
Comparison of Conservative Interventions for Proximal Hamstring Tendinopathy: A Systematic Review and Recommendations for Rehabilitation

Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Study Selection
2.4. Level of Evidence and Grade of Recommendation
2.5. Data Extraction
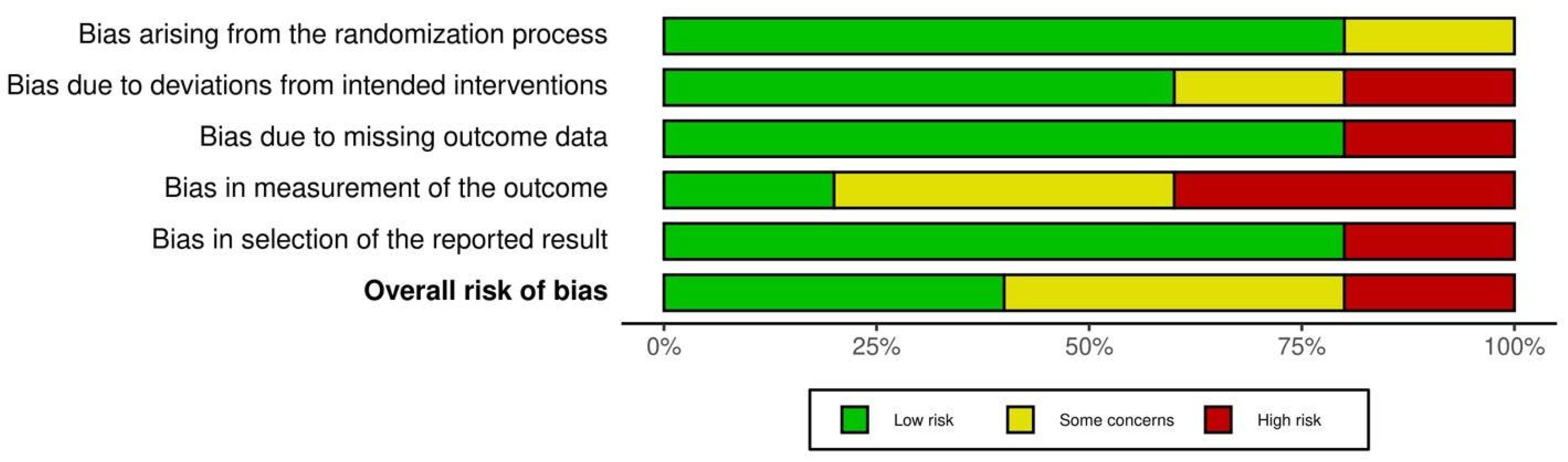
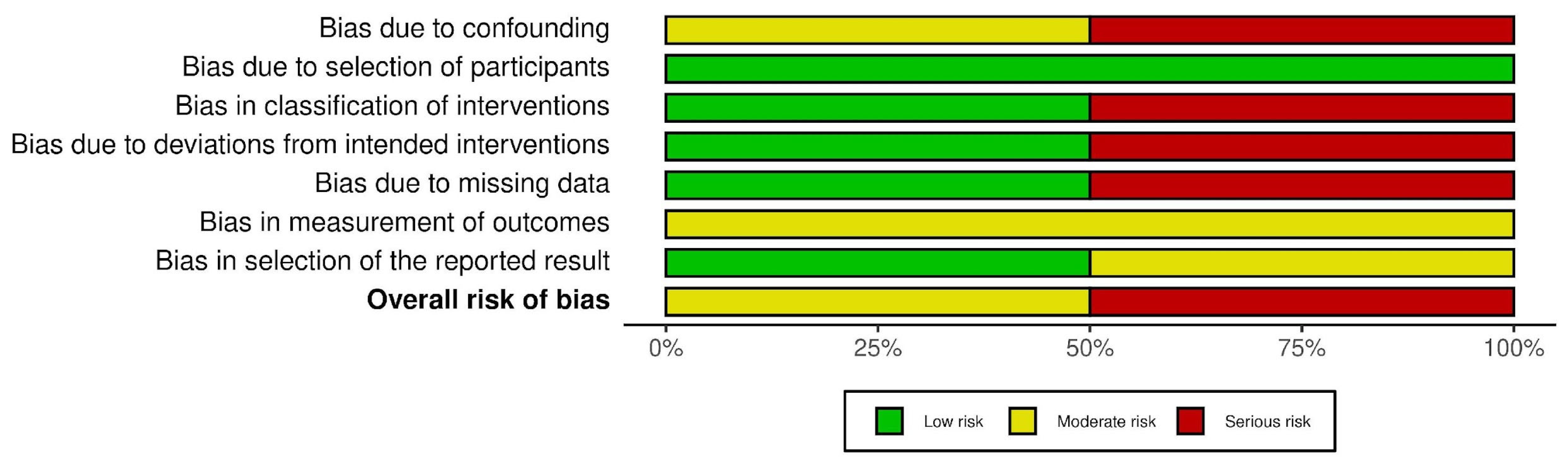
2.6. Risk of Bias Assessment
3. Results
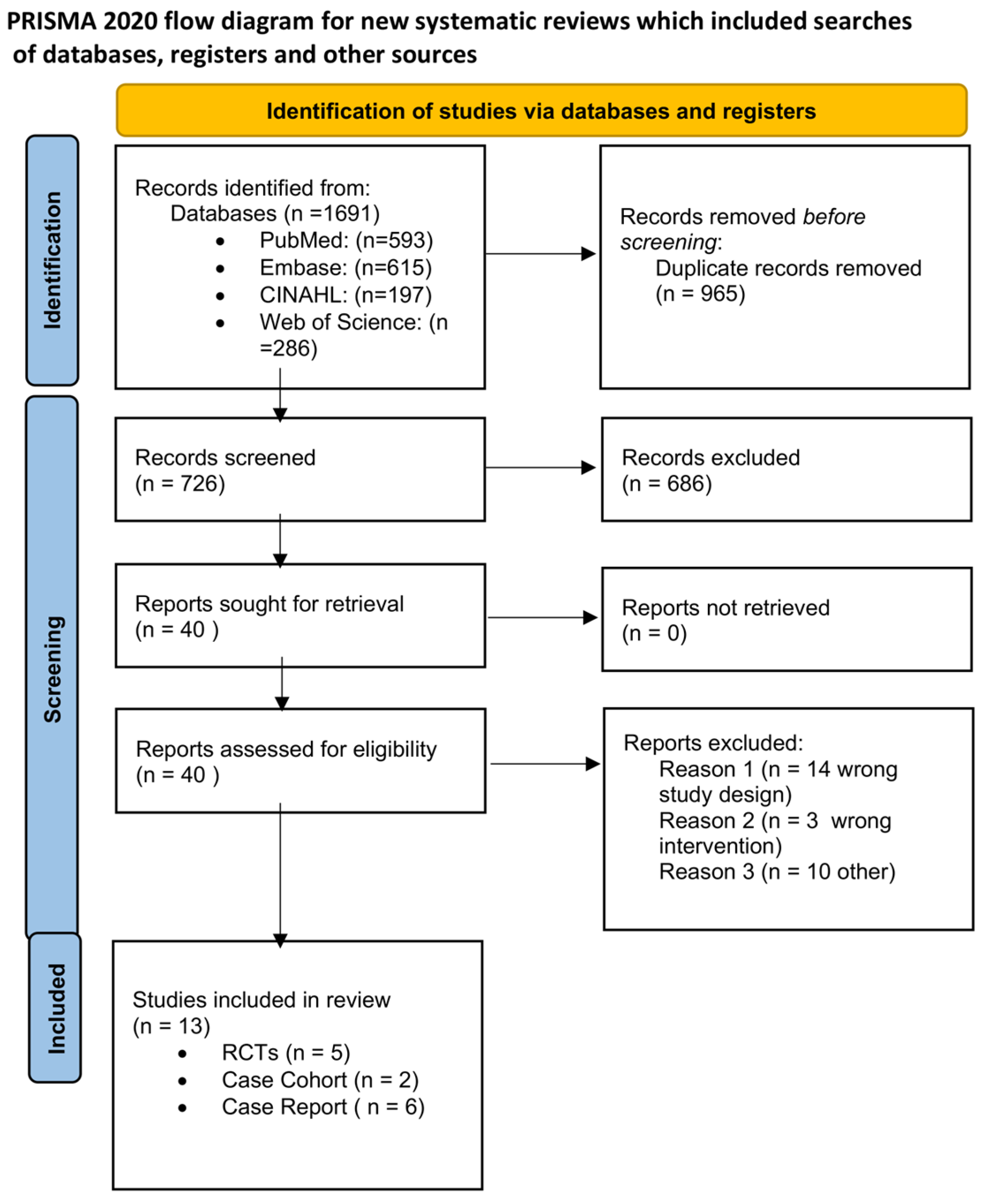
3.1. Study Selection and Characteristics
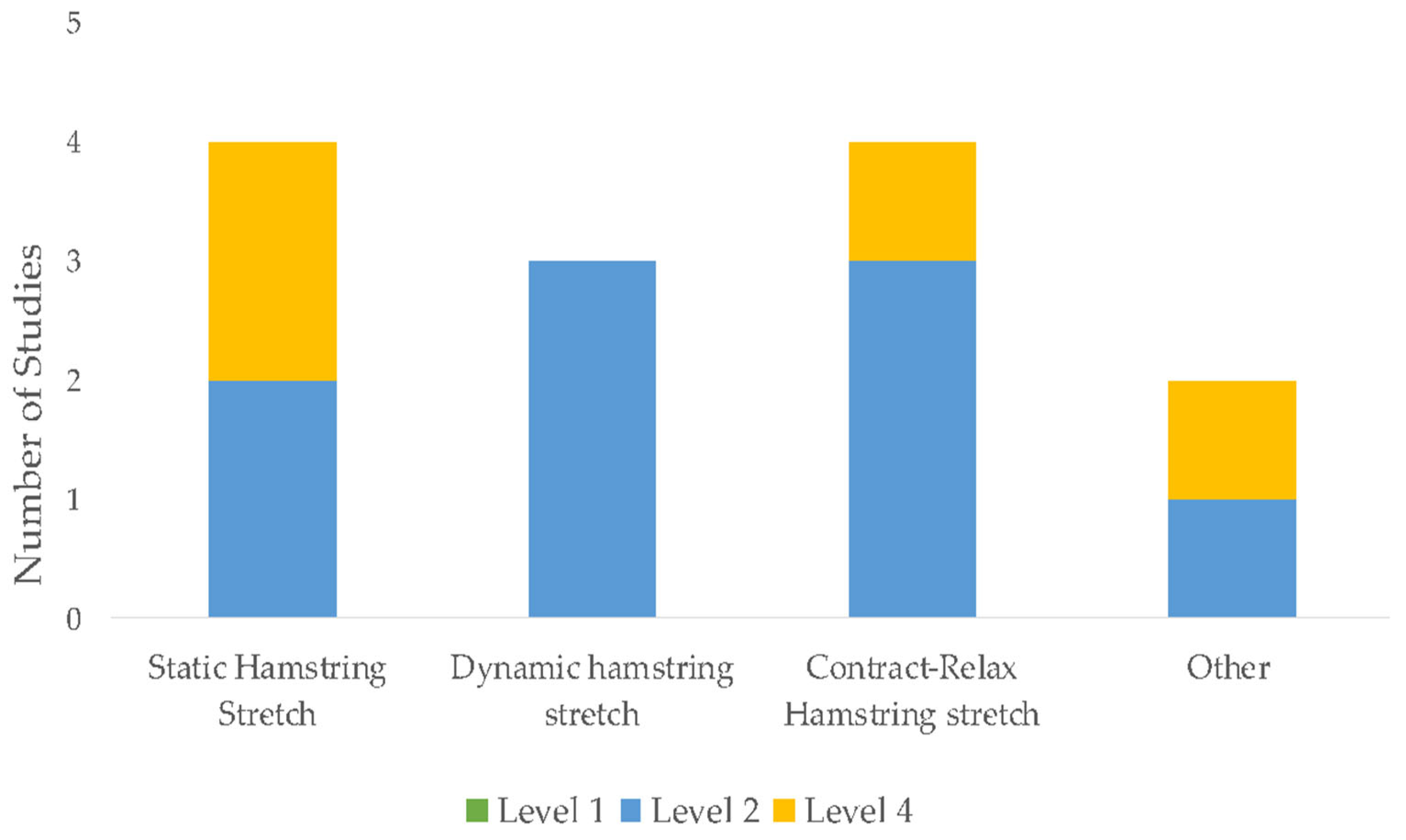
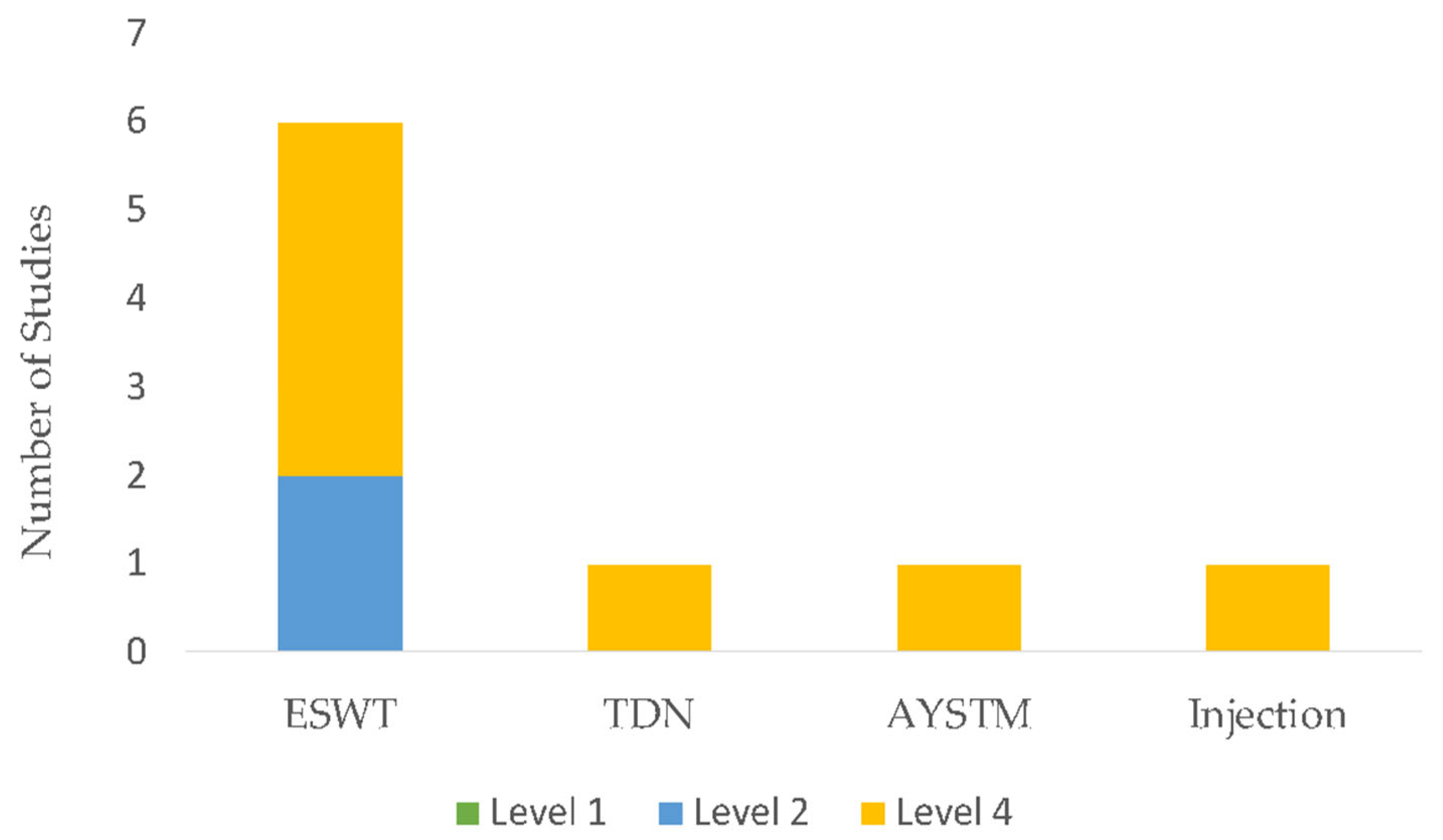
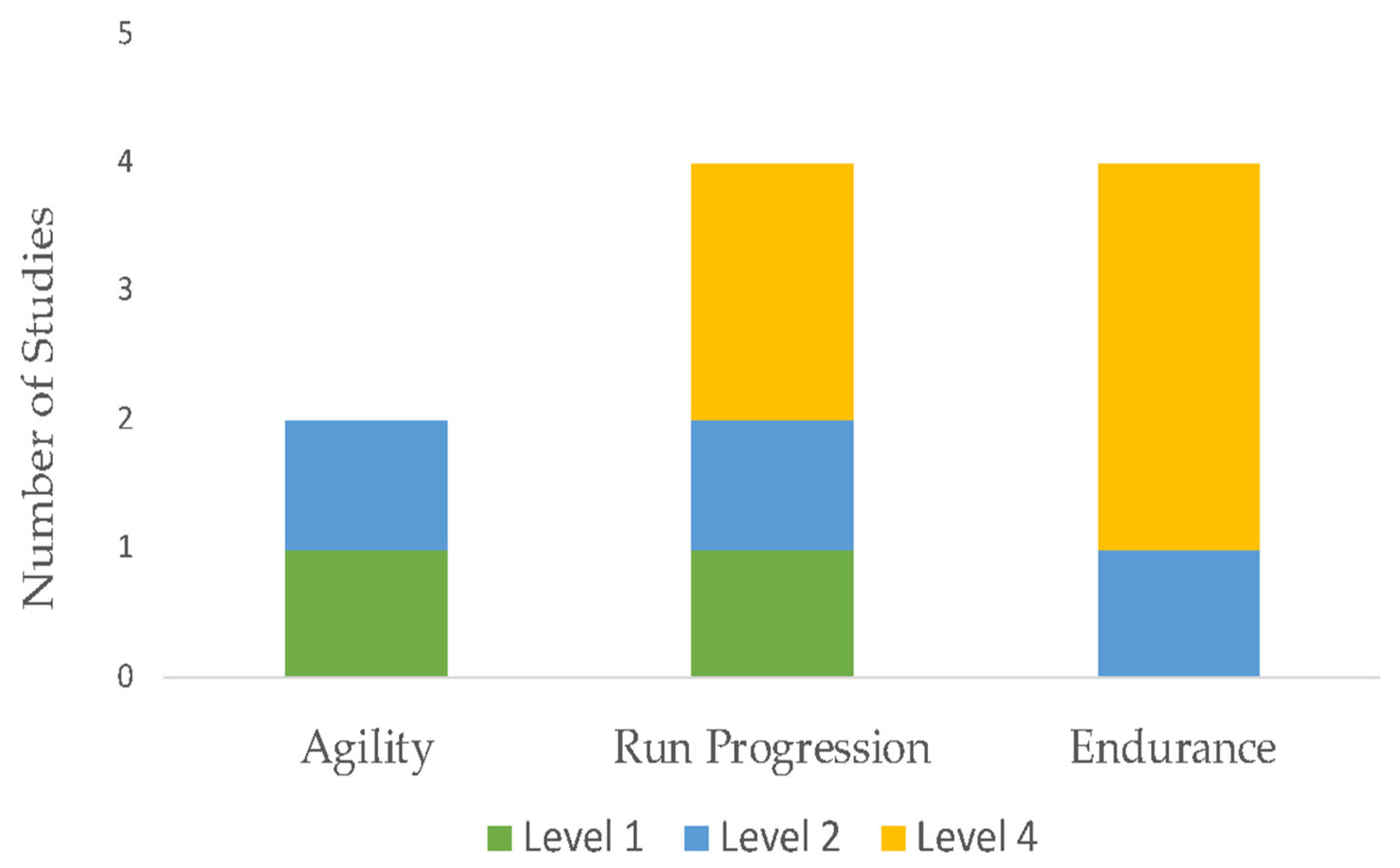
3.2. Grade of Recommendations
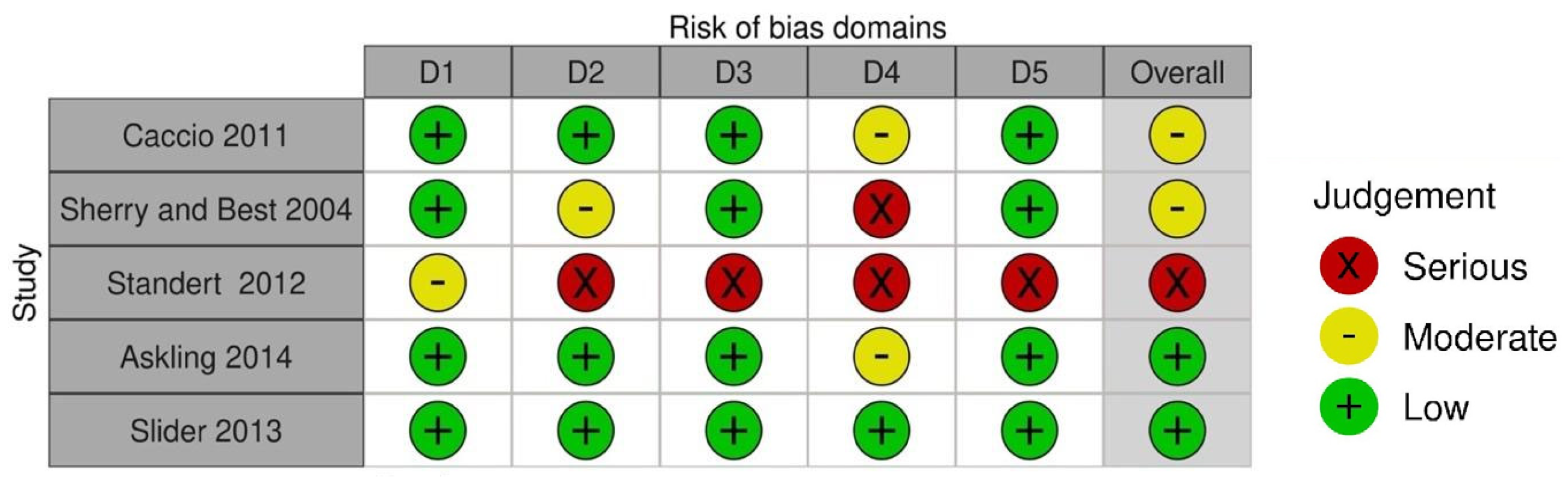
3.3. Risk of Bias Assessment
- Were the patient demographic characteristics clearly described?
- Was the patient’s history clearly described and presented as a timeline?
- Was the current clinical condition of the patient presentation clearly described?
- Were diagnostic tests or assessment methods and the results clearly described?
- Was the intervention(s) or treatment procedure(s) clearly described?
- Was the post-intervention clinical condition clearly described?
- Were adverse events (harms) or unanticipated events identified and described?
- Does the case report provide takeaway lessons?
4. Discussion
4.1. Pain Outcome
4.2. Percent Disability as Measured by the LEFS/VISA-H
4.3. Return to Sport and Re-Injury Rate
4.4. Joint Angle Loading and Kinematic Considerations with Respect to Hamstring Muscular Activation
4.5. Comparison to Prior Review
4.6. Limitations with Included Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martínez, J.P.M.; Gómez, J.P.; Vivas, J.C. The influence of fatigue in hamstrings:quadriceps ratio. A systematic review. Arch. Med. Deporte 2016, 9, 267–275. [Google Scholar]
- Schroeter, S.; Heiss, R.; Hammer, C.M.; Grim, C.; Engelhardt, M.; Hotfiel, T. Diagnosis of Proximal Hamstring Injuries. Sport. Orthop. Traumatol. 2022, 38, 47–57. [Google Scholar] [CrossRef]
- Onishi, K.; Fredericson, M.; Dragoo, J.L. Tendinopathy: From basic science to clinical management. PMR 2015, 7, 1017. [Google Scholar]
- Goom, T.S.H.; Malliaras, P.; Reiman, M.P.; Purdam, C.R. Proximal Hamstring Tendinopathy: Clinical Aspects of Assessment and Management. J. Orthop. Sports Phys. Ther. 2016, 46, 483–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reilly, J.M.; Tenforde, A.S. The Role of Extracorporeal Shockwave Therapy in Return to Competition for Endurance Runners: Two Case Reports. PM&R 2020, 12, 516–517. [Google Scholar] [CrossRef]
- Krueger, K.; Washmuth, N.B.; Williams, T.D. The Management of proximal hamstring tendinopathy in a competitive powerlifter with heavy slow resistance training—A case report. Int. J. Sports Phys. Ther. 2020, 15, 814–822. [Google Scholar] [CrossRef]
- Cushman, D.; Rho, M.E. Conservative Treatment of Subacute Proximal Hamstring Tendinopathy Using Eccentric Exercises Performed With a Treadmill: A Case Report. J. Orthop. Sports Phys. Ther. 2015, 45, 557–562. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Swartz, M.K. The PRISMA Statement: A Guideline for Systematic Reviews and Meta-Analyses. J. Pediatr. Health Care 2011, 25, 1–2. [Google Scholar] [CrossRef]
- Swanson, J.A.; Schmitz, D.; Chung, K.C. How to practice evidence-based medicine. Plast. Reconstr. Surg. 2010, 126, 286–294. [Google Scholar] [CrossRef]
- Howick, J.; Chalmers, I.; Greenhalgh, T.; Heneghan, C.; Liberti, A.; Moschetti, I. Explanation of the 2011 Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence, University of Oxford. 2001. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 1 February 2023).
- Martin, R.L.; Cibulka, M.T.; Bolgla, L.A.; Koc, J.T.A.; Loudon, J.K.; Manske, R.C.; Weiss, L.; Christoforetti, J.J.; Heiderscheit, B.C. Hamstring Strain Injury in Athletes: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability and Health From the Academy of Orthopaedic Physical Therapy and the American Academy of Sports Physical Therapy of the American Physical Therapy Association. J. Orthop. Sport. Phys. Ther. 2022, 52, CPG1–CPG44. [Google Scholar] [CrossRef]
- Mehta, S.P.; Fulton, A.; Quach, C.; Thistle, M.; Toledo, C.; Evans, N.A. Measurement Properties of the Lower Extremity Functional Scale: A Systematic Review. J. Orthop. Sports Phys. Ther. 2016, 46, 200–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cacchio, A.; De Paulis, F.; Maffulli, N. Development and validation of a new visa questionnaire (VISA-H) for patients with proximal hamstring tendinopathy. Br. J. Sports Med. 2014, 48, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Silder, A.; Sherry, M.A.; Sanfilippo, J.; Tuite, M.J.; Hetzel, M.S.J.; Heiderscheit, B.C. Clinical and Morphological Changes Following 2 Rehabilitation Programs for Acute Hamstring Strain Injuries: A Randomized Clinical Trial. J. Orthop. Sports Phys. Ther. 2013, 43, 284–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherry, M.A.; Best, T.M. A Comparison of 2 Rehabilitation Programs in the Treatment of Acute Hamstring Strains. Res. Rep. 2004, 34, 10. [Google Scholar]
- Jayaseelan, D.J.; Moats, N.; Ricardo, C.R. Rehabilitation of Proximal Hamstring Tendinopathy Utilizing Eccentric Training, Lumbopelvic Stabilization, and Trigger Point Dry Needling: 2 Case Reports. J. Orthop. Sports Phys. Ther. 2014, 44, 198–205. [Google Scholar] [CrossRef] [Green Version]
- McCormack, J.R. The management of bilateral high hamstring tendinopathy with ASTYM ® treatment and eccentric exercise: A case report. J. Man. Manip. Ther. 2012, 20, 142–146. [Google Scholar] [CrossRef] [Green Version]
- Askling, C.M.; Tengvar, M.; Tarassova, O.; Thorstensson, A. Acute hamstring injuries in Swedish elite sprinters and jumpers: A prospective randomised controlled clinical trial comparing two rehabilitation protocols. Br. J. Sports Med. 2014, 48, 532–539. [Google Scholar] [CrossRef]
- Cacchio, A.; Rompe, J.D.; Furia, J.P.; Susi, P.; Santilli, V.; De Paulis, F. Shockwave Therapy for the Treatment of Chronic Proximal Hamstring Tendinopathy in Professional Athletes. Am. J. Sports Med. 2011, 39, 146–153. [Google Scholar] [CrossRef]
- Mitchkash, M.; Robinson, D.; Tenforde, A.S. Efficacy of Extracorporeal Pulse-Activated Therapy in the Management of Lower-Extremity Running-Related Injuries: Findings From a Large Case Cohort. J. Foot Ankle Surg. 2020, 59, 795–800. [Google Scholar] [CrossRef]
- Fredericson, M.; Moore, W.; Guillet, M.; Beaulieu, C. High hamstring tendinopathy in runners: Meeting the challenges of diagnosis, treatment, and rehabilitation. Phys. Sportsmed. 2005, 33, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Standaert, C.J. Shockwave Therapy for Chronic Proximal Hamstring Tendinopathy. Clin. J. Sport Med. 2012, 22, 170–171. [Google Scholar] [CrossRef] [PubMed]
- Yun, P.H.; DeLuca, S.; Robinson, D.; Park, A.; Rosenberg, C.; Kohler, M.; Tenforde, A. Radial versus Combined Shockwave Therapy in the Management of Proximal Hamstring Tendinopathy: Similar Functional Outcomes in Running Cohort. Muscle Ligaments Tendons J. 2021, 11, 742. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Keerasomboon, T.; Mineta, S.; Hirose, N. Influence of Altered Knee Angle and Muscular Contraction Type on Electromyographic Activity of Hamstring Muscles during 45° Hip Extension Exercise. J. Sports Sci. Med. 2020, 19, 630–636. [Google Scholar]
- Millar, N.L.; Silbernagel, K.G.; Thorborg, K.; Kirwan, P.D.; Galatz, L.M.; Abrams, G.D.; Murrell, G.A.C.; McInnes, I.B.; Rodeo, S.A. Tendinopathy. Nat. Rev. Dis. Primers 2021, 7, 1. [Google Scholar] [CrossRef]
- Agergaard, A.-S.; Svensson, R.B.; Malmgaard-Clausen, N.M.; Couppé, C.; Hjortshoej, M.H.; Doessing, S.; Kjaer, M.; Magnusson, S.P. Clinical Outcomes, Structure, and Function Improve With Both Heavy and Moderate Loads in the Treatment of Patellar Tendinopathy: A Randomized Clinical Trial. Am. J. Sports Med. 2021, 49, 982–993. [Google Scholar] [CrossRef]
- Farup, J.; Rahbek, S.K.; Riis, S.; Vendelbo, M.H.; de Paoli, F.; Vissing, K. Influence of exercise contraction mode and protein supplementation on human skeletal muscle satellite cell content and muscle fiber growth. J. Appl. Physiol. 2014, 117, 898–909. [Google Scholar] [CrossRef] [Green Version]
- Kongsgaard, M.; Kovanen, V.; Aagaard, P.; Doessing, S.; Hansen, P.; Laursen, A.H.; Kaldau, N.C.; Kjaer, M.; Magnusson, S.P. Corticosteroid injections, eccentric decline squat training and heavy slow resistance training in patellar tendinopathy. Scand. J. Med. Sci. Sport. 2009, 19, 790–802. [Google Scholar] [CrossRef]
- Ackerman, J.E.; Bah, I.; Jonason, J.H.; Buckley, M.R.; Loiselle, A.E. Aging does not alter tendon mechanical properties during homeostasis, but does impair flexor tendon healing: Aging impairs flexor tendon healing. J. Orthop. Res. 2017, 35, 2716–2724. [Google Scholar] [CrossRef] [Green Version]
- van der Horst, N.; Smits, D.W.; Petersen, J.; Goedhart, E.A.; Backx, F.J.G. The preventive effect of the Nordic hamstring exercise on hamstring injuries in amateur soccer players: Study protocol for a randomised controlled trial. Inj. Prev. 2014, 20, e8. [Google Scholar] [CrossRef] [PubMed]
- Guruhan, S.; Kafa, N.; Ecemis, Z.B.; Guzel, N.A. Muscle Activation Differences During Eccentric Hamstring Exercises. Sports Health 2021, 13, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Van Hooren, B.; Vanwanseele, B.; Rossom, S.; Teratsias, P.; Willems, P.; Drost, M.; Meijer, K. Muscle forces and fascicle behavior during three hamstring exercises. Scand. Med. Sci. Sports 2022, 32, 997–1012. [Google Scholar] [CrossRef] [PubMed]
- Askling, C.M.; Tengvar, M.; Saartok, T.; Thorstensson, A. Proximal Hamstring Strains of Stretching Type in Different Sports: Injury Situations, Clinical and Magnetic Resonance Imaging Characteristics, and Return to Sport. Am. J. Sports Med. 2008, 36, 1799–1804. [Google Scholar] [CrossRef] [Green Version]
- Lempainen, L.; Sarimo, J.; Mattila, K.; Vaittinen, S.; Orava, S. Proximal Hamstring Tendinopathy: Results of Surgical Management and Histopathologic Findings. Am. J. Sports Med. 2009, 37, 727–734. [Google Scholar] [CrossRef]
- Youm, T. Proximal Hamstring Tears: From Endoscopic Repair to Open Reconstruction; Springer International Publishing: Cham, Switzerland, 2021. [Google Scholar]
- Kalkhoven, J.T.; Sides, D.L.; McLean, B.D.; Watsford, M. The evidence indicates that the hamstrings do not behave isometrically during the swing phase of the sprint cycle: A narrative review. SportRxiv 2020. [Google Scholar] [CrossRef]
- Nasser, A. Proximal hamstring tendinopathy: A systematic review of interventions. J. Sci. Med. Sport 2018, 21, S96–S97. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question Component | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population |
|
|
| Intervention |
|
|
| Comparison |
| |
| Outcome |
| |
| Study Design |
|
| Study Type/Level of Evidence | Author | Control Group | Intervention Group | Diagnostic Criteria | Age | Gender | Activity Level | Follow-Up Time |
|---|---|---|---|---|---|---|---|---|
| Case report//Level IV | Reilly et al. [5] | NA | 1 | Clinical exam | 25 | F:2 | Ultramarathoner | 6 weeks; 10 month |
| Case report//Level IV | Kreuger et al. [6] | NA | 1 | Med Dx as assessed via sports physician | 31 | M | Power lifter | 12 week–12 month follow-up |
| Case report//Level IV | Cushman et al. [7] | NA | 1 | Ultrasound | 34 | M | Triathlete (14 local triathlons for 14 years) | 12 week |
| Randomized, double-blind, parallel-group clinical trial//Level I b | Silder et al. [15] | 16 PATS | 13 PRES | MRI | 16–43 | 6 F 23 M | Runners | MRI and physical examinations conducted after completion of rehabilitation and up to 6 month following return to sport |
| Prospective randomized comparison//Level II | Sherry & Best et al. [16] | 11 PATS | 13 STS | Clinical exam | 14–49 | 8 F: PATS M: 18, STST: F: 4. M: 18 | Active in sports | 4 weeks |
| Case study//Level IV | Jayasleen et al. [17] | NA | 2 | Med Dx as assessed via ortho surgeon | 71; 69 | M | (A) Active running 40–48 km, biking 80 km per week—discontinued due to pain (B) Triathlete | 8/10 week = discharge |
| Case report//Level IV | McCormack et al. [18] | NA | 1 | Med dx | 41 | M | Recreational runner | 12 week |
| Prospective randomized comparison//Level II | Askling et al. [19] | 28 L protocol | 28 C protocol | MRI | 15–29 | 32 F 68 M | Swedish track and field athletes | 1 year for re-injuries Number of days to return to full training |
| RCT/Level II | Cacchio et al. [20] | 20 TCM | 20 ESWT | MRI T1 and T2 imaging | 23 | M: 27 F: 13 | Professional athletes | pts evaluated before tx, at week 1, 3, 6, and 12 months after end of use |
| Case cohort//Level IV | Mitchkash et al. [21] | NA | 32 | Chart reviewed for “running related injury” that was interfered with normal training and ability to compete >7 days | 39 | M: 10 F: 22 | Runners | 8 weeks from initiation tx |
| Case report//Level IV | Fredericson et al. [22] | NA | 1 | MRI | 32 | F | Olympic athlete | 6 month |
| RCT//Level II | Standert et al. [23] | Rest and to take 600-mg ibuprofen twice daily for the first week. 2 weeks PT: modalities + strengthening | n = 20 ESWT | MRI | not stated | 27 M 13 F | NR | 12 month |
| Case cohort//Level IV | Yun et al. [24] | 40 RSWT | 23 CSWT | MRI | 42 | F: 41 M: 22 | Runner | 2 years |
| Intervention (s) | Study | Strengthening | Agility/Plyometrics/Endurance | Lumbopelvic Stability | Stretching | Other Modalities (Shockwave, Needling, etc.) |
|---|---|---|---|---|---|---|
| Exercise | Kreuger et al. [6] | ✅ | ||||
| Cushman et al. [7] | ✅ | ✅ | ✅ | ✅ | ||
| Silder et al. [15] | ✅ | ✅ | ✅ | |||
| Sherry & Best et al. [16] | ✅ | ✅ | ✅ | ✅ | ||
| Askling et al. [19] | ✅ | ✅ | ✅ | ✅ | ||
| Exercise + Modality | Reilly et al. [5] | ✅ | ✅ | ✅ | ||
| Jayasleen et al. [17] | ✅ | ✅ | ✅ | |||
| McCormack et al. [18] | ✅ | ✅ | ✅ | |||
| Cacchio et al. [20] | ✅ | ✅ | ||||
| Mitchkash et al. [21] | ✅ | ✅ | ||||
| Fredericson et al. [22] | ✅ | ✅ | ✅ | ✅ | ✅ | |
| Standert et al. [23] | ✅ | ✅ | ✅ | |||
| Yun et al. [24] | ✅ | ✅ | ✅ | ✅ |
| Intervention (s) | Study | Reduction of VAS | Final VAS | Activity-Related Pain | MCD % | Weighted % Disability Improvement | Return to Sport | Reinjury rate (Percentage %) |
|---|---|---|---|---|---|---|---|---|
| Exercise | Kreuger et al. [6] | −6 | 2 | Initial: unable to sit >30 min 84 d: 2/10 with sitting >30 min 360 d: 2/10 with sitting >60 min | NR | NR | NR | NR |
| Cushman et al. [7] ẞ | −7 | 0 | 28 d: pain with sitting present 56 d: pain-free sitting | 22% | 272% | NR | NR | |
| Sherry & Best et al. [16] | NR | NR | NR | NR | NR | PATS: 22.2 d STST: 37.4 d | STS: 70% PATS: 7.7% | |
| Askling et al. [19] | NR | NR | NR | NR | NR | L protocol: median: 62 days C protocol: median: 120 days | L protocol: 0 C protocol: 7% | |
| Silder et al. [15] | PATS: −9 PRES: −5 | 0 | NR | NR | NR | PATS: 25.2 d PRES: 28.8 d | PRES: 23% PATS: 6% | |
| Jayasleen et al. [17] ɑ | −5 | 0 | NR | 11.2% | 144%, 122% | NR | NR | |
| Exercise + Modality | Mitchkash et al. [21] ẞ | NR | NR | NR | 22% | 118% | NR | NR |
| McCormack et al. [18] ɑ | −6 | 0 | 56 d: 2.5 mile pain-free 84 d: 1 mile jog without pain 112 d: 2.5 mi run without pain | 11.2% | 111% | NR | NR | |
| Cacchio et al. [20] | SWT: −4.1 TCT: 0.1 | SWT: 2.1 TCT: 6.8 | SWT: pain not present during activity but resolves within <48 h TCT: pain present during all activities and with ADLs | NR | NR | SWT: 80% in 63 d TCT: none | NR | |
| Reilly et al. [5] | NR | 0 | NR | NR | NR | 300 d | NR | |
| Standert et al. [23] | SWT: −5 TCT: −0.2 | SWT: 1.8 TCT: 5.5 | SWT: pain not present during activity but resolves within <48 h TCT: pain present during all activities and with ADLs | NR | NR | TCT: none SWT: 80% in 63 d | NR | |
| Fredericson et al. [22] | NR | 0 | NR | NR | NR | 180 d | NR | |
| Yun et al. [24] ẞ | NR | NR | NR | 22% | 102% | NR | NR |
| Sets | Reps | Load | Frequency/Week | Duration of Tx | |
|---|---|---|---|---|---|
| Average | 3 | 11 | 63% RM | 5 | 8 |
| Range | 1–4 | 6–20 | 30–90% | 2–7 | 6–24 |
| Standard deviation | 0.74 | 4.2 | 15.8 | 2 | 5.5 |
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Total | Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Reilly et al. [5] | Y | Y | Y | N | Y | Y | N | Y | 6 | Moderate |
| Krueger et al. [6] | Y | Y | Y | Y | Y | Y | Y | Y | 8 | High |
| Cushman et al. [7] | Y | Y | Y | Y | Y | Y | Y | Y | 8 | High |
| Jayasleen et al. [17] | Y | N | Y | Y | Y | Y | Y | Y | 7 | Moderate |
| McCormack et al. [18] | Y | Y | Y | Y | Y | Y | Y | Y | 8 | High |
| Fredericson et al. [22] | Y | Y | Y | Y | Y | Y | N | Y | 7 | Moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dizon, P.; Jeanfavre, M.; Leff, G.; Norton, R. Comparison of Conservative Interventions for Proximal Hamstring Tendinopathy: A Systematic Review and Recommendations for Rehabilitation. Sports 2023, 11, 53. https://doi.org/10.3390/sports11030053
Dizon P, Jeanfavre M, Leff G, Norton R. Comparison of Conservative Interventions for Proximal Hamstring Tendinopathy: A Systematic Review and Recommendations for Rehabilitation. Sports. 2023; 11(3):53. https://doi.org/10.3390/sports11030053
Chicago/Turabian StyleDizon, Pilar, Michael Jeanfavre, Gretchen Leff, and Rachel Norton. 2023. "Comparison of Conservative Interventions for Proximal Hamstring Tendinopathy: A Systematic Review and Recommendations for Rehabilitation" Sports 11, no. 3: 53. https://doi.org/10.3390/sports11030053