

In Vivo Monitoring of Acute and Intermittent Fatigue in Sport Climbing Using Near-Infrared Spectroscopy Wearable Biosensors
 , , ,
, , ,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Data Acquisition
2.2. General Measurement Procedure
2.3. Statistical Analysis
3. Results
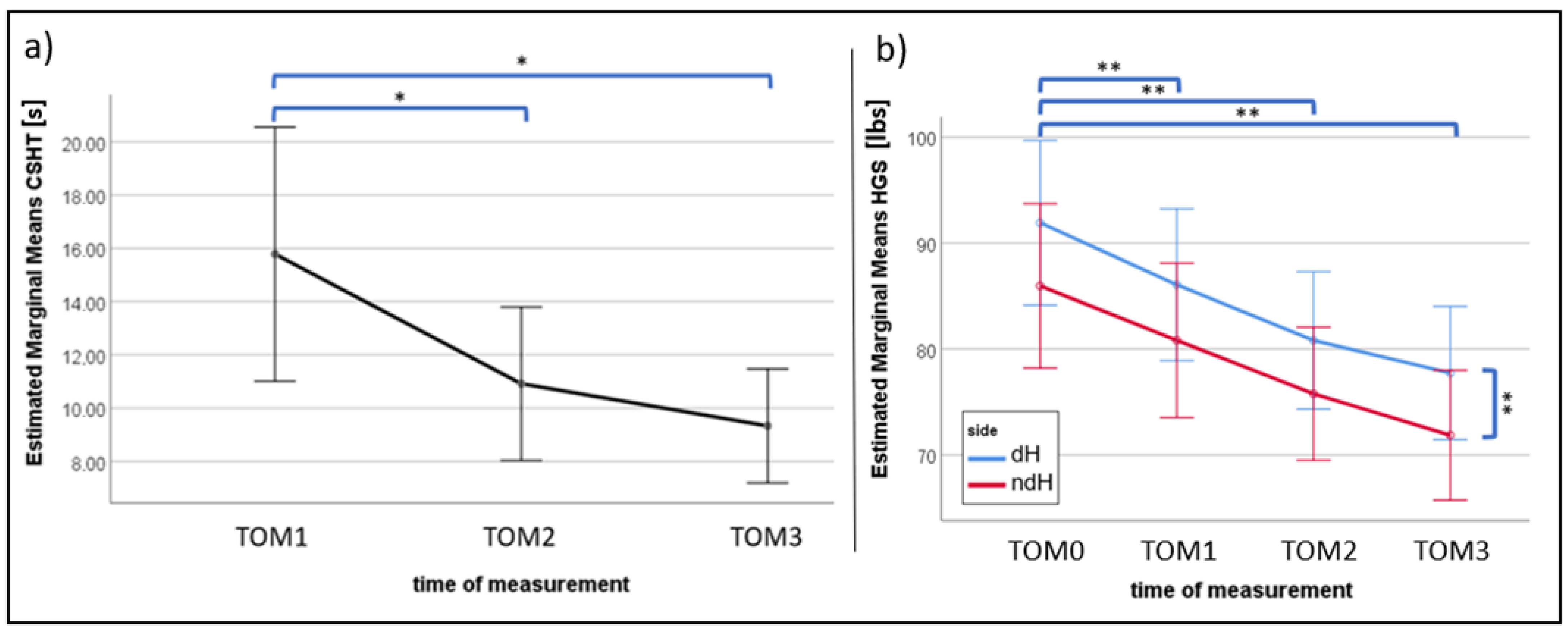
3.1. Research Question (a): Effects of Cumulative Fatigue on Maximal CSHT and HGS
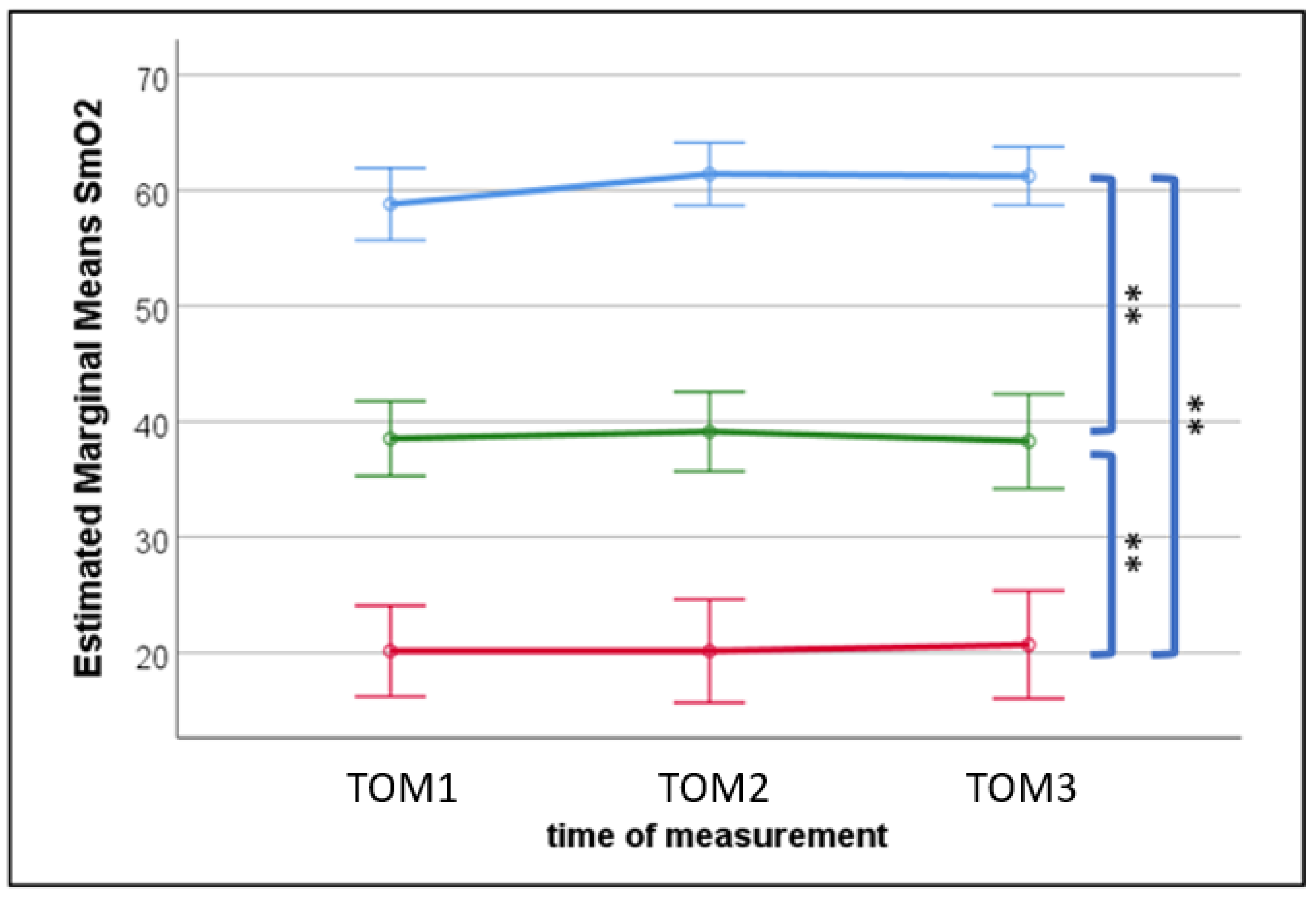
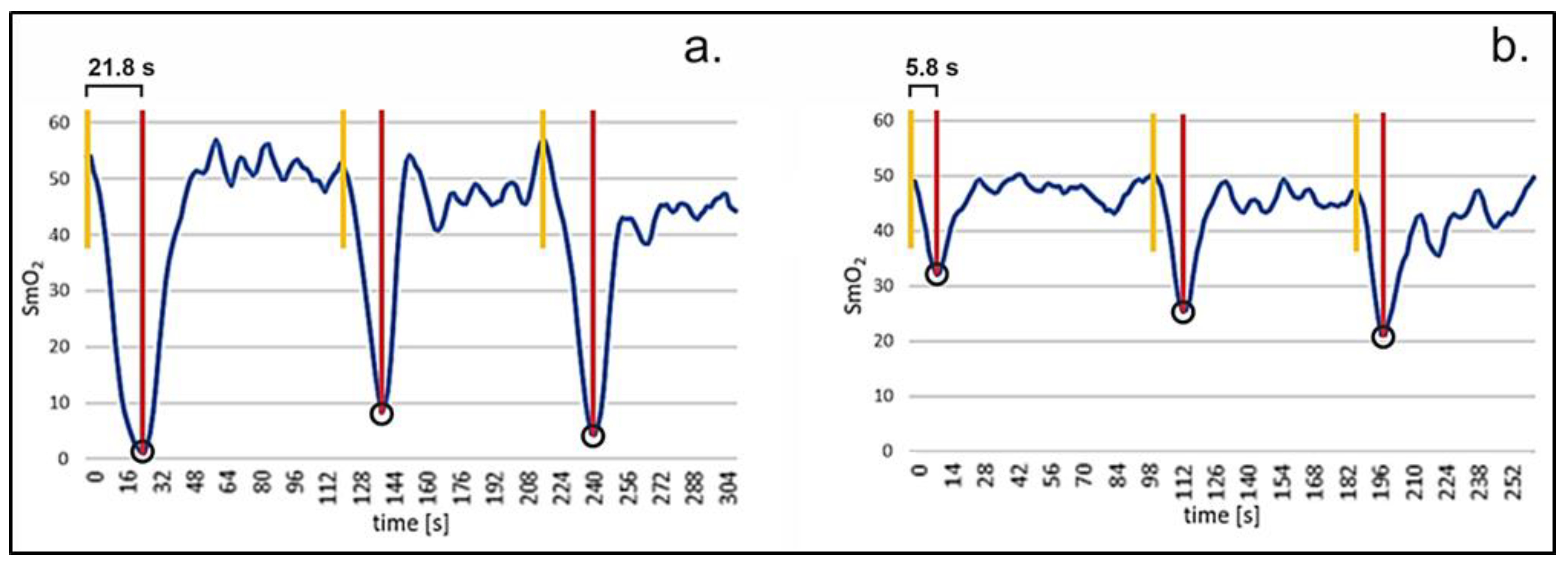
3.2. Research Question (b): Effects of Acute and Cumulative Fatigue on Muscle Oxidative Metabolism
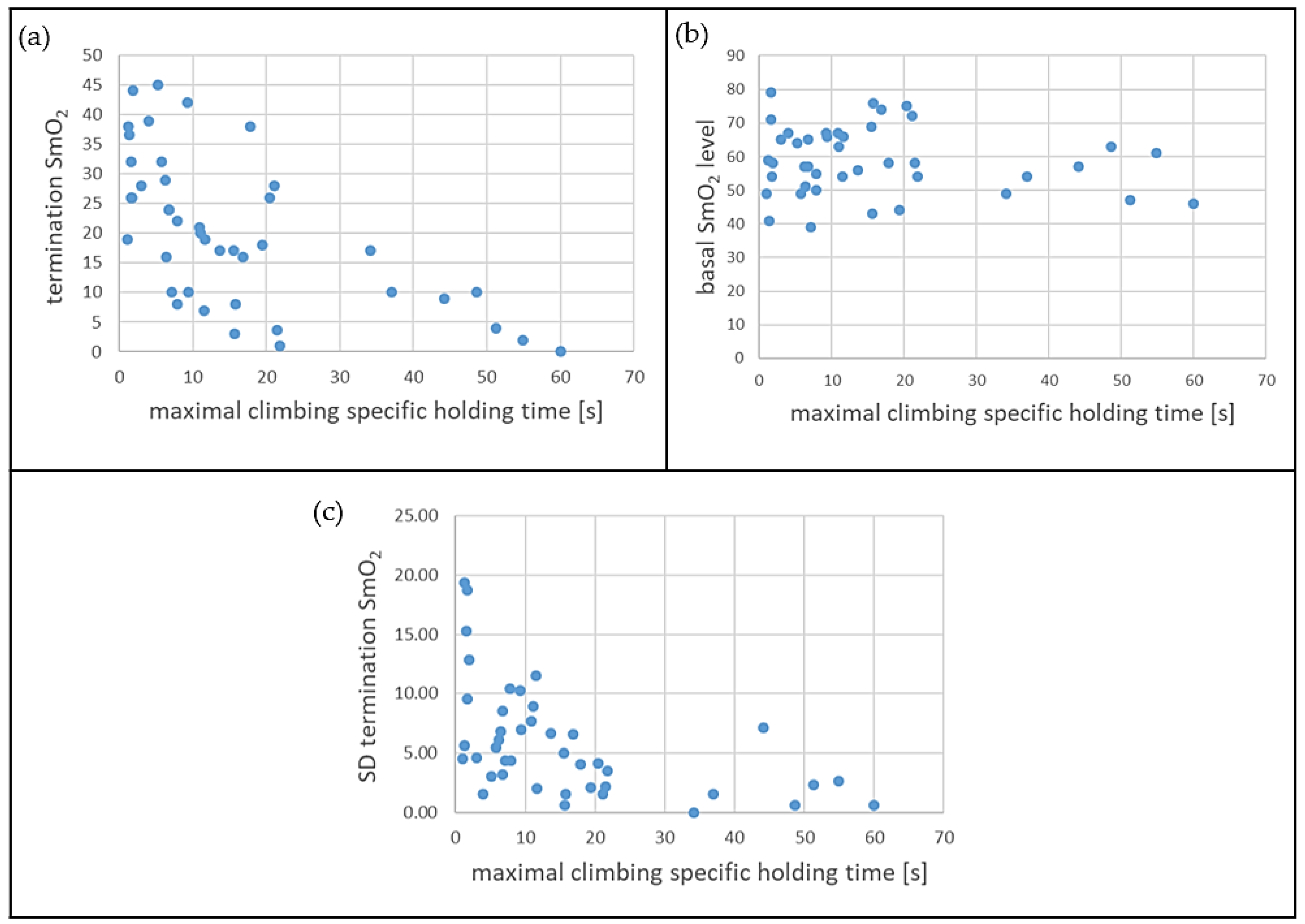
3.3. Research Question (c): Relationships between Different Levels of Maximal CSHTs and SmO2 Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- España-Romero, V.; Ortega Porcel, F.B.; Artero, E.G.; Jiménez-Pavón, D.; Gutiérrez Sainz, A.; Castillo Garzón, M.J.; Ruiz, J.R. Climbing time to exhaustion is a determinant of climbing performance in high-level sport climbers. Eur. J. Appl. Physiol. 2009, 107, 517–525. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, R.; Monaghan, L.; Masson, R.A.; Werner, A.K.; Caprez, T.S.; Johnston, L.; Kemi, O.J. Physical and Physiological Determinants of Rock Climbing. Int. J. Sports Physiol. Perform. 2020, 15, 168–179. [Google Scholar] [CrossRef] [PubMed]
- Baláš, J.; MrskoČ, J.; PanáČková, M.; Draper, N. Sport-specific finger flexor strength assessment using electronic scales in sport climbers. Sports Technol. 2014, 7, 151–158. [Google Scholar] [CrossRef]
- Dindorf, C.; Bartaguiz, E.; Dully, J.; Sprenger, M.; Merk, A.; Becker, S.; Fröhlich, M.; Ludwig, O. Evaluation of influencing factors on the maximum climbing specific holding time—An inferential statistical and machine learning approach. Funct. Morphol. Kinesiol. 2022, 7, 95. [Google Scholar] [CrossRef]
- Macdonald, G.A.; Manning, J.W.; Bodell, N.G.; Young, J.C.; Schilling, B.K.; Lee, S.-P.; Navalta, J.W. Acute Handgrip Fatigue and Forearm Girth in Recreational Sport Rock Climbers. Int. J. Exerc. Sci. 2022, 15, 834–845. [Google Scholar] [PubMed]
- Mencarini, E.; Leonardi, C.; Cappelletti, A.; Giovanelli, D.; De Angeli, A.; Zancanaro, M. Co-designing wearable devices for sports: The case study of sport climbing. Int. J. Hum.-Comput. Stud. 2019, 124, 26–43. [Google Scholar] [CrossRef]
- Watts, P.B.; Daggett, M.; Gallagher, P.; Wilkins, B. Metabolic response during sport rock climbing and the effects of active versus passive recovery. Int. J. Sports Med. 2000, 21, 185–190. [Google Scholar] [CrossRef]
- Ladha, C.; Hammerla, N.Y.; Olivier, P.; Plötz, T. ClimbAX. In Proceedings of the 2013 ACM International Joint Conference on Pervasive and Ubiquitous Computing (UbiComp’13), Zurich, Switzerland, 8–12 September 2013; Mattern, F., Santini, S., Canny, J.F., Langheinrich, M., Rekimoto, J., Eds.; ACM: New York, NY, USA, 2013; pp. 235–244, ISBN 9781450317702. [Google Scholar]
- Kosmalla, F.; Wiehr, F.; Daiber, F.; Krüger, A.; Löchtefeld, M. ClimbAware. In Proceedings of the 34th Annual CHI Conference on Human Factors in Computing Systems (CHI 2016), San Jose, CA, USA, 7–12 May 2016; Kaye, J., Druin, A., Lampe, C., Morris, D., Hourcade, J.P., Eds.; The Association for Computing Machinery: New York, NY, USA, 2016; pp. 1097–1108, ISBN 9781450333627. [Google Scholar]
- Hamaoka, T.; McCully, K.K.; Niwayama, M.; Chance, B. The use of muscle near-infrared spectroscopy in sport, health and medical sciences: Recent developments. Philos. Trans. R. Soc. 2011, 369, 4591–4604. [Google Scholar] [CrossRef]
- Crum, E.M.; O’Connor, W.J.; van Loo, L.; Valckx, M.; Stannard, S.R. Validity and reliability of the Moxy oxygen monitor during incremental cycling exercise. Eur. J. Sport Sci. 2017, 17, 1037–1043. [Google Scholar] [CrossRef]
- Muramatsu, Y.; Kobayashi, H. Assessment of local muscle fatigue by NIRS. In Proceedings of the 2013 Seventh International Conference on Sensing Technology (ICST), Wellington, New Zealand, 3–5 December 2013; IEEE: Wellington, New Zealand, 2013; pp. 1–4. [Google Scholar]
- Fryer, S.; Stoner, L.; Stone, K.; Giles, D.; Sveen, J.; Garrido, I.; España-Romero, V. Forearm muscle oxidative capacity index predicts sport rock-climbing performance. Eur. J. Appl. Physiol. 2016, 116, 1479–1484. [Google Scholar] [CrossRef]
- Feldmann, A.; Lehmann, R.; Wittmann, F.; Wolf, P.; Baláš, J.; Erlacher, D. Acute Effect of High-Intensity Climbing on Performance and Muscle Oxygenation in Elite Climbers. J. Sci. Sport Exerc. 2022, 4, 145–155. [Google Scholar] [CrossRef]
- Baláš, J.; Kodejška, J.; Krupková, D.; Hannsmann, J.; Fryer, S. Reliability of Near-Infrared Spectroscopy for Measuring Intermittent Handgrip Contractions in Sport Climbers. J. Strength Cond. Res. 2018, 32, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Woollings, K.Y.; McKay, C.D.; Emery, C.A. Risk factors for injury in sport climbing and bouldering: A systematic review of the literature. Br. J. Sports Med. 2015, 49, 1094–1099. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Amca, A.M.; Vigouroux, L.; Aritan, S.; Berton, E. The effect of chalk on the finger-hold friction coefficient in rock climbing. Sports Biomech. 2012, 11, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Ambrasat, J.; Schupp, J. Handgreifkraftmessung Im Sozio-Oekonomischen Panel (SOEP) 2006 und 2008; Deutsches Institut für Wirtschaftsforschung (DIW): Berlin, Germany, 2011. [Google Scholar]
- Mathiowetz, V.; Weber, K.; Volland, G.; Kashman, N. Reliability and validity of grip and pinch strength evaluations. J. Hand Surg. 1984, 9, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Philippe, M.; Wegst, D.; Müller, T.; Raschner, C.; Burtscher, M. Climbing-specific finger flexor performance and forearm muscle oxygenation in elite male and female sport climbers. Eur. J. Appl. Physiol. 2012, 112, 2839–2847. [Google Scholar] [CrossRef]
- Watts, P.B. Physiology of difficult rock climbing. Eur. J. Appl. Physiol. 2004, 91, 361–372. [Google Scholar] [CrossRef]
- Alomari, M.A.; Mekary, R.A.; Welsch, M.A. Rapid vascular modifications to localized rhythmic handgrip training and detraining: Vascular conditioning and deconditioning. Eur. J. Appl. Physiol. 2010, 109, 803–809. [Google Scholar] [CrossRef] [Green Version]
- Feldmann, A.M.; Erlacher, D.; Pfister, S.; Lehmann, R. Muscle oxygen dynamics in elite climbers during finger-hang tests at varying intensities. Sci. Rep. 2020, 10, 3040. [Google Scholar] [CrossRef] [PubMed]
- Bergua, P.; Montero-Marin, J.; Gomez-Bruton, A.; Casajús, J.A. Hanging ability in climbing: An approach by finger hangs on adjusted depth edges in advanced and elite sport climbers. Int. J. Perform. Anal. Sport 2018, 18, 437–450. [Google Scholar] [CrossRef]
- Baláš, J.; Pecha, O.; Martin, A.J.; Cochrane, D. Hand-arm strength and endurance as predictors of climbing performance. Eur. J. Sport Sci. 2012, 12, 16–25. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dindorf, C.; Bartaguiz, E.; Dully, J.; Sprenger, M.; Becker, S.; Fröhlich, M.; Ludwig, O. In Vivo Monitoring of Acute and Intermittent Fatigue in Sport Climbing Using Near-Infrared Spectroscopy Wearable Biosensors. Sports 2023, 11, 37. https://doi.org/10.3390/sports11020037
Dindorf C, Bartaguiz E, Dully J, Sprenger M, Becker S, Fröhlich M, Ludwig O. In Vivo Monitoring of Acute and Intermittent Fatigue in Sport Climbing Using Near-Infrared Spectroscopy Wearable Biosensors. Sports. 2023; 11(2):37. https://doi.org/10.3390/sports11020037
Chicago/Turabian StyleDindorf, Carlo, Eva Bartaguiz, Jonas Dully, Max Sprenger, Stephan Becker, Michael Fröhlich, and Oliver Ludwig. 2023. "In Vivo Monitoring of Acute and Intermittent Fatigue in Sport Climbing Using Near-Infrared Spectroscopy Wearable Biosensors" Sports 11, no. 2: 37. https://doi.org/10.3390/sports11020037