1. Introduction
Hospital buildings are complex facilities with different needs regarding health, prevention, and care. Therefore, the starting point for any kind of design choice should always be the extreme fragility of patients. Hospitals also represent important nodes in the territorial services network and should be designed as such: safe and welcoming places, both in terms of the quality of the services provided and for the functionality of their spaces [
1].
Many environmental factors contribute to the achievement of the desired quality and affect the health of patients [
2,
3]: indoor air quality, good natural ventilation, and the quality of natural light, as well as aspects related to the quality of healthcare services and the concept of patient-centered care [
4]. In particular, light makes it possible to perceive the quality of living and care environments, affects human behaviors and has a direct and indirect influence on mood and cognitive processes [
5]. Indeed, natural light, as a factor identified among those that would require more study and research [
6], is the specific focus of this work.
Important studies have shown through evidence how the extra-visual effects of light on the human body plays a decisive role on physiology, on psychology, and on the ability to generate conditions of well-being in humans [
7], and have linked natural lighting with the circadian rhythm [
8,
9], responsible for the regulation of many daily activities (e.g., energy metabolism, feeding times, and endocrine and immune functions with related pathological conditions) [
10]. Exposure to natural light during the day inhibits the production of melatonin, allowing the regulation of the wake–sleep rhythm [
11,
12], especially for bedridden or elderly people [
13].
Regarding healthcare buildings and specifically patient rooms, it has been shown that most patients prefer natural light [
14,
15,
16] because it has specific patterns of time variations in color, contrast, and luminance of surfaces, which are difficult to achieve with artificial devices [
17]. In any case, the achievement of adequate lighting levels—both quantitative and qualitative—must be guaranteed in the patient rooms in relation to general lighting conditions (100 lx) or to the performance of specific activities, such as reading (300 lx) or observation of a patient by personnel (250 lx). Higher lighting conditions are instead required for other technologically intensive healthcare environments, such as intensive care rooms (e.g., 1000 lx for carrying out examination and treatment activities) and for which daylight and access to the outside views are key factors to improve the healing environment for patients and working conditions for healthcare providers [
18]. Even more, in operating theaters general lighting must be maintained in an adequate range of values (not less than 1000 lx) [
19].
The paper focuses on patient rooms, where appropriate levels of natural and artificial lighting can help to reduce depression [
20] and anxiety, improve sleep and rest rhythm, and shorten the length of stay for patients with mental illness [
21], whereas a too high level of lighting may worsen the health conditions of the patients (e.g., 2000–3000 lx may increase the anxiety levels in patients with dementia) [
22].
Further positive effects of natural light have also been demonstrated on staff productivity [
23]. In a survey conducted in a hospital environment on access to natural light [
24], 70% of the medical staff rated the increase in natural light as having a positive impact on their work life. Another study by CABE [
25] produced similar findings: an improved physical environment has a significant influence on the nurses’ performance in their work and has a positive impact on their recruitment and retention.
However, there are still few studies that consider the influence of design variables linked to the environmental and technological characteristics of hospitalization spaces with specific reference to natural light [
26,
27], whereas some studies focus on the selection of appropriate glazing specifications and on how the adoption of wider openings can result in significant energy savings and lower costs, as well as in strong positive effects on patients and staff well-being [
28].
In addition, other variables are important, such as the photometric characteristics of the finishing materials of floors, walls, ceilings, and the features and placement of furnishings, which can play a key role in determining the quality of natural light. Ultimately, the characteristics of natural light may depend strongly on the geometry, morphology, and properties of the various materials that light radiation intercepts on its path.
Therefore, the overall objective of this paper is to determine how the quality of natural light can be affected by the morphological, dimensional, and furnishing characteristics of hospital rooms and then to propose possible design strategies for efficient and effective use of light.
Specifically, this paper proposes the results of research funded by Sapienza University of Rome, referring to the development of a methodology for the evaluation of all significant variables that affect natural light during the use of hospital rooms, to serve as a basis for simulated solutions that are subsequently evaluated according to physical variable quantities including daylight factor, illuminance, color rendering index, etc., selecting those that can demonstrate appreciable improvements over ante operam natural light conditions.
The daylight quality assessment was tested on a sample of patient rooms of a thoracic surgery department as a case study, diversified by visual comfort conditions. The experimentation involved the elaboration of a set of improvement solutions. These alternative design solutions have been obtained by considering specific areas such as interior finishes, furnishings, and exterior fixtures with related shading systems and devices, and selecting those with greater impact on light quality factors.
2. Materials and Methods
2.1. Materials
The connection between the knowledge of how the buildings were designed and used and the decisional aspect of planning and construction is represented by a group of pre-design activities related to interventions known as pre- and post-occupancy evaluation. The results of studies on usage (or anticipated) performance can shed light on the ‘functioning’ and management of existing buildings, generate new knowledge on how users interact with space, and provide feedback on key decisions to make in the design and construction process [
29].
In particular, the evaluation of natural lighting levels in inpatient rooms falls within the broader field of building performance evaluation (BPE) methodologies [
30], which involve evaluation activities downstream of each phase (from briefing to design, to execution, and to use) to retrieve information (making feedback, etc.), and to introduce changes in decision making, as well as physical and organizational arrangements that bring improvements in the future (for feedforward, etc.) [
31].
Pre-occupancy evaluation methodologies have been applied [
32,
33] using building modeling and performance simulation tools in inpatient rooms to obtain feedback that can guide the design phase of improvement interventions and verify the effectiveness of the proposed solutions. Such performance feedback also represents valuable input to support evidence-based design [
34]. In this specific case, the evaluated performance covered natural light and basic minimum requirements for specific physical quantities, highlighting for each parameter the different impact on patient health in an average care room.
The assessment methodology was developed by following the six steps briefly shown in
Figure 1 [
35].
The first phase started with a study of the fundamental variables for the evaluation of natural light quality in a given space. For this reason, the minimum requirements to be met in an inpatient room were defined and sorted into four categories: temporal light patterns, spatial patterns, quantity, and spectral quality of light. Specific health effects were related to each of these categories (
Figure 2) [
36,
37].
Temporal patterns of light: the circadian stimulus (
Figure 3) [
38], i.e., the melatonin suppression percentage during the day (which in a healthy individual is about 40%) that must be achieved to control sleep–wake rhythms; and vitamin D production, ensured by a minimum of 3–6 h of indoors daylight exposure.
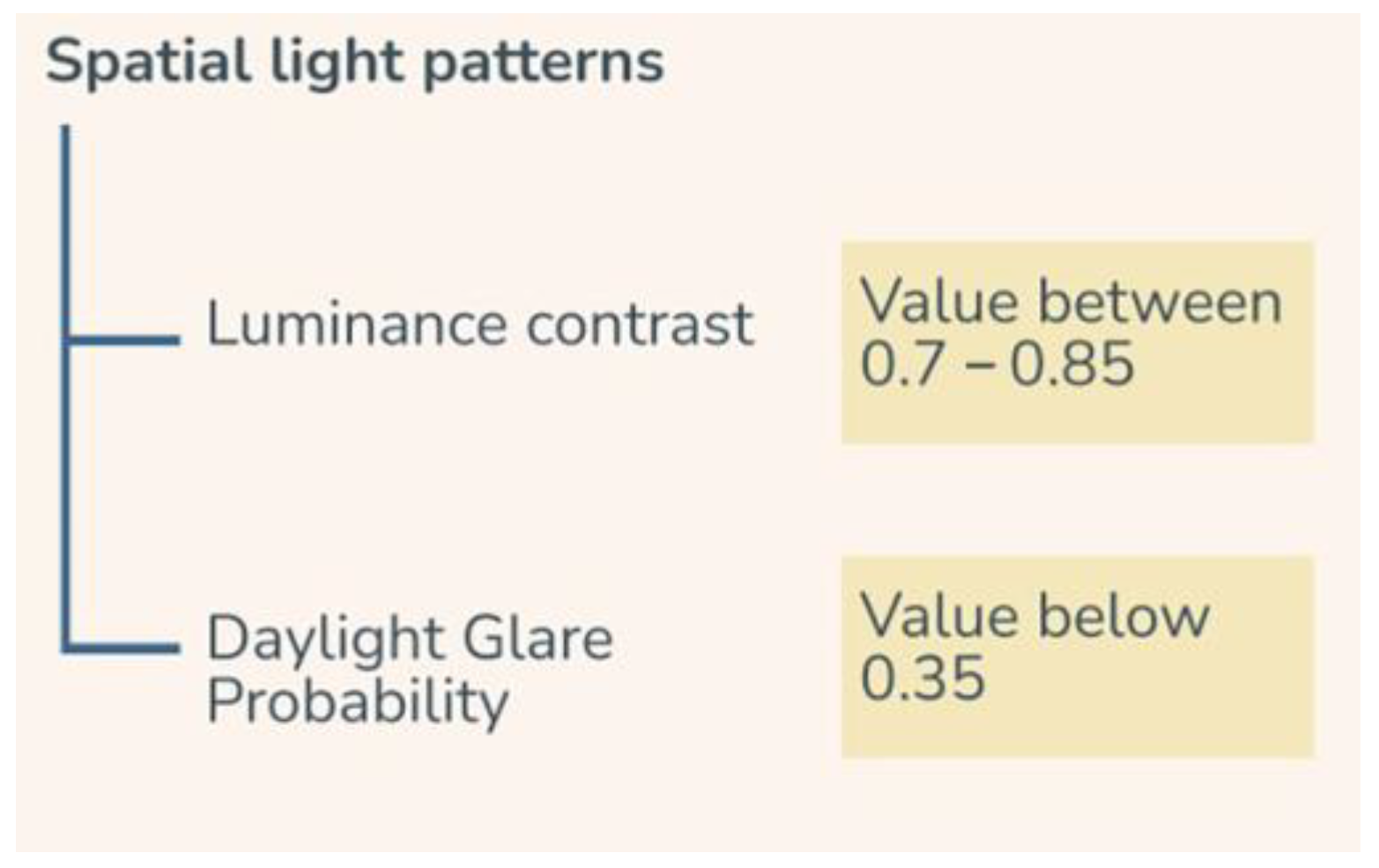
Spatial patterns of light: they are defined through glare, which in turn is measured through three quantities: luminance contrast, daylight glare probability, and unified glare rating (
Figure 4). Luminance contrast must be between 0.7 and 0.85 so that glare does not occur in the field of view. This can also be ensured by daylight glare probability and by unified glare rating, which estimate glare probability for natural and artificial light, respectively [
39].
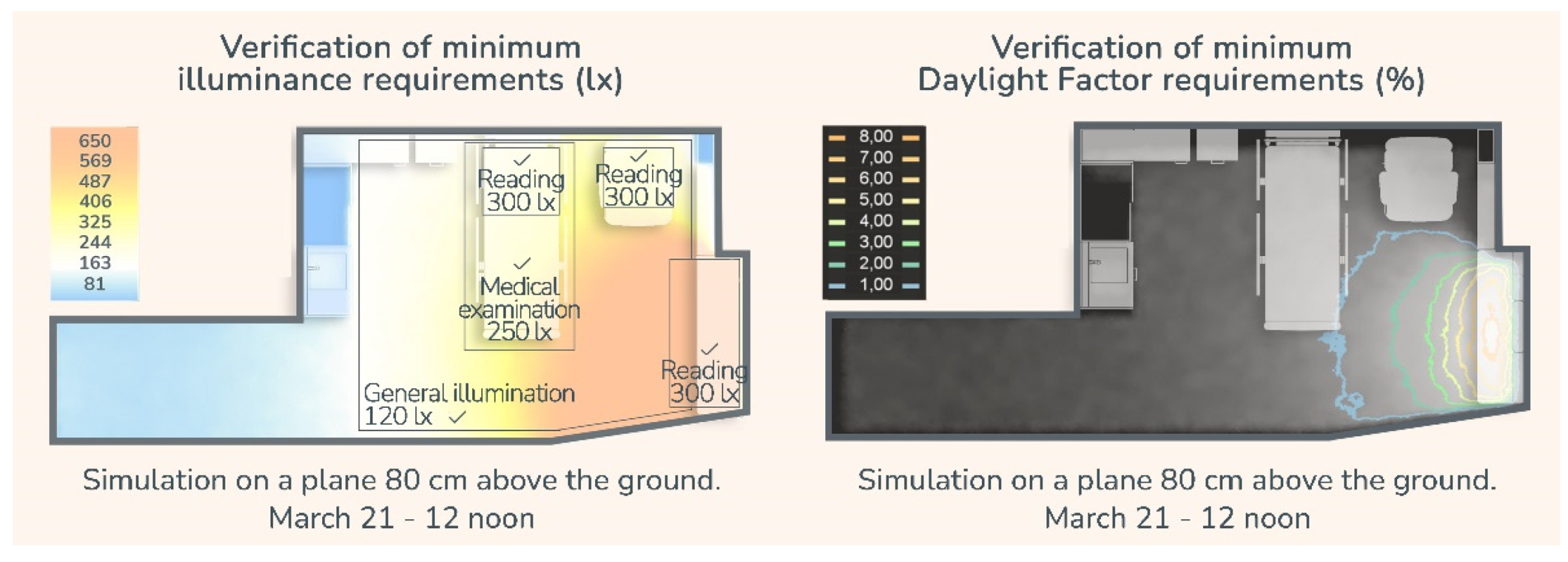
Light quantity: the requirements to be measured are daylight factor (at least 3%) and illuminance (lx optimal levels vary according to specific activities) [
40,
41]. These ensure good visibility conditions for users and, thus, their performance and well-being (
Table 1).
Spectral quality of light: the requirements are colorimetric parameters such as color rendering index and correlated color temperature of light sources. The color rendering index (CRI) (
Table 2) measures the capacity of a light source to accurately reproduce the colors of the object it illuminates, while correlated color temperature (CCT) (
Table 3) is a numerical value used to measure the color characteristics of a light source on a spectrum ranging from warm colors to cool colors, with values referred to as Kelvin degrees (K) [
19].
Other factors that contribute to the assessment of the light environment in the patient room were also examined such as the latitude of the location, topographical or anthropogenic obstructions, building and room geometry, and orientation.
Window characteristics were also included among the variables to be evaluated for design purposes: proportions and the physical and geometric properties of the components (frame and glass) that greatly affect the amount of incoming light. The shading system as a function of orientation and possible redirection systems of light for a more uniform distribution in space was also considered.
Special consideration was given to the reflectance values of finishing surfaces. Those recommended by the Illuminating Engineering Society and used as a reference for this study are as follows: above 80% for ceilings, between 50 and 70% for walls, between 20 and 40% for floors, and between 25 and 45% for furniture [
19].
These reference values guided the second phase of the study: the selection of a collection of technical solutions that meet the requirements identified for use within a patient room, ensuring adequate light comfort conditions though their light reflectance value (LRV). The collection is organized into categories and subcategories:
Finishes: (1a) floors, (1b) walls, (1c) suspended ceilings, (1d) interior doors;
Furniture coating: (2a) opaque furniture coating, (2b) glossy furniture coating;
Windows: (3a) glass; (3b) exterior fixtures, (3c) shading systems, (3d) films and filters.
For each of the analyzed solutions, only colors and textures that conformed to the predetermined reflectance indexes were considered, in addition to the mandatory durability, safety, comfort, and sustainability performances in a healthcare setting (
Figure 5).
2.2. Methods
The development of the evaluation made use of field research conducted in the third phase: a number of inpatient rooms were selected within the Thoracic and Cardiovascular Surgery Department of the Policlinico Universitario di Tor Vergata in Rome, exploring different natural light conditions and internal layout. Poorly designed finishes in terms of colors and textures affected both, as well as obsolete furniture and fixtures.
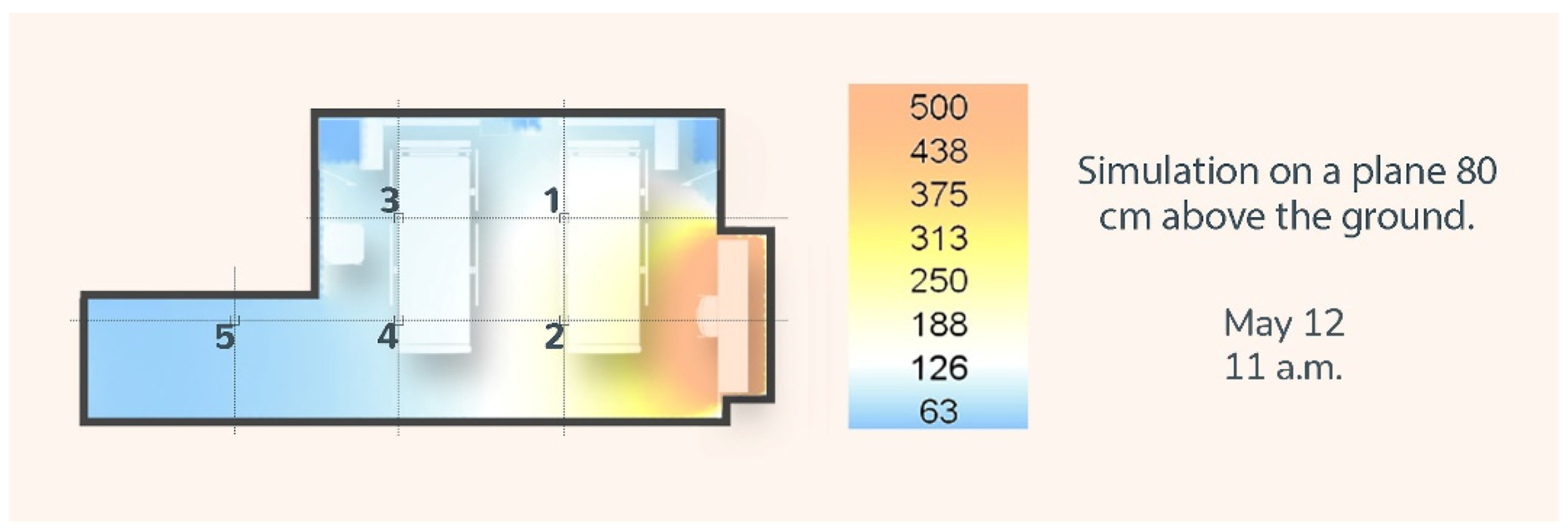
The phase of direct detection of natural light conditions, carried out with a “testo 545” light meter (resolution 1 lx (0 to 32,000 lx)), was preceded by 3D modeling of the actual state and simulation of the relevant conditions. The tools used were specific Grasshopper plug-ins (Ladybug and Honeybee) and Velux.
The results obtained were compared with the actual light conditions measured on site, using a five-fixed-point grid within the individual chambers, on a plane lying at the level of the patient bed. A difference of approximately 30% emerged between the measured and simulated data, which was taken into account for the verification of the minimum requirements (
Figure 6;
Table 4). This 30% difference is likely to be generated by non-optimal measurement conditions, especially the non-contemporaneity of the measurements made regarding the indoor versus outdoor illuminance levels, and the degree of accuracy of the input data [
35].
This phase brought out criticalities for both rooms regarding the minimal requirements of temporal patterns, such as insufficient circadian stimulus for the patient in room 1; light quality, such as insufficient and excessive illuminance in room 1 and room 2, respectively; spatial patterns, for example the critical luminance contrasts caused by the finishing material choice or room 2’s glare issue; and spectral quality, which can be linked to each material’s reflectance and its overall effect on the perception of indoor space.
The results obtained from the evaluation of all the variables that affect light in the wardroom, and from the compliance with the minimum requirements, allowed the identification of the possible improvement design proposals for the fourth phase, which were structured into the same groups of features as the collection of solutions (1—finishes, 2—furnishings, and 3—exterior fixtures).
The design choices were then supported by the collection. In the fifth phase, three technical alternatives were formulated for each area, subsequently evaluated in the sixth phase through further simulations, taking into consideration those that show evidence of improved visual comfort quality, which were also verified in terms of technical, financial, and logistical feasibility.
The selected solutions together generated a guiding project for the technological and functional reorganization of the patient room, later compared with the assessment of the ante operam layout. The achievement of appreciable improvement of lighting conditions means that the solutions can be incorporated into the executive project; otherwise, the process starts again with the evaluation of new proposals.
3. Results
The methodology has been tested on two in-patient rooms in a hospital in Rome, chosen as a case study for this research. The University Polyclinic of Tor Vergata is situated within a university campus and was built in the 1990s in an area southeast from the center of Rome. It consists of a 4-story concrete slab generally dedicated to diagnostic areas, while inpatient rooms are located in the two 11-story towers occupying the south and west areas of the building. The location of these rooms is shown in
Figure 7. They are both in tower 6, which occupies the southern portion of the building. The criteria by which the wards were chosen is based on very different natural light conditions (room 1 is facing south and room 2 is facing east) and on different layouts.
Climatic analyses based on the local climate data showed that the south façade receives twice as much annual solar radiation as the east façade. Furthermore, the surrounding environment is substantially devoid of other tall buildings or natural obstacles, which simplifies the simulation process. This also means that all the lighting differences between the two rooms are likely to be caused by their own architecture.
Room 1 (19.48 square meters) has an unsatisfactory aero-illuminant ratio (the window area to floor area ratio is less than 1/8) and shows evident criticalities in terms of pathways and natural light distribution, despite its favorable exposure.
Room 2, on the other hand, is larger (24 square meters) and has a strong glare problem, which is particularly apparent during field surveys.
3.1. Room 1 (South Facing)
From the ante operam simulations data, the critical points concern illuminance levels: the illuminance values obtained not only do not meet the minimum requirements but are also unevenly distributed within the room because of the thick window opening (
Figure 8).
Furthermore, there are obvious visual discomfort problems when analyzing luminance contrasts, which are very strong because of the reflectance of the materials. The dark-colored window frame and the glossy floor and wall finishes generate glare throughout the year, especially on the wall opposite the hospital beds [
42] (
Figure 9).
The first improvement was the transformation of the room from a double bed to a single bed, which was agreed to by the hospital’s health management. A reconfiguration/selection of furnishings followed: the bed is positioned in a barycentric position, accessible on three sides, with an equipped wall and a sanitation area for health personnel and easily accessible storage. It is also raised off the floor to facilitate cleaning. On the opposite side of the room, there is a visitor’s area with a reclining chair, a charging station for electronic devices, and a folding table, so as not to obstruct the entry of light and approach to the window (
Figure 10).
To overcome the poor distribution of light in the room, an inexpensive but effective solution was the placement of an opaque but highly reflective plasterboard panel at the boarding, which greatly increases the illuminance values in the room. In particular, it ensures that all the necessary illuminance requirements are achieved, both in the bed area and for the visitor, as well as the general illuminance conditions (
Figure 11).
The second area of design experimentation concerned the choice of finishing materials (scope 1). This represents a predominant area for mitigating luminance contrasts and thus glare risks for patients. Three different technical alternatives were envisaged, selected from the products studied and systematized in the collection of technical solutions (
Figure 12).
3.1.1. Scope 1
It is evident that, in the first alternative, the glare at the entrance to the room is completely eliminated, but the patient’s viewpoint still presents discomfort. Furthermore, the recorded luminances improve compared to the starting condition, but remain low and uneven. In the second alternative, luminance values are higher and more uniform than in the first alternative. Conversely, the risk of glare remains, although diminished, during the winter solstice, when the sun is lower and penetrates deeper into the room. The third one has fairly strong luminance contrasts from both the entrance and patient perspectives, and luminances relative to surfaces are also poorly uniform and excessively low in places. From the evaluation of all variables influencing natural light, the choice of the second alternative therefore follows.
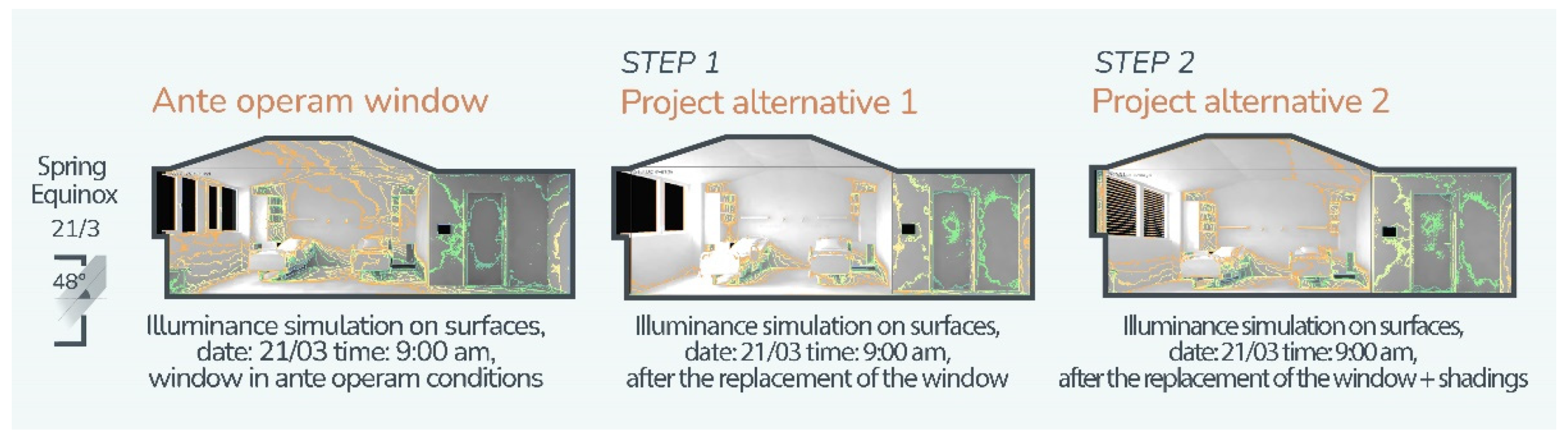
The last area of design experimentation relates to the improvement solutions on the window (scope 3), which is also considered the most expensive as its replacement would involve the entire hospital façade, thus requiring a considerable financial investment, as well as long implementation times that would require the suspension of health services. For this reason, the choice criterion for the two alternatives proceeds by levels of technical and financial feasibility and by successive steps that can be planned over time. In the first alternative (first step), the type of window frame and shading system (roller shutters) of the existing state are maintained. Only the replacement of the frame is carried out, choosing a thinner solution (from 10 cm to 6 cm). This allows the transparent surface area to be increased, a fundamental choice because of the insufficient illuminating air ratio that characterizes the room. The second step involves the installation of an internal and external light redirection system that works in an integrated manner with the high reflectance ceiling. To then counter the risk of glare without obstructing the view to the outside and the entry of diffuse light, a motorized adjustable louvre shading system was selected, which can be operated remotely by the patient (
Figure 13).
3.1.2. Scope 2
From the analysis of the illuminance on the surfaces on an annual basis, for each alternative, one can visually appreciate how progressing with the three alternatives results in increasingly better natural lighting conditions. It is for this reason that the last, best performing alternative was chosen for the guiding project.
3.1.3. Scope 3
The next step was to verify the functioning of the shading system to counter the risk of glare. First, the length, distance, and number of slats were taken into account for the annual percentage of shading to be verified. In addition, a new luminance analysis was carried out from the entrance and from the patient’s point of view, with very satisfactory results. In fact, the risk of glare is decreased and the luminance values have greater uniformity.
3.2. Room 2 (East-Facing)
The data obtained through the ante operam simulations and the field analysis show that the critical feature for this room is an uneven distribution of illuminance. The illuminance for the patient’s bed farthest from the window in fact turns out to be insufficient. For the patient closest to the window, the illuminance complies with the minimum requirements, but glare problems were detected throughout the year, especially in the morning hours (
Figure 14).
To carry out the pre-occupancy assessment, a number of improvement solutions were formulated and simulated for the three scopes.
In this case, scopes 1 and 2 (finishing materials and furniture) were considered at the same time. The simulations show the effects of a sloping ceiling with high reflectance, which, combined with a symmetrical arrangement of the furniture (scope 2), favor illuminance distribution. Several alternative configurations (suspended ceiling and furniture) were then evaluated, and the choice fell upon the one that manages to guarantee compliance with all requirements, with particular attention to the shadow effects in the most disadvantaged areas (
Figure 15).
For the critical issues related to luminance contrasts and glare, three intervention alternatives were developed referring to area 3 finishes (
Figure 16), which helped in solving the uniformity of natural light distribution but not glare.
Because of this, two project steps were assessed concerning the three-window scope, the first one by intervening only on the opaque part of the window frame by reducing its thickness. In the second one, the shading system is also replaced with a solution with adjustable slats integrated inside the double glazing. The quality of the glass also contributes to the improvement of visual comfort, since low emissivity glass integrated with a special adhesive film (selected from the phase 2 collection) for radiation control, which guarantees 84% reduction in glare, was selected for the assessment.
Scope 1, Finishing Materials
Alternative 1 shows very strong luminance contrasts, especially near the window. The solution involves the use of opaque materials that redistribute light without reflecting it directly, creating a brighter, glare-free environment. In particular, a ceiling with a very high LRV was chosen to be able to evenly distribute light within the room (uniform luminances).
In alternative 2, the use of light-colored finishes is evaluated to slightly attenuate the luminance contrast and to obtain high luminance values but not uniform luminances. Such finishes, however, do not fully resolve the risk of glare. This suggested a further improved design proposal for specific glare-shielding from the east.
In alternative 3, the choice of finishes turns out to generate higher luminances than the previous alternatives. Nonetheless, a strong inhomogeneity is detected, caused mainly by the high reflectance of the wall in front of the patients together with the HPL furniture with a semi-gloss finish, which decrease the lighting comfort.
Through the evaluation of the minimum requirements, alternative 1 turns out to be the most efficient, especially with regard to the uniformity of natural light distribution, although it does not solve the glare problem (
Figure 17).
4. Discussion
Comparing the design outcomes of the two rooms showed how factors such as the number of patients and window orientation not only tend to generate different criticalities and require specific design strategies but can also widely predict the quality of the finished design beforehand.
It is evident that room 1, having a single bed and being south facing, makes controlling the well-being parameters substantially easier than room 2. Although the results in the latter definitely highlight an improvement over the ante operam situation, the glare problem (a discomfort factor that is difficult to counteract without precluding the entry of natural light) and the necessary trade-off between privacy and natural lighting mean that rooms with this orientation suffer from a physiological disadvantage regarding comfort and a greater complexity from the design point of view.
Furthermore, the comparison of the post operam simulations of both rooms allows an appreciation of the greater effectiveness of the high-reflectance inclined planes that are orthogonal rather than parallel to the floor, a solution that again shows better results in the design of room 1.
The overall effect of the selected design options is easily shown through a comparison between pictures taken during the site inspection (ante operam) and post operam project renders. Each of the design choices contributes in fact to achieving optimal lighting comfort conditions. Comparing the ante operam and post operam conditions in both room 1 and room 2, it is shown how the most upfront difference is given by the finishing materials. Those present at the time of the inspection are inadequate not only in terms of light reflection (LRV index) but also because of the color of the light itself. The environments are aseptic, cold, and inhospitable, and these characteristics, combined with the discomfort generated by unmet physical requirements, contribute to increased stress levels for patients. Indeed, it is important to remember that design must take into account the humanization of spaces, which is inseparable from the mere achievement of minimum requirements. The requirement is for designed environments to adequately satisfy not only functional needs, but also the psycho-emotional nature of its users. This should now be considered increasingly essential, especially in the case of architecture intended for care and assistance. The approach to the design of socio-medical environments is no longer to be understood only in terms of the treatment of illnesses, but must be able to connect the demands of humanization with the set of information and knowledge acquired in the sphere of scientific research conducted in various disciplinary fields united by the interest in improving the conditions of patients and staff through the design of healthcare environments (medicine, environmental psychology, ergonomics, proxemics, sociology, and hospital hygiene). In particular, in the case of social and healthcare environments, it is believed that the psycho-social characteristics of spaces can have an effect on patients in terms of improving the clinical outcomes of illness and safety conditions, as well as on staff in terms of improving performance, and are also reflected in the effectiveness and quality of care [
43]. Reducing stressful conditions and situations by raising the environmental quality perceived by users has become imperative.
5. Conclusions
This paper proposed and validated a methodology for assessing the quality of natural light in hospital rooms based on pre-occupancy evaluation. In particular, the methodology was applied to simulated design solutions to measure the increments related to the physical variables that influence natural light in indoor environments. The performed simulations of the design solutions for the hospital rooms under analysis provided the necessary feedback to ensure the best comfort conditions for patients, as well as to support the decisions on the interventions to implement during the redevelopment of the hospital building.
The paper highlights the extent within which the morphological, dimensional, material, and furniture characteristics affect the level of natural lighting. In particular, the selection of the three scopes (1—finishes, 2—furnishings, and 3—exterior fixtures) was guided by the need to strictly act on the main elements of interior design. These elements have been demonstrated to have an impact on visual comfort, and they qualify the design choices also in relation to the usability and humanization requirements from a patient-centered perspective. In fact, room 1 has been transformed into a single room by proposing a new spatial configuration with the bed in a central position to favor privacy and usability, thus obtaining an area dedicated to the visitor (which was absent in the room’s ante operam configuration), with a reclining chair and a folding table in correspondence with the window (
Figure 18). The choice of material characteristics and the relative reflectance of the new furnishings and finishes (matt vinyl coating for the LRV 69% walls, linoleum for the LRV 35% floor, high reflectance plasterboard for the ceiling LRV 87%, acacia wood cladding for furniture LRV 55%, wood-effect laminate for doors LRV 63%, and eco-leather for textiles LRV 94%) determined an efficient use of natural light, improving the control of luminance contrasts and, therefore, the risk of unpleasant glaring effects for patients. Furthermore, it also contributed to defining a perceptually comfortable and emotionally positive space. In addition, the new design of the window and the motorized shading system have resulted in an increase in the glass surface, improving the window-to-floor ratio, but also the restorative potential of some environmental factors such as the external view over the natural surroundings. The evaluation of the post operam simulations related to the improving design solutions for room 1 showed that, with respect to the same day of the year and the same climatic conditions, the average illuminance passes from a value of 51 lx to one of 338 lx with a better distribution of light inside the space. This has positive repercussions on the patients’ conditions, on the organizational-functional aspects of the room, and on the perceptual aspects related to the quality of the care spaces.
Similarly, the same design approach was adopted for room 2 to ensure equal conditions for patients, both from the visual comfort and the organizational-functional perspective of the spaces (
Figure 19). To level off the imbalance between the natural light conditions of the two patients measured in the ante operam configuration, design solutions structured according to the three selected scopes were simulated and evaluated. Control of the reflectance of selected finishing materials and furnishings (water-based paint for walls LRV 71%, vinyl flooring LRV 22%, laminate finish for furniture LRV 44%, recycled imitation leather for textiles LRV 87%, HPL coating for LRV doors 60%, and high reflectance rock wool ceiling LRV 85%) allowed the deeper distribution of the light into the environment, counteracting unwanted glare issues through the use of opaque surfaces. At the same time, the dimensions and the morphological solutions adopted have allowed a more rational functional subdivision of the hospital room, so as to obtain the “family zone” missing in the ante operam, through flexible furniture anchored to the wall in front of the patients to facilitate verbal interaction. In the post operam simulation, with respect to the same day of the year and the same climatic conditions, these design solutions, together with the replacement of the frame with the modification of the scanning of the glass parts, resulted in an average level of illumination of 700 lx compared to the 559 lx measured in ante operam conditions. At the same time, in redesigning the furnishings and equipment of the hospital room, the need to reduce the perception of the environment as too “institutional” was also met by taking care of the camouflage of the equipment and plant terminals, thus positively acting on the psycho-emotional well-being of patients and family members.
The methodology of assessing natural light using ex ante simulation tools has therefore provided the necessary feedback for improved design solutions, though it can also offer new opportunities for patient-centered design, in an integrated perspective.
























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}