
Causal Model Analysis of the Effect of Policy Formalism, COVID-19 Fear, Social Support and Work Stress on Construction Workers’ Anxiety during the Epidemic

Abstract
:1. Introduction
Environment of a Construction Site
2. Literature Review and Hypotheses Development
2.1. Policy Formalism
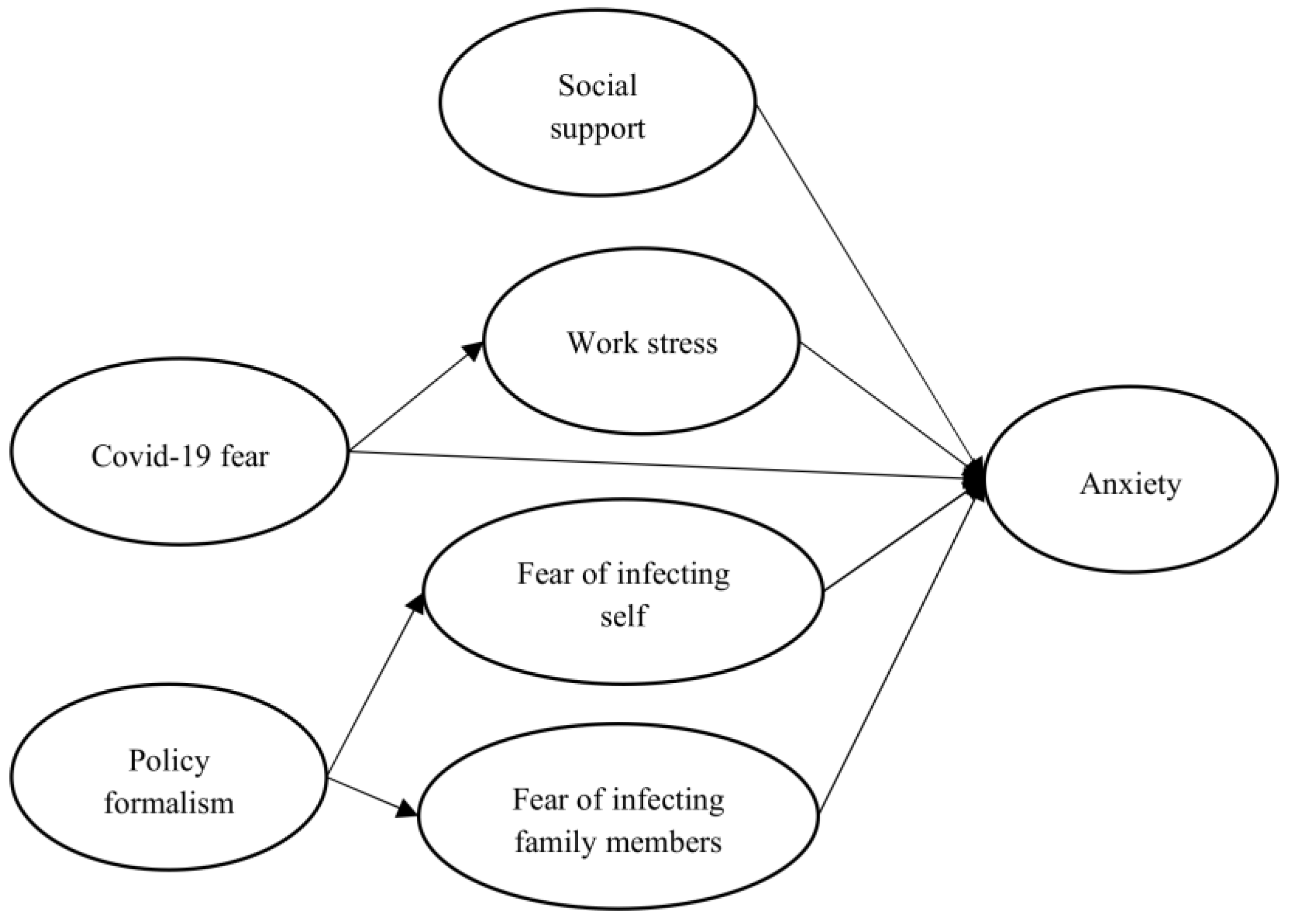
2.2. Hypotheses Development
3. Materials and Methods
3.1. Sample, Tools, and Procedure
3.2. Measures
3.3. Controlling for Common Method Variance (CMV)
4. Results
4.1. Validity and Reliability Analysis
4.2. Path Coefficients
5. Discussion
6. Conclusions
6.1. Theoretical Implications
6.2. Practical Implications
7. Further Study
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Liu, X.; Zhang, M.; Cheng, Q.; Zhang, Y.; Ye, G.; Huang, X.; Kang, M. Dengue fever transmission between a construction site and its surrounding communities in China. Parasites Vectors 2021, 14, 22. [Google Scholar] [CrossRef] [PubMed]
- Koh, D. Migrant workers and COVID-19. Occup. Environ. Med. 2020, 77, 634–636. [Google Scholar] [CrossRef] [PubMed]
- Penaloza, G.A.; Saurin, T.A.; Formoso, C.T. Monitoring complexity and resilience in construction projects: The contribution of safety performance measurement systems. Appl. Ergon. 2020, 82, 102978. [Google Scholar] [CrossRef] [PubMed]
- Selleck, R.; Hassall, M.; Cattani, M. Determining the Reliability of Critical Controls in Construction Projects. Safety 2022, 8, 64. [Google Scholar] [CrossRef]
- Deep, S.; Joshi, R.; Patil, S. Identifying the Contractor’s core competencies in post-COVID-19 scenario: Developing a survey instrument. Eng. Constr. Archit. Manag. 2022. ahead-of-print. [Google Scholar] [CrossRef]
- Xiang, Y.T.; Wen, Y.Y.; Zhang, L.; Zhang, L.; Cheung, T.; Chee, H.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Zamani, S.; Rahman, R.; Fauzi, M.; Yusof, L. Effect of COVID-19 on building construction projects: Impact and response mechanisms. In IOP Conference Series: Earth and Environmental Science, Proceedings of the 4th National Conference on Wind & Earthquake Engineering, Putrajaya, Malaysia, 16–17 October 2020; IOP Publishing: Bristol, UK, 2021. [Google Scholar]
- Assaad, R.; El-adaway, I.H. Guidelines for responding to COVID-19 pandemic: Best practices, impacts, and future research directions. J. Manag. Eng. 2021, 37, 06021001. [Google Scholar] [CrossRef]
- Ilatova, E.; Abraham, Y.S.; Celik, B.G. Exploring the Early Impacts of the COVID-19 Pandemic on the Construction Industry in New York State. Architecture 2022, 2, 26. [Google Scholar] [CrossRef]
- Alsharef, A.; Banerjee, S.; Uddin, S.M.J.; Albert, A.; Jaselskis, E. Early impacts of the COVID-19 pandemic on the United States construction industry. Int. J. Environ. Res. Public Health 2021, 18, 1559. [Google Scholar] [CrossRef]
- Rigotti, T.; De Cuyper, N.; Sekiguchi, T. The Corona crisis: What can we learn from earlier studies in applied psychology? Appl. Psychol. 2020, 69, 1–6. [Google Scholar] [CrossRef]
- Pamidimukkala, A.; Kermanshachi, S. Impact of COVID-19 on field and office workforce in construction industry. Proj. Leadersh. Soc. 2021, 2, 100018. [Google Scholar] [CrossRef]
- Ekpanyaskul, C.; Padungtod, C. Occupational Health Problems and Lifestyle Changes among Novice Working-from-Home Workers amid the COVID-19 Pandemic. Saf. Health Work 2021, 12, 384–389. [Google Scholar] [CrossRef]
- Barlow, D.H. Unraveling the mysteries of anxiety and its disorders from the perspective of emotion theory. Am. Psychol. 2000, 55, 1247. [Google Scholar] [CrossRef]
- Rubin, G.J.J.; Wessely, S. Coronavirus: The Psychological Effects of Quarantining a City. The BMJ Opinion. 2020. Available online: https://blogs.bmj.com/bmj/2020/01/24/coronavirus-the-psychological-effects-ofquarantining-a-city/ (accessed on 3 August 2022).
- De Hoog, N.N.; Stroebe, W.W.; de Wit, J.B. The processing of fear-arousing communications: How biased processing leads to persuasion. Soc. Influ. 2008, 3, 84–113. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2022, 20, 1537–1545. [Google Scholar] [CrossRef] [Green Version]
- Beidel, D.C.; Bulik, C.M.; Stanley, M.A. Abnormal Psychology; Pearson: Boston, MA, USA, 2014. [Google Scholar]
- Taylor, B. Vaccines and the changing epidemiology of autism. Child Care Health Dev. 2006, 32, 11–19. [Google Scholar] [CrossRef]
- Omran, A.; Zaid, H. Determining factors affecting safety performance practices OF construction contractors IN Gaza strip, Palestine. J. Acad. Res. Econ. 2014, 6, 350–360. [Google Scholar]
- Nawi, M.N.M.; Ibrahim, S.H.; Affandi, R.; Rosli, N.A.; Basri, F.M. Factor affecting safety performance construction industry. Int. Rev. Manag. Market. 2017, 6, 280–285. [Google Scholar]
- Dirani, K.M.; Abadi, M.; Alizadeh, A.; Barhate, B.; Garza, R.C.; Gunasekara, N.; Ibrahim, G.; Majzun, Z. Leadership competencies and the essential role of human resource development in times of crisis: A response to COVID-19 pandemic. Hum. Resour. Dev. Int. 2020, 23, 380–394. [Google Scholar] [CrossRef]
- Demerouti, E.; Mostert, K.; Bakker, A.B. Burnout and work engagement: A thorough investigation of the independency of both constructs. J. Occup. Health Psychol. 2010, 15, 209. [Google Scholar] [CrossRef] [Green Version]
- Obradovich, N.; Migliorini, R.; Paulus, M.P.; Rahwan, I. Empirical evidence of mental health risks posed by climate change. Proc. Natl. Acad. Sci. USA 2018, 115, 10953–10958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Rio-Chanona, R.M.; Mealy, P.; Pichler, A.; Lafond, F.; Farmer, J.D. Supply and demand shocks in the COVID-19 pandemic: An industry and occupation perspective. Oxf. Rev. Econ. Policy 2020, 36 (Suppl. 1), S94–S137. [Google Scholar] [CrossRef]
- Stiles, S.; Golightly, D.; Ryan, B. Impact of COVID-19 on health and safety in the construction sector. Hum. Factors Man. 2021, 31, 425–437. [Google Scholar] [CrossRef] [PubMed]
- Koçak, O.; Koçak, Ö.E.; Younis, M.Z. The Psychological Consequences of COVID-19 Fear and the Moderator Effects of Individuals’ Underlying Illness and Witnessing Infected Friends and Family. Int. J. Environ. Res. Public Health 2021, 18, 1836. [Google Scholar] [CrossRef]
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Kniffin, K.M.; Narayanan, J.; Anseel, F.; Antonakis, J.; Ashford, S.P.; Bakker, A.B.; Bamberger, P.; Bapuji, H.; Bhave, D.P.; Choi, V.K. COVID-19 and the workplace: Implications, issues, and insights for future research and action. Am. Psychol. 2021, 76, 63. [Google Scholar] [CrossRef]
- Alkilani, S.Z.; Jupp, J.; Sawhney, A. Issues of construction health and safety in developing countries: A case of Jordan. Australas. J. Constr. Econ. Build. 2013, 13, 141. [Google Scholar] [CrossRef] [Green Version]
- Bentley, T.A.; Teo, S.; McLeod, L.; Tan, F.; Bosua, R.; Gloet, M. The role of organisational support in teleworker wellbeing: A socio-technical systems approach. Appl. Ergon. 2016, 52, 207–215. [Google Scholar] [CrossRef]
- Sinclair, R.R.; Allen, T.; Barber, L.; Bergman, M.; Britt, T.; Butler, A.; Ford, M.; Hammer, L.; Kath, L.; Probst, T.; et al. Occupational health science in the time of COVID-19: Now more than ever. Occup. Health Sci. 2020, 4, 1–22. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Recchi, E.; Ferragina, E.; Helmeid, E.; Pauly, S.; Safi, M.; Sauger, N.; Schradie, J. The ‘Eye of the Hurricane’ paradox: An unexpected and unequal rise of well-being during the COVID-19 lockdown in France. Res. Soc. Stratif. Mobil. 2020, 68, 100508. [Google Scholar] [CrossRef]
- Liu, H.T. Analysis of formalism’s moderating effect on the relationships between role stressors and work anxiety—Viewpoints from oriental public administration. Int. J. Inf. Manag. Sci. 2015, 26, 85–101. [Google Scholar]
- Liu, H.-T. The Influence of Public Servant’s Perceived Formalism and Organizational Environmental Strategy on Green Behavior in Workplace. Sustainability 2021, 13, 11020. [Google Scholar] [CrossRef]
- Amaechi, O.; Ayeni, E.; Madu, C.P. The Prismatic Sala Model and Its Relevance to Nigeria’s Public Administrative System. CCU J. Humanit. 2019, 1, 113–122. [Google Scholar]
- Fox, G.; Joiner, C. Perceptions of the Vietnamese public administration system. Adm. Sci. Q. 1964, 8, 443–481. [Google Scholar] [CrossRef]
- Riggs, F.W. An ecological approach: The ‘Sala’ model. In Papers in Comparative Administration; Heady, F., Stokes, S., Eds.; University of Michigan Press: Ann Arbor, MI, USA, 1962; pp. 19–36. [Google Scholar]
- Braibanti, R. Transnational inducement of administrative reform: A survey of scope and critique of issues. In Approaches to Development; Montgomery, J.D., Sffin, W.J., Eds.; McGraw-Hill: New York, NY, USA, 1966; pp. 133–183. [Google Scholar]
- Thompson, V.A. Administrative objectives for development administration. Adm. Sci. Q. 1964, 9, 91–108. [Google Scholar] [CrossRef]
- Argyris, C. Some Causes of Organizational Ineffectiveness within the Department of State; U.S. Department of State: Washington, DC, USA, 1967. [Google Scholar]
- Burns, T.; Stalker, G.M. The Management of Innovation; Tavistock: London, UK, 1961. [Google Scholar]
- Milne, R. Mechanistic and organic models of public administration in developing countries. Adm. Sci. Q. 1970, 15, 57. [Google Scholar] [CrossRef]
- Bennis, W.G. A new role for the behavioral sciences: Effecting organizational change. Adm. Sci. Q. 1963, 8, 125–165. [Google Scholar] [CrossRef]
- Pharr, S.J.; Putnam, R.D. Disaffected Democracies: What is Troubling the Trilateral Countries? Princeton University Press: Princeton, NJ, USA, 2000. [Google Scholar]
- Welch, E.W.; Hinnant, C.C.; Moon, M.J. Linking citizen satisfaction with e government and trust in government. J. Public Adm. Res. Theory 2005, 15, 371–391. [Google Scholar] [CrossRef] [Green Version]
- Vigoda-Gadot, E.; Mizrahi, S. Managing Democracies in Turbulent Times; Springer: New York, NY, USA, 2014. [Google Scholar]
- Mizrahi, S.; Vigoda-Gadot, E.; Cohen, N. How Well Do They Manage a Crisis? The Government’s Effectiveness during the COVID-19 Pandemic. Public Adm. Rev. 2021, 81, 1120–1130. [Google Scholar] [CrossRef]
- Nannestad, P. What Have we Learned about Generalized Trust, if Anything? Annu. Rev. Polit. Sci. 2008, 11, 413–436. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. STAI Manual: For the State-Trait Anxiety Inventory, “Self Evaluation Questionnaire”; Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Mirabito, D. Social work theory and practice for crisis, disaster and trauma. In Social Work Treatment: Interlocking Theoretical Approaches; Francis, J.T., Ed.; Oxford University Press: New York, NY, USA, 2017; Volume 6, pp. 117–130. [Google Scholar]
- Carleton, R.N. The intolerance of uncertainty construct in the context of anxiety disorders: Theoretical and practical perspectives. Expert Rev. Neurother. 2012, 12, 937–947. [Google Scholar] [CrossRef] [PubMed]
- Grills-Taquechel, A.E.; Littleton, H.L.; Axsom, D. Social support, world assumptions, and exposure as predictors of anxiety and quality of life following a mass trauma. J. Anxiety Disord. 2011, 25, 498–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langford, C.P.; Bowsher, J.; Maloney, J.P.; Lillis, P.P. Social support: A conceptual analysis. J. Adv. Nurs. 1997, 25, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.J.; Petitte, D.M.M.; Leocadio, M.C.; Van Bogaert, P.; Tsaras, K. Perceptions of organizational support and its impact on nurses’ job outcomes. Nurs. Forum 2018, 53, 339–347. [Google Scholar] [CrossRef]
- Widows, M.R.; Jacobsen, P.B.; Booth-Jones, M.; Fields, K.K. Predictors of posttraumatic growth following bone marrow transplantation for cancer. Health Psychol. 2005, 24, 266. [Google Scholar] [CrossRef] [Green Version]
- Kaniasty, K. Predicting social psychological well-being following trauma: The role of postdisaster social support. Psychol. Trauma Theory Res. Pract. Policy 2012, 4, 22–33. [Google Scholar] [CrossRef] [Green Version]
- Woodward, M.J.; Eddinger, J.; Henschel, A.V.; Dodson, T.S.; Tran, H.N.; Beck, J.G. Social support, posttraumatic cognitions, and PTSD: The influence of family, friends, and a close other in an interpersonal and non-interpersonal trauma group. J. Anxiety Disord. 2015, 35, 60–67. [Google Scholar] [CrossRef]
- Zhu, W.; Wei, Y.; Meng, X.; Li, J. The mediation effects of coping style on the relationship between social support and anxiety in Chinese medical staff during COVID-19. BMC Health Serv. Res. 2020, 20, 1007. [Google Scholar] [CrossRef]
- Yin, Y.; Yang, X.; Gao, L.; Zhang, S.; Qi, M.; Zhang, L.; Tan, Y.; Chen, J. The association between social support, COVID19 exposure, and medical students’ mental health. Front. Psychiatry 2021, 12, 555893. [Google Scholar] [CrossRef]
- Bourion-Bedes, S.; Tarquinio, C.; Batt, M.; Tarquinio, P.; Lebreuilly, R.; Sorsana, C.; Legrand, K.; Rousseau, H.; Baumann, C. Psychological impact of the COVID-19 outbreak on students in a French region severely affected by the disease: Results of the PIMS-CoV 19 study. Psychiatry Res. 2021, 295, 113559. [Google Scholar] [CrossRef]
- Li, D.; Zou, L.; Zhang, Z.; Zhang, P.; Zhang, J.; Fu, W.; Mao, J.; Cao, S. The psychological effect of COVID-19 on homequarantined nursing students in China. Front. Psychiatry 2021, 12, 652296. [Google Scholar] [CrossRef]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Mai, Y.; Wu, Y.J.; Huang, Y. What type of social support is important for student resilience during COVID-19? A latent profile analysis. Front. Psychol. 2021, 12, 646145. [Google Scholar] [CrossRef]
- Yalcin, I.; Can, N.; Calisir, O.M.; Yalcin, S.; Colak, B. Latent profile analysis of COVID-19 fear, depression, anxiety, stress, mindfulness, and resilience. Curr. Psychol. 2021, 41, 459–469. [Google Scholar] [CrossRef]
- Mo, Y.; Deng, L.; Zhang, L.; Lang, Q.; Liao, C.; Wang, N.; Huang, H. Work stress among Chinese nurses to support Wuhan in fighting against COVID-19 epidemic. J. Nurs. Manag. 2020, 28, 1002–1009. [Google Scholar] [CrossRef] [Green Version]
- Shanafelt, T.; Ripp, J.; Trockel, M. Understanding and Addressing Sources of Anxiety among Health Care Professionals during the COVID-19 Pandemic. JAMA 2020, 323, 2133–2134. [Google Scholar] [CrossRef] [Green Version]
- Neria, Y.; Besser, A.; Kiper, D.; Westphal, M. A longitudinal study of posttraumatic stress disorder, depression, and generalized anxiety disorder in Israeli civilians exposed to war trauma. J. Trauma. Stress 2010, 23, 322–330. [Google Scholar] [CrossRef]
- Bokszczanin, A. Social support provided by adolescents following a disaster and perceived social support, sense of community at school, and proactive coping. Anxiety Stress Coping 2012, 25, 575–592. [Google Scholar] [CrossRef]
- Xiao, H.; Zhang, Y.; Kong, D.; Li, S.; Yang, N. The effects of social support on sleep quality of medical staff treating patients with coronavirus disease 2019 (COVID-19) in January and February 2020 in China. Med. Sci. Monit. 2020, 26, e923549. [Google Scholar] [CrossRef]
- Mikkola, L.; Suutala, E.; Parviainen, H. Social support in the workplace for physicians in specialization training. Med. Educ. Online 2018, 23, 1435114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Hidalgo, A.J.; Pantaleón, Y.; Dios, I.; Falla, D. Fear of COVID-19, Stress, and Anxiety in University Undergraduate Students: A Predictive Model for Depression. Front. Psychol. 2020, 11, 591797. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Chandran, K.M.; Valsan, T.; Naveena, K.; Krishnakumar, K. Analysis of the uncertainty among people due to the COVID-19 Pandemic. Int. J. Indian Psychol. 2020, 8, 1894–1901. [Google Scholar]
- Daniel, R.; Hall, J.K. Conspiracy theories as barriers to controlling the spread of COVID-19 in the U.S. Soc. Sci. Med. 2020, 263, 113356. [Google Scholar]
- Muhammad, S.R. Dialogic Content Analysis of Misinformation about COVID-19 on Social Media in Pakistan. Linguist. Lit. Rev. 2020, 6, 131–143. [Google Scholar]
- Nussbaumer-Streit, B.; Mayr, V.; Dobrescu, A.I.; Chapman, A.; Persad, E.; Klerings, I.; Wagner, G.; Siebert, U.; Ledinger, D.; Zachariah, C.; et al. Quarantine alone or in combination with other public health measures to control COVID-19: A rapid review. Cochrane Database Syst. Rev. 2020, 4, CD013574. [Google Scholar]
- Hooley, J.M.; Butcher, J.N.; Matthew, K.N.; Mineka, S. Abnormal Psychology; Pearson: Boston, UK, 2016. [Google Scholar]
- Dozois, D.J.A.; Rnic, K. Classification and diagnosis. In Abnormal Psychology Perspectives; Dozois, D.J.A., Ed.; Pearson: Toronto, ON, Canada, 2019; pp. 48–61. [Google Scholar]
- Pakpour, A.H.; Griffiths, M.D. The fear of COVID-19 and its role in preventive behaviors. J. Concurr. Disord. 2020, 2, 58–63. [Google Scholar]
- Taylor, S.; Landry, C.; Paluszek, M.; Fergus, T.A.; Mckay, D.; Asmundson, G.J.G. Development and initial validation of the COVID stress scales. J. Anxiety Disord. 2020, 72, 102232. [Google Scholar] [CrossRef]
- Maunder, R. The experience of the 2003 SARS outbreak as a traumatic stress among frontline healthcare workers in Toronto: Lessons learned. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 2004, 359, 1117–1125. [Google Scholar] [CrossRef] [Green Version]
- Bisson, J.I.; Tavakoly, B.; Witteveen, A.B.; Ajdukovic, D.; Jehel, L.; Johnson, V.J.; Nordanger, D.; Garcia, F.O.; Punamaki, R.; Schnyder, U.; et al. TENTS guidelines: Development of postdisaster psychological care guidelines through a Delphi process. Br. J. Psychiatry 2010, 196, 69–74. [Google Scholar] [CrossRef]
- Sinclair, R.R.; Probst, T.M.; Watson, G.P.; Bazzoli, A. Caught between scylla and charybdis: How economic stressors and occupational risk factors influence workers’ occupational health reactions to COVID-19. Appl. Psychol. 2021, 70, 85–119. [Google Scholar] [CrossRef]
- Bajrami, D.D.; Terzi´c, A.; Petrovi´c, M.D.; Radovanovi´c, M.; Tretiakova, T.N.; Hadoud, A. Will we have the same employees in hospitality after all? The impact of COVID-19 on employees’ work attitudes and turnover intentions. Int. J. Hosp. Manag. 2021, 94, 102754. [Google Scholar] [CrossRef]
- Jung, H.S.; Jung, Y.S.; Yoon, H.H. COVID-19: The effects of job insecurity on the job engagement and turnover intent of deluxe hotel employees and the moderating role of generational characteristics. Int. J. Hosp. Manag. 2021, 92, 102703. [Google Scholar] [CrossRef]
- Wong, A.K.F.; Kim, S.S.; Kim, J.; Han, H. How the COVID-19 pandemic affected hotel employee stress: Employee perceptions of occupational stressors and their consequences. Int. J. Hosp. Manag. 2021, 93, 102798. [Google Scholar] [CrossRef]
- Chen, H.; Eyoun, K. Do mindfulness and perceived organizational support work? Fear of COVID-19 on restaurant frontline employees’ job insecurity and emotional exhaustion. Int. J. Hosp. Manag. 2021, 94, 102850. [Google Scholar] [CrossRef]
- Maben, J.; Bridges, J. COVID-19: Supporting nurses’ psychological and mental health. J. Clin. Nurs. 2020, 29, 2742–2750. [Google Scholar] [CrossRef] [Green Version]
- Preti, E.; Di Mattei, V.; Perego, G.; Ferrari, F.; Mazzetti, M.; Taranto, P.; di Pierro, R.; Madeddu, F.; Calati, R. The psychological impact of epidemic and pandemic outbreaks on healthcare workers: Rapid review of the evidence. Curr. Psychiatry Rep. 2020, 22, 43. [Google Scholar] [CrossRef]
- Magnavita, N.; Tripepi, G.; Di Prinzio, R.R. Symptoms in Health Care Workers during the COVID-19 Epidemic. A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 5218. [Google Scholar] [CrossRef]
- Shacham, M.; Hamama-Raz, Y.; Kolerman, R.; Mijiritsky, O.; Ben-Ezra, M.; Mijiritsky, E. COVID-19 Factors and Psychological Factors Associated with Elevated Psychological Distress among Dentists and Dental Hygienists in Israel. Int. J. Environ. Res. Public Health 2020, 17, 2900. [Google Scholar] [CrossRef] [Green Version]
- Heymann, D.L. Ebola: Transforming fear into appropriate action. Lancet 2017, 390, 219–220. [Google Scholar] [CrossRef] [Green Version]
- Vergara-Buenaventura, A.; Chavez-Tuñon, M.; Castro-Ruiz, C. The Mental Health Consequences of Coronavirus Disease 2019 Pandemic in Dentistry. Disaster Med. Public Health Prep. 2020, 14, e31–e34. [Google Scholar] [CrossRef] [PubMed]
- Perogamvros, L.; Castelnovo, A.; Samson, D.; Dang-Vu, T.T. Failure of fear extinction in insomnia: An evolutionary perspective. Sleep Med. Rev. 2020, 51, 101277. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Cao, X.; Wang, P.; Wang, G.; Lei, G.; Shou, Z.; Xiao, Q. Emotional “inflection point” in public health emergencies with the 2019 new coronavirus pneumonia (NCP) in China. J. Affect. Disord. 2020, 276, 797–803. [Google Scholar] [CrossRef] [PubMed]
- Hagerty, S.L.; Williams, L.M. The impact of COVID-19 on mental health: The interactive roles of brain biotypes and human connection. Brain Behav. Immun. Health 2020, 5, 100078. [Google Scholar] [CrossRef]
- Spoorthy, M.S.; Pratapa, S.K.; Mahant, S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic—A review. Asian J. Psychiatry 2020, 51, 102119. [Google Scholar] [CrossRef]
- Wu, P.E.; Styra, R.; Gold, W.L. Mitigating the psychological effects of COVID-19 on health care workers. Can. Med. Assoc. J. 2020, 192, E459–E460. [Google Scholar] [CrossRef] [Green Version]
- Jahan Nipa, T.; Kermanshachi, S.; Patel, R.K. Impact of Family Income on Public’s Disaster Preparedness and Adoption of DRR Courses. In Proceedings of the Creative Construction E-Conference 2020, Opatija, Croatia, 28 June–1 July 2020; Budapest University of Technology and Economics: Budapest, Hungary, 2020; pp. 94–102. [Google Scholar]
- Hall, R.; Hall, R.; Chapman, M. The 1995 Kikwit Ebola outbreak: Lessons hospitals and physicians can apply to future viral epidemics. Gen. Hosp. Psychiatry 2008, 30, 446–452. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus Disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- McAlonan, G.; Lee, A.; Cheung, V.; Cheung, C.; Tsang, K.; Sham, P.; Chua, S.E.; Wong, J.G. Immediate and sustained psychological impact of an emerging infectious disease outbreak on health care workers. Can. J. Psychiatry 2007, 52, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Cheung, E.Y. An outbreak of fear, rumours and stigma. Intervention 2015, 13, 70–76. [Google Scholar] [CrossRef] [Green Version]
- Tsang, S.; Avery, A.R.; Duncan, G.E. Fear and depression linked to COVID-19 exposure A study of adult twins during the COVID-19 pandemic. Psychiatry Res. 2020, 296, 113699. [Google Scholar] [CrossRef]
- Huang, L.; Lei, W.; Xu, F.; Liu, H.; Yu, L. Emotional responses and coping strategies in nurses and nursing students during Covid-19 outbreak: A comparative study. PLoS ONE 2020, 15, e0237303. [Google Scholar] [CrossRef]
- Lu, W.; Wang, H.; Lin, Y.; Li, L. Psychological status of medical workforce during the COVID-19 pandemic: A crosssectional study. Psychiatry Res. 2020, 288, 112936. [Google Scholar] [CrossRef]
- Greenberg, N.; Docherty, M.; Gnanapragasam, S.; Wessely, S. Managing mental health challenges faced by healthcare workers during COVID-19 pandemic. Br. Med. J. 2020, 368, m1211. [Google Scholar] [CrossRef] [Green Version]
- Baloch, S.; Baloch, M.A.; Zheng, T.; Pei, X. The Coronavirus Disease 2019 (COVID-19) Pandemic. Tohoku J. Exp. Med. 2020, 250, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Asmundson, G.J.G.; Taylor, S. Coronaphobia: Fear and the 2019-nCoV outbreak. J. Anxiety Disord. 2020, 70, 102196. [Google Scholar] [CrossRef]
- Aslan, I.; Ochnik, D.; Çınar, O. Exploring Perceived Stress among Students in Turkey during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8961. [Google Scholar] [CrossRef]
- Dong, L.; Hu, S.; Gao, J. Discovering drugs to treat coronavirus disease 2019 (COVID-19). Drug Discov. Ther. 2020, 14, 58–60. [Google Scholar] [CrossRef]
- Liu, T.; Liang, W.; Zhong, H.; He, J.; Chen, Z.; He, G.; Song, T.; Chen, S.; Wang, P.; Li, J.; et al. Risk factors associated with COVID-19 infection: A retrospective cohort study based on contacts tracing. Emerg. Microbes Infect. 2020, 9, 1546–1553. [Google Scholar] [CrossRef]
- Van Der Velden, P.G.; Contino, C.; Das, M.; Van Loon, P.; Bosmans, M.W. Anxiety and depression symptoms, and lack of emotional support among the general population before and during the COVID-19 pandemic. A prospective national study on prevalence and risk factors. J. Affect. Disord. 2020, 277, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, M.; Arslan, G.; Özaslan, A. Perceived risk and mental health problems among healthcare professionals during COVID-19 pandemic: Exploring the mediating effects of resilience and coronavirus fear. Int. J. Ment. Health Addict. 2020, 20, 1035–1045. [Google Scholar] [CrossRef] [PubMed]
- Rovai, L.; Maremmani, A.G.; Rugani, F.; Bacciardi, S.; Pacini, M.; Dell’Osso, L.; Akiskal, H.S.; Maremmani, I. Do Akiskal & Mallya’s affective temperaments belong to the domain of pathology or to that of normality? Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 2065–2079. [Google Scholar] [PubMed]
- Tyrer, P. COVID-19 health anxiety. World Psychiatry 2020, 19, 307–308. [Google Scholar] [CrossRef] [PubMed]
- Zangoulechi, Z.; Yousefi, Z.; Keshavarz, N. The role of anxiety sensitivity, intolerance of uncertainty, and obsessive-compulsive symptoms in the prediction of cyberchondria. Adv. Biosci. Clin. Med. 2018, 6, 1–6. [Google Scholar] [CrossRef]
- Guyot, J.F. Bureaucratic transformation in Burma. In Bureaucratic Systems Emergent from the British Imperial Tradition; Ralph, B., Ed.; Asian Duke University Press: Durham, UK, 1966; pp. 354–443. [Google Scholar]
- Pye, L.W. Politics, Personality, and Nation Building: Burma’s Search for Identity; Yale University Press: New Haven, CT, USA, 1962. [Google Scholar]
- Shukla, A.; Srivastava, R. Development of short questionnaire to measure an extended set of role expectation conflict, coworker support and work-life balance: The new job stress scale. Cogent Bus. Manag. 2016, 3, 1. [Google Scholar] [CrossRef]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef]
- Tasso, A.F.; Sahin, N.H.; Roman, G.J.S. COVID-19 disruption on college students: Academic and socioemotional implications. Psychol. Trauma Theory Res. Pract. Policy 2021, 13, 9–15. [Google Scholar] [CrossRef]
- Spatafora, F.; Fialho, P.M.M.; Busse, H.; Helmer, S.M.; Zeeb, H.; Stock, C.; Wendt, C.; Pischke, C.R. Fear of Infection and Depressive Symptoms among German University Students during the COVID-19 Pandemic: Results of COVID-19 International Student Well-Being Study. Int. J. Environ. Res. Public Health 2022, 19, 1659. [Google Scholar] [CrossRef]
- Nunnally, J.C. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1967. [Google Scholar]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Murray, J.Y.; Kotabe, M.; Zhou, J.N. Strategic alliance-based sourcing and market performance: Evidence from foreign firms operating in China. J. Int. Bus. Stud. 2005, 36, 187–208. [Google Scholar] [CrossRef]
- Fuller, C.M.; Simmering, M.J.; Atinc, G.; Atinc, Y.; Babin, B.J. Common methods variance detection in business research. J. Bus. Res. 2016, 69, 3192–3198. [Google Scholar] [CrossRef]
- Hair, J.; Black, W.; Babin, B.; Anderson, R. Multivariate Data Analysis; Prentice-Hall, Inc.: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Fornell, C.R.; Larcker, F.F. Structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–51. [Google Scholar] [CrossRef]
- Hulland, J.S. Use of partial least squares (PLS) in strategic management research: A review of four recent studies. Strateg. Manag. J. 1999, 20, 195–204. [Google Scholar] [CrossRef]
- Jöreskog, K.G.; Söbom, D. LISREL 8: Structural Equation Modeling with the SIMPLIS Command Language; Scientific Software International: Chicago, IL, USA, 1993. [Google Scholar]
- Baron, R.M.; Kenny, D.A. The Moderator–Mediator Variable Distinction in Social Psychological Research: Conceptual, Strategic, and Statistical Considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]


{kind=link}
| Gender | Percentage (%) | Seniority | Percentage (%) |
|---|---|---|---|
| Male | 52.2% | 1–3 years | 33.9% |
| Female | 47.8% | 4–7 years | 15.9% |
| Age | Percentage (%) | 8–11 years | 13.3% |
| 20–29 years old | 24.9% | 12–15 years | 5.7% |
| 30–39 years old | 42.7% | 16 years or above | 31.2% |
| 40–49 years old | 9.0% | Marriage | Percentage (%) |
| 50 years old or older | 23.4% | Unmarried | 31.1% |
| Occupation | Percentage (%) | Married | 63.8% |
| Director | 3.0% | other | 5.1% |
| Engineer | 3.5% | Number of children | Percentage (%) |
| Supervisor | 3.2% | 1 | 12.5% |
| Administrator | 18.0% | 2 | 35.1% |
| Technical staff | 14.7% | 3 | 15.3% |
| Worker | 57.6% | 4 or more | 5.8% |
| none | 31.2% |
| Variables | Items | Lambda | z Values | Composite Reliability | Cronbach’s Alpha |
|---|---|---|---|---|---|
| Policy formalism | Policy formalism 1 | 0.88 | -- | 0.95 | 0.95 |
| Policy formalism 2 | 0.91 | 98.9 | |||
| Policy formalism 3 | 0.96 | 99.3 | |||
| Policy formalism 4 | 0.90 | 95.2 | |||
| Social support | Social support 1 | 0.82 | -- | 0.94 | 0.94 |
| Social support 2 | 0.93 | 51 | |||
| Social support 3 | 0.86 | 51.1 | |||
| Social support 4 | 0.92 | 51.6 | |||
| Social support 5 | 0.81 | 48.8 | |||
| Work stress | Work stress 1 | 0.92 | -- | 0.95 | 0.94 |
| Work stress 2 | 0.91 | 181.7 | |||
| Work stress 3 | 0.88 | 186.8 | |||
| Work stress 4 | 0.85 | 172.9 | |||
| Work stress 5 | 0.93 | 188.6 | |||
| Work stress 6 | 0.67 | 132.6 | |||
| Anxiety | Anxiety 1 | 0.78 | -- | 0.91 | 0.90 |
| Anxiety 2 | 0.84 | 154.0 | |||
| Anxiety 3 | 0.89 | 169.1 | |||
| Anxiety4 | 0.86 | 170.1 | |||
| COVID-19 fear | COVID-19 fear 1 | 0.79 | -- | 0.92 | 0.92 |
| COVID-19 fear 2 | 0.80 | 150.9 | |||
| COVID-19 fear 3 | 0.80 | 153.7 | |||
| COVID-19 fear 4 | 0.90 | 162.5 | |||
| COVID-19 fear 5 | 0.88 | 165.7 | |||
| COVID-19 fear 6 | 0.70 | 152.3 | |||
| Fear of infecting family members | Fear of infecting family members 1 | 0.80 | -- | 0.92 | 0.91 |
| Fear of infecting family members 2 | 0.88 | 134.2 | |||
| Fear of infecting family members 3 | 0.92 | 138.8 | |||
| Fear of infecting family members 4 | 0.81 | 131.4 | |||
| Fear of infecting family members 5 | 0.69 | 111.8 | |||
| Fear of infecting self | Fear of infecting self 1 | 0.92 | -- | 0.96 | 0.96 |
| Fear of infecting self 2 | 0.92 | 201.5 | |||
| Fear of infecting self 3 | 0.93 | 201.1 | |||
| Fear of infecting self 4 | 0.94 | 199.6 | |||
| Fear of infecting self 5 | 0.83 | 166.8 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | ASV | MSV | AVE | |
|---|---|---|---|---|---|---|---|---|---|---|
| Policy formalism (1) | (0.91) | 0.11 | 0.27 | 0.83 | ||||||
| COVID-19 fear (2) | 0.34 | (0.81) | 0.26 | 0.49 | 0.66 | |||||
| Fear of infecting family members (3) | 0.52 | 0.54 | (0.84) | 0.21 | 0.33 | 0.70 | ||||
| Fear of infecting self (4) | 0.35 | 0.70 | 0.57 | (0.92) | 0.26 | 0.49 | 0.84 | |||
| Anxiety (5) | 0.22 | 0.59 | 0.42 | 0.61 | (0.85) | 0.23 | 0.40 | 0.72 | ||
| Social support (6) | 0.13 | 0.05 | 0.26 | 0.07 | −0.15 | (0.87) | 0.02 | 0.07 | 0.75 | |
| Work stress (7) | 0.30 | 0.54 | 0.35 | 0.52 | 0.63 | 0.01 | (0.88) | 0.20 | 0.40 | 0.77 |
| Hypotheses | Causal Path | Coefficients | Standard Deviation | z Statistics | Accept or Reject |
|---|---|---|---|---|---|
| H1 | Social support->Anxiety | −0.28 *** | 0.03 | −11.37 | accepted |
| H2 | COVID-19 fear->Anxiety | 0.18 *** | 0.04 | 4.65 | accepted |
| H3 | COVID-19 fear->Work stress | 0.80 *** | 0.06 | 19.88 | accepted |
| H4 | Work stress ->Anxiety | 0.60 *** | 0.03 | 13.72 | accepted |
| H6 | Fear of infecting family members->Anxiety | 0.07 ** | 0.02 | 2.92 | accepted |
| H7 | Fear of infecting self->Anxiety | 0.26 *** | 0.02 | 10.88 | accepted |
| H8 | Policy formalism->Fear of infecting family members | 0.60 *** | 0.04 | 16.27 | accepted |
| H9 | Policy formalism->Fear of infecting self | 0.50 *** | 0.05 | 13.70 | accepted |
| Path Estimates | Label | Estimate | SE | z | p | % Mediation |
|---|---|---|---|---|---|---|
| COVID-19 fear->Work stress | a | 0.79 | 0.03 | 28.8 | <0.001 | |
| Work stress->Anxiety | b | 0.36 | 0.02 | 17.9 | <0.001 | |
| COVID-19 fear->Anxiety | c | 0.28 | 0.02 | 12.8 | <0.001 | |
| Mediation Estimates | ||||||
| Indirect | a × b | 0.28 | 0.02 | 15.2 | <0.001 | 50.3 |
| Direct | c | 0.28 | 0.02 | 12.8 | <0.001 | 49.7 |
| Total | c + a × b | 0.56 | 0.02 | 31.4 | <0.001 | 100.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, T.-L.; Liu, H.-T. Causal Model Analysis of the Effect of Policy Formalism, COVID-19 Fear, Social Support and Work Stress on Construction Workers’ Anxiety during the Epidemic. Buildings 2023, 13, 10. https://doi.org/10.3390/buildings13010010
Wu T-L, Liu H-T. Causal Model Analysis of the Effect of Policy Formalism, COVID-19 Fear, Social Support and Work Stress on Construction Workers’ Anxiety during the Epidemic. Buildings. 2023; 13(1):10. https://doi.org/10.3390/buildings13010010
Chicago/Turabian StyleWu, Tsung-Lin, and Hsiang-Te Liu. 2023. "Causal Model Analysis of the Effect of Policy Formalism, COVID-19 Fear, Social Support and Work Stress on Construction Workers’ Anxiety during the Epidemic" Buildings 13, no. 1: 10. https://doi.org/10.3390/buildings13010010