
Bacteria Patterns on Tonsillar Surface and Tonsillar Core Tissue among Patients Scheduled for Tonsillectomy at Bugando Medical Centre, Mwanza, Tanzania


 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Culture Results Per Recurrence Status
2.2. Culture and Susceptibility Patterns of Bacteria from the Tonsillar Core and Surface
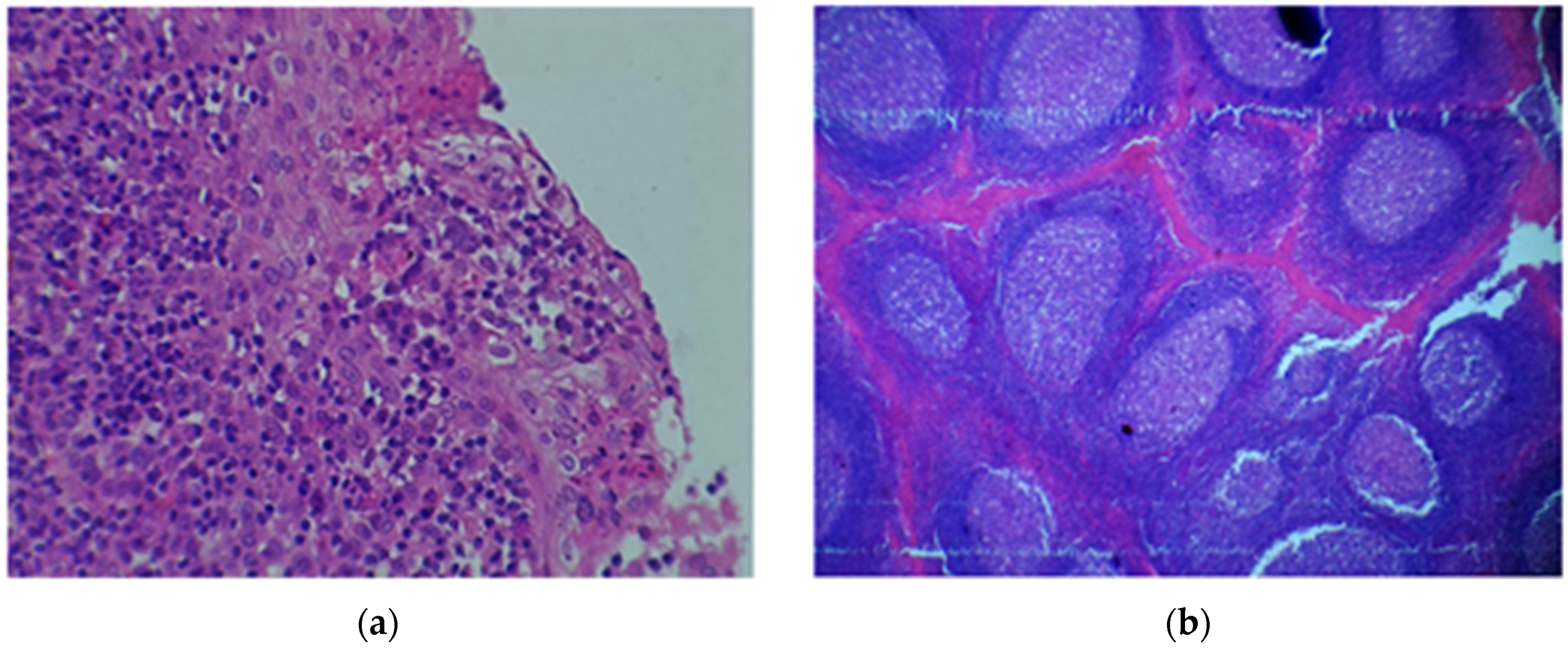
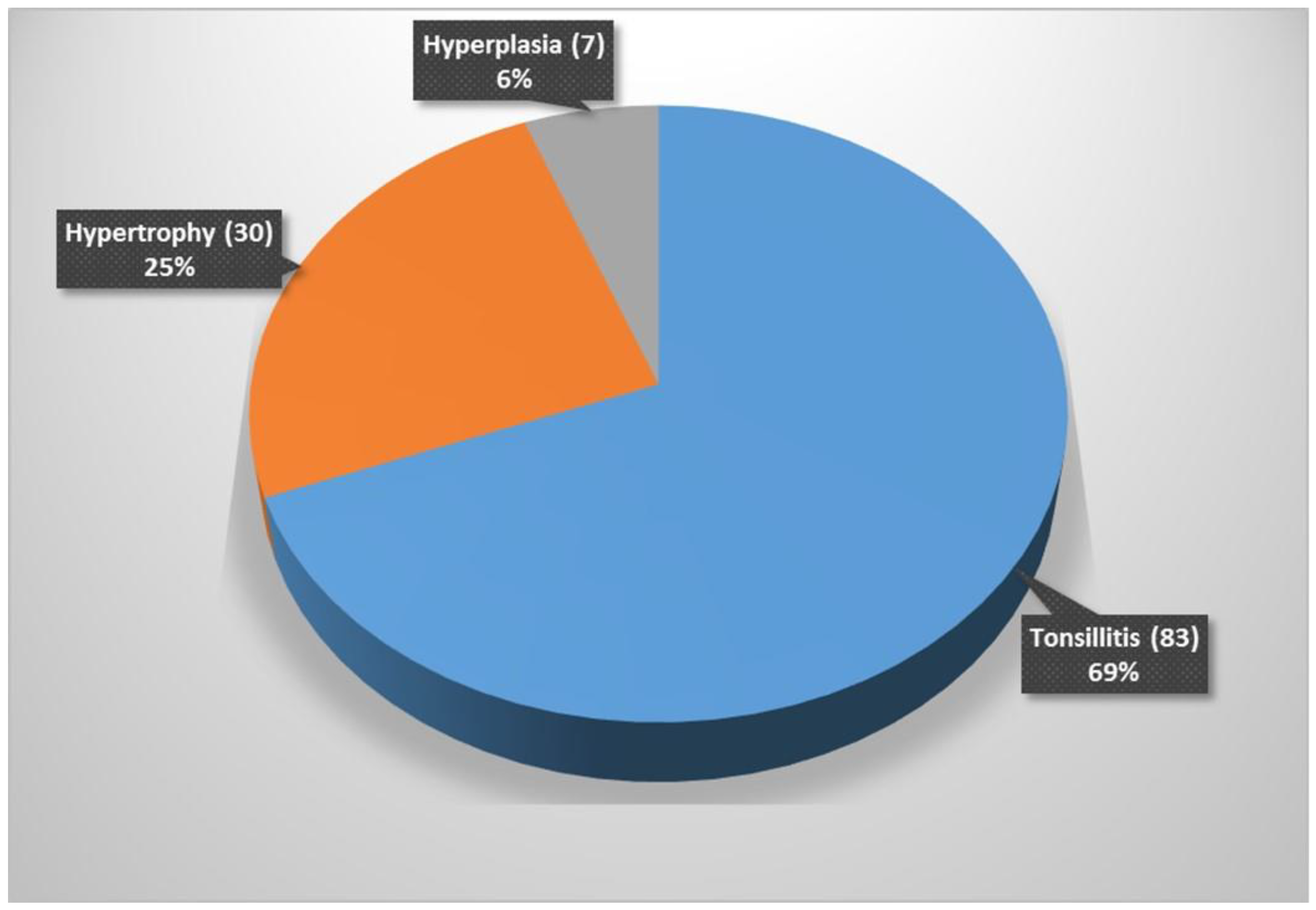
2.3. Histology Results
3. Discussion
4. Limitations
5. Conclusions and Recommendations
6. Methodology
6.1. Sample Collection and Processing
6.2. Histological Analysis
6.3. Data Analysis
6.4. Ethical Considerations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ingram, D.G.; Friedman, N.R. Toward adenotonsillectomy in children: A review for the general pediatrician. JAMA Pediatr. 2015, 169, 1155–1161. [Google Scholar] [CrossRef]
- Gul, M.; Okur, E.; Ciragil, P.; Yildirim, I.; Aral, M.; Kilic, M.A. The comparison of tonsillar surface and core cultures in recurrent tonsillitis. Am. J. Otolaryngol. 2007, 28, 173–176. [Google Scholar] [CrossRef]
- Yousef, R.Y.; Yousef, R.Y. Comparison of the bacteriology of tonsil surface and core in bacterial profile isolated from children with chronic tonsillitis. Med. J. Babylon 2010, 7, 52–57. [Google Scholar]
- Oburra, H.O.; Idenya, M. Frequency of adenotonsillectomy in some Nairobi hospitals. East Afr. Med. J. 2001, 78, 338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrawal, A.; Kumar, D.; Goyal, A.; Gupta, R.; Bhooshan, S. Bacteriological Evaluation and Their Antibiotic Sensitivity Pattern in Tonsillitis. IOSR J. Dent. Med. Sci. 2014, 13, 51–55. [Google Scholar] [CrossRef]
- Bista, M.; Sinha, B.; Amatya, R.; Tuladhar, N.; Pokharel, B. Comparison of core and surface cultures in recurrent tonsillitis. J. Inst. Med. 2007, 27, 60–65. [Google Scholar] [CrossRef]
- Brook, I.; Yocum, P.; Shah, K. Surface vs. core-tonsillar aerobic and anaerobic flora in recurrent tonsillitis. JAMA 1980, 244, 1696–1698. [Google Scholar] [CrossRef]
- Kumai, A.; Gupta, V.; Chandra, K.; Gupta, P.; Varshney, S. Clinico bacteriological evaluation of surface and core microflora in chronic tonsillitis. Indian J. Otolaryngol. Head Neck Surg. 2005, 57, 118–120. [Google Scholar] [CrossRef] [PubMed]
- Kurien, M.; Sheelan, S.; Jeyaseelan, L.; Thomas, K. Fine needle aspiration in chronic tonsillitis: Reliable and valid diagnostic test. J. Laryngol. Otol. 2003, 117, 973–975. [Google Scholar] [CrossRef] [PubMed]
- Loganathan, A.; Arumainathan, U.D.; Raman, R. Comparative study of bacteriology in recurrent tonsillitis among children and adults. Singap. Med. J. 2006, 47, 271–275. [Google Scholar]
- Kardooni, M.; Mosavian, S.M.; Lotfinia, M.; Eghbalnejad, A.M.; Mofrad, M.S.; Saki, N.; Abshirini, H. Study of common bacterial agents and antibiotic susceptibility in patients with chronic and repeated tonsillitis. J. Adv. Pharm. Educ. Res. 2020, 10, 90–95. [Google Scholar]
- Hadi, U.; El-Hajj, M.; Uwaydah, M.; Fuleihan, N.; Matar, G.M. Characteristics of pathogens recovered from the tonsils and adenoids in a group of Lebanese children undergoing tonsillectomy and adenoidectomy. J. Appl. Res. Clin. Exp. Ther. 2005, 5, 473. [Google Scholar]
- Moyo, S.J.; Steinbakk, M.; Aboud, S.; Mkopi, N.; Kasubi, M.; Blomberg, B.; Manji, K.; Lyamuya, E.F.; Maselle, S.Y.; Langeland, N. Penicillin resistance and serotype distribution of Streptococcus pneumoniae in nasopharyngeal carrier children under 5 years of age in Dar es Salaam, Tanzania. J. Med. Microbiol. 2012, 61, 952–959. [Google Scholar] [CrossRef]
- Emgård, M.; Msuya, S.E.; Nyombi, B.M.; Mosha, D.; Gonzales-Siles, L.; Nordén, R.; Geravandi, S.; Mosha, V.; Blomqvist, J.; Franzén, S.; et al. Carriage of penicillin-non-susceptible pneumococci among children in northern Tanzania in the 13-valent pneumococcal vaccine era. Int. J. Infect. Dis. 2019, 81, 156–166. [Google Scholar] [CrossRef] [Green Version]
- Mboya, E.A.; Sanga, L.A.; Ngocho, J.S. Irrational use of antibiotics in the Moshi Municipality Northern Tanzania: A cross sectional study. Pan Afr. Med. J. 2018, 31, 165. [Google Scholar] [CrossRef] [PubMed]
- Vijayashree, M.; Viswanatha, B.; Sambamurthy, B. Clinical and Bacteriological Study of Acute Tonsillitis. IOSR J. Dent. Med. Sci. 2014, 13, 37–43. [Google Scholar] [CrossRef]
- DeWyer, A.; Scheel, A.; Webel, A.R.; Longenecker, C.T.; Kamarembo, J.; Aliku, T.; Engel, M.E.; Bowen, A.; Bwanga, F.; Hovis, I.; et al. Prevalence of group A β-hemolytic streptococcal throat carriage and prospective pilot surveillance of streptococcal sore throat in Ugandan school children. Int. J. Infect. Dis. 2020, 93, 245–251. [Google Scholar] [CrossRef]
- Sarkar, S.; Sil, A.; Sarkar, S.; Sikder, B. A comparison of tonsillar surface swabbing, fine-needle aspiration core sampling, and dissected tonsillar core biopsy culture in children with recurrent tonsillitis. Ear Nose Throat J. 2017, 96, E29–E32. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.; Mirambo, M.M.; Mushi, M.F.; Hokororo, A.; Mshana, S.E. Bacteremia caused by multidrug-resistant bacteria among hospitalized malnourished children in Mwanza, Tanzania: A cross sectional study. BMC Res. Notes 2017, 10, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mushi, M.F.; Mwalutende, A.E.; Gilyoma, J.M.; Chalya, P.L.; Seni, J.; Mirambo, M.M.; Mshana, S.E. Predictors of disease complications and treatment outcome among patients with chronic suppurative otitis media attending a tertiary hospital, Mwanza Tanzania. BMC Ear, Nose Throat Disord. 2016, 16, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silago, V.; Mushi, M.F.; Remi, B.A.; Mwayi, A.; Swetala, S.; Mtemisika, C.I.; Mshana, S.E. Methicillin resistant Staphylococcus aureus causing osteomyelitis in a tertiary hospital, Mwanza, Tanzania. J. Orthop. Surg. Res. 2020, 15, 95–96. [Google Scholar] [CrossRef] [PubMed]
- Perry, M.; Whyte, A. Immunology of the tonsils. Immunol. Today 1998, 19, 414–421. [Google Scholar] [CrossRef]
- McKerrow, W.S. Recurrent tonsillitis. Am. Fam. Physician 2002, 66, 1735. [Google Scholar] [PubMed]
- Bauer, A.W.; Kirby, W.M.; Sherris, J.C.; Turck, M. Antibiotic susceptibility testing by a standardized single disk method. Am. J. Clin. Pathol. 1966, 45, 493–496. [Google Scholar] [CrossRef]
- Clinical Lab Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing; Clinical Lab Standards Institute: Wayne, PA, USA, 2016. [Google Scholar]
- Bieluch, V.M.; Chasin, W.D.; Martin, E.T.; Tally, F.P. Recurrent Tonsillitis: Histologic and Bacteriologic Evaluation. Ann. Otol. Rhinol. Laryngol. 1989, 98, 332–335. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Median/Frequency | * IQR/Percentage (%) |
|---|---|---|
| Age | 6 | 4–11 |
| Sex | ||
| Male | 73 | 60.8 |
| Female | 47 | 39.2 |
| Parents residence | ||
| Rural | 22 | 18.3 |
| Urban | 98 | 81.7 |
| Parents Education level | ||
| Uneducated | 3 | 2.5 |
| Primary | 19 | 15.8 |
| Secondary | 52 | 43.3 |
| University | 46 | 38.3 |
| Variable | Frequency | Percentage |
|---|---|---|
| Breathing difficulty | ||
| Yes | 114 | 95.0 |
| No | 6 | 5.0 |
| Fever | ||
| Yes | 60 | 50.0 |
| No | 60 | 50.0 |
| Tonsillitis infection history in family | ||
| Yes | 14 | 11.7 |
| No | 106 | 88.3 |
| Previous operation? | ||
| Yes | 11 | 9.2 |
| No | 109 | 90.8 |
| History of hospital admission | ||
| Yes | 31 | 25.8 |
| No | 89 | 74.2 |
| Recurrent tonsillitis | ||
| Yes | 99 | 82.5 |
| No | 21 | 17.5 |
| Dysphagia | ||
| Yes | 93 | 77.5 |
| No | 27 | 22.5 |
| Antibiotic usage in past two months | ||
| Yes | 90 | 75.0 |
| No | 30 | 25.0 |
| Antibiotic usage decision | ||
| Health care worker | 64 | 71.1 |
| Self | 26 | 28.9 |
| Health care seeking | ||
| On symptom insert | 64 | 53.3 |
| Several days post infection | 32 | 26.7 |
| After drug failure | 24 | 20.0 |
| Patients AMR * awareness | ||
| Yes | 29 | 24.2 |
| No | 91 | 75.8 |
| Bacteria Isolated (n) | E n(%) | DA n(%) | LZD n(%) | SXT n(%) | CIP n(%) | CN n(%) | AK n(%) | FOX n(%) |
|---|---|---|---|---|---|---|---|---|
| Surface | ||||||||
| S. aureus (29) | 14 (48.3) | 18 (62.1) | 4 (13.8) | 5 (17.2) | 15 (51.7) | 18 (62.1) | 23 (79.3) | 18 (62.1) |
| S. pyogenes (17) | 11 (64.7) | 12 (70.6) | 10 (58.8) | 0 (0.0) | 11 (64.7) | 14 (82.4) | 14 (82.4) | |
| S. viridans (15) | 2 (13.3) | 13 (86.7) | 14 (93.3) | 2 (13.3) | 10 (66.7) | 11 (73.3) | 12 (80) | |
| S. pneumoniae (4) | 3 (75) | 3 (75) | 3 (75) | 3 (75) | 2 (50) | 2 (50) | 2 (50) | |
| Enterococcous spp. (3) | 2 (66.7) | 2 (66.7) | 2 (66.7) | 1 (33.3) | 3 (100) | 3 (100) | 2 (66.7) | |
| Core | ||||||||
| S. aureus (22) | 9 (40.9) | 12 (54.5) | 12 (54.5) | 8 (36.4) | 13 (59.1) | 14 (63.6) | 15 (68.2) | 13 (59.1) |
| S. pyogenes (12) | 11 (91.7) | 6 (50.0) | 9 (75.0) | 0 (0.0) | 8 (66.7) | 9 (75.0) | 9 (75.0) | |
| S. viridans (6) | 3 (50.0) | 5 (83.3) | 4 (66.7) | 1 (16.7) | 2 (33.3) | 3 (50.0) | 3 (50.0) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buname, G.; Kiwale, G.A.; Mushi, M.F.; Silago, V.; Rambau, P.; Mshana, S.E. Bacteria Patterns on Tonsillar Surface and Tonsillar Core Tissue among Patients Scheduled for Tonsillectomy at Bugando Medical Centre, Mwanza, Tanzania. Pathogens 2021, 10, 1560. https://doi.org/10.3390/pathogens10121560
Buname G, Kiwale GA, Mushi MF, Silago V, Rambau P, Mshana SE. Bacteria Patterns on Tonsillar Surface and Tonsillar Core Tissue among Patients Scheduled for Tonsillectomy at Bugando Medical Centre, Mwanza, Tanzania. Pathogens. 2021; 10(12):1560. https://doi.org/10.3390/pathogens10121560
Chicago/Turabian StyleBuname, Gustave, Gapto Aristides Kiwale, Martha F. Mushi, Vitus Silago, Peter Rambau, and Stephen E. Mshana. 2021. "Bacteria Patterns on Tonsillar Surface and Tonsillar Core Tissue among Patients Scheduled for Tonsillectomy at Bugando Medical Centre, Mwanza, Tanzania" Pathogens 10, no. 12: 1560. https://doi.org/10.3390/pathogens10121560