
Impact of a 5-Week Individualised Training Program on Physical Performance and Measures Associated with Musculoskeletal Injury Risk in Army Personnel: A Pilot Study

Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Procedures
2.4. Warm Up
2.5. Countermovement Jump Assessments
2.6. Balance Assessments
2.7. Plank Assessments
2.8. Push-Ups and Multistage Shuttle Test
2.9. Muscular Strength Assessments
2.10. Weight-Loaded March
2.11. Outcome Measures
2.12. Physical Training
2.13. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. BJSM 2020, 54, 1451. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, S.D.; Sinnott, A.M.; Krajewski, K.T.; Johnson, C.D.; Eagle, S.R.; LaGoy, A.D.; Beckner, M.E.; Beethe, A.Z.; Turner, R.; Lovalekar, M.; et al. Prevention of exertional lower body musculoskeletal injury in tactical populations: Protocol for a systematic review and planned meta-analysis of prospective studies from 1955 to 2018. Syst. Rev. 2018, 7, 73. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, K.M.; Spencer, V.; Fehl, N.; Carlos Poston, W.S. Mission essential fitness: Comparison of functional circuit training to traditional army physical training for active duty military. Mil. Med. 2012, 177, 1125–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westphalen, N. Rehabilitation in the Australian Defence Force. JMVH 2019, 27, 7–14. [Google Scholar]
- Lisman, P.J.; De la Motte, S.J.; Gribbin, T.C.; Jaffin, D.P.; Murphy, K.; Deuster, P.A. A systematic review of the association between physical fitness and musculoskeletal injury tisk: Part 1—Cardiorespiratory endurance. J. Strength Cond. Res. 2017, 31, 1744–1757. [Google Scholar] [CrossRef]
- Knapik, J.J. The importance of physical fitness for injury prevention: Part 1. J. Spec. Oper. Med. 2015, 15, 123–127. [Google Scholar] [CrossRef]
- De la Motte, S.J.; Gribbin, T.C.; Lisman, P.; Murphy, K.; Deuster, P.A. Systematic review of the association between physical fitness and musculoskeletal injury risk: Part 2-muscular endurance and muscular strength. J. Strength Cond. Res. 2017, 31, 3218–3234. [Google Scholar] [CrossRef]
- Trank, T.V.; Ryman, D.H.; Minagawa, R.Y.; Trone, D.W.; Shaffer, R.A. Running mileage, movement mileage, and fitness in male U.S. Navy recruits. Med. Sci. Sports Exerc. 2001, 33, 1033–1038. [Google Scholar] [CrossRef]
- Carstairs, G.L.; Ham, D.J.; Savage, R.J.; Best, S.A.; Beck, B.; Billing, D.C. A method for developing organisation-wide manual handling based physical employment standards in a military context. J. Sci. Med. Sport 2018, 21, 1162–1167. [Google Scholar] [CrossRef] [Green Version]
- Sharp, M.A.; Cohen, B.S.; Boye, M.W.; Foulis, S.A.; Redmond, J.E.; Larcom, K.; Hydren, J.R.; Gebhardt, D.L.; Canino, M.C.; Warr, B.J.; et al. U.S. Army physical demands study: Identification and validation of the physically demanding tasks of combat arms occupations. J. Sci. Med. Sport 2017, 20 (Suppl. S4), S62–S67. [Google Scholar] [CrossRef]
- Stockbrugger, B.G.; Reilly, T.J.; Blacklock, R.E.; Gagnon, P.J. Reliability of the individual components of the Canadian Armed Forces Physical Employment Standard. Appl. Physiol. Nutr. Metab. 2018, 43, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Knapik, J.J. The importance of physical fitness for injury prevention: Part 2. J. Spec. Oper. Med. 2015, 15, 112–115. [Google Scholar] [CrossRef] [PubMed]
- Kercher, V.M.; Kercher, K.; Bennion, T.; Yates, B.A.; Feito, Y.; Alexander, C.; Amaral, P.C.; Soares, W.; Li, Y.-M.; Han, J.; et al. Fitness trends from around the globe. ACSMs Health Fit. J. 2021, 25, 20–31. [Google Scholar] [CrossRef]
- Smith, C.; Doma, K.; Heilbronn, B.; Leicht, A. Effect of exercise training programs on physical fitness domains in military personnel: A systematic review and meta-analysis. Mil. Med. 2022, 187, 1065–1073. [Google Scholar] [CrossRef]
- Merrigan, J.J.; Stone, J.D.; Martin, J.R.; Hornsby, W.G.; Galster, S.M.; Hagen, J.A. Applying force plate technology to inform human performance programming in tactical populations. Appl. Sci. 2021, 11, 6538. [Google Scholar] [CrossRef]
- Hando, B.R.; Scott, W.C.; Bryant, J.F.; Tchandja, J.N.; Angadi, S.S. The use of force plate vertical jump scans to identify special warfare trainees at risk for musculoskeletal injury: A large cohort study. Am. J. Sports Med. 2022, 50, 1687–1694. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.; Doma, K.; Heilbronn, B.; Leicht, A. Reliability of force plate metrics during standard jump, balance, and plank assessments in military personnel. Mil. Med. 2022, 2022, usac387. [Google Scholar] [CrossRef]
- Mayberry, J.K.; Patterson, B.; Wagner, P. Improving vertical jump profiles through prescribed movement plans. J. Strength Cond. Res. 2018, 32, 1619–1626. [Google Scholar] [CrossRef]
- Kozinc, Ž.; Šarabon, N.; Kovčan, B.; Simenko, J.; Pori, P.; Vodičar, J.; Hadzic, V. Effects of 12-week full body resistance exercise on vertical jumping with and without military equipment in Slovenian Armed Forces. BMJ Mil. Health 2021. [Google Scholar] [CrossRef]
- Šimenko, J.; Kovčan, B.; Pori, P.; Vodičar, J.; Vodičar, M.; Hadžić, V. The relationship between army physical fitness and functional capacities in infantry members of the Slovenian Armed Forces. J. Strength Cond. Res. 2021, 35, 3506–3512. [Google Scholar] [CrossRef]
- Pontillo, M.; Sennett, B. Prediction of lower extremity injuries from vertical jump kinetic data in collegiate athletes. Med. Sci. Sports Exerc. 2019, 51, 950. [Google Scholar] [CrossRef]
- Laffaye, G.; Wagner, P.P.; Tombleson, T.I. Countermovement jump height: Gender and sport-specific differences in the force-time variables. J. Strength Cond. Res. 2014, 28, 1096–1105. [Google Scholar] [CrossRef] [PubMed]
- Mayberry, J.; Mullen, S.; Murayama, S. What can a jump tell us about elbow injuries in professional baseball pitchers? Am. J. Sports Med. 2020, 48, 1220–1225. [Google Scholar] [CrossRef] [PubMed]
- Léger, L.A.; Lambert, J. A maximal multistage 20-m shuttle run test to predict VO2max. Eur. J. Appl. Physiol. 1982, 49, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Heilbronn, B.E.; Doma, K.; Gormann, D.; Schumann, M.; Sinclair, W.H. Effects of periodized vs. nonperiodized resistance training on army-specific fitness and skills performance. J. Strength Cond. Res. 2020, 34, 738–753. [Google Scholar] [CrossRef]
- Pontillo, M.; Milic-Strkalj, I.; Sennett, B.J. Prediction of trunk injuries from core stability testing in collegiate athletes. Sports Orthop. Traumatol. 2021, 37, 338–342. [Google Scholar] [CrossRef]
- Troester, J.C.; Jasmin, J.G.; Duffield, R. Reliability of single-leg balance and landing tests in rugby union; prospect of using postural control to monitor fatigue. J. Sports Sci. Med. 2018, 17, 174–180. [Google Scholar]
- Pontillo, M.; Hines, S.M.; Sennett, B.J. Prediction of ACL injuries from vertical jump kinetics in divison 1 collegiate athletes. Int. J. Sports Phys. Ther. 2021, 16, 156–161. [Google Scholar] [CrossRef]
- Foster, C.; Florhaug, J.A.; Franklin, J.; Gottschall, L.; Hrovatin, L.A.; Parker, S.; Doleshal, P.; Dodge, C. A new approach to monitoring exercise training. J. Strength Cond. Res. 2001, 15, 109–115. [Google Scholar]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect size estimates: Current use, calculations, and interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [Green Version]
- Burley, S.D.; Drain, J.R.; Sampson, J.A.; Nindl, B.C.; Groeller, H. Effect of a novel low volume, high intensity concurrent training regimen on recruit fitness and resilience. J. Sci. Med. Sport 2020, 23, 979–984. [Google Scholar] [CrossRef] [PubMed]
- De la Motte, S.J.; Lisman, P.; Gribbin, T.C.; Murphy, K.; Deuster, P.A. Systematic review of the association between physical fitness and musculoskeletal injury risk: Part 3—Flexibility, power, speed, balance, and agility. J. Strength Cond. Res. 2019, 33, 1723–1735. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.E. The impact of duration on effectiveness of exercise, the implication for periodization of training and goal setting for individuals who are overfat, a meta-analysis. Biol. Sport 2016, 33, 309–333. [Google Scholar] [CrossRef]
- Hackshaw, A. Small studies: Strengths and limitations. Eur. Respir. J. 2008, 32, 1141. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CON (n = 9) | EXP (n = 8) | |
|---|---|---|
| Age (years) | 30.9 ± 9.4 | 24.9 ± 3.8 |
| Height (cm) | 172.7 ± 6.7 | 178.9 ± 9.3 |
| Mass (kg) | 78.4 ± 12.9 | 75.9 ± 9.5 |
| BMI (kg/m2) | 26.3 ± 4.0 | 23.8 ± 2.6 |
| CON (n = 5–9) | EXP (n = 7–8) | |||||
|---|---|---|---|---|---|---|
| Week 0 | Week 6 | Change (%) | Week 0 | Week 6 | Change (%) | |
| Muscular endurance | ||||||
| Push-ups in 60-s | 29.3 ± 8.5 | 31.1 ± 8.5 | 7.5 ± 10.8 | 37.4 ± 10.1 | 38.1 ± 13.9 | 0.8 ± 11.8 |
| Cardiorespiratory fitness | ||||||
| Predicted rate of oxygen consumption (mL/kg/min) | 41.5 ± 7.6 | 40.9 ± 6.2 | −0.5 ± 6.7 | 43.8 ± 3.5 | 43.9 ± 3.7 | 0.3 ± 4.6 |
| Muscular strength | ||||||
| Squat—3RM (kg) | 70.7 ± 13.0 | 83.9 ± 11.7 | 20.1 ± 14.2 | 82.9 ± 25.8 | 97.1 ± 29.1 | 17.9 ± 9.0 |
| Strict press—3RM (kg) | 39.3 ± 5.3 | 42.6 ± 3.8 | 9.1 ± 9.2 | 39.3 ± 9.3 | 43.9 ± 12.3 | 10.8 ± 9.4 |
| Deadlift—3RM (kg) | 98.8 ± 19.4 | 106.3 ± 17.7 | 8.4 ± 6.8 | 92.9 ± 26.7 | 111.4 ± 32.8 | 20.6 ± 11.9 † |
| Floor press—3RM (kg) | 63.1 ± 13.6 | 70.0 ± 12.2 | 12.4 ± 11.4 | 62.9 ± 21.0 | 67.9 ± 25.1 | 6.8 ± 7.8 |
| Occupational capacity | ||||||
| 5 km weight loaded march time (min) | 50.5 ± 1.4 | 47.9 ± 2.7 | −5.1 ± 3.0 | 44.1 ± 3.1 * | 43.8 ± 3.6 | −0.7 ± 4.0 * |
| CON (n = 7–9) | EXP (n = 7–8) | |||||
|---|---|---|---|---|---|---|
| Week 0 | Week 6 | Change | Week 0 | Week 6 | Change | |
| Two-leg CMJ | ||||||
| Sparta total score | 78.8 ± 4.9 | 76.7 ± 5.7 | −2.1 ± 4.3 | 78.1 ± 3.1 | 79.3 ± 2.0 | 1.1 ± 2.0 |
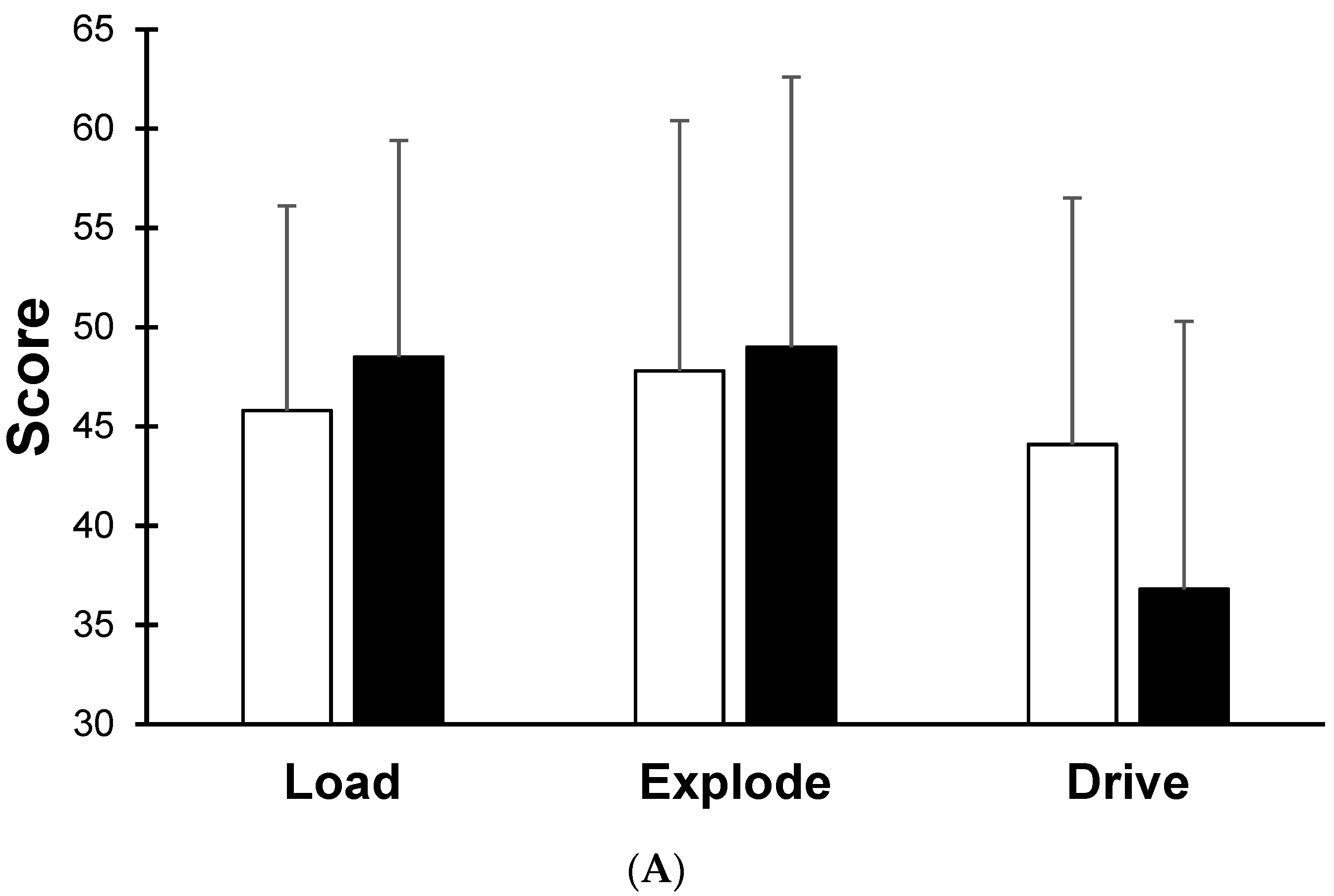
| Load score | 45.8 ± 10.3 | 48.5 ± 10.9 | 2.8 ± 4.0 | 40.8 ± 5.3 | 42.7 ± 2.4 | 1.8 ± 3.9 |
| Explode score | 47.8 ± 12.6 | 49.0 ± 13.6 | 1.2 ± 5.6 | 39.5 ± 4.9 | 43.7 ± 6.5 | 4.2 ± 5.9 |
| Drive score | 44.1 ± 12.4 | 36.8 ± 13.5 | −7.3 ± 9.2 | 51.2 ± 11.0 | 44.1 ± 9.6 | −7.1 ± 8.2 |
| Jump height (cm) | 37.3 ± 10.0 | 33.6 ± 8.8 | −8.9 ± 9.7 | 35.0 ± 8.2 | 34.4 ± 7.7 | −1.4 ± 9.4 |
| Injury risk score | 1.78 ± 1.56 | 1.89 ± 1.05 | 0.1 ± 1.5 | 1.50 ± 0.93 | 1.25 ± 0.71 | −0.3 ± 0.7 |
| One-leg dominant | ||||||
| Sparta total score | 66.1 ± 2.5 | 66.4 ± 3.0 | 0.3 ± 1.1 | 68.0 ± 1.8 | 67.1 ± 4.6 | −0.6 ± 5.5 |
| Load score | 41.0 ± 13.4 | 39.5 ± 11.6 | −1.5 ± 3.5 | 34.6 ± 4.2 | 36.7 ± 6.0 | 1.9 ± 7.5 |
| Explode score | 28.3 ± 11.3 | 29.9 ± 9.9 | 1.7 ± 4.7 | 21.9 ± 2.8 | 21.4 ± 6.7 | 0.0 ± 7.5 |
| Drive score | 32.7 ± 15.4 | 27.4 ± 13.3 | −5.3 ± 9.4 | 47.5 ± 5.4 | 57.0 ± 32.9 | 7.9 ± 37.4 |
| Jump height (cm) | 17.3 ± 3.5 | 17.3 ± 3.9 | 0.3 ± 10.7 | 17.9 ± 4.0 | 18.7 ± 4.6 | 4.1 ± 9.4 |
| Injury risk score | 2.14 ± 1.57 | 1.86 ± 1.57 | −0.3 ± 0.8 | 2.71 ± 1.38 | 3.57 ± 1.51 | 0.3 ± 2.4 |
| One-leg non-dominant | ||||||
| Sparta total score | 65.8 ± 1.8 | 65.1 ± 6.3 | −0.6 ± 6.5 | 67.9 ± 3.2 | 69.1 ± 3.1 | 1.3 ± 3.2 |
| Load score | 36.6 ± 8.4 | 38.3 ± 8.9 | 1.7 ± 4.1 | 35.7 ± 3.1 | 36.5 ± 3.2 | 0.8 ± 3.4 |
| Explode score | 23.6 ± 9.0 | 26.6 ± 9.1 | 2.9 ± 5.4 | 21.8 ± 4.6 | 24.1 ± 5.2 | 2.3 ± 5.0 |
| Drive score | 47.7 ± 27.0 | 28.6 ± 16.5 | −19.1 ± 21.1 | 49.3 ± 12.8 | 43.4 ± 12.8 | −5.9 ± 14.5 |
| Jump height (cm) | 18.1 ± 5.8 | 15.5 ± 4.1 | −11.0 ± 18.0 | 17.4 ± 4.4 | 17.6 ± 4.0 | 1.8 ± 9.3 |
| Injury risk score | 3.00 ± 1.51 | 2.25 ± 1.83 | −0.8 ± 2.4 | 2.50 ± 1.77 | 2.50 ± 1.77 | 0.0 ± 2.1 |
| Balance | ||||||
| Dominant (D) leg score | 52.6 ± 5.3 | 45.2 ± 8.5 | −7.4 ± 11.4 | 55.3 ± 8.2 | 49.3 ± 7.8 | −5.9 ± 3.6 |
| Non-dominant (ND) leg score | 51.6 ± 6.5 | 48.3 ± 7.5 | −3.2 ± 10.4 | 54.7 ± 7.9 | 51.1 ± 7.5 | −3.6 ± 3.6 |
| Asymmetry ratio (D:ND) | 1.03 ± 0.08 | 0.95 ± 0.23 | −0.07 ± 0.20 | 1.01 ± 0.07 | 0.96 ± 0.03 | −0.04 ± 0.08 |
| Plank | ||||||
| Dominant (D) arm score | 45.5 ± 2.4 | 43.7 ± 2.7 | −1.7 ± 2.7 | 54.5 ± 18.7 | 45.0 ± 2.3 | −9.6 ± 18.9 |
| Non-dominant (ND) arm score | 47.2 ± 3.4 | 45.9 ± 3.0 | −1.3 ± 1.6 | 61.9 ± 21.7 | 46.6 ± 2.9 | −15.3 ± 19.7 |
| Asymmetry ratio (D:ND) | 0.97 ± 0.04 | 0.96 ± 0.09 | −0.01 ± 0.06 | 0.92 ± 0.21 | 0.97 ± 0.07 | 0.05 ± 0.16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, C.; Doma, K.; Heilbronn, B.; Leicht, A. Impact of a 5-Week Individualised Training Program on Physical Performance and Measures Associated with Musculoskeletal Injury Risk in Army Personnel: A Pilot Study. Sports 2023, 11, 8. https://doi.org/10.3390/sports11010008
Smith C, Doma K, Heilbronn B, Leicht A. Impact of a 5-Week Individualised Training Program on Physical Performance and Measures Associated with Musculoskeletal Injury Risk in Army Personnel: A Pilot Study. Sports. 2023; 11(1):8. https://doi.org/10.3390/sports11010008
Chicago/Turabian StyleSmith, Chelsea, Kenji Doma, Brian Heilbronn, and Anthony Leicht. 2023. "Impact of a 5-Week Individualised Training Program on Physical Performance and Measures Associated with Musculoskeletal Injury Risk in Army Personnel: A Pilot Study" Sports 11, no. 1: 8. https://doi.org/10.3390/sports11010008