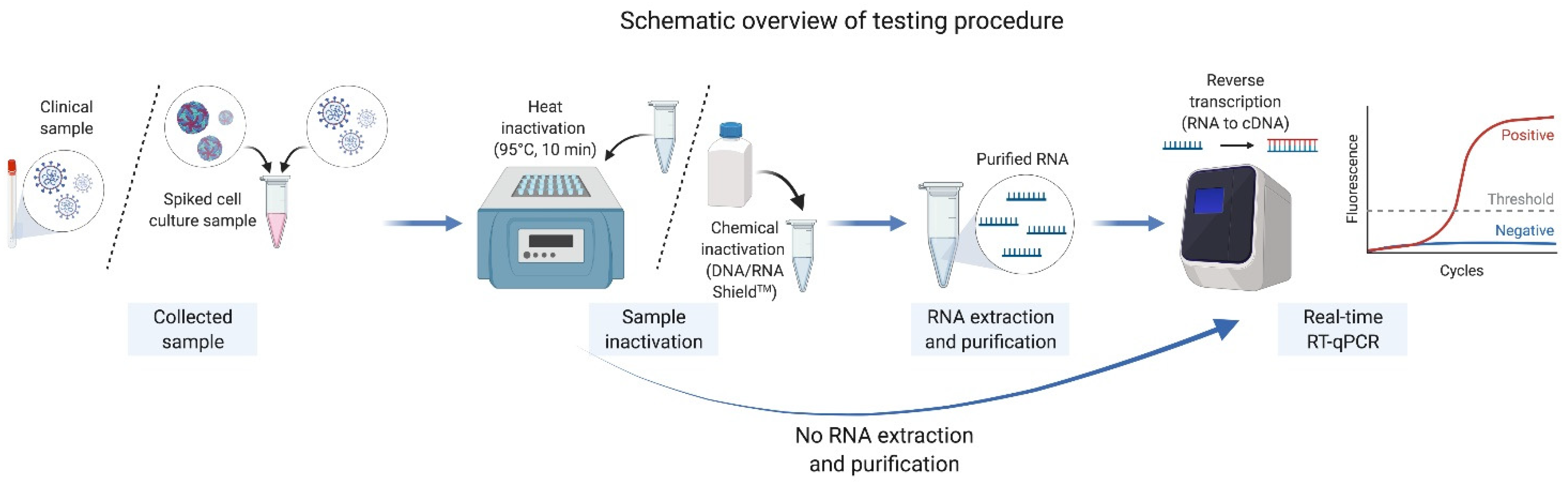
2.5. Inactivation of Viruses in Cell Cultures and Clinical Samples
2.6. Viral RNA Extraction and Purification
2.7. Quantification of DENV-2 and SARS-CoV-2 Viral RNA by Real-Time RT-qPCR
2.8. Statistical Analysis
3. Results
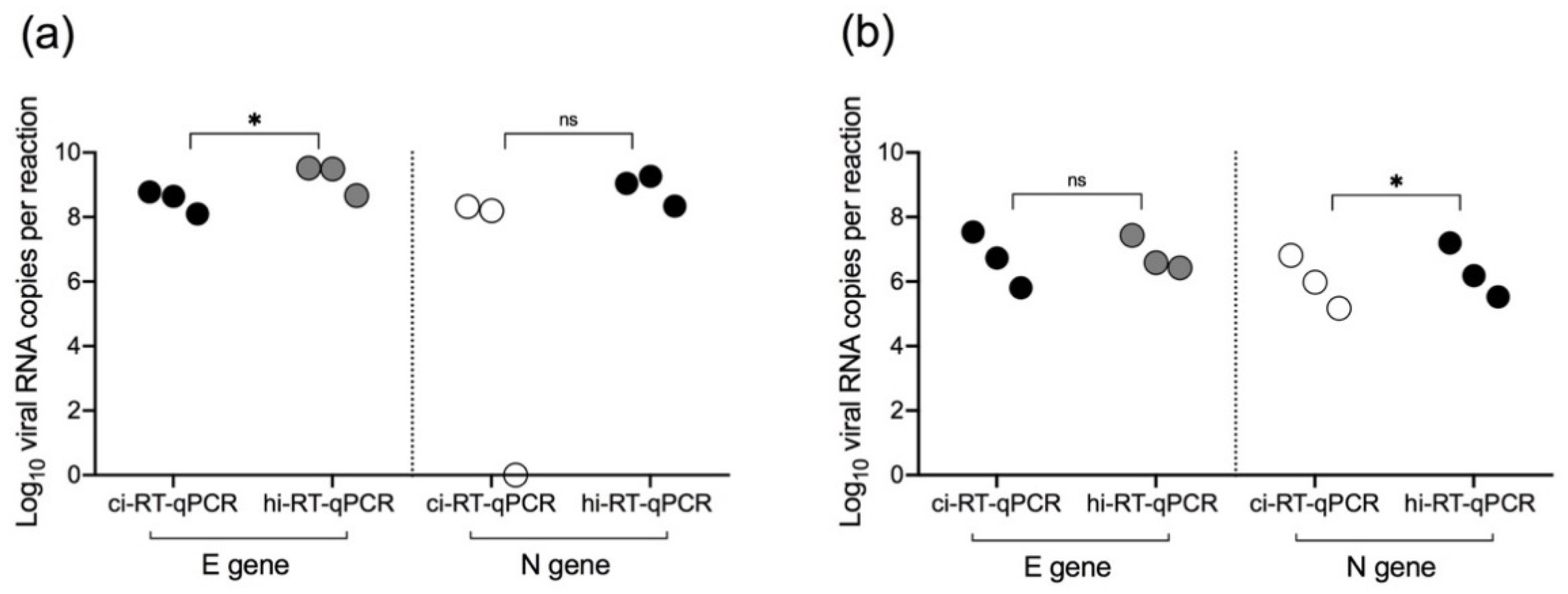
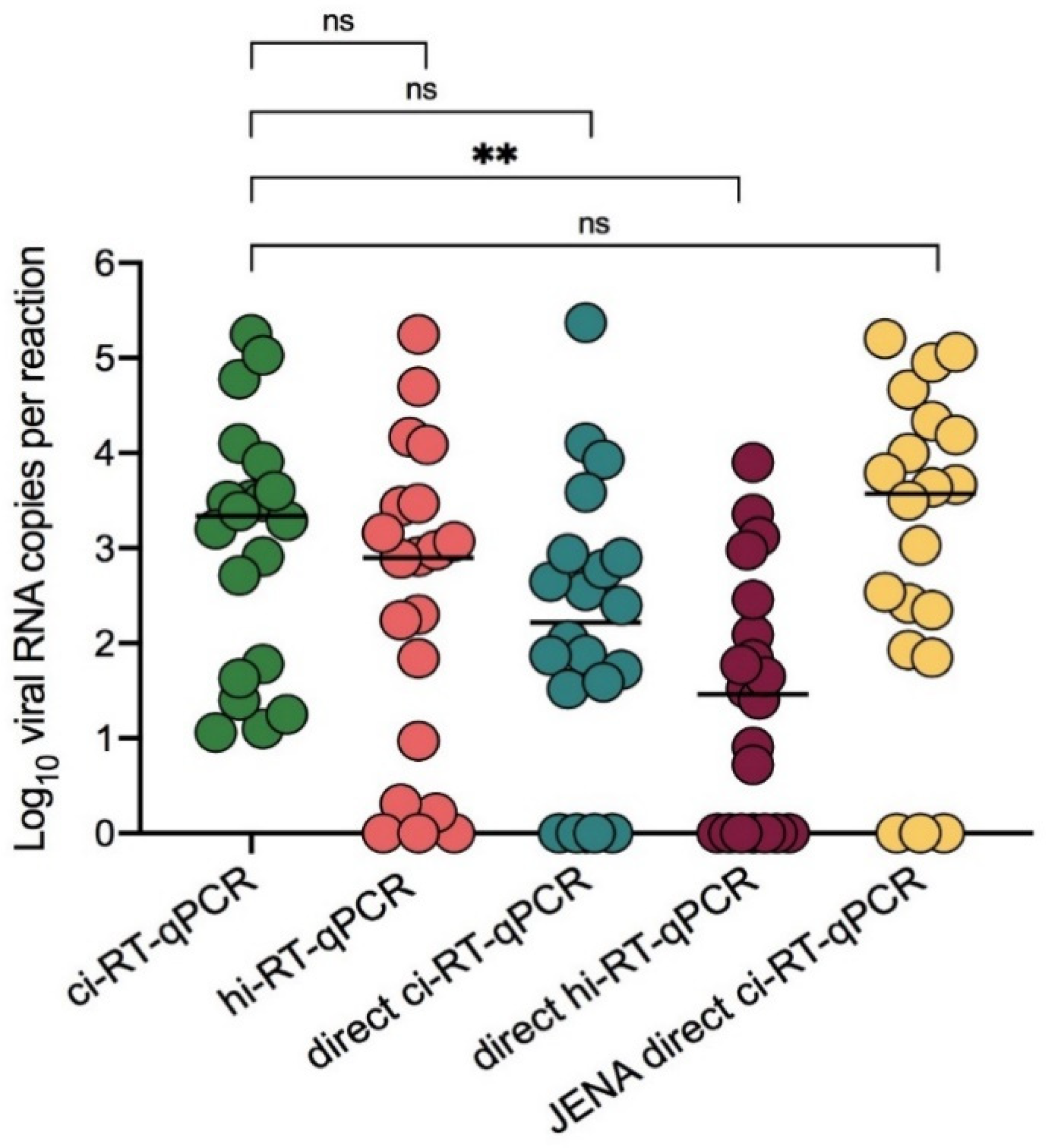
3.1. Comparison of Chemical Inactivation and Heat Inactivation Real-Time RT-qPCR on COVID-19 Clinical Samples
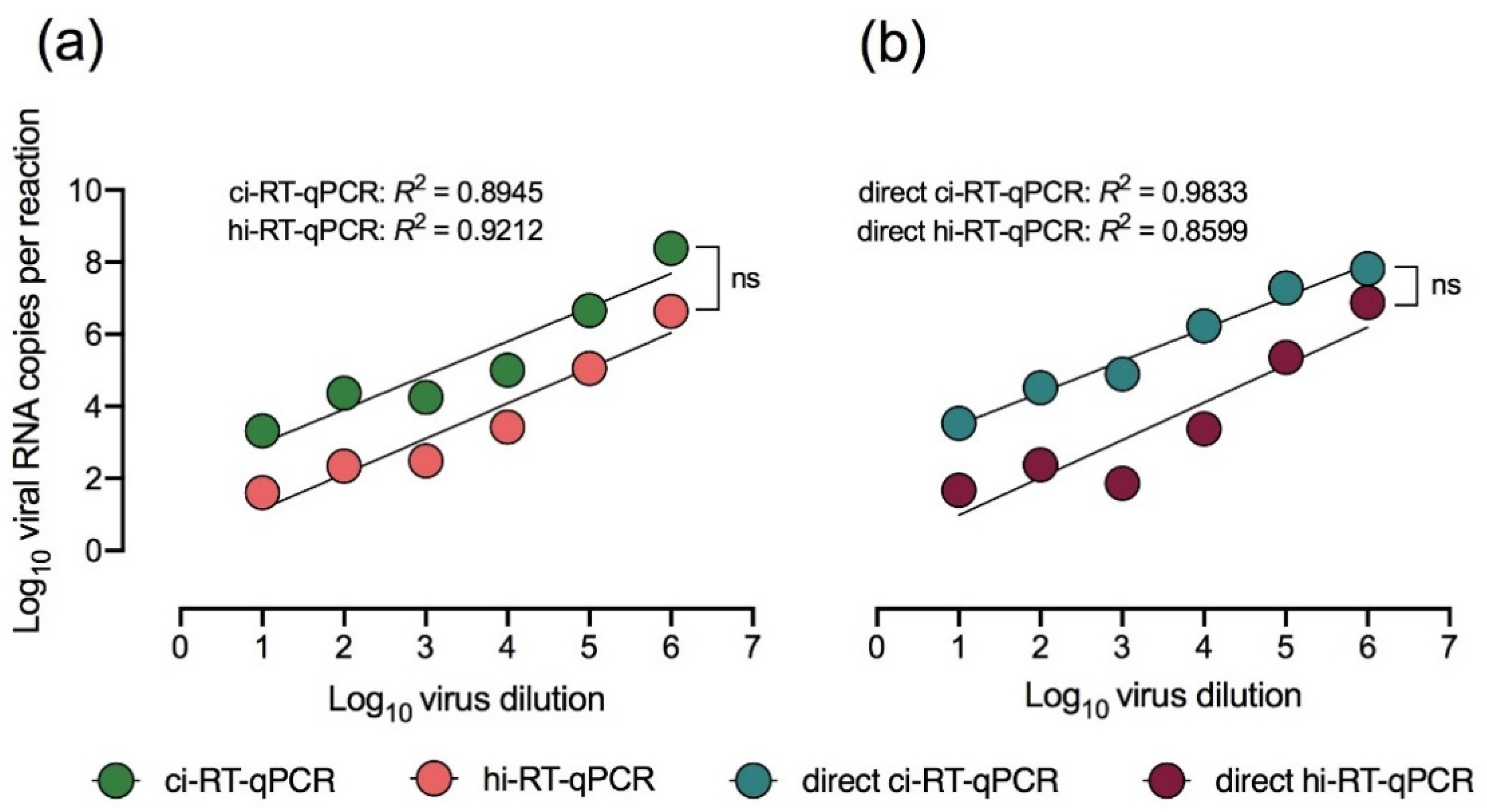
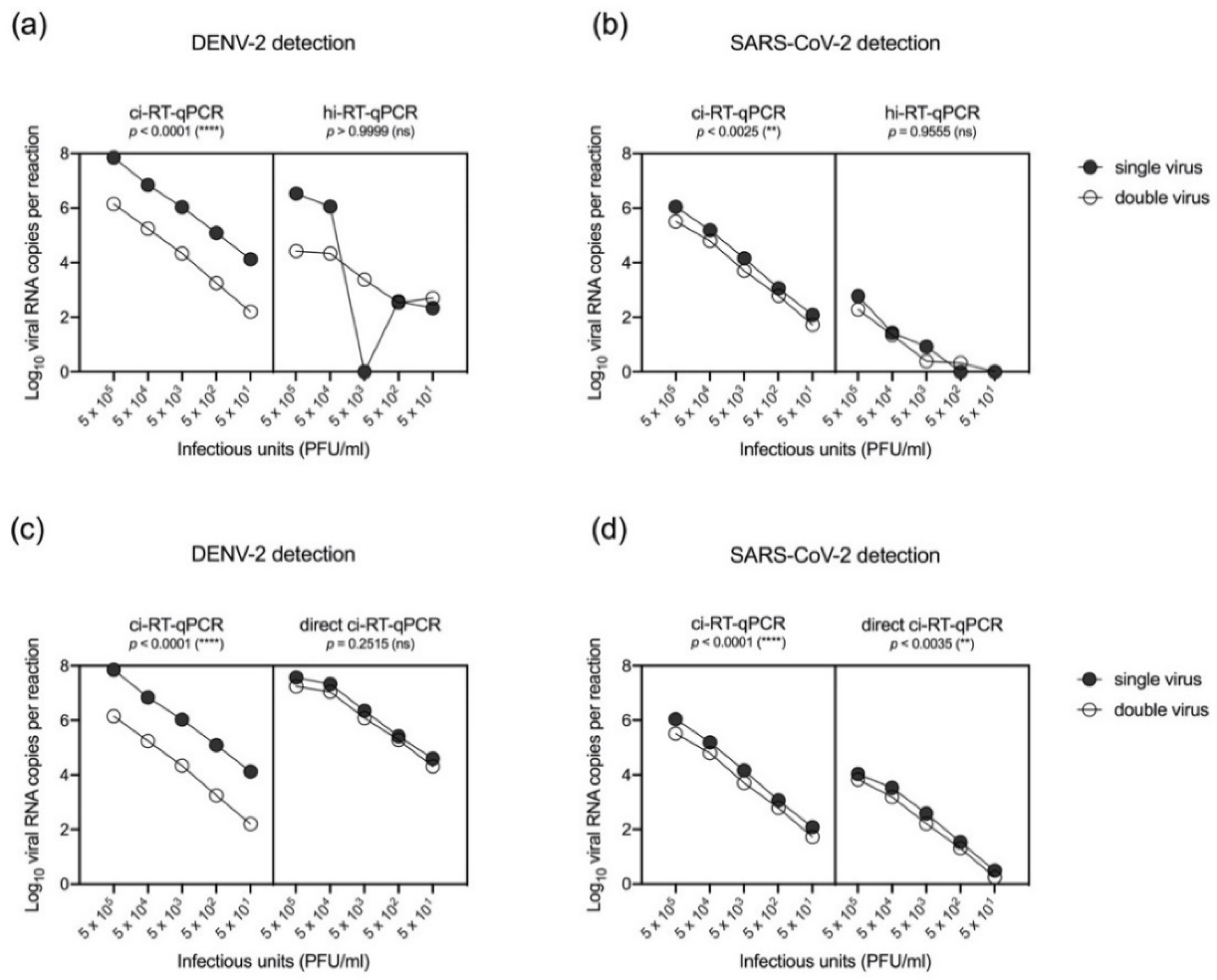
3.2. Chemical and Heat Inactivation and Direct Real-Time RT-qPCR of Cell Culture-Propagated DENV-2
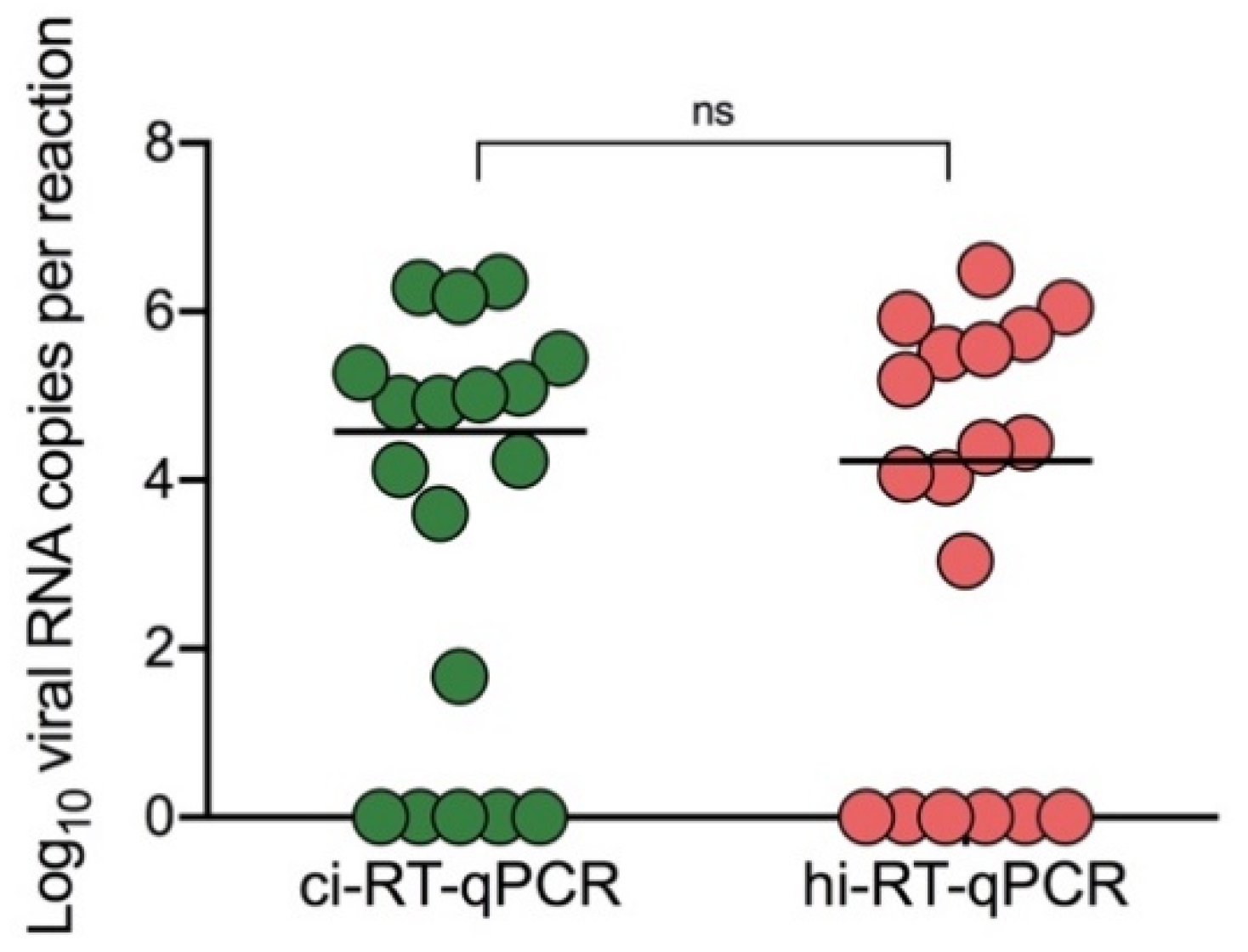
3.3. Heat Inactivation and Direct Real-Time RT-qPCR of DENV-2 Clinical Samples
3.4. Differential Detection of Chemical-Inactivated SARS-CoV-2 and DENV-2 in Spiked Samples by Real-Time RT-qPCR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Borges do Nascimento, I.J.; Cacic, N.; Abdulazeem, H.M.; von Groote, T.C.; Jayarajah, U.; Weerasekara, I.; Marcolino, M.S. Novel Coronavirus Infection (COVID-19) in Humans: A Scoping Review and Meta-Analysis. J. Clin. Med. 2020, 9, 941. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Plebani, M.; Henry, B.M. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A meta-analysis. Clin. Chim. Acta 2020, 506, 145–148. [Google Scholar] [CrossRef]
- da Silva, S.J.R.; de Magalhães, J.J.F.; Pena, L. Simultaneous Circulation of DENV, CHIKV, ZIKV and SARS-CoV-2 in Brazil: An Inconvenient Truth. One Health 2021, 12, 100205. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Zhong, N.S. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef]
- Gregory, C.J.; Santiago, L.M.; Arguello, D.F.; Hunsperger, E.; Tomashek, K.M. Clinical and laboratory features that differentiate dengue from other febrile illnesses in an endemic area–Puerto Rico, 2007–2008. Am. J. Trop. Med. Hyg. 2010, 82, 922–929. [Google Scholar] [CrossRef]
- Malavige, G.N.; Velathanthiri, V.G.N.S.; Wijewickrama, E.S.; Fernando, S.; Jayaratne, S.D.; Aaskov, J.; Seneviratne, S.L. Patterns of disease among adults hospitalized with dengue infections. J. Assoc. Physicians 2006, 99, 299–305. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Dengue Guidelines for Diagnosis, Treatment, Prevention and Control, 2009; World Health Organization: Geneva, Switzerland, 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/44188/9789241547871_eng.pdf?sequence=1&isAllowed=y (accessed on 10 June 2021).
- Korhonen, E.M.; Huhtamo, E.; Virtala, A.-M.K.; Kantele, A.; Vapalahti, O. Approach to non-invasive sampling in dengue diagnostics: Exploring virus and NS1 antigen detection in saliva and urine of travelers with dengue. J. Clin. Virol. 2014, 61, 353–358. [Google Scholar] [CrossRef]
- Yap, G.; Sil, B.K.; Ng, L.C. Use of saliva for early dengue diagnosis. PLoS Negl. Trop. Dis. 2011, 5, e1046. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.; Han, H.; Liu, F.; Lv, Z.; Wu, K.; Liu, Y.; Zhu, C. Positive rate of RT–qPCR detection of SARS-CoV-2 infection in 4880 cases from one hospital in Wuhan, China, from Jan to Feb 2020. Clin. Chim. Acta 2020, 505, 172–175. [Google Scholar] [CrossRef]
- Wang, B.; Li, R.; Lu, Z.; Huang, Y. Does comorbidity increase the risk of patients with COVID-19: Evidence from meta-analysis. Aging 2020, 12, 6049–6057. [Google Scholar] [CrossRef]
- Ranney, M.L.; Griffeth, V.; Jha, A.K. Critical supply shortages – the need for ventilators and personal protective equipment during the COVID-19 pandemic. N. Engl. J. Med. 2020, 382, e41. [Google Scholar] [CrossRef]
- Moi, M.L.; Lim, C.K.; Kotaki, A.; Takasaki, T.; Ichiro, K. Discrepancy in dengue virus neutralizing antibody titers between plaque reduction neutralizing tests with Fcγ receptor (FcγR)-negative and FcγR-expressing BHK-21 cells. Clin. Vaccine Immunol. 2010, 17, 402–407. [Google Scholar] [CrossRef] [Green Version]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Drosten, C. Detection of 2019 novel coronavirus (2019-nCoV) by real-time, RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [Green Version]
- Ito, M.; Takasaki, T.; Yamada, K.I.; Nerome, R.; Tajima, S.; Kurane, I. Development and Evaluation of Fluorogenic TaqMan Reverse Transcriptase qPCR Assays for Detection of Dengue Virus Types 1 to 4. J. Clin. Microbiol. 2004, 42, 5935–5937. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Wu, R.; Xing, Y.; Du, Q.; Xue, Z.; Xi, Y.; Ma, C. Influence of different inactivation methods on severe acute respiratory syndrome coronavirus 2 RNA copy number. J. Clin. Microbiol. 2020, 58, e00958-20. [Google Scholar] [CrossRef]
- Zymo Research. The first 510(k)-cleared transport medium for COVID-19 testing. Irvine: Zymo Research. 2020. Available online: https://www.zymoresearch.com/pages/shield-510k (accessed on 16 June 2021).
- Pastorino, B.; Touret, F.; Gilles, M.; de Lamballerie, X.; Charrel, R.N. Heat inactivation of different types of SARS-CoV-2 samples: What protocols for biosafety, molecular detection and serological diagnostics? Viruses 2020, 12, 735. [Google Scholar] [CrossRef]
- Iglói, Z.; Leven, M.; Abdel-Karem Abou-Nouar, Z.; Weller, B.; Matheeussen, V.; Coppens, J.; Koopmans, M.; Molenkamp, R. Comparison of commercial realtime reverse transcription qPCR assays for the detection of SARS-CoV-2. J. Clin. Virol. 2020, 129, 104510. [Google Scholar] [CrossRef]
- Gambino, G.; Perrone, I.; Gribaudo, I. A Rapid and effective method for RNA extraction from different tissues of grapevine and other woody plants. Phytochem. Anal. 2008, 19, 520–525. [Google Scholar] [CrossRef]
- Sahajpal, N.S.; Mondal, A.K.; Njau, A.; Ananth, S.; Jones, K.; Ahluwalia, P.K.; Kolhe, R. Proposal of RT-qPCR–based mass population screening for severe acute respiratory syndrome coronavirus 2 (Coronavirus Disease 2019). J. Mol. Diagn. 2020, 22, 1294–1299. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Real-Time RT-qPCR Panel for Detection 2019-Novel Coronavirus; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/downloads/rt-pcr-panel-for-detection-instructions.pdf (accessed on 16 June 2021).
- Centers for Disease Control and Prevention. Information for Laboratories: 2019-nCoV. Acceptable Commercial Primers and Probes; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/index.html (accessed on 16 June 2021).
- Smyrlaki, I.; Ekman, M.; Lentini, A.; de Sousa, N.R.; Papanicolaou, N. Massive and rapid COVID-19 testing is feasible by extraction-free SARS-CoV-2 RT-PCR. Nat. Comm. 2020, 11, 4812. [Google Scholar] [CrossRef]
- Andries, A.C.; Duong, V.; Ly, S.; Cappelle, J.; Kim, K.S.; Lorn Try, P.; Buchy, P. Value of Routine Dengue Diagnostic Tests in Urine and Saliva Specimens. PLoS Negl. Trop. Dis. 2015, 9, e0004100. [Google Scholar] [CrossRef] [Green Version]
- Colonetti, T.; Rocha, B.V.; Grande, A.J.; Alexandre, M.; Dondossola, E.R.; Madeira, K.; Rosa, M.I. Accuracy of immunoglobulin M and immunoglobulin A of saliva in early diagnosis of dengue: Systematic Review and Meta-analysis. Anais da Acad. Bras. De Ciências 2018, 90, 3147–3154. [Google Scholar] [CrossRef]
- Humaidi, M.; Tien, W.P.; Yap, G.; Chua, C.R.; Ng, L.C. Non-Invasive Dengue Diagnostics—The Use of Saliva and Urine for Different Stages of the Illness. Diagnostics 2021, 11, 1345. [Google Scholar] [CrossRef]
- Mizuno, Y.; Kotaki, A.; Harada, F.; Tajima, S.; Kurane, I.; Takasaki, T. Confirmation of dengue virus infection by detection of dengue virus type 1 genome in urine and saliva but not in plasma. Trans. R. Soc. Trop. Med. Hyg. 2007, 101, 738–739. [Google Scholar] [CrossRef]
- Poloni, T.R.; Dornas, F.P.; dos Santos, N.N., Jr.; Soares, A.M.; Amarilla, A.A.; Alfonso, H.L.; Aquino, V.H. High prevalence of clinically unsuspected dengue disease among children in Ribeirao Preto city, Brazil. J. Med. Virol. 2016, 88, 1711–1719. [Google Scholar] [CrossRef]
- López-Martínez, B.; Guzmán-Ortiz, A.L.; Nevárez-Ramírez, A.J.; Parra-Ortega, I.; Olivar-López, V.B.; Ángeles-Floriano, T.; Quezada, H. Saliva as a promising biofluid for SARS-CoV-2 detection during the early stages of infection. Boletín Médico Del Hosp. Infant. De México 2020, 77, 228–233. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| hi-RT-qPCR | Total | |||
|---|---|---|---|---|
| Positive | Negative | |||
| ci-RT-qPCR | Positive | 12 | 1 | 13 |
| Negative | 0 | 5 | 5 | |
| Total | 12 | 6 | 18 | |
| * PPA = 92.3%; ** NPA = 100% | ||||
| hi-RT-qPCR | cid-RT-qPCR | hid-RT-qPCR | JENA cid-RT-qPCR | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| + | − | Total | + | − | Total | + | − | Total | + | − | Total | ||
| ci-RT-qPCR | + | 18 | 2 | 20 | 16 | 4 | 20 | 15 | 5 | 20 | 17 | 3 | 20 |
| − | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Total | 18 | 2 | 20 | 16 | 4 | 20 | 15 | 5 | 20 | 17 | 3 | 20 | |
| * PPA = 90% | PPA = 80% | PPA = 75% | PPA = 85% | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mao, Z.Q.; Fukuta, M.; Balingit, J.C.; Nguyen, T.T.N.; Nguyen, C.T.; Inoue, S.; Nguyen, T.T.T.; Nguyen, L.K.H.; Minakawa, N.; Morita, K.; et al. Direct Viral RNA Detection of SARS-CoV-2 and DENV in Inactivated Samples by Real-Time RT-qPCR: Implications for Diagnosis in Resource Limited Settings with Flavivirus Co-Circulation. Pathogens 2021, 10, 1558. https://doi.org/10.3390/pathogens10121558
Mao ZQ, Fukuta M, Balingit JC, Nguyen TTN, Nguyen CT, Inoue S, Nguyen TTT, Nguyen LKH, Minakawa N, Morita K, et al. Direct Viral RNA Detection of SARS-CoV-2 and DENV in Inactivated Samples by Real-Time RT-qPCR: Implications for Diagnosis in Resource Limited Settings with Flavivirus Co-Circulation. Pathogens. 2021; 10(12):1558. https://doi.org/10.3390/pathogens10121558
Chicago/Turabian StyleMao, Zhan Qiu, Mizuki Fukuta, Jean Claude Balingit, Thi Thanh Ngan Nguyen, Co Thach Nguyen, Shingo Inoue, Thi Thu Thuy Nguyen, Le Khanh Hang Nguyen, Noboru Minakawa, Kouichi Morita, and et al. 2021. "Direct Viral RNA Detection of SARS-CoV-2 and DENV in Inactivated Samples by Real-Time RT-qPCR: Implications for Diagnosis in Resource Limited Settings with Flavivirus Co-Circulation" Pathogens 10, no. 12: 1558. https://doi.org/10.3390/pathogens10121558