1. Introduction
The outbreak of COVID-19 has had a direct and devastating impact on the global economy [
1] and has posed an unprecedented challenge to the medical system around the world [
2]. At the beginning of 2022, COVID-19 broke out repeatedly in various places, and Shanghai became the city with the largest population infection scale. In order to effectively control the epidemic, the Shanghai Epidemic Prevention and Control Headquarters dispatched the national emergency medical rescue team and medical teams from all over the country to Shanghai and organized the establishment of a shelter hospital [
3]. The purpose of establishing the Fangcang shelter hospital was to centralize the management of patients and prevent the spread of disease [
4]. Secondly, it is necessary to avoid some patients with basic diseases being isolated at home alone, lacking medication and professional medical facilities, thereby increasing the severity of virus infection [
5]. The Fangcang shelter hospital is a new type of public health project, which provides medical treatment, disease monitoring, food and social activities for patients with infectious diseases. It was first proposed and implemented by China in February 2020 [
6]. Due to the long-term existence and multiple variations of COVID-19, its infectivity has been greatly enhanced, the number of infected people has grown extremely fast, and the demand for Fangcang shelter hospitals has risen significantly, which has also led to the improvement and updating of the design guidelines of shelter hospitals, so as to achieve the standardization and rationalization of the design of shelter hospitals [
7]. Therefore, in order to meet the growing isolation needs of infected people, the exhibition hall, gymnasium and other large spaces have become the reconstruction objects of the Fangcang shelter hospital. COVID-19 is mainly transmitted through the respiratory tract, so it is necessary to focus on the control of infectious sources and maintain high indoor air quality. Therefore, the transformation of the ventilation system in the Fangcang shelter hospital is an extremely important part of the construction of the Fangcang shelter hospital [
8].
Shanghai is located in the eastern coastal area of China and has a subtropical monsoon climate. The precipitation in Shanghai from May to September is about 60% of the whole year, especially from July to August: it is a summer drought. The climate is humid and hot, so the requirements for the ventilation system are particularly strict. As the outbreak of the epidemic in Shanghai occurred in March, when the weather is relatively cool, so it is only necessary to meet the indoor environment requirements through mechanical ventilation and natural air supplement temporarily. However, with the increase in time, the arrival of the plum rain season and summer drought weather, the air-conditioning fresh air system must be used to ensure the comfort of indoor personnel. As for the design of the ventilation system, the Fangcang shelter of the Shanghai World Expo Hall was rebuilt in the form of a cloth bag air duct, and the temperature in the lower area is almost not stratified, and the distribution is relatively uniform [
9,
10]. The tuyere of the Beijing Capital Gymnasium combines slot tuyere and shutter tuyere, and uses valves to switch tuyeres, so as to meet various wind speed requirements [
11]. In the Tokyo Metropolitan Gymnasium, Japan, the air conditioning is divided into three areas to refine the air conditioning, which can meet the needs of the spectators and the competition site at the same time. At the same time, the side-air supply mode is used to supply air to the auditorium area, so that the temperature distribution of the auditorium is uniform [
11].
CFD technology is currently widely used in mechanical engineering, energy, and environmental fields. In the field of mechanical engineering, CFD technology can be used to simulate the flow of fluids through blades, pumps, fans, and other mechanical components, improving their performance and efficiency. Nan Wang et al. [
12] applied effective artificial intelligence algorithms to centrifugal pumps, and analyzed and optimized them through CFD to improve their performance. In the field of energy, CFD technology can be used to simulate the flow of fluids and energy conversion processes in gas turbines, turbines, generators, and other energy conversion devices. Yeop Kim et al. [
13] designed a transcritical cycle radial inflow turbine for geothermal power generation systems and evaluated the performance of the designed turbine using CFD to obtain design parameters to improve turbine efficiency. In the environmental field, CFD technology can be used to simulate the motion and distribution of fluids and pollutants in air, water, soil, and ocean environments. Bay Ezgi et al. [
14] used CFD technology to evaluate the natural ventilation strategy of historical buildings in hot and humid climates. GonKim et al. [
15] and Fathollahzadeh MH et al. [
16] used CFD technology to study the airflow organization under the floor air supply of large-space buildings, and obtained the optimal parameter scheme through the analysis of the temperature field and velocity field. Ascione Fabrizio et al. [
17] used CFD to simulate the campus of the University of Camposo in Italy, and studied the operation mode of the air-conditioning system in the safety classroom of the teaching building for disease infection and transmission. Zhao et al. [
18] used CFD to simulate the diffusion of oral droplets carrying respiratory infectious viruses under different ventilation times, and obtained that most of the droplets can be discharged under sufficient indoor ventilation, thus effectively maintaining a relatively healthy indoor air environment. It is pointed out that fresh air should be used as much as possible and the air exchange rate should be increased if conditions permit. Li et al. [
19] took a gymnasium project in Harbin as an example, and simulated the environment through CFD. The results showed that the project feasibility of transforming the existing gymnasium into a Fangcang shelter hospital provided a certain degree of theoretical support for the Fangcang shelter hospital transformation project.
The research on airflow organization in Fangcang shelter hospitals is targeted, and personnel comfort and pollutant control should be considered at the same time. At present, some scholars have designed and studied the ventilation system of the Fangcang shelter hospital, including the research on the comfortable environment of personnel, as well as the research on pollutant emission. Pradip Aryal et al. [
20] analyzed the impact of a partition wall on thermal comfort during air-conditioning operations in large-space buildings through CFD simulation. Xia et al. [
21] concluded by comparing the ventilation forms and airflow organization of different gyms that setting an exhaust under the hospital bed while supplying fresh air at the upper part can effectively avoid the intrusion and threat of viruses. Wang et al. [
22,
23] conducted a simulation study in the sickbed area of the Wuhan Dahuashan Fangcang Shelter Hospital. The phenomenon of thermal stratification and poor ventilation increased the risk of infection due to the accumulation of pollutants exhaled by patients, and baffles were used to solve the air seepage velocity near the make-up air inlet. Following China’s successful experience in building Fangcang shelter hospitals, other countries began to establish Fangcang shelter hospitals and carry out research. For example, the 627th field hospital in the United States transformed from the activity center, the Garvitz field hospital transformed from the conference center, and the Spanish Madrid shelter hospital transformed from the convention center [
24,
25,
26]. Machida et al. [
27] found in the simulation test that the diffusion of tuberculosis bacteria after using the radiation air-conditioning system will be much less than that of the convection air-conditioning system. In addition, increasing the distance between beds and heightening the isolation wall can effectively prevent cross-infection [
28]. Liu et al. [
29] found that the indoor temperature and humidity will affect the indoor propagation of droplets with different particle sizes, and the droplets are greatly affected by turbulence, and the unstable airflow will accelerate the virus transmission.
According to the existing studies, reasonable renovation of makeshift hospitals can cope with the spread of the novel coronavirus in a timely manner, but the application of CFD simulation of different ventilation design schemes on the comfort of personnel in the internal environment of makeshift hospitals and the common impact of air flow organization and pollutant transmission are still insufficient. The original ventilation design mainly aims to maintain good thermal comfort and indoor air quality for the occupants, or only consider reasonable air distribution and pollutant emission. Advanced ventilation strategies should be further developed to reduce the risk of infection, combined with thermal comfort considerations [
30,
31]. As the COVID-19 epidemic is urgent and spreading rapidly, medical resources are in short supply, and patients with mild illnesses are in the majority. Most of the Fangcang shelter hospitals have abandoned the traditional “three areas and two channels” [
32], namely: clean area, semi-polluted area, polluted area, patient channel and medical channel. The interior of the reconstructed Fangcang shelter hospital is planned as a pollution area as a whole, so it is only necessary to consider the overall negative pressure formed in the Fangcang shelter to avoid the internal airflow overflow.
Based on the above background, this paper simulated the living environment quality and pollutant emission in the Fangcang shelter hospital under different ventilation parameter schemes under hot summer conditions through CFD software, and obtains appropriate parameters to allow the Fangcang shelter hospital interior to reach a comfortable living condition. Taking the gymnasium of a university in Shanghai as an example, the second floor of the gymnasium was transformed into a temporary Fangcang shelter hospital, and the air-conditioning system used the method of bag air supply. In order to better deal with the epidemic situation that may occur in the future, combined with the case of small- and medium-sized venues rebuilding Fangcang shelter hospitals, how to better design and plan the ventilation system in consideration of the local climate was studied, and the impact of air supply parameters on the distribution of pollutants and viruses through simulation was analyzed. Finally, the appropriate ventilation system design and air supply parameters were presented. The method used in this paper has an important reference significance for the future actual construction design.
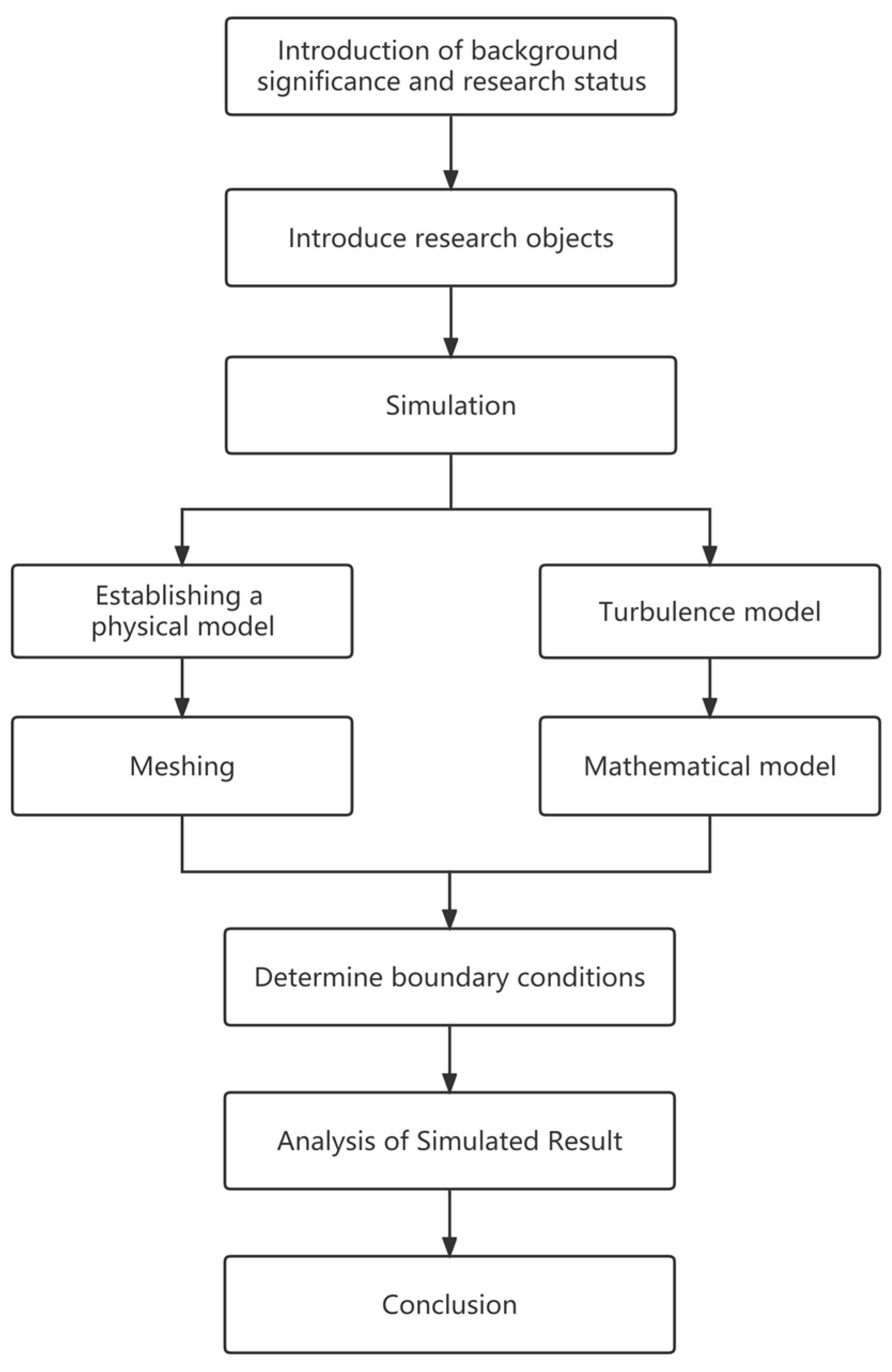
The second chapter of this article introduces the research object of the renovation, the third chapter establishes a simulation model, the fourth chapter focuses on analyzing the numerical simulation results, and finally conclusions are drawn in the fifth chapter. The flowchart of the study is shown in
Figure 1.
The main contributions of this article are as follows:
(1) In emergency situations, the traditional three-zone and two-channel renovation of the gymnasium into a shelter hospital is not considered.
(2) Comprehensively consider the impact of different parameters on airflow organization and pollutant emissions.
(3) In the case of reasonable airflow organization, it is also necessary to meet the comfort level of personnel.
2. Research Object Description
2.1. Ventilation System and Hospital Bed Layout
Under the objective condition of an extremely short construction period, what kind of fast, effective and reliable ventilation scheme should be adopted to dilute the polluted air in the area where the personnel are located and meet the requirements for the comfort of the personnel.
According to the requirements of functional departments, users and relevant specifications, the reconstruction of Fangcang shelter hospitals should achieve the following objectives:
(1) The transformed Fangcang shelter hospital can ensure the health of medical staff, staff and patients, and prevent the spread of viruses in the contaminated area to the surrounding environment; (2) as the time for transformation is very short, the transformation of ventilation and air conditioning should be based on the current situation, and the equipment and materials to be transformed should be existing; (3) the Fangcang shelter hospital can quickly and simply restore its original functions after use [
3].
Before the transformation of the university gymnasium in Shanghai, natural ventilation was used, with smoke exhaust windows on both sides, and a central air-conditioning top-air supply was used in several small rooms on the west side. As the school is located in a coastal city, the wind is strong all year round and the ventilation effect is good. In the design specifications of the ventilation system in infectious disease wards, it is usually recommended to use a fresh air system with an upper supply and lower return air [
33]. The original ventilation system failed to create an effective negative pressure in the gymnasium, and the airflow organization was unreasonable in the discharge of pollutants, which may cause cross-infection among personnel. Additionally, due to the high temperature in summer, the comfort of personnel is poor, so a new ventilation system needs to be established.
Under the special circumstances of demanding time and materials, the cloth bag air duct system that is easy to install and disassemble is adopted. This refers to a flexible air distribution system that is mainly woven by special fiber materials. It mainly adopts the air outlet mode of fiber penetration and an orifice jet, which can provide a uniform linear air supply. The cloth bag air duct air supply system has the following advantages: (1) Reduce the load on the roof. (2) Simple installation and short construction period. (3) High comfort. (4) Easy to clean. (5) Anti condensation. (6) The system has low-cost and high-cost performance.
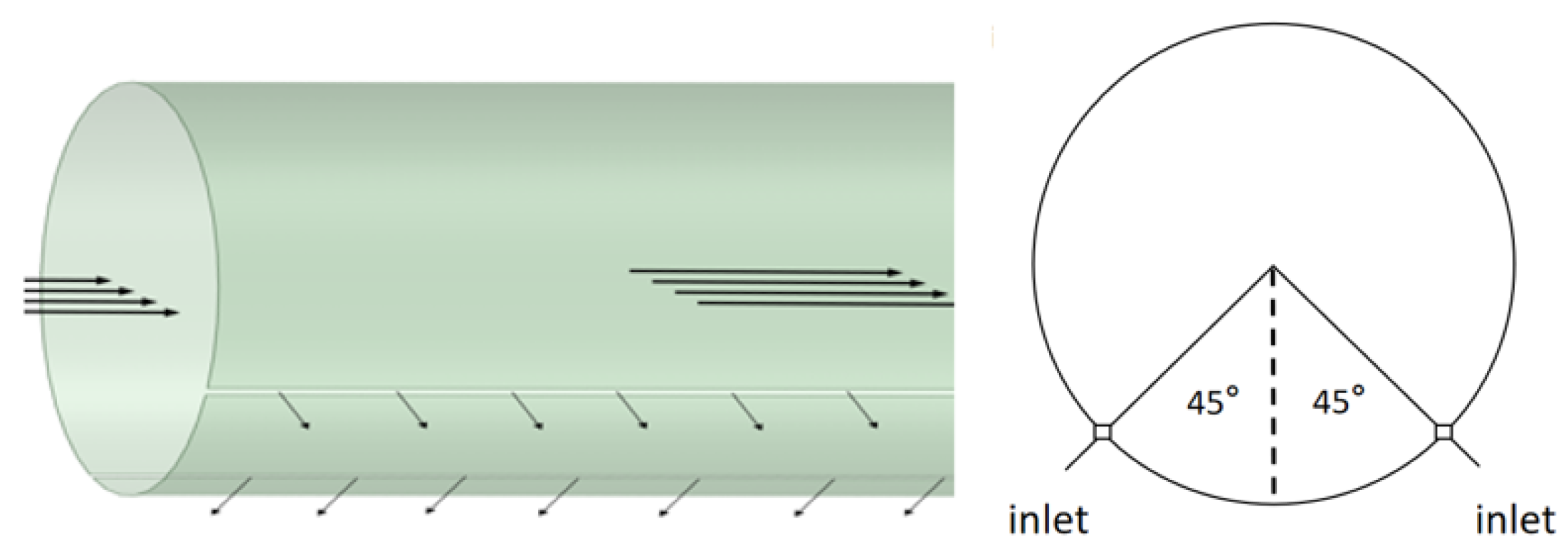
To sum up, it is proposed to use the cloth bag air duct system in the reconstruction. The west air supply system will be modified and extended into 5 longitudinal metal air ducts passing through the top center of the second floor of the gymnasium. The strips on both sides of the air ducts will supply air at a downward angle of 45°, which will be used as the fresh air inlet. Exhaust outlets will be set at the bottom of both sides, and mechanical fans will be used for auxiliary ventilation. According to the design guidelines in China for emergency medical buildings, the air outlet in the pollution area should be set as close to the pollution source as possible. Except that the patient receiving area uses the original system in a large space for ventilation, the height of the lower edge of the indoor air outlet of the new air exhaust system from the ground should not be higher than 2 m. The air exhaust volume in the patient receiving area is calculated as 150 m3/h per bed, and the air outlet is installed with an efficient filter. As the gymnasium is a lightly polluted area, the restricted area and clean area are designed outside the Fangcang shelter hospital. It is only necessary to maintain negative pressure in the shelter as a whole, to prevent polluted air in the Fangcang shelter hospital from leaking into the restricted area and clean area. Therefore, the interior layout of the entire gymnasium reconstruction shelter does not consider the traditional three-zone and two-channel renovation.
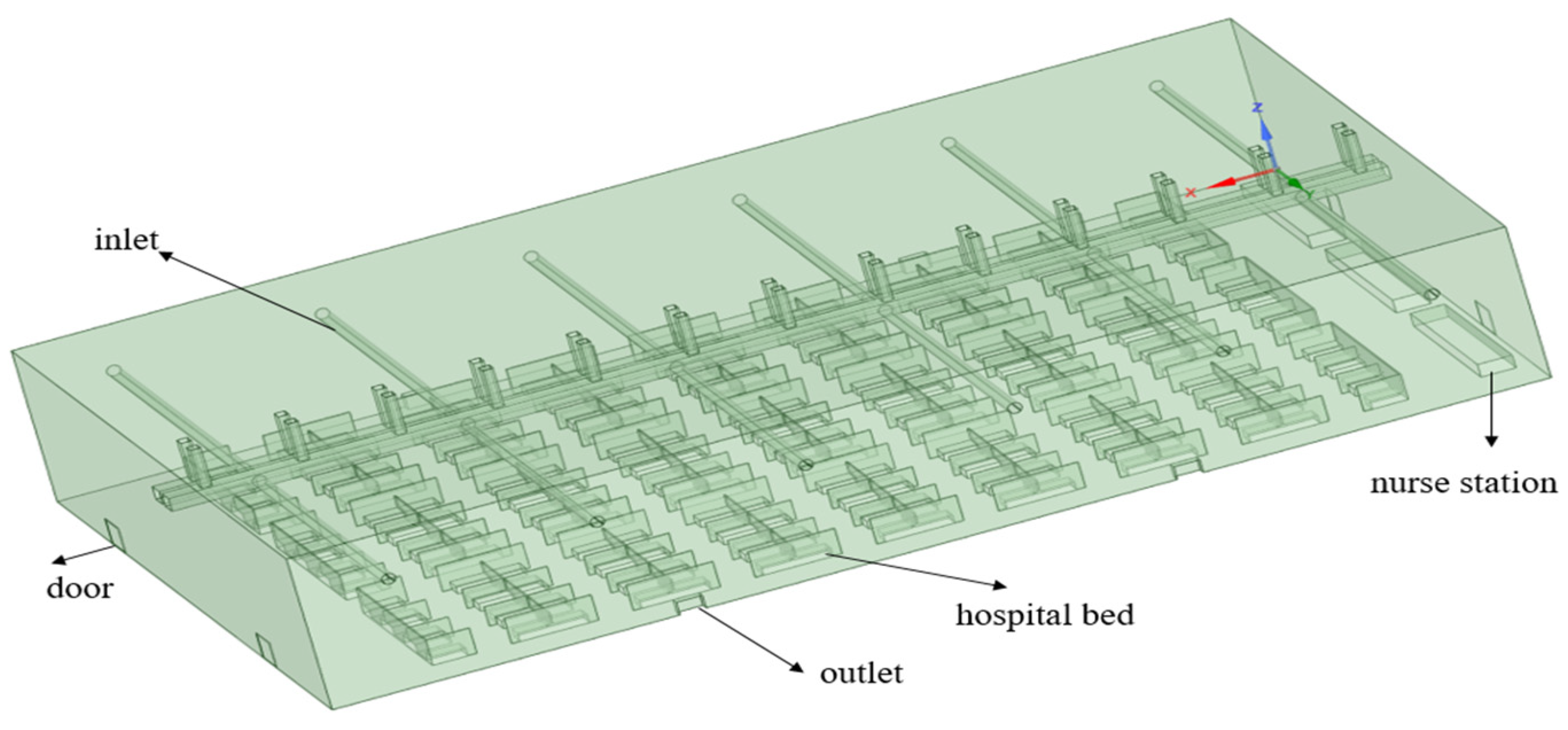
The second floor space of the gymnasium with a size of 70.1 m × 40.8 m × 10 m is divided into a hospital bed area, a nurse station and a passage area. Referring to the Fangcang shelter hospital recently renovated by the Shanghai New International Expo Center, the hospital beds are divided into 3 sections, each corresponding to 1 nurse station, each bed area has 12 × 8 beds, and a passageway of 2.5 m is left between the bed areas. Each ward is separated by a partition, and the height of the outer partition is 2 m. The site is 2860.08 m2 in total, with 288 beds and a per capita living area of 9.5 m2. The size of the single bed adopts the size of a temporary single bed of 1.95 m × 0.9 m × 0.6 m, and the nurse station occupies an area of 10 m × 2 m.
2.2. Physical Model
Using Space Claim software, a model based on the 1:1 scale of the proposed Fangcang shelter hospital on the second floor of the sports hall was established, as shown in
Figure 2.
The bag air duct is installed by lifting, and a row of air inlets is arranged on both sides of the duct in a 45° downward direction, equivalent to two 15 mm wide slits. The bag air duct supply system model is shown in
Figure 3.
The dimensions of each part of the model are shown in
Table 1.
Because the simulated gymnasium has a large geometric space, many air supplies and exhaust outlets, and the sizes of the air supply and exhaust outlets are smaller than that of the entire gymnasium, the difference between the maximum and minimum geometric dimensions is huge, which would inevitably lead to the establishment of too-dense mesh during simulation. Too-dense mesh often leads to difficulty in fast implementation of the calculation, and even difficulty in the convergence of results. Therefore, in combination with the structural symmetry of the exhibition hall, the east–west center is the axis of symmetry, and half of the space is taken as the simulation object. This can not only ensure the accuracy and reliability of the simulation experiment, but also allow the whole simulation process to become efficient and fast.
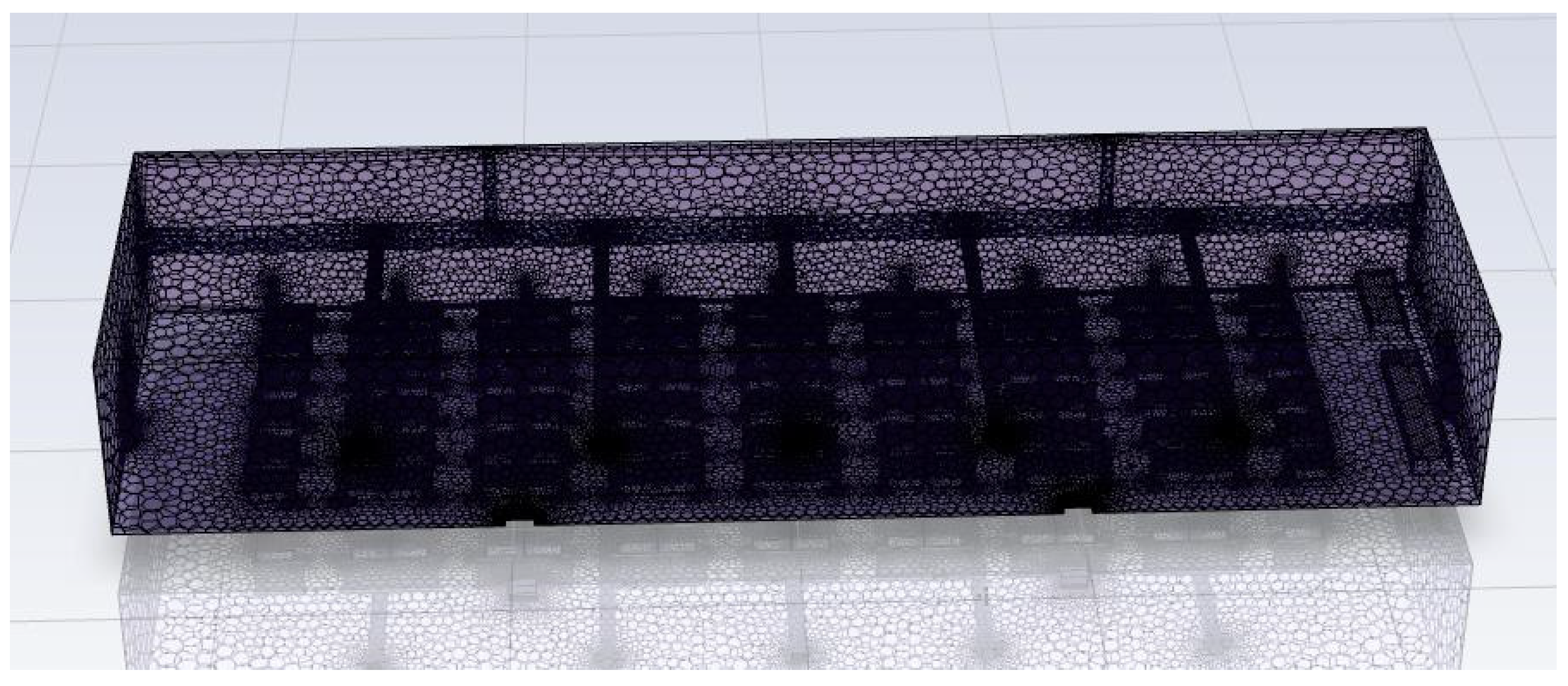
2.3. Meshing
Importing the physical model into Meshing for mesh generation, the Poly Hexcore volume mesh-generation method was used. The Poly Hexcore volume mesh-generation method based on mosaic technology can ensure the hexahedron mesh and the polyhedron mesh realize the common node connection, and compared with the traditional hexahedron mesh generation, it does not need any additional manual mesh settings. It can not only ensure the complete automation of the work, but also increase the number of hexahedrons in the mesh, thus improving the efficiency and accuracy of the solution. The air inlet, air outlet, door seam and bed are partially densified, and the rest are thinned. Finally, the mesh was obtained as shown in
Figure 4.
In order to exclude the influence of the number of meshes on the calculation results, it is necessary to perform independence verification on the meshes. The average temperature of the horizontal plane at heights of 1.65 m (Plane 1) and 0.65 m (Plane 2) above the ground under the same scheme was calculated.
Table 2 shows the calculation results for different meshes.
From the table, it can be seen that there is a certain gap in the data results when the number of meshes is 2.84 million and 3.03 million, respectively; when the number of meshes is 3.04 million and 3.26 million, the data results are similar. Therefore, 3.04 million meshes were selected for numerical simulation.
5. Conclusions
In this paper, Spaceclaim software is used to establish the model of the Fangcang shelter hospital and CFD software is used to simulate the internal airflow organization with different parameters. In order to improve the rationality of airflow organization in the Fangcang shelter hospital and ensure its internal environment meets human comfort while effectively discharging pollutants, the effects of different air supply heights, air supply temperatures and exhaust air volumes on the internal environment were studied. Through the above discussion, the following conclusions were obtained:
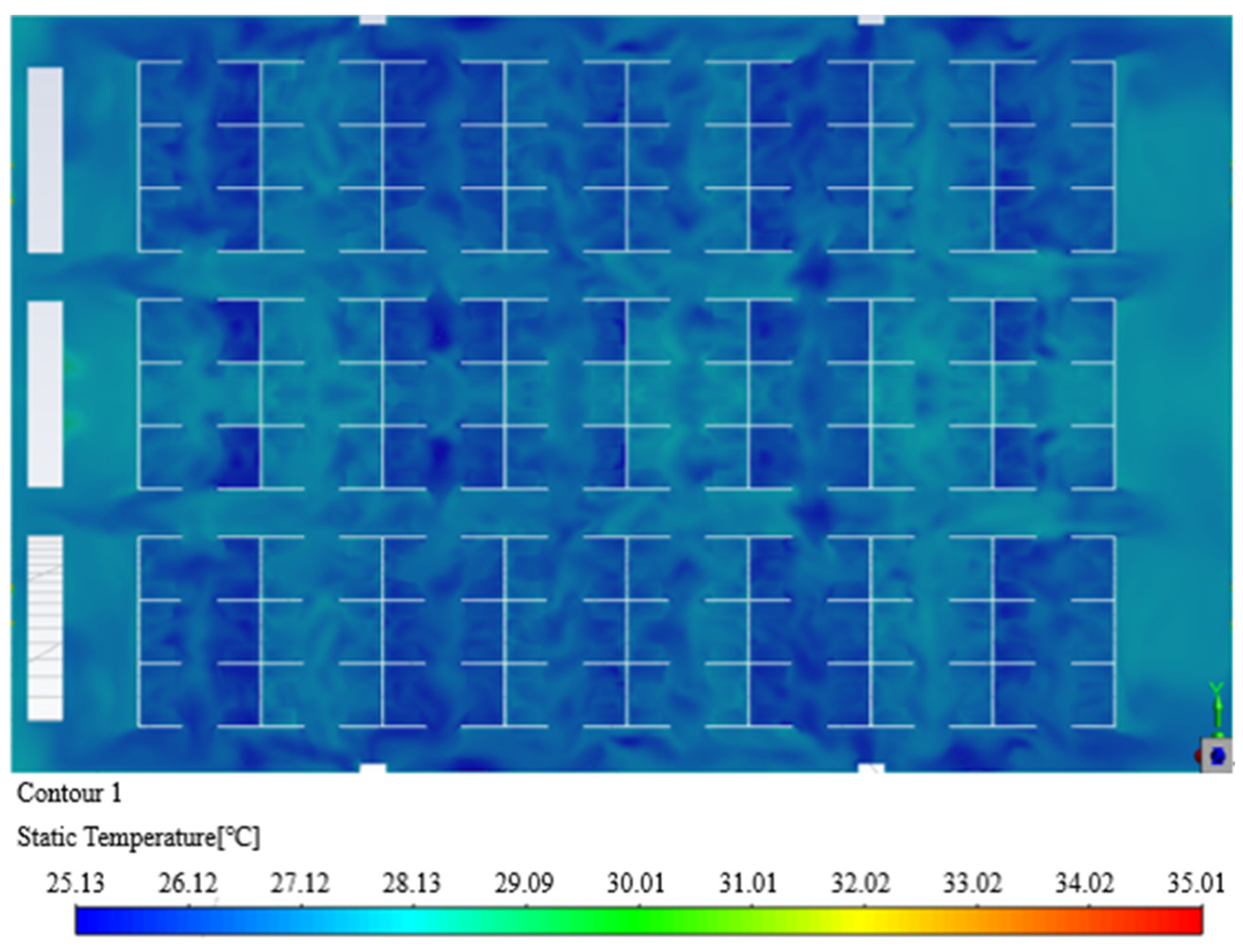
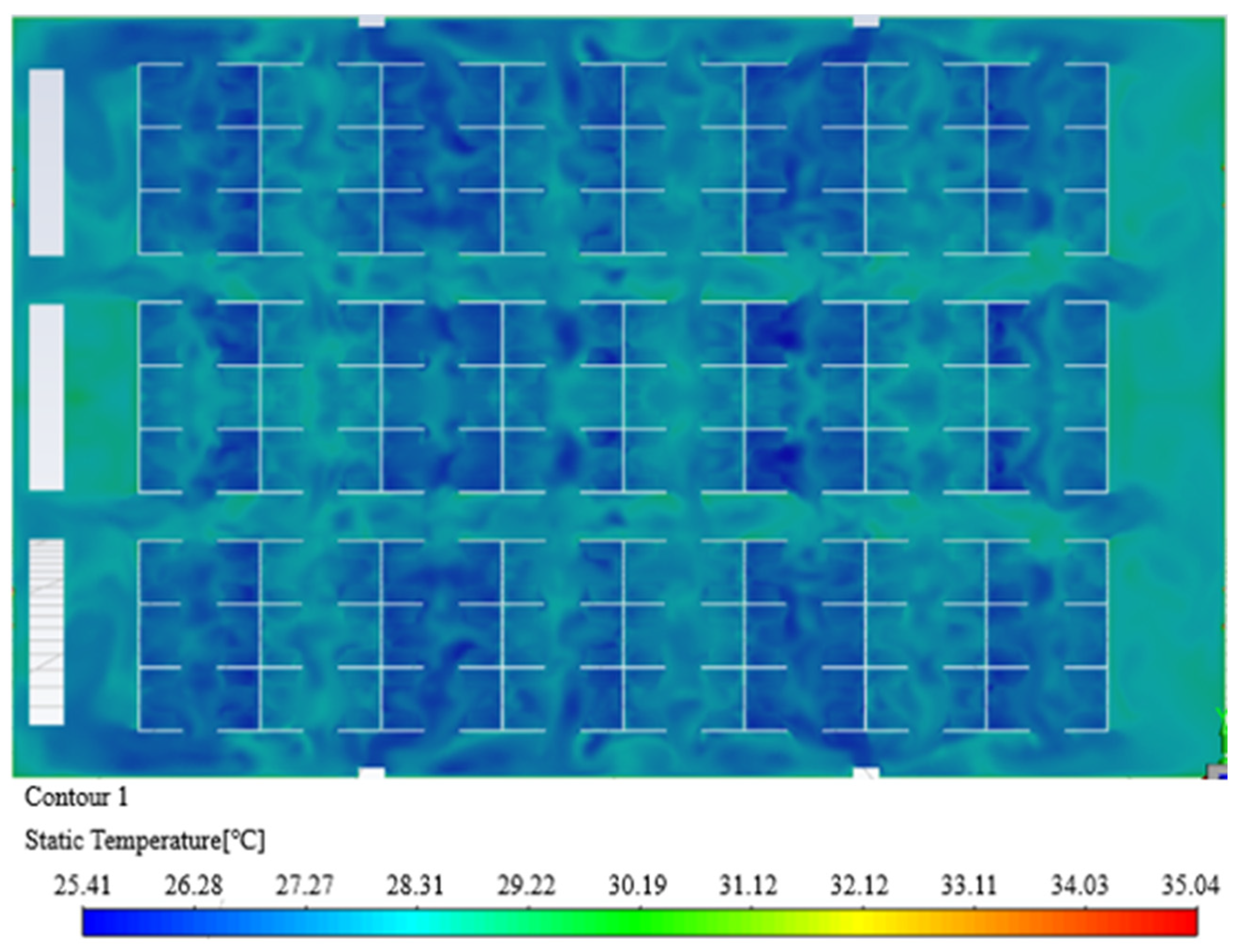
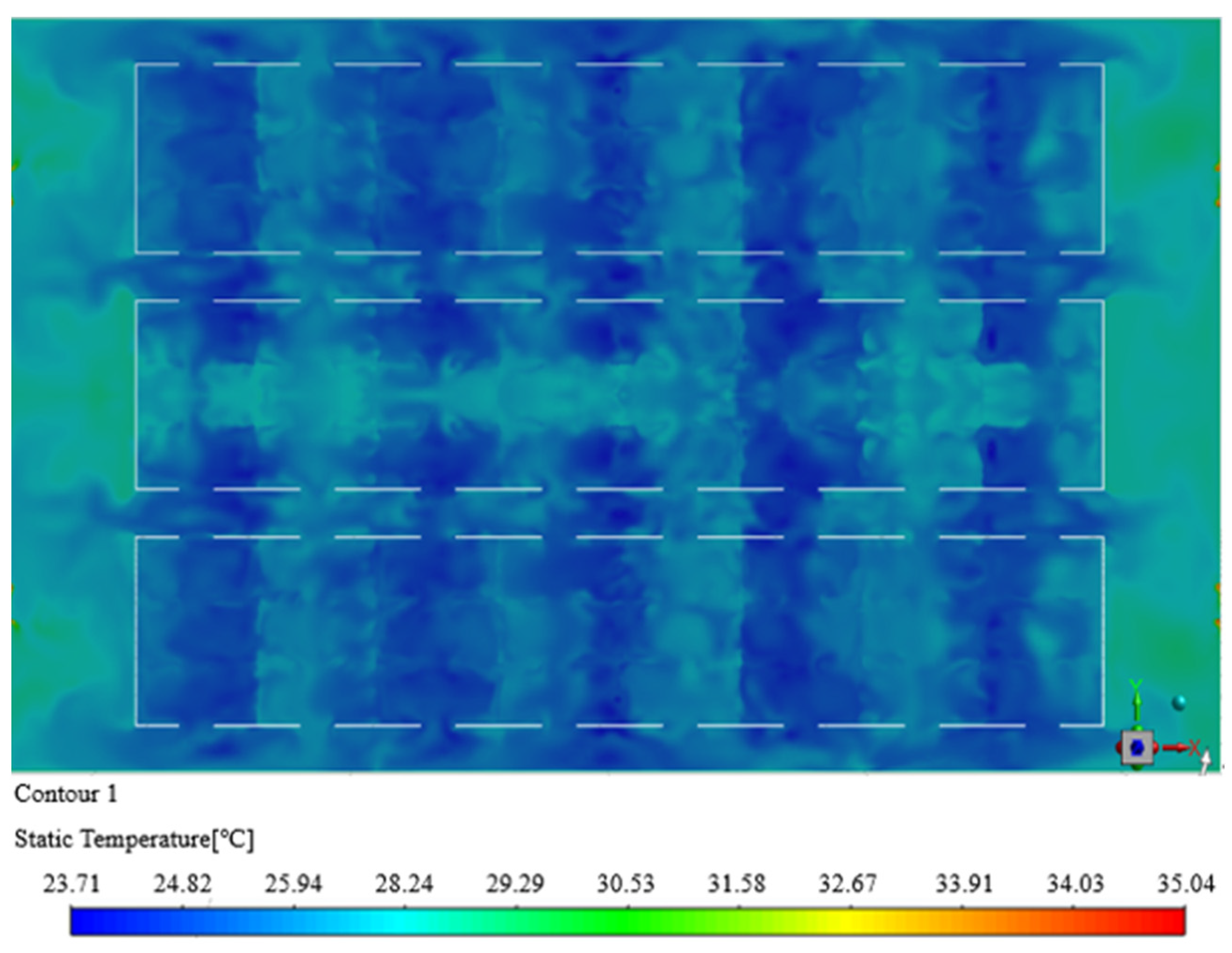
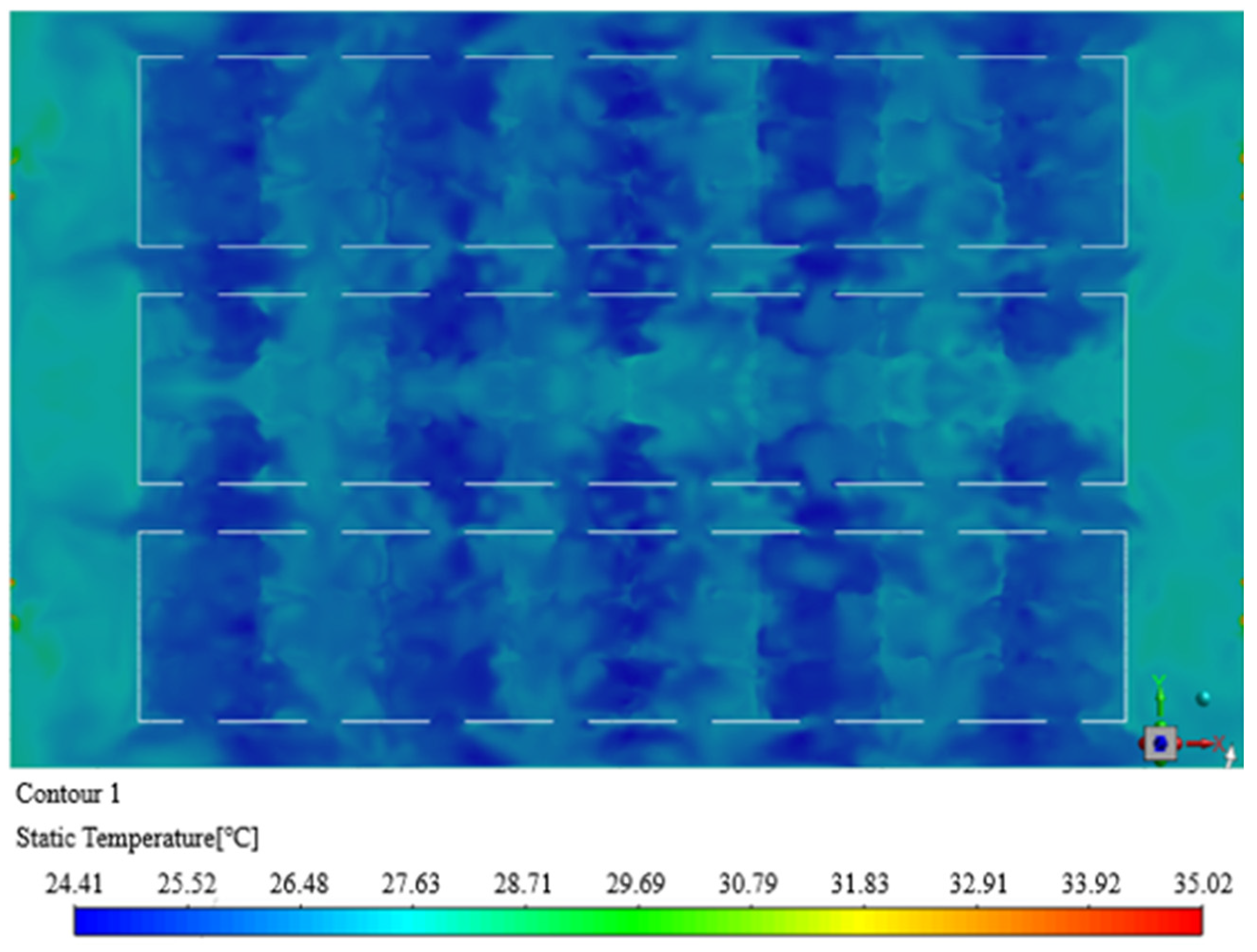
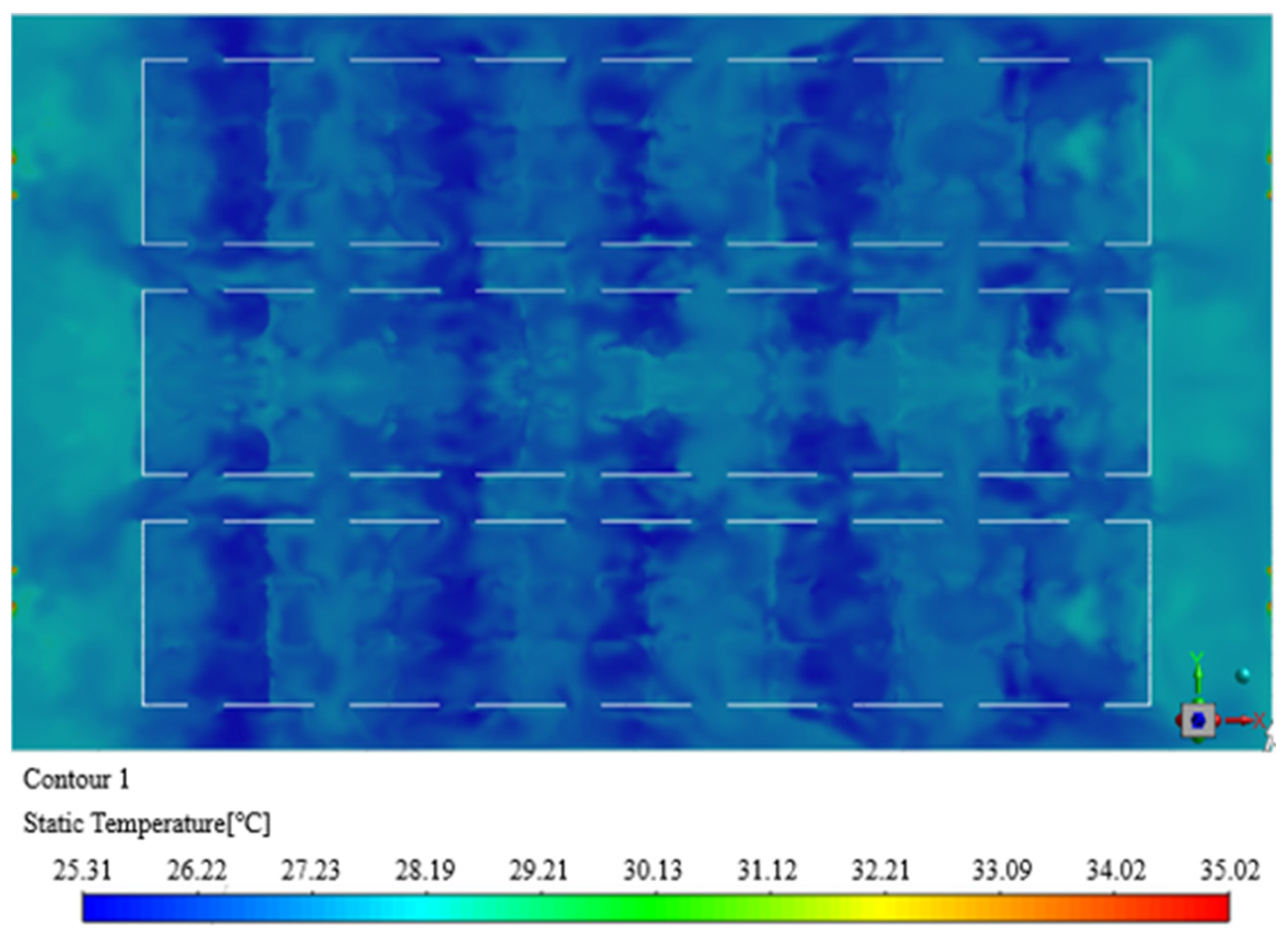
(1) When studying the air supply mode of the Fangcang shelter hospital, the control variables were used to simulate and analyze the parameter plan set considering environmental factors to determine the appropriate air supply parameters. The simulation results showed that when the air supply height is 4.5 m, the air supply temperature is 18 °C, the exhaust air volume of a single bed is 150 m3/h and the equivalent air supply speed is 1.74 m/s. The air temperature distribution in the space was relatively uniform and the airflow maintained directional flow. At the same time, the comfort level reached Level I at the personnel activity height of 1.65 m. The average wind speed of 0.25 m/s would not cause an uncomfortable blowing feeling to the human body and ensures the comfort of patients in the Fangcang shelter hospital.
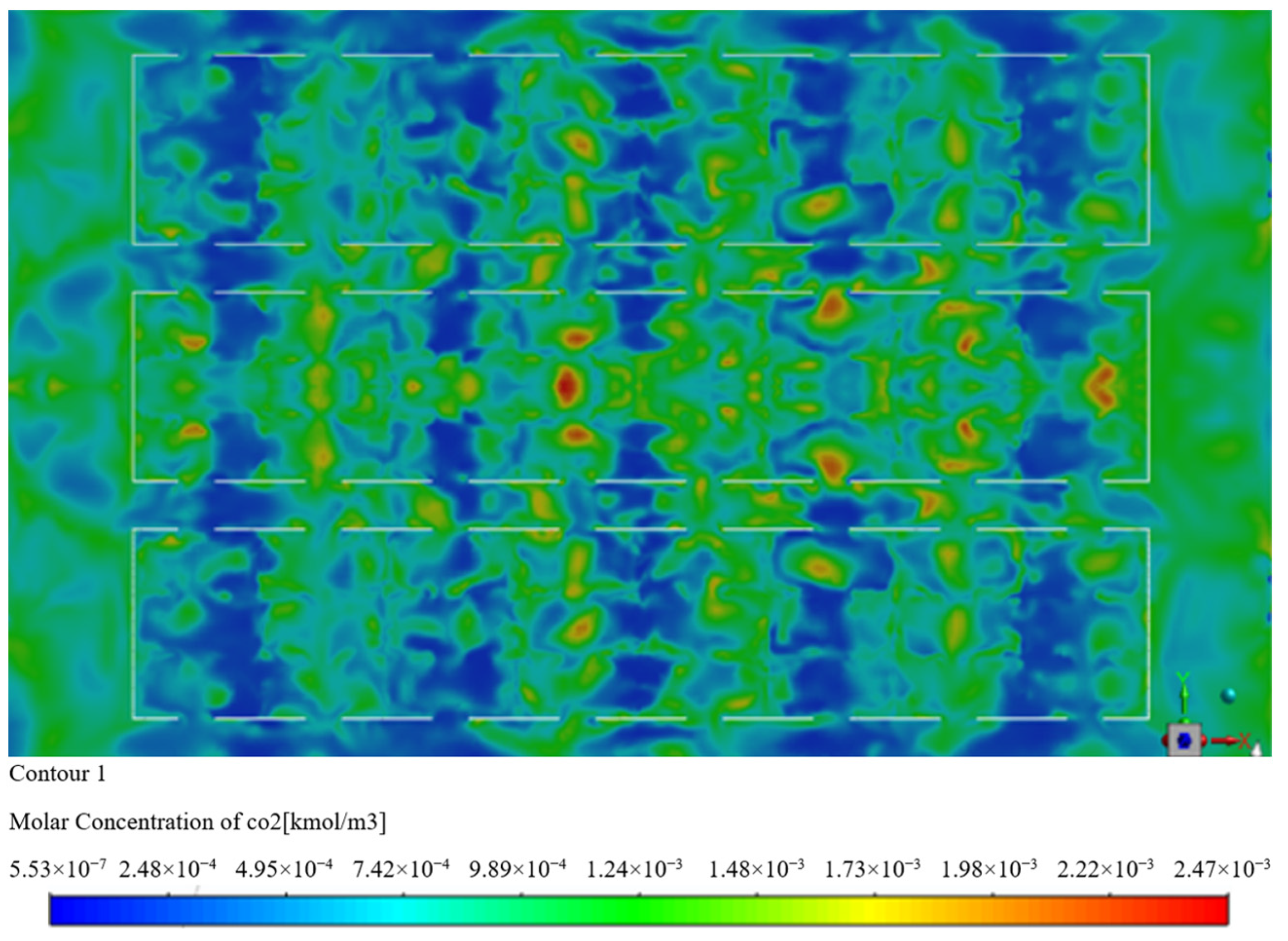
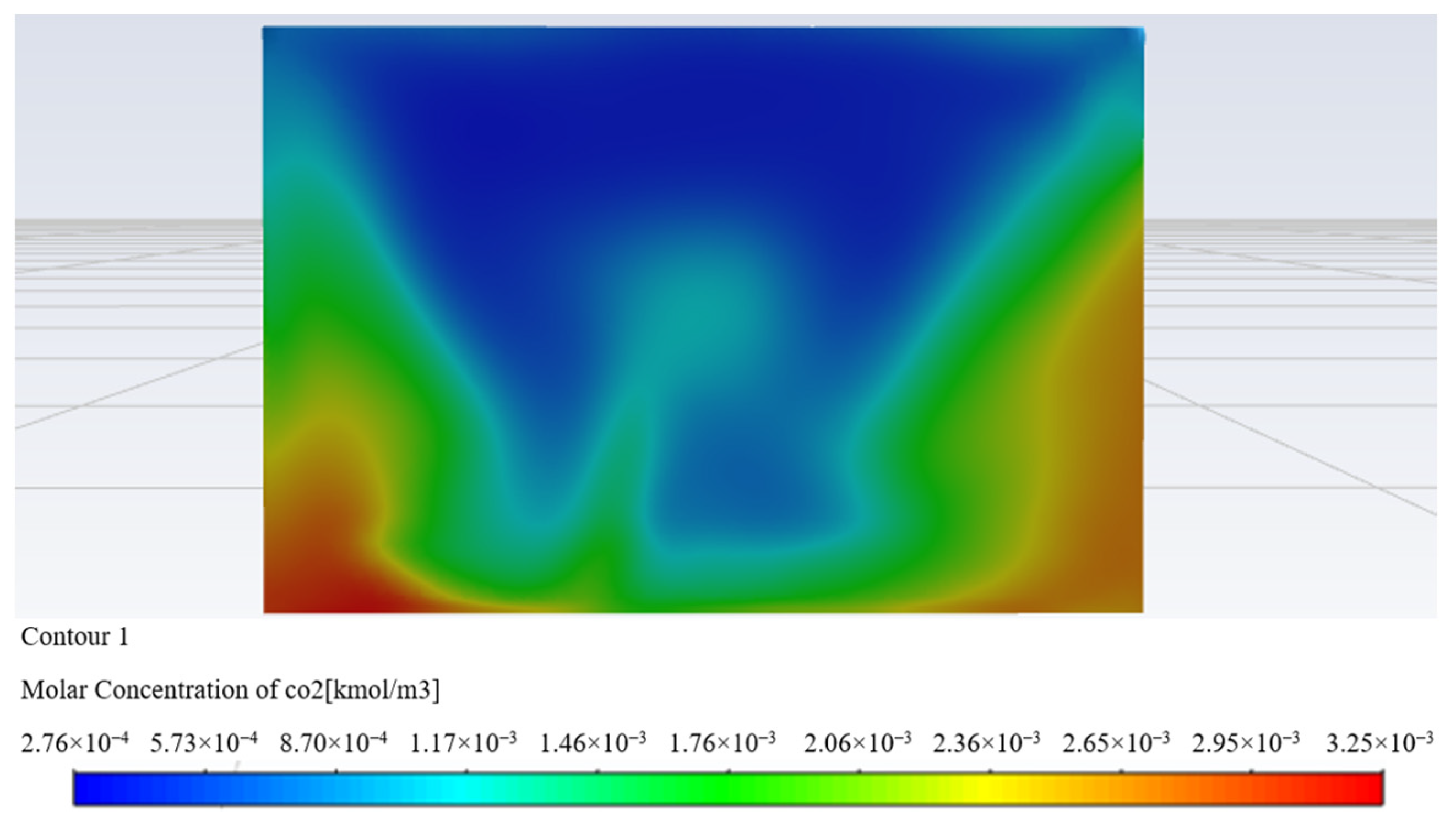
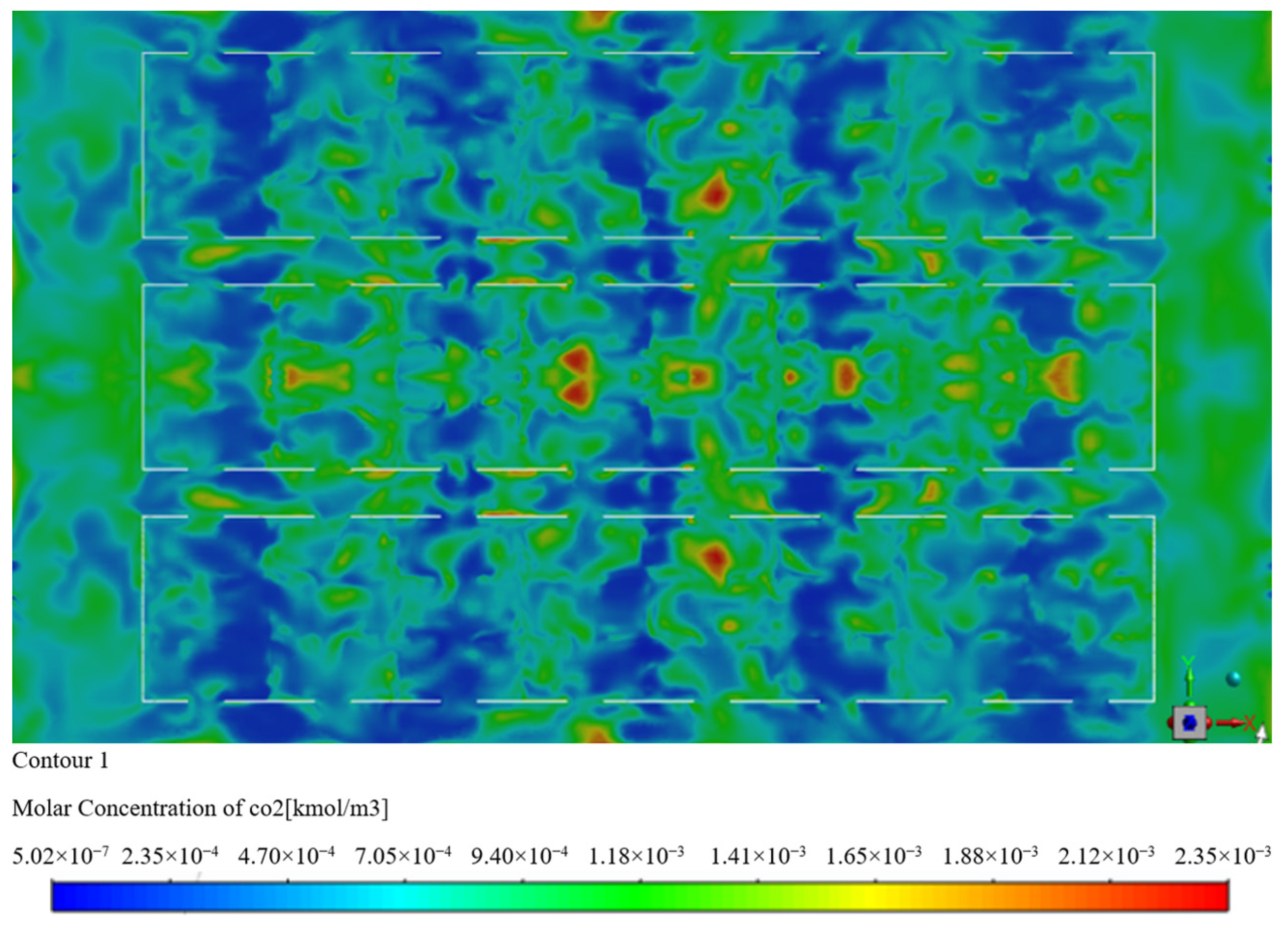
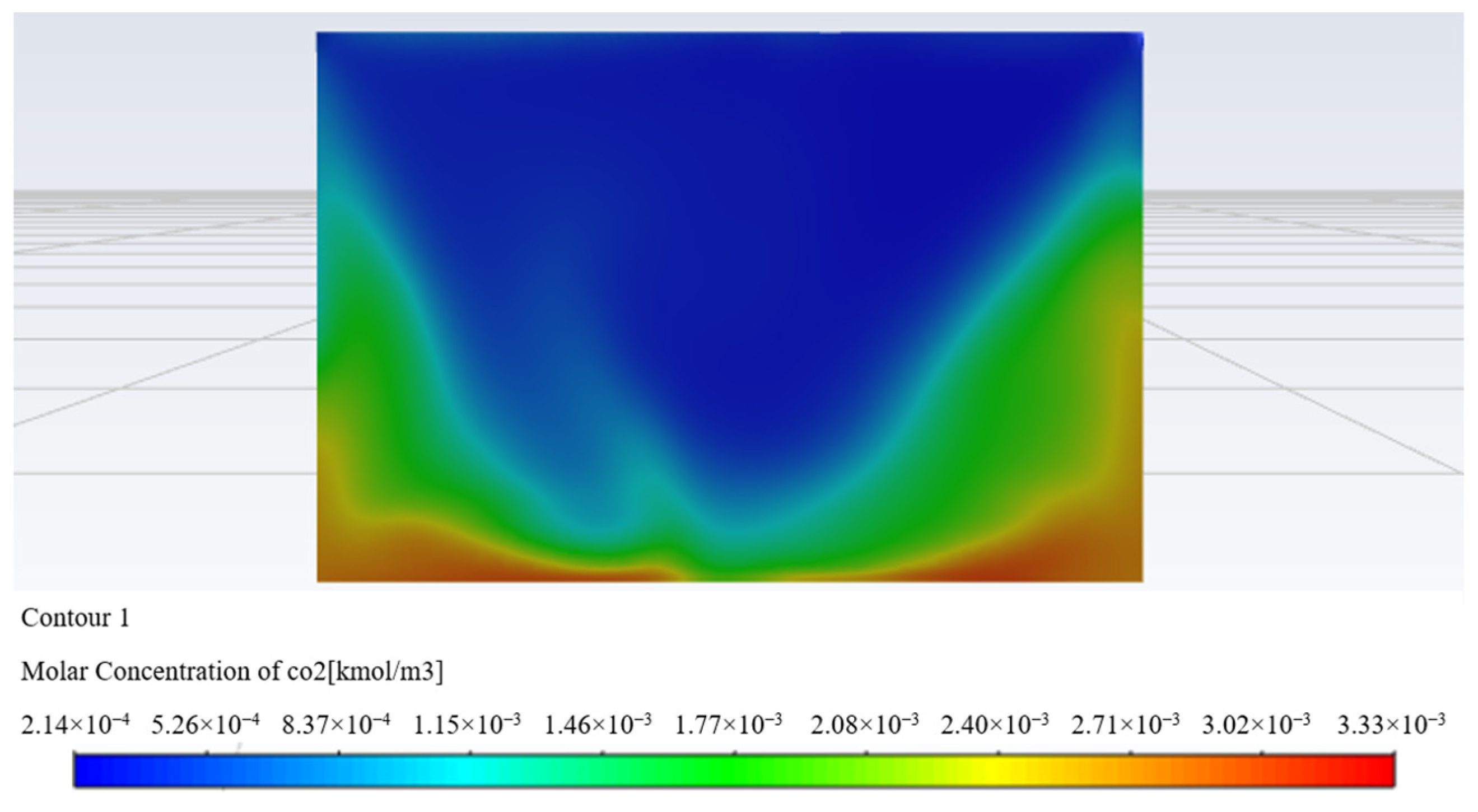
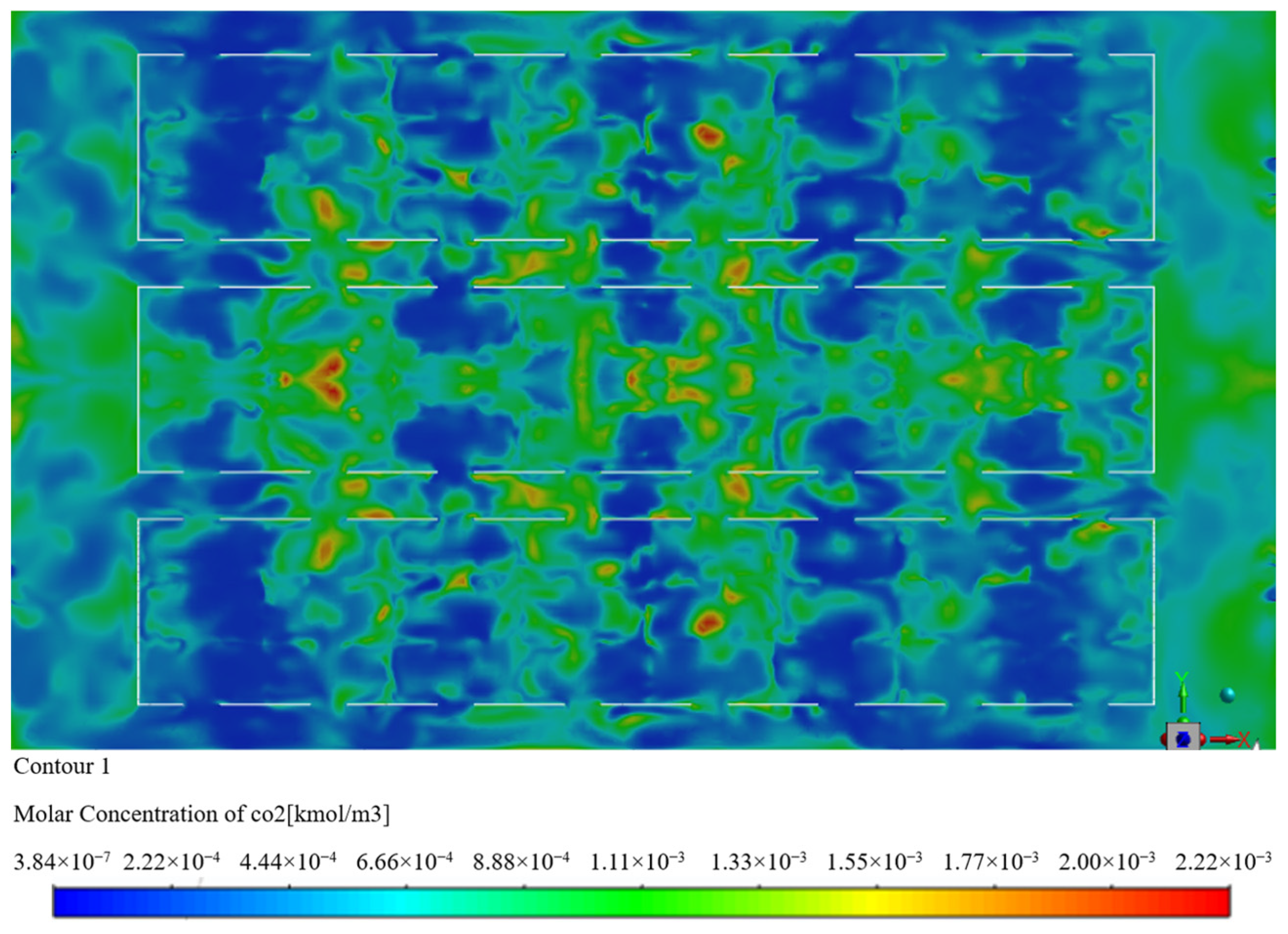
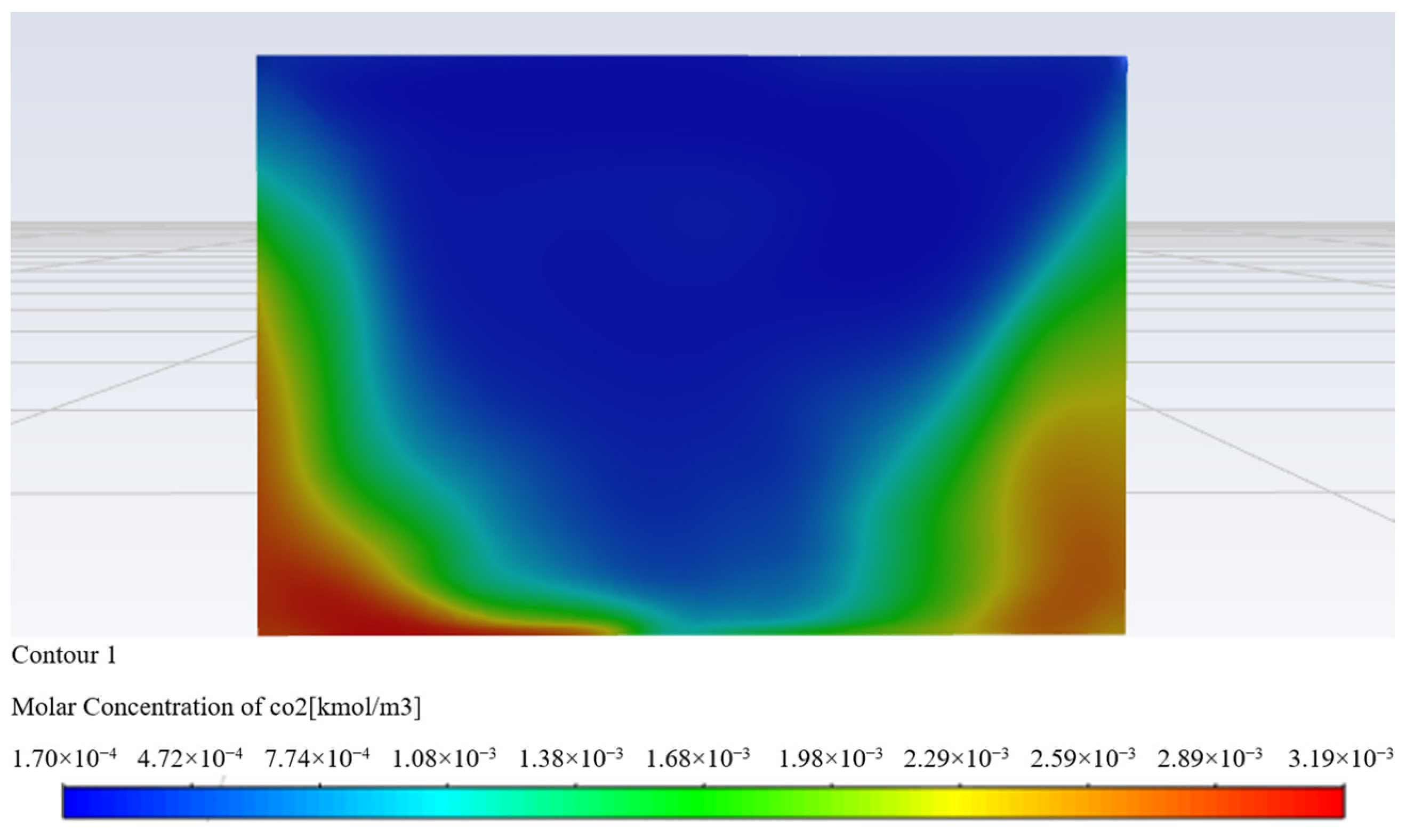
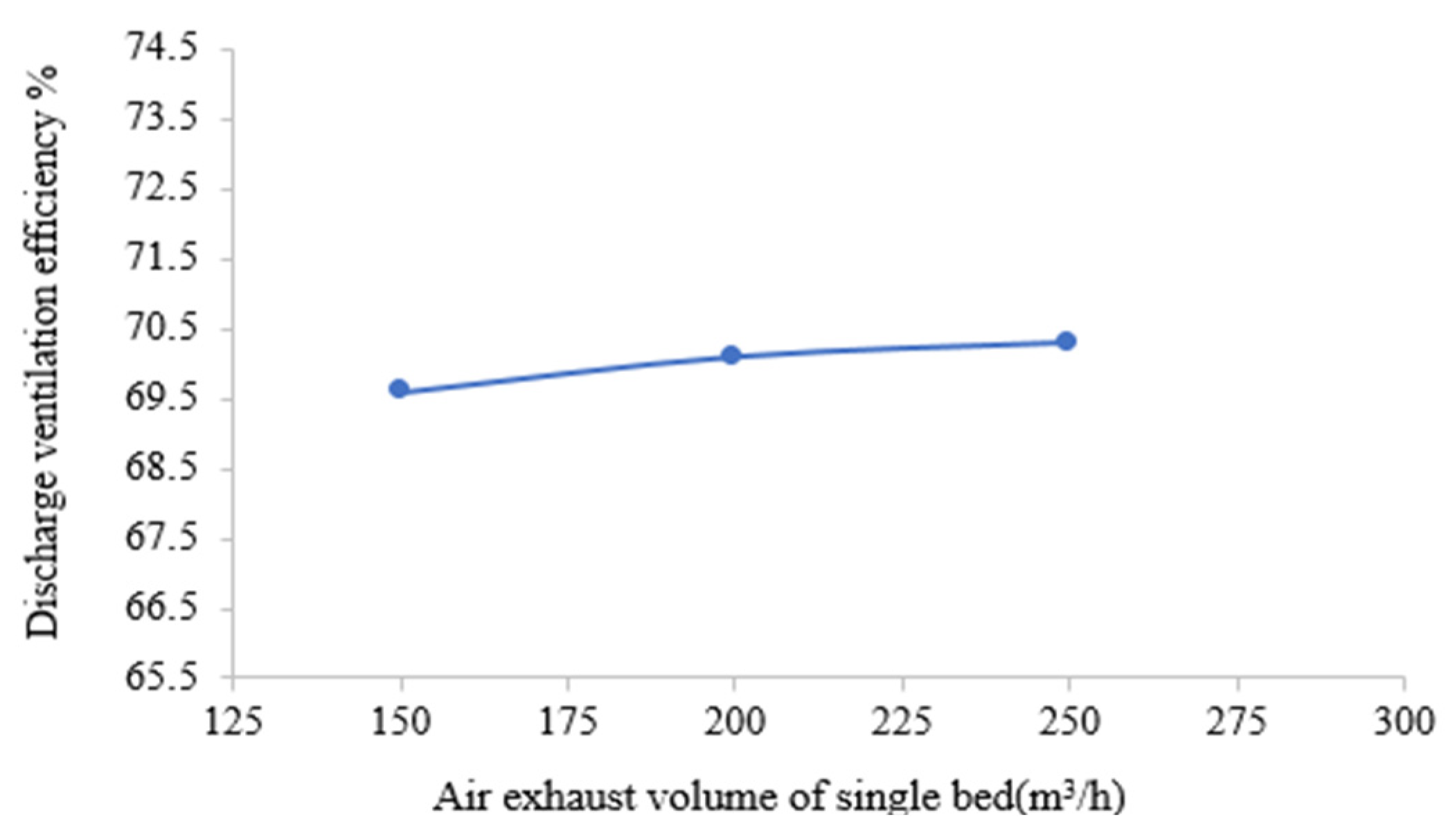
(2) The exhaust efficiency represents the efficiency index of pollutants discharged. This paper simulated the problem of pollutant emission efficiency by increasing the exhaust air volume. Through the analysis of simulation results, it was concluded that the dilution degree of pollutants grew with the increase in exhaust air volume, but the growth rate was slowed down with the increase in exhaust air volume. When the exhaust air volume is increased from 150 m3/h to 200 m3/h, the ventilation efficiency is increased by 0.5%. The ventilation efficiency increased by 0.2% from 200 m3/h to 250 m3/h, which means that with the increase in exhaust air volume, the discharge of pollutants cannot be effectively increased. In addition, the increase in exhaust air volume would produce a strong sense of blowing when the wind speed was greater than 0.3 m/s for the height of personnel activities. In the case of comprehensive consideration of pollutants’ discharge efficiency and airflow organization, the single bed exhaust air volume of 150 m3/h is optimal, which can effectively avoid the impact of a blowing feeling on patient comfort and ensure the ventilation efficiency reaches 69.6%.
In summary, the bag air duct system with the layout height of 4.5 m, exhaust air volume of 150 m3/h, and the air supply temperature of 18 °C is optimal for adoption in the Fangcang shelter hospital, and which can meet the special environmental requirements of the reconstructed Fangcang shelter hospital to jointly meet patient comfort and pollutant emissions. The simulation method and analysis provide a reasonable parameter scheme design of airflow organization and pollutant control in the Fangcang shelter hospital, a special building.



























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}