
Energy Analysis and Forecast of a Major Modern Hospital


Abstract
:1. Introduction
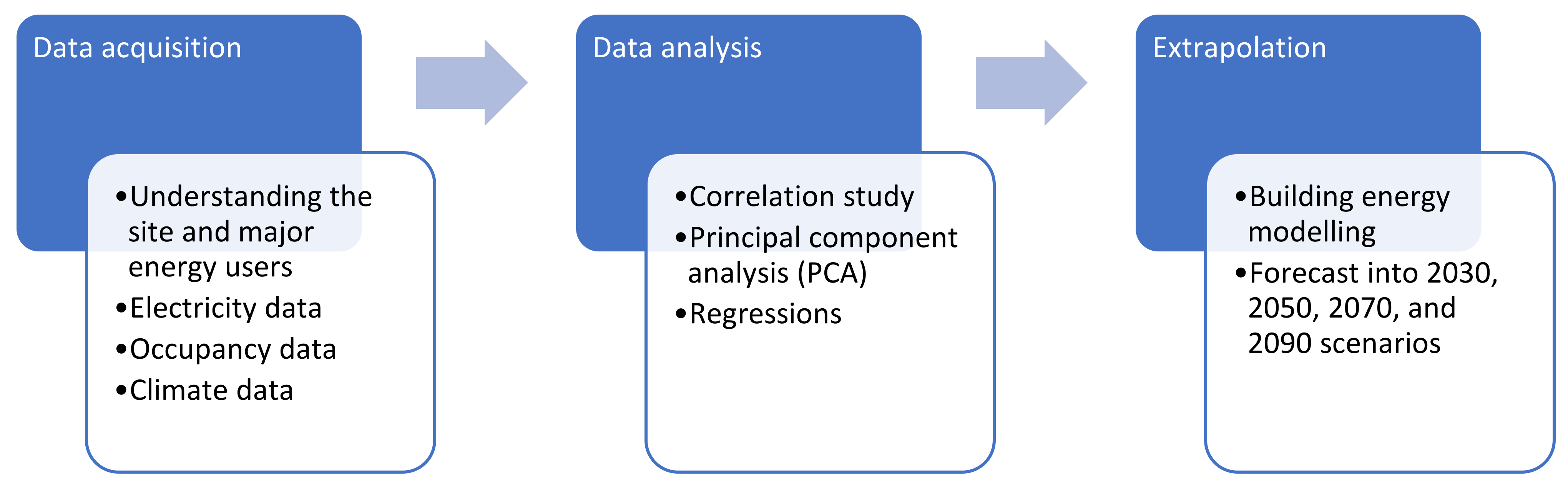
2. Inputs and Methods
2.1. Data Acquisition
2.2. Data Analysis
2.3. Forecasting
- No significant expansion is considered for the site precinct. The case study is a modern major urban vertical hospital and the physical site boundary is limited.
- Like-for-like replacements are considered for existing facility assets when they are out of service lifetime. Potentially new assets would have higher efficiency for the same output rating.
- Increased energy use due to new clinical equipment is largely offset by energy efficiency improvements from other facility assets.
- Indoor thermal comfort is maintained through the 2030 to 2090 scenarios. For example, HVAC systems fully meet the thermal conditioning and ventilation needs of the site buildings.
3. Case Study Results
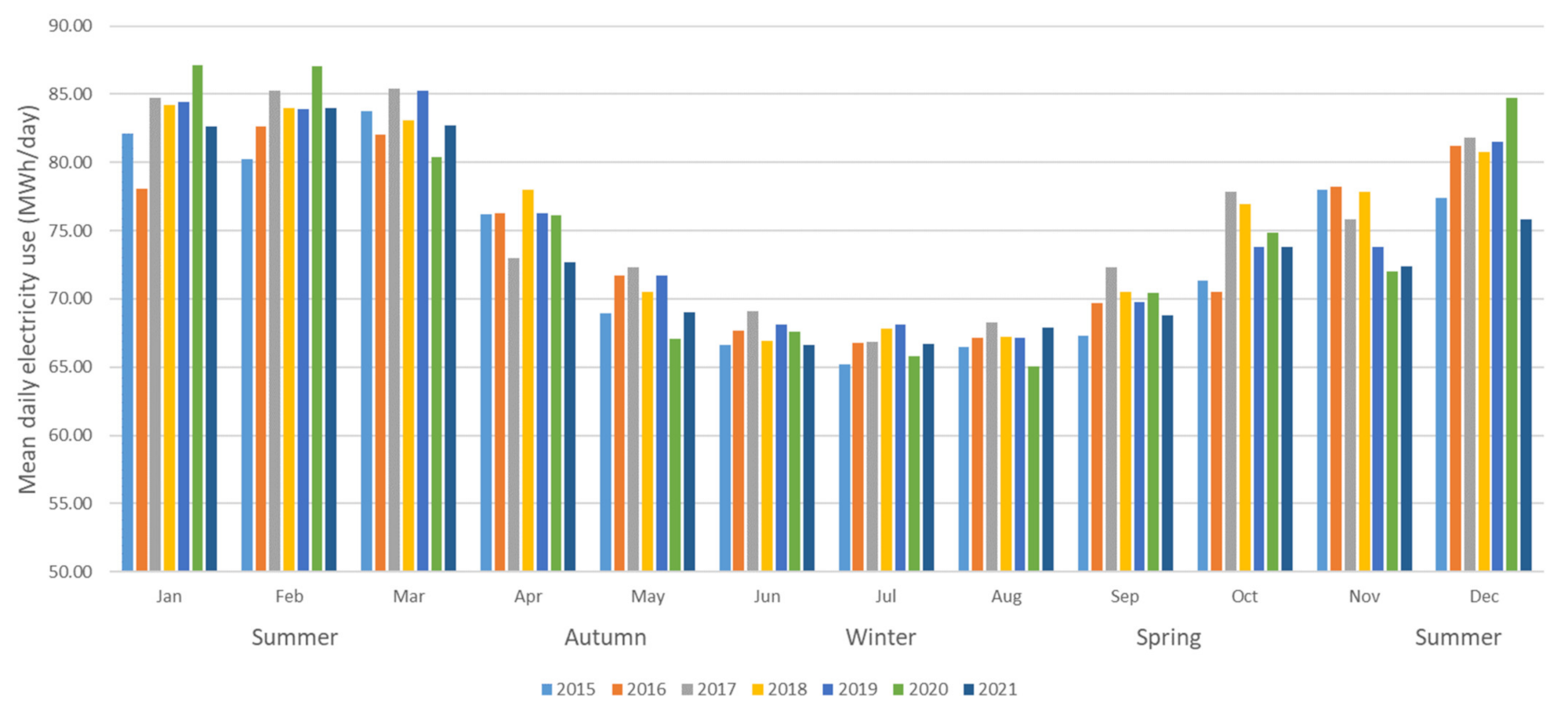
3.1. Case Study Site
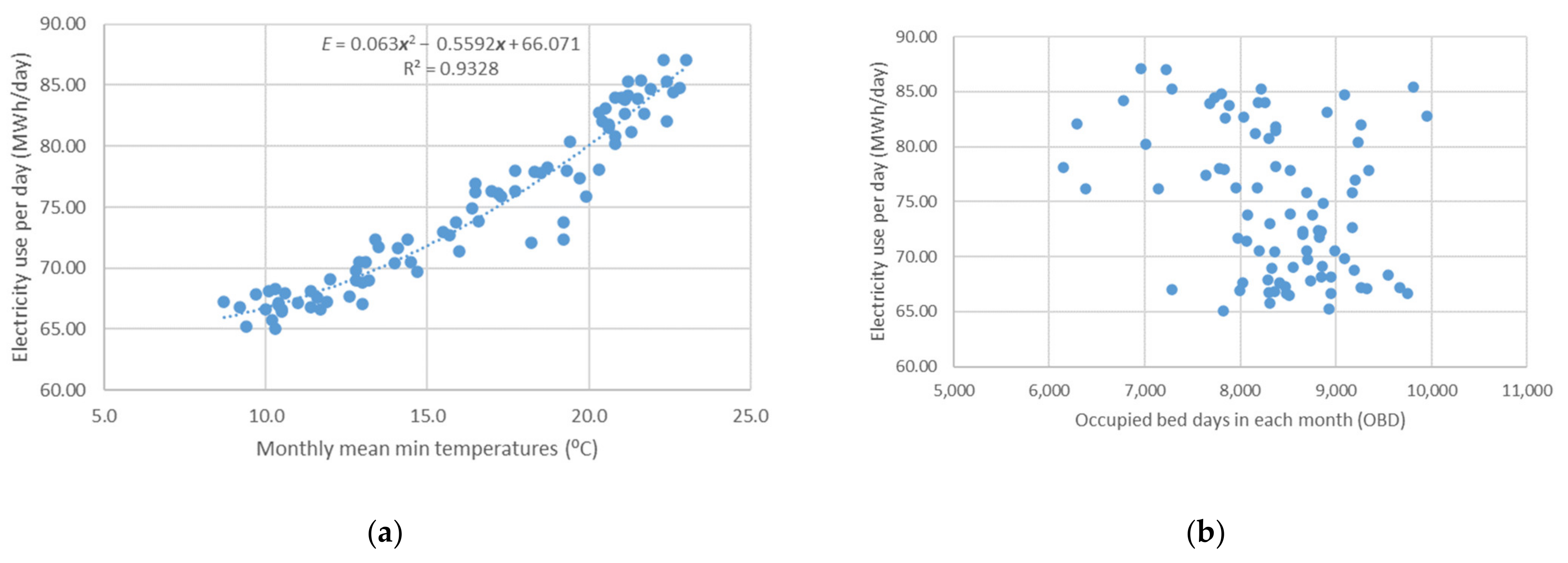
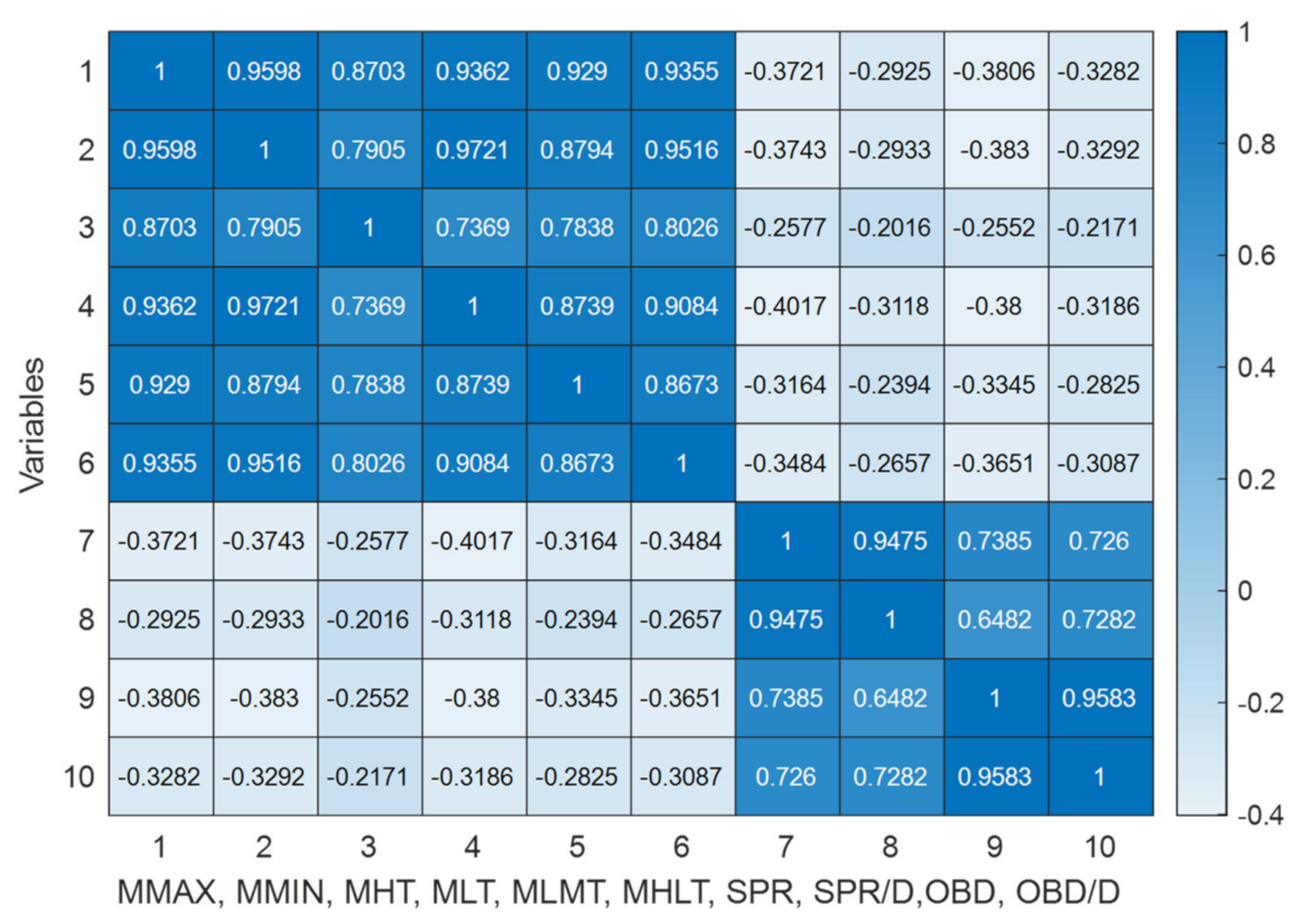
3.2. Correlation Study
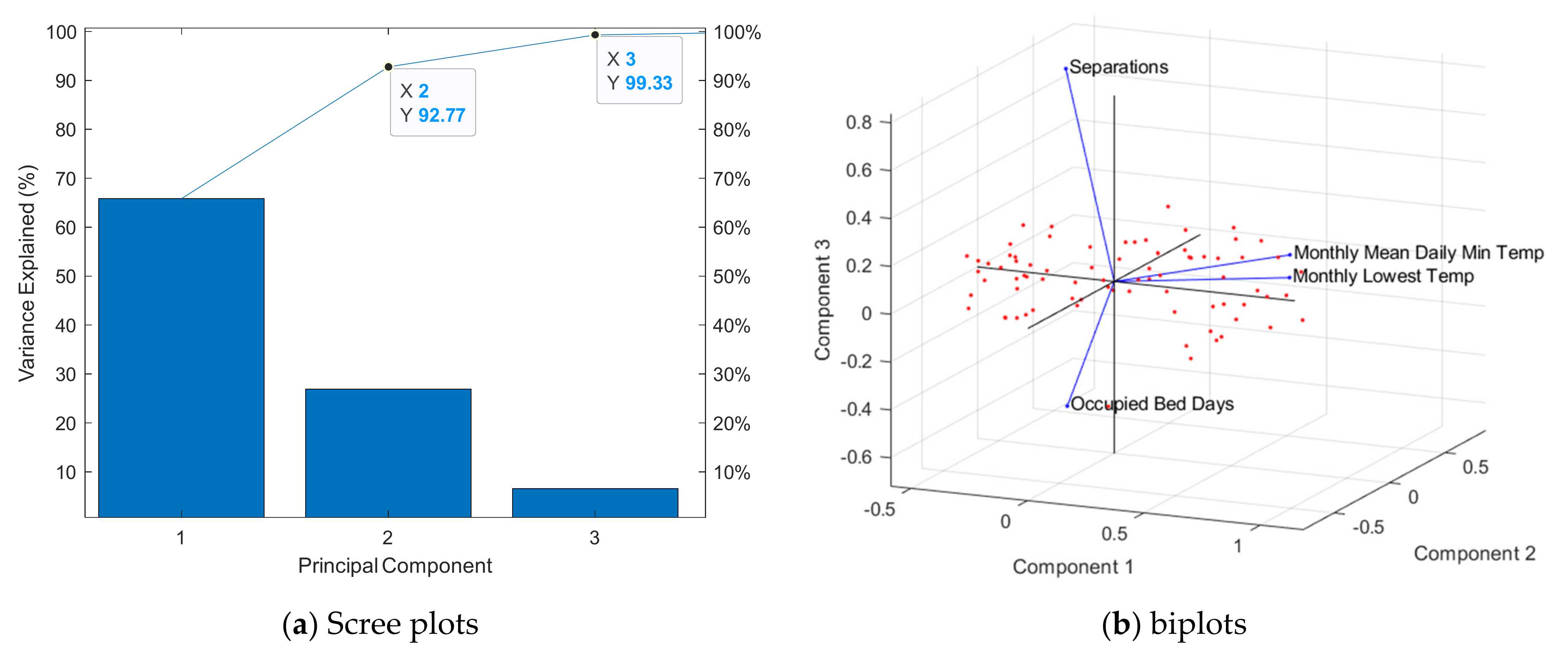
3.3. Principal Component Analysis
3.4. Regressions
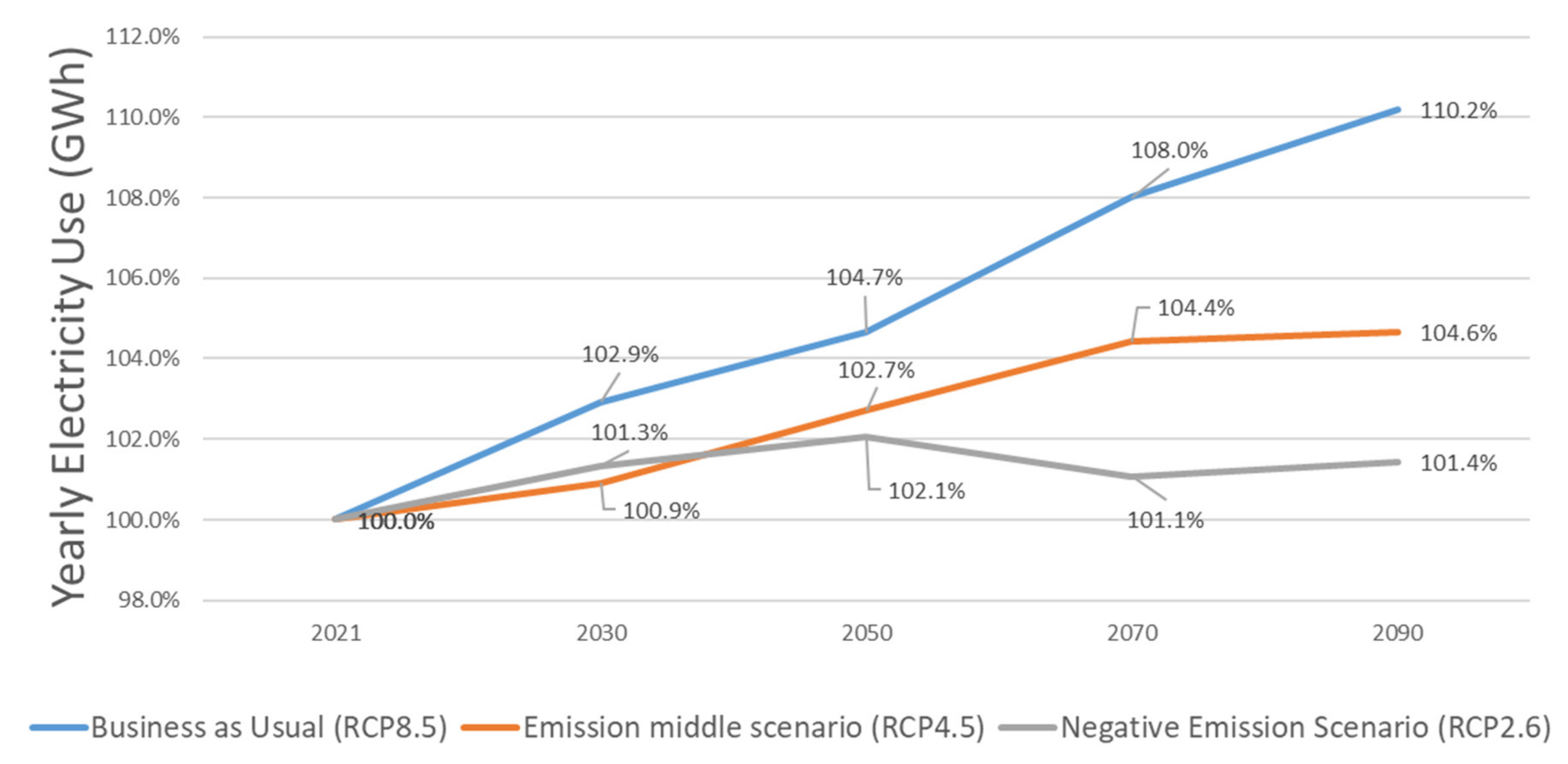
3.5. Forecast into 2030–2090 Scenarios
4. Discussion
4.1. Implication for Operational Expenditure
4.2. Implication for Renewable Energy
4.3. Implication for Policy and Future Developments
- For the case study, cooling is the dominant HVAC operation mode; electricity is the energy source for cooling. The major hospital is built with concrete and steel structures. Cooling to remove occupants’ metabolic load would probably be much less than the cooling needs for buildings’ thermal mass in the warm climate.
- The HVAC settings in hospitals are typically determined by standards and regulations based on health, safety, and clinical reasons. The HVAC is typically centrally controlled, with little potential for patients and clinicians to change the thermostat settings. This particular hospital is air-conditioned 24-7 and uses 100% fresh air. This case study provides evidence from another angle to support [12]: occupancy may not be as significant as occupants’ behaviour in influencing energy use.
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Acronyms | Description |
| PCC | Pearson Correlation Coefficient |
| PCA | Principal Component Analysis |
| NN | Neural Network |
| LR | Linear Regression |
| CSIRO | The Commonwealth Scientific and Industrial Research Organisation |
| OBD | Occupied Bed Days in a Calendar Month |
| OBD/D | Occupied Bed Days per Day in a Calendar Month |
| SPR | Separations in a Calendar Month |
| SPR/D | Separations per Day in a Calendar Month |
| MMAX | Monthly Mean Daily Maximum Temperature |
| MMIN | Monthly Mean Daily Minimum Temperature |
| MHT | Monthly Highest Temperature |
| MLT | Monthly Lowest Temperature |
| MLMT | Monthly Lowest Daily Maximum Temperature |
| MHLT | Monthly Highest Daily Minimum Temperature |
| RCP | Representative Concentration Pathway |
| SVD | Singular Value Decomposition |
| RMSE | Root Mean Squared Error |
References
- Australian Institute of Health and Welfare Data Table: Hospital Resources 2018–2019. Available online: https://www.aihw.gov.au/reports-data/myhospitals/content/data-downloads (accessed on 9 May 2022).
- Xia, B.; E, J.; Chen, Q.; Buys, L.; Yigitcanlar, T.; Susilawati, C. Understanding Spatial Distribution of Retirement Villages: An Analysis of the Greater Brisbane Region. Urban Sci. 2021, 5, 89. [Google Scholar] [CrossRef]
- Miller, W.F.; Liu, A.; Crompton, G.; Ma, Y. Healthcare Sector Energy Baseline and Key Performance Indicators; Australian Institute of Refrigeration, Air-Conditioning and Heating (AIRAH): Brisbane, Australia, 2020. [Google Scholar]
- Building Energy Use in NSW Public Hospitals; New South Wales Government: Sydney, Australia, 2013.
- Karliner, J.; Slotterback, S.; Boyd, R.; Ashby, B.; Steele, K. Health Care’s Climate Footprint How the Health Sector Contributes to the Global Crisis and Opportunities for Action—Green Paper Number One; Health Care without Harm: Reston, VA, USA, 2019. [Google Scholar]
- Health Care Without Harm. Arup Australia Health Sector Emissions Fact Sheet; Health Care without Harm: Reston, VA, USA, 2018. [Google Scholar]
- Malik, A.; Lenzen, M.; McAlister, S.; McGain, F. The Carbon Footprint of Australian Health Care. Lancet Planet. Health 2018, 2, e27–e35. [Google Scholar] [CrossRef] [Green Version]
- Victorian Auditor-General’s Report Australia (Ed.) Energy Efficiency in the Health Sector; Victorian Government: Melbourne, Australia, 2012.
- Anand, P.; Deb, C.; Ke, Y.; Yang, J.; Cheong, D.; Sekhar, C. Occupancy-Based Energy Consumption Modelling Using Machine Learning Algorithms for Institutional Buildings. Energy Build. 2021, 252, 111478. [Google Scholar] [CrossRef]
- Zhan, S.; Chong, A. Building Occupancy and Energy Consumption: Case Studies across Building Types. Energy Built Environ. 2021, 2, 167–174. [Google Scholar] [CrossRef]
- Liu, A.; Miller, W.; Chiou, J.; Zedan, S.; Chen, X.; Susilawati, C. How Is Occupancy Related to Energy Use in Healthcare Buildings? In Proceedings of the 10th IEEE PES Innovative Smart Grid Technologies Conference—Asia, Brisbane, QLD, Australia, 5–8 December 2021; Saha, T.K., Ed.; IEEE: Brisbane, Australia, 2021. [Google Scholar]
- Ahn, K.-U.; Park, C.-S. Correlation between Occupants and Energy Consumption. Energy Build. 2016, 116, 420–433. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, Q.; Hong, T.; Kang, C. Review of Smart Meter Data Analytics: Applications, Methodologies and Challenges. IEEE Trans. Smart Grid 2018, 10, 3125–3148. [Google Scholar] [CrossRef] [Green Version]
- Liu, A.; Miller, W.; Cholette, M.E.; Ledwich, G.; Crompton, G.; Li, Y. A Multi-Dimension Clustering-Based Method for Renewable Energy Investment Planning. Renew. Energy 2021, 172, 651–666. [Google Scholar] [CrossRef]
- Bawaneh, K.; Ghazi Nezami, F.; Rasheduzzaman, M.; Deken, B. Energy Consumption Analysis and Characterization of Healthcare Facilities in the United States. Energies 2019, 12, 3775. [Google Scholar] [CrossRef] [Green Version]
- Watts, N.; Adger, W.N.; Agnolucci, P.; Blackstock, J.; Byass, P.; Cai, W.; Chaytor, S.; Colbourn, T.; Collins, M.; Cooper, A.; et al. Health and Climate Change: Policy Responses to Protect Public Health. Lancet 2015, 386, 1861–1914. [Google Scholar] [CrossRef]
- Pencheon, D.; Rissel, C.E.; Hadfield, G.; Madden, D.L. Health Sector Leadership in Mitigating Climate Change: Experience from the UK and NSW. In New South Wales Public Health Bulletin; CSIRO: Sydney, Australia, 2009; Volume 20, pp. 173–176. [Google Scholar] [CrossRef] [Green Version]
- Nematchoua, M.K.; Yvon, A.; Kalameu, O.; Asadi, S.; Choudhary, R.; Reiter, S. Impact of Climate Change on Demands for Heating and Cooling Energy in Hospitals: An in-Depth Case Study of Six Islands Located in the Indian Ocean Region. Sustain. Cities Soc. 2019, 44, 629–645. [Google Scholar] [CrossRef]
- Liu, A.; Miller, W.F. Healthcare Living Laboratories: Queensland Children’s Hospital—Energy Baseline Data; Australian Institute of Refrigeration, Air-Conditioning and Heating (AIRAH): Brisbane, Australia, 2020. [Google Scholar]
- NABERS. Energy and Water for Hospitals: Rules for Collecting and Using Data; The National Australian Built Environment Rating System (NABERS): Sydney, Australia, 2017.
- Australian Bureau of Meterology Climate Data Online. Available online: http://www.bom.gov.au/climate/data/ (accessed on 15 June 2021).
- Trindade, F.C.L.; Ochoa, L.F.; Freitas, W. Data Analytics in Smart Distribution Networks: Applications and Challenges. In Proceedings of the 2016 IEEE Innovative Smart Grid Technologies—Asia (ISGT-Asia), Melbourne, Australia, 28 November–1 December 2016; pp. 574–579. [Google Scholar]
- Ma, Z.; Yan, R.; Nord, N. A Variation Focused Cluster Analysis Strategy to Identify Typical Daily Heating Load Profiles of Higher Education Buildings. Energy 2017, 134, 90–102. [Google Scholar] [CrossRef] [Green Version]
- Liu, A.L.; Shafiei, M.; Ledwich, G.; Miller, W.; Nourbakhsh, G.; Liu, L.; Shafiei, M.; Ledwich, G.; Miller, W.; Nourbakhsh, G. Correlation Study of Residential Community Demand with High PV Penetration. In Proceedings of the Australasian Universities Power Engineering Conference, Melbourne, Australia, 19–22 November 2017; Volume 2017, p. 6. [Google Scholar]
- Li, K.; Hu, C.; Liu, G.; Xue, W. Building’s Electricity Consumption Prediction Using Optimized Artificial Neural Networks and Principal Component Analysis. Energy Build. 2015, 108, 106–113. [Google Scholar] [CrossRef]
- Lolli, F.; Gamberini, R.; Regattieri, A.; Balugani, E.; Gatos, T.; Gucci, S. Single-Hidden Layer Neural Networks for Forecasting Intermittent Demand. Int. J. Prod. Econ. 2017, 183, 116–128. [Google Scholar] [CrossRef]
- Bennett, C.; Stewart, R.A.; Beal, C.D. ANN-Based Residential Water End-Use Demand Forecasting Model. Expert Syst. Appl. 2013, 40, 1014–1023. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Dong, Z.; Ding, L.; Petersen, H.; Qiu, Z.; Chen, G.; Prasad, D. Interpretable Memristive LSTM Network Design for Probabilistic Residential Load Forecasting. IEEE Trans. Circuits Syst. I Regul. Pap. 2022, 69, 1–14. [Google Scholar] [CrossRef]
- Yildiz, B.; Bilbao, J.I.; Dore, J.; Sproul, A.B. Recent Advances in the Analysis of Residential Electricity Consumption and Applications of Smart Meter Data. Appl. Energy 2017, 208, 402–427. [Google Scholar] [CrossRef]
- Hu, M.; Xiao, F.F.; Jørgensen, J.B.; Li, R. Price-Responsive Model Predictive Control of Floor Heating Systems for Demand Response Using Building Thermal Mass. Appl. Therm. Eng. 2019, 153, 316–329. [Google Scholar] [CrossRef]
- Ren, Z.; Tang, Z.; James, M. Projected Weather Files for Building Energy Modelling—User Guide; CSIRO: Canberra, Australia, 2022.
- IPCC. Climate Change 2014: Synthesis Report; Intergovernmental Panel on Climate Change (IPCC): Geneva, Switzerland, 2014. [Google Scholar]
- Foo, G. Climate Change: Impact on Building Design and Energy Final Report; DeltaQ: Canberra, Australia, 2020. [Google Scholar]
- Liu, A.; Miller, W.F. Healthcare Living Laboratories: Queensland Children’s Hospital—Operation Manual and Baseline Data; Queensland University of Technology: Brisbane, Australia, 2020. [Google Scholar]
- Australian Institute of Health and Welfare Australian Hospital Peer Groups Appendix C: Alphabetical Listing of Public and Private Hospitals by Peer Group 2019. Available online: https://www.aihw.gov.au/reports/hospitals/australian-hospital-peer-groups/data (accessed on 9 May 2022).
- Reserve Bank of Australia. Australia’s Inflation Target; Reserve Bank of Australia: Sydney, Australia, 2017.
- Ma, Y.; Saha, S.C.; Miller, W.; Guan, L. Parametric Analysis of Design Parameter Effects on the Performance of a Solar Desiccant Evaporative Cooling System in Brisbane, Australia. Energies 2017, 10, 849. [Google Scholar] [CrossRef] [Green Version]
- Liu, A.; Miller, W. Healthcare Living Laboratories: Queensland Children’s Hospital—Exergenics QCH Chiller System Digital Twin and Optimisation; Australian Institute of Refrigeration, Air-Conditioning and Heating (AIRAH): Brisbane, Australia, 2021. [Google Scholar]
- Burch, H.; Anstey, M.H.; McGain, F. Renewable Energy Use in Australian Public Hospitals. Med. J. Aust. 2021, 215, 160–163. [Google Scholar] [CrossRef]
- Cortese, T.T.P.; Almeida, J.F.S.D.; Batista, G.Q.; Storopoli, J.E.; Liu, A.; Yigitcanlar, T. Understanding Sustainable Energy in the Context of Smart Cities: A PRISMA Review. Energies 2022, 15, 2382. [Google Scholar] [CrossRef]
- Chen, X.; Qu, K.; Calautit, J.; Ekambaram, A.; Lu, W.; Fox, C.; Gan, G.; Riffat, S. Multi-Criteria Assessment Approach for a Residential Building Retrofit in Norway. Energy Build. 2020, 215, 109668. [Google Scholar] [CrossRef]
- Guidelines for Sustainability in Capital Works—Creating Healthier Resilient Buildings for a Changing Climate; Victoria State Government: Melbourne, Australia, 2020.
- Liu, A.; Miller, W. Healthcare Living Laboratories: Queensland Children ’s Hospital: Technology Evaluation Report for Exergenics’ Optimised Chiller Staging; Queensland University of Technology: Brisbane, Australia, 2022. [Google Scholar]
- Panteli, M.; Mancarella, P. Influence of Extreme Weather and Climate Change on the Resilience of Power Systems: Impacts and Possible Mitigation Strategies. Electr. Power Syst. Res. 2015, 127, 259–270. [Google Scholar] [CrossRef]
- Moazami, A.; Nik, V.M.; Carlucci, S.; Geving, S. Impacts of Future Weather Data Typology on Building Energy Performance—Investigating Long-Term Patterns of Climate Change and Extreme Weather Conditions. Appl. Energy 2019, 238, 696–720. [Google Scholar] [CrossRef]
- Queensland Government. Queensland State Budget 2021–2022. Available online: https://www.treasury.qld.gov.au/resource/state-budget-2021-22/ (accessed on 1 February 2022).
- Evans, M.; Belusko, M.; Taghipour, A.; Liu, M.; Keane, P.F.; Nihill, J.; Amin, R.; Liu, A.; Assaf, J.; Lau, T.; et al. RACE for 2030 CRC Research Theme B3 Electrification & Renewables to Displace Fossil Fuel Process Heating Opportunity Assessment Final Report; University of South Australia: Adelaide, Australia, 2021. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Description | Units |
|---|---|---|
| 1 | Monthly electricity use | Kilowatt-hours (kWh) |
| 2 | Daily maximum temperatures | Degree Celsius (°C) |
| 3 | Daily minimum temperatures | Degree Celsius (°C) |
| 4 | Monthly separations | Separations (SPR) |
| 5 | Monthly occupied bed days | Occupied bed days (OBD) |
| Future Scenario Names | Description | Pathways |
|---|---|---|
| 2030 | representing a typical year between 2020 and 2040 | |
| 2050 | representing a typical year between 2040 and 2060 | |
| 2070 | representing a typical year between 2060 and 2080 | |
| 2090 | representing a typical year between 2080 and 2100 |
| No. | Types | Monthly Mean Daily Electricity Use vs. | PCC | p-Values |
|---|---|---|---|---|
| 1 | Temperature variables | Monthly mean daily maximum temperatures (MMAX) | 0.932 | 5.320 × 10−38 |
| 2 | Monthly mean daily minimum temperatures (MMIN) | 0.956 | 1.626 × 10−45 | |
| 3 | Monthly highest temperatures (MHT) | 0.775 | 5.397 × 10−18 | |
| 4 | Monthly lowest temperatures (MLT) | 0.938 | 2.317 × 10−39 | |
| 5 | Monthly lowest daily maximum temperature (MLMT) | 0.849 | 2.113 × 10−24 | |
| 6 | Monthly highest daily minimum temperature (MHLT) | 0.922 | 1.423 × 10−35 | |
| 7 | Occupancy variables | Separations in each calendar month (SPR) | −0.300 | 0.006 |
| 8 | Separations per day in each calendar month (SPR/D) | −0.224 | 0.041 | |
| 9 | Occupied bed days in each calendar month (OBD) | −0.331 | 0.002 | |
| 10 | OBD per day in each calendar month (OBD/D) | −0.279 | 0.010 |
| No. | Description | RMSE | MAE |
|---|---|---|---|
| 1 | 1st order polynomial with MMIN | 2.6639 | 1.9587 |
| 2 | 1st order polynomial with MMIN and OBD | 2.8670 | 1.9970 |
| 3 | 1st order polynomial with MMIN and SPR | 2.7079 | 1.9611 |
| 4 | 2nd order polynomial with MMIN | 2.3618 | 1.4807 |
| 5 | 2nd order polynomial with MMIN and OBD | 2.6299 | 1.7080 |
| 6 | 2nd order polynomial with MMIN and SPR | 2.3974 | 1.5322 |
| 7 | ANN with MMIN (10 neurons) | 1.8093 | 1.4593 |
| 8 | ANN with MMIN and OBD (15 neurons) | 2.3234 | 1.8113 |
| 9 | ANN with MMIN and SPR (11 neurons) | 2.0346 | 1.5951 |
| Climate Scenario Names | Description | Emission Business as Usual (RCP8.5) | Emission Middle Scenario (RCP 4.5) | Emission Negative Scenario (RCP2.6) |
|---|---|---|---|---|
| 2021 | Yearly electricity use (GWh) | 26.846 (base) | ||
| 2030 | Typical yearly use between 2020 and 2040 (GWh) | 27.632 | 27.089 | 27.206 |
| Increase compared to 2021 | 2.9% | 0.9% | 1.3% | |
| 2050 | Typical yearly use between 2040 and 2060 (GWh) | 28.094 | 27.572 | 27.397 |
| Increase compared to 2021 | 4.7% | 2.7% | 2.1% | |
| 2070 | Typical yearly use between 2060 and 2080 (GWh) | 28.995 | 28.033 | 27.133 |
| Increase compared to 2021 | 8.0% | 4.4% | 1.1% | |
| 2090 | Typical yearly use between 2080 and 2100 (GWh) | 29.579 | 28.093 | 27.230 |
| Increase compared to 2021 | 10.2% | 4.6% | 1.4% | |
| Climate Scenarios | Business as Usual (RCP8.5) a,b | Emission Middle Scenario (RCP4.5) a,b | Negative Emission Scenario (RCP2.6) a,b | Savings Comparing RCP2.6 to RCP8.5 |
|---|---|---|---|---|
| 2030 | $147,255 | $45,602 | $67,501 | $79,754 |
| 2050 | $383,318 | $223,028 | $169,246 | $214,073 |
| 2070 | $1,081,181 | $597,236 | $144,658 | $936,523 |
| 2090 | $2,253,117 | $1,027,949 | $316,407 | $1,936,710 |
| Energy | 2016/17 | 2017/18 | 2018/19 |
|---|---|---|---|
| National baseline renewables | 15.7% | 17.0% | 24.0% |
| Total hospital energy consumed | 4,132,162 MWh | 4,213,694 MWh | 4,121,911 MWh |
| Hospital renewable energy produced | 13,651 MWh | 18,350 MWh | 94,415 MWh |
| Hospital energy % renewable | 0.33% | 0.44% | 2.29% |
| Climate Scenarios | Business as Usual (RCP8.5) a | Emission Middle Scenario (RCP4.5) a | Negative Emission Scenario (RCP2.6) a |
|---|---|---|---|
| 2030 | 513 | 159 | 235 |
| 2050 | 815 | 474 | 360 |
| 2070 | 1402 | 775 | 188 |
| 2090 | 1783 | 814 | 250 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, A.; Ma, Y.; Miller, W.; Xia, B.; Zedan, S.; Bonney, B. Energy Analysis and Forecast of a Major Modern Hospital. Buildings 2022, 12, 1116. https://doi.org/10.3390/buildings12081116
Liu A, Ma Y, Miller W, Xia B, Zedan S, Bonney B. Energy Analysis and Forecast of a Major Modern Hospital. Buildings. 2022; 12(8):1116. https://doi.org/10.3390/buildings12081116
Chicago/Turabian StyleLiu, Aaron, Yunlong Ma, Wendy Miller, Bo Xia, Sherif Zedan, and Bruce Bonney. 2022. "Energy Analysis and Forecast of a Major Modern Hospital" Buildings 12, no. 8: 1116. https://doi.org/10.3390/buildings12081116