
Implementation and Evaluation of a School-Based Educational Program Targeting Healthy Diet and Exercise (DIEX) for Greek High School Students

 ,
,
Abstract
:1. Introduction
1.1. Theory of Planned Behavior (TPB) and School-Based Educational Programs Targeting Healthy Diets
1.2. TPB and School-Based Educational Programs Targeting Exercise
1.3. Life Skills and School-Based Programs Targeting Healthy Diet and Exercise
1.4. Aim of the Study
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedures
2.4. Data Analysis
3. Results
4. Discussion
Limitations and Future Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Global Nutrition Report. Available online: https://globalnutritionreport.org/reports/2021-global-nutrition-report/progress-towards-the-nutrition-for-growth-commitments (accessed on 28 August 2022).
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 24 September 2022).
- Singh, A.S.; Mulder, C.; Twisk, J.W.; van Mechelen, W.; Chinapaw, M.J. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 16, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Finkelstein, E.A.; Khavjou, O.A.; Thompson, H.; Trogdon, J.G.; Pan, L.; Sherry, B.; Dietz, W. Obesity and severe obesity forecasts through 2030. Am. J. Prev. Med. 2012, 42, 563–570. [Google Scholar] [CrossRef]
- Corona, M. The Association between Depression and Overweight/Obesity among Ethnic Minority Youth. Ph.D. Thesis, University of Washington, Seattle, WA, USA, 2014. [Google Scholar]
- Waasdorp, T.E.; Mehari, K.; Bradshaw, C.P. Obese and overweight youth: Risk for experiencing bullying victimization and internalizing symptoms. Am. J. Orthopsychiatry 2018, 88, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Mond, J.; van den Berg, P.; Boutelle, K.; Hannan, P.; Neumark-Sztainer, D. Obesity, body dissatisfaction, and emotional well-being in early and late adolescence: Findings from the project EAT study. J. Adolesc. Health 2011, 48, 373–378. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Obesity: Health Consequences of Being Overweight. Available online: https://www.who.int/news-room/questions-and-answers/item/obesity-health-consequences-of-being-overweight (accessed on 1 October 2022).
- Patton, G.C.; Sawyer, S.M.; Santelli, J.S.; Ross, D.A.; Afifi, R.; Allen, N.B.; Arora, M.; Azzopardi, P.; Baldwin, W.; Bonell, C.; et al. Our future: A Lancet commission on adolescent health and wellbeing. Lancet 2016, 387, 2423–2478. [Google Scholar] [CrossRef] [Green Version]
- Langford, R.; Bonell, C.; Jones, H.; Pouliou, T.; Murphy, S.; Waters, E.; Campbell, R. The World Health Organization’s health promoting schools framework: A Cochrane systematic review and meta-analysis. BMC Public Health 2015, 15, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craigie, A.M.; Lake, A.A.; Kelly, S.A.; Adamson, A.J.; Mathers, J.C. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas 2011, 70, 266–284. [Google Scholar] [CrossRef] [Green Version]
- Telama, R. Tracking of physical activity from childhood to adulthood: A review. Obes. Facts 2009, 2, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Pulimeno, M.; Piscitelli, P.; Colazzo, S.; Colao, A.; Miani, A. School as ideal setting to promote health and wellbeing among young people. Health Promot. Perspect. 2020, 10, 316–324. [Google Scholar] [CrossRef]
- Medeiros, G.C.B.S.; Azevedo, K.P.M.; Garcia, D.; Oliveira Segundo, V.H.; Mata, Á.N.S.; Fernandes, A.K.P.; Santos, R.P.D.; Trindade, D.D.B.B.; Moreno, I.M.; Guillén Martínez, D.; et al. Effect of school-based food and nutrition education interventions on the food consumption of adolescents: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2022, 24, 10522. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. Int. J. Nurs. Stud. 2013, 50, 587–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, R.; Campbell, R.; Hildon, Z.; Hobbs, L.; Michie, S. Theories of behaviour and behaviour change across the social and behavioural sciences: A scoping review. Health Psychol. Rev. 2015, 9, 323–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glanz, K.; Bishop, D.B. The role of behavioral science theory in development and implementation of public health interventions. Annu. Rev. Public Health 2010, 31, 399–418. [Google Scholar] [CrossRef] [Green Version]
- Lytle, L.A. Nutrition education, behavioral theories, and the scientific method: Another viewpoint. J. Nutr. Educ. Behav. 2005, 37, 90–93. [Google Scholar] [CrossRef]
- Ajzen, I. The Theory of Planned Behavior; Handbook of Theories of Social Psychology; Lawrence Erlbaum Associates: New York, NY, USA, 2012; pp. 438–459. [Google Scholar] [CrossRef]
- Fertman, C.I.; Grim, M. Health Promotion Programs: From Theory to Practice; Wiley: Hoboken, NJ, USA, 2016. [Google Scholar]
- Gourlan, M.; Bernard, P.; Bortolon, C.; Romain, A.J.; Lareyre, O.; Carayol, M.; Ninot, G.; Boiché, J. Efficacy of theory-based interventions to promote physical activity. A meta-analysis of randomised controlled trials. Health Psychol. Rev. 2016, 10, 50–66. [Google Scholar] [CrossRef]
- Malek, L.; Umberger, W.J.; Makrides, M.; ShaoJia, Z. Predicting healthy eating intention and adherence to dietary recommendations during pregnancy in Australia using the Theory of Planned Behaviour. Appetite 2017, 116, 431–441. [Google Scholar] [CrossRef]
- Ajzen, I.; Schmidt, P. Changing Behavior Using the Theory of Planned Behavior; The Handbook of Behavior Change; Cambridge University Press: New York, NY, USA, 2020; pp. 17–31. [Google Scholar] [CrossRef]
- Riebl, S.K.; Estabrooks, P.A.; Dunsmore, J.C.; Savla, J.; Frisard, M.I.; Dietrich, A.M.; Peng, Y.; Zhang, X.; Davy, B.M. A systematic literature review and meta-analysis: The Theory of Planned Behavior’s application to understand and predict nutrition-related behaviors in youth. Eat. Behav. 2015, 18, 160–178. [Google Scholar] [CrossRef]
- Verduci, E.; Di Profio, E.; Fiore, G.; Zuccotti, G. Integrated Approaches to Combatting Childhood Obesity. Ann. Nutr. Metab. 2022, 78, 8–19. [Google Scholar] [CrossRef]
- Drenowatz, C.; Greier, K. Association of Sports Participation and Diet with Motor Competence in Austrian Middle School Students. Nutrients 2018, 10, 1837. [Google Scholar] [CrossRef] [Green Version]
- Bremer, E.; Cairney, J. Fundamental movement skills and health-related outcomes: A narrative review of longitudinal and intervention studies targeting typically developing children. Am. J. Lifestyle Med. 2016, 12, 148–159. [Google Scholar] [CrossRef]
- Meng, Y.; Manore, M.M.; Schuna, J.M.J.; Patton-Lopez, M.M.; Branscum, A.; Wong, S.S. Promoting healthy diet, physical activity, and life-skills in high school athletes: Results from the WAVE ripples for change childhood obesity prevention two-year intervention. Nutrients 2018, 23, 947. [Google Scholar] [CrossRef] [Green Version]
- Koletzko, B.; Fishbein, M.; Lee, W.S.; Moreno, L.; Mouane, N.; Mouzaki, M.; Verduci, E. Prevention of childhood obesity: A position paper of the global federation of international societies of paediatric gastroenterology, hepatology and nutrition (FISPGHAN). J. Pediatr. Gastroenterol Nutr. 2020, 70, 702–710. [Google Scholar] [CrossRef] [PubMed]
- Meiklejohn, S.; Ryan, L.; Palermo, C. A systematic review of the impact of multi-strategy nutrition education programs on health and nutrition of adolescents. J. Nutr. Educ. Behav. 2016, 48, 631–646. [Google Scholar] [CrossRef] [PubMed]
- Steinmetz, H.; Knappstein, M.; Ajzen, I.; Schmidt, P.; Kabst, R. How effective are behavior change interventions based on the theory of planned behavior? A three-level meta-analysis. Z. Psychol. 2016, 224, 216–233. [Google Scholar] [CrossRef]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behavior; Prentice-Hall: Englewood Cliffs, NJ, USA, 1980. [Google Scholar]
- Montano, D.E.; Kasprzyk, D. Theory of reasoned action, theory of planned behavior, and the integrated behavioral model. In Health Behavior: Theory, Research, and Practice; Glanz, K., Rimer, B.K., Viswanath, K.V., Eds.; Jossey-Bass/Wiley: San Francisco, CA, USA, 2015; pp. 95–124. [Google Scholar]
- Nilsen, P. Making Sense of Implementation Theories, Models, and Frameworks. In Implementation Science 3.0; Springer: Cham, Switzerland, 2020; pp. 53–79. [Google Scholar]
- Conner, M.; Rodgers, W.M.; Murray, T.C. Conscientiousness and the intention behavior relationship: Predicting exercise behavior. J. Sport Exerc. Psychol. 2007, 29, 518–533. [Google Scholar] [CrossRef]
- Arrizabalaga-López, M.; de Jáuregui, D.R.F.; Portillo, M.P.; Martinez, O.; Etaio, I.; Mauleon, J.R.; Rodríguez, V.M. A randomised controlled trial of a program based on the theory of planned behavior to promote fruit and vegetable intake among schoolchildren: PROFRUVE study protocol. BMC Public Health 2018, 18, 1–7. [Google Scholar] [CrossRef]
- Harrington, M.R.; Ickes, M.; Bradley, K.; Noland, M. The Theory of Planned Behavior and the USDA summer food service program. J. Nutr. Educ. Behav. 2020, 52, 944–951. [Google Scholar] [CrossRef]
- Singh, U.K.; Gautam, N.; Bhandari, T.R.; Sapkota, N. Educational intervention of intention change for consumption of junk food among school adolescents in Birgunj Metropolitan city, Nepal, based on Theory of Planned Behaviors. J. Nutr. Metab. 2020, 27, 7932–7934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaveh, M.H.; Darabi, F.; Khalajabadi-Farahani, F.; Yaseri, M.; Mohammadi, M.J.; Adeli Behrooz, H.R.; Shojaeizadeh, D.; Rohban, A. The impact of a Tpb-based educational intervention on nutritional behaviors in Iranian adolescent girls: A randomized controlled trial. Fresenius Environ. Bull. 2018, 27, 4349–4356. [Google Scholar] [CrossRef] [Green Version]
- Dhauvadel, A.S.; Wagle, S.; Bhandari, T.R. Effects of nutrition education program in intention change for consuming healthy food among adolescents: A School-based study. J. Sci. Soc. 2019, 46, 41–45. [Google Scholar] [CrossRef]
- Salam, R.A.; Padhani, Z.A.; Das, J.K.; Shaikh, A.Y.; Hoodbhoy, Z.; Jeelani, S.M.; Lassi, Z.S.; Bhutta, Z.A. Effects of lifestyle modification interventions to prevent and manage child and adolescent obesity: A systematic review and meta-analysis. Nutrients 2020, 12, 2208. [Google Scholar] [CrossRef] [PubMed]
- De Bourdeaudhuij, I.; Van Cauwenberghe, E.; Spittaels, H.; Oppert, J.M.; Rostami, C.; Brug, J.; Van Lenthe, F.; Lobstein, T.; Maes, L. School-based interventions promoting both physical activity and healthy eating in Europe: A systematic review within the HOPE project. Obes. Rev. 2011, 12, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Hackman, C.L.; Knowlden, A.P. Theory of reasoned action and theory of planned behavior-based dietary interventions in adolescents and young adults: A systematic review. Adolesc. Health Med. Ther. 2014, 6, 101–114. [Google Scholar] [CrossRef] [Green Version]
- Beck Silva, K.B.; Miranda Pereira, E.; Santana, M.L.P.; Costa, P.R.F.; Silva, R.C.R. Effects of computer-based interventions on food consumption and anthropometric parameters of adolescents: A systematic review and metanalysis. Crit. Rev. Food Sci. Nutr. 2022, 5, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kolbe, L.J. School health as both a strategy to improve both public health and education. Annu. Rev. Public Health 2019, 40, 443–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, A.; Lo, A.; Li, Q.; Keung, V.; Kwong, A. Health Promoting Schools: An Update. Appl. Health Econ. Health Policy 2020, 15, 605–623. [Google Scholar] [CrossRef] [Green Version]
- Abdelkarim, O.; Ammar, A.; Chtourou, H.; Wagner, M.; Knisel, E.; Hökelmann, A.; Bös, K. Relationship between motor and cognitive learning abilities among primary school-aged children. Alex. J. Med. 2017, 53, 325–331. [Google Scholar] [CrossRef]
- Cholevas, N.K.; Loucaides, C.A. Factors that facilitate and barriers towards the implementation of health educational programmes in primary education schools of the prefecture of Achaia, Greece. Health Educ. J. 2012, 71, 365–375. [Google Scholar] [CrossRef]
- Hirschler, V.; Buzzano, K.; Erviti, A.; Ismael; Silva, S.; Dalamon, R. Overweight and lifestyle behaviors of low socioeconomic elementary school children in Buenos Aires. BMC Pediatr. 2009, 24, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. The Theory of Planned Behaviour: Reactions and Reflections. Psychol. Health 2011, 26, 1113–1127. [Google Scholar] [CrossRef] [PubMed]
- Webb, T.L.; Joseph, J.; Yardley, L.; Michie, S. Using the internet to promote health behavior change: A systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J. Med. Internet Res. 2010, 12, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McIntosh, J.R.D.; Jay, S.; Hadden, N.; Whittaker, P.J. Do E-health interventions improve physical activity in young people: A systematic review. Public Health 2017, 148, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Plotnikoff, R.C.; Lubans, D.R.; Costigan, S.A.; Trinh, L.; Spence, J.C.; Downs, S.; McCargar, L. A test of the theory of planned behavior to explain physical activity in a large population sample of adolescents from Alberta, Canada. J. Adolesc. Health 2011, 49, 547–549. [Google Scholar] [CrossRef] [PubMed]
- Dobbins, M.; Husson, H.; DeCorby, K.; LaRocca, R.L. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst. Rev. 2013, 21, 1–228. [Google Scholar] [CrossRef]
- Kriemler, S.; Meyer, U.; Martin, E.; van Sluijs, E.M.F.; Andersen, L.B.; Martin, B.W. Effect of school-based interventions on physical activity and fitness in children and adolescents: A review of reviews and systematic update. Br. J. Sport. Med. 2011, 45, 923–930. [Google Scholar] [CrossRef] [Green Version]
- Hsu, M.S.H.; Rouf, A.; Allman-Farinelli, M. Effectiveness and behavioral mechanisms of social media interventions for positive nutrition behaviors in adolescents: A systematic review. J. Adolesc. Health 2018, 63, 531–545. [Google Scholar] [CrossRef]
- Chatzisarantis, N.L.D.; Kamarova, S.; Wang, J.; Kawabata, M.; Hagger, M.S. Developing and evaluating effects of an intervention based on the theory of planned behaviour in promoting leisure-time physical activity. Int. J. Sport. Psychol. 2015, 46, 95–116. [Google Scholar] [CrossRef]
- Chatzisarantis, N.L.D.; Hagger, M.S. Effects of a brief intervention based on the theory of planned behavior on leisure-time physical activity participation. J. Sport Exerc. Psychol. 2005, 27, 470–487. [Google Scholar] [CrossRef]
- Kawabata, M.; Chua, K.L.; Chatzisarantis, N.L.D. A school-based intervention program in promoting leisure-time physical activity: Trial protocol. BMC Public Health 2018, 18, 433. [Google Scholar] [CrossRef] [Green Version]
- Metcalf, B.; Henley, W.; Wilkin, T. Effectiveness of intervention on physical activity of children: Systematic review and meta-analysis of controlled trials with objectively measured outcomes. BMJ 2012, 27, 345. [Google Scholar] [CrossRef] [Green Version]
- Love, R.E.; Adams, J.; van Sluijs, E.M.F. Equity effects of children’s physical activity interventions: A systematic scoping review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coulson, N.S.; Eiser, C.; Eiser, J.R. Diet, smoking and exercise: Interrelationships between adolescent health behaviours. Child Care Health Dev. 1997, 23, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.J.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Yin, Y.; Liu, J.; Yang, M.; Liu, Z.; Ma, X. Impact of Combined Theory-Based Intervention on Psychological Effects and Physical Activity among Chinese Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 3026. [Google Scholar] [CrossRef]
- Hodge, K.; Danish, S.; Forneris, T.; Miles, A. Life Skills and Basic Psychological Needs. In Positive Youth Development through Sport; Routledge: London, UK, 2016; pp. 45–56. [Google Scholar] [CrossRef]
- Danish, S.; Forneris, T.; Hodge, K.; Heke, I. Enhancing youth development through sport. World Leis. J. 2004, 46, 38–49. [Google Scholar] [CrossRef]
- Goudas, M. Prologue: A review of life skills teaching in sport and physical education. Hell. J. Psychol. 2010, 7, 241–258. [Google Scholar] [CrossRef]
- World Health Organization. Life Skills Education School Handbook: Prevention of Noncommunicable Diseases: Approaches for Schools; World Health Organization: Geneva, Switzerland, 2020; pp. 11–13. [Google Scholar]
- Brooks, F.; Klemera, E.; Chester, K.; Magnusson, J.; Spencer, N. HBSC England National Report: Findings from the 2018 HBSC Study for England; University of Hertfordshire: Hatfield, UK, 2020; pp. 3–7. [Google Scholar]
- Aishath, N.; Haslinda Binti, A.; Steven Eric, K.; Nobaya Binti, A. A narrative systematic review of life skills education: Effectiveness, research gaps and priorities. Int. J. Adolesc. Youth 2018, 24, 362–379. [Google Scholar] [CrossRef] [Green Version]
- Saraf, D.S.; Nongkynrih, B.; Pandav, C.S.; Gupta, S.K.; Shah, B.; Kapoor, S.K.; Krishnan, A. A systematic review of school-based interventions to prevent risk factors associated with noncommunicable diseases. Asia Pac. J. Public Health 2012, 24, 733–752. [Google Scholar] [CrossRef]
- Tiwari, P.; Naik, P.R.; Nirgude, A.S.; Datta, A. Effectiveness of life skills health education program: A quasi-experimental study among school students of South India. J. Educ. Health Promot. 2020, 9, 336. [Google Scholar] [CrossRef]
- Hale, D.R.; Fitzgerald-Yau, N.; Viner, R.M. A systematic review of effective interventions for reducing multiple health risk behaviors in adolescence. Am. J. Public Health 2014, 104, 19–42. [Google Scholar] [CrossRef] [PubMed]
- Anand, T.; Ingle, G.K.; Meena, G.S.; Kishore, J.; Yadav, S. Effect of life skills training on physical activity patterns amongst school adolescents in Delhi: A non-randomized interventional study. Int. J. Adolesc. Med. Health 2014, 26, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Givaudan, M.; Barriga, M.; García, G.; Valdez, I.; Silver, C. School-Based Life Skills Program to Reduce Psychosocial Barriers to Achieving Child Nutrition and Obesity Prevention. Am. J. Appl. Psychol. 2020, 9, 131–139. [Google Scholar] [CrossRef]
- Baranowski, T.; Cullen, K.W.; Nicklas, T.; Thompson, D.; Baranowski, J. Are current health behavioral change models helpful in guiding prevention of weight gain efforts? Obes. Res. 2003, 11, 23S–43S. [Google Scholar] [CrossRef]
- McEwan, D.; Beauchamp, M.R.; Kouvousis, C.; Ray, C.; Wyrough, A.; Rhodes, R.E. Examining the active ingredients of physical activity interventions underpinned by theory versus no stated theory: A meta-analysis. Health Psychol. Rev. 2019, 13, 1–17. [Google Scholar] [CrossRef]
- Hassandra, M.; Theodorakis, Y.; Kosmidou, E.; Grammatikopoulos, V.; Hatzigeorgiadis, A. I do not smoke-I exercise: A pilot study of a new educational resource for secondary education students. Scand. J. Public Health 2009, 37, 372–379. [Google Scholar] [CrossRef]
- Kolovelonis, A.; Goudas, M.; Theodorakis, Y. Examining the effectiveness of the smoking prevention program “I do not smoke, I exercise” in elementary and secondary school settings. Health Promot. Pract. 2016, 17, 827–835. [Google Scholar] [CrossRef]
- Booth, M.L.; Okely, A.D.; Chey, T.; Bauman, A. The reliability and validity of the physical activity questions in the WHO health behaviour in schoolchildren (HBSC) survey: A population study. Br. J. Sports Med. 2001, 35, 263–267. [Google Scholar] [CrossRef] [Green Version]
- Kokkevi, A.; Stavrou, M.; Kanavou, E.; Fotiou, A. The Repercussions of the Economic Recession in Greece on Adolescents and Their Families; Innocenti Working Paper No. 2014-07; UNICEF Office of Research: Florence, Italy, 2004. [Google Scholar]
- Ajzen, I. Constructing a TPB Questionnaire: Conceptual and Methodological Considerations. 2002. Available online: http://www.people.umass.edu/aizen/pdf/tpb.measurement.pdf (accessed on 5 October 2022).
- Ajzen, I. Constructing a Theory of Planned Behavior Questionnaire. 2006. Available online: https://people.umass.edu/~aizen/pdf/tpb.measurement.pdf (accessed on 5 October 2022).
- Theodorakis, Y. Planned behavior, attitude strength, role identity, and the prediction of exercise behavior. TSP 1994, 8, 149–165. [Google Scholar] [CrossRef]
- Daher, J.; El Khoury, D.; Dwyer, J.J. Education interventions to improve knowledge, beliefs, intentions and practices with respect to dietary supplements and doping substances: A narrative review. Nutrients 2021, 13, 3935. [Google Scholar] [CrossRef]
- Arlinghaus, K.R.; Johnston, C.A. Advocating for behavior change with education. Am. J. Lifestyle Med. 2018, 12, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Partida, S.; Marshall, A.; Henry, R.; Townsend, J.; Toy, A. Attitudes toward nutrition and dietary habits and effectiveness of nutrition education in active adolescents in a private school setting: A pilot study. Nutrients 2018, 10, 1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koca, B.; Arkan, G. The relationship between adolescents’ nutrition literacy and food habits, and affecting factors. Public Health Nutr. 2020, 29, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Champion, K.E.; Newton, N.; Barrett, E.L.; Teesson, M. A systematic review of school-based alcohol and other drug prevention programs facilitated by computers or the internet. Drug Alcohol. Rev. 2013, 32, 115–123. [Google Scholar] [CrossRef] [PubMed]
- do Amaral, E.; Melo, G.R.; de Carvalho Silva Varga, F.; Dos Santos Chagas, C.M.; Toral, N. Nutritional interventions for adolescents using information and communication technologies (ICTs): A systematic review. PLoS ONE 2017, 12, e0184509. [Google Scholar] [CrossRef]
- de Sousa, D.; Fogel, A.; Azevedo, J.; Padrão, P. The Effectiveness of Web-Based Interventions to Promote Health Behaviour Change in Adolescents: A Systematic Review. Nutrients 2022, 14, 1258. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.C.; Kwon, J.; Nichols, D.; Rew, M. Evaluation of the nutrition knowledge, attitudes, and food consumption behaviors of high school students before and after completion of a nutrition course. Fam. Consum. Sci. Res. J. 2009, 37, 523–534. [Google Scholar] [CrossRef]
- Evans, N.; Gilpin, E.; Farkas, A.J.; Shenassa, E.; Pierce, J.P. Adolescents’ perceptions of their peers’ health norms. Am. J. Public Health 1995, 85, 1064–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kothe, E.J.; Mullan, B.A. Interaction effects in the theory of planned behaviour: Predicting fruit and vegetable consumption in three prospective cohorts. Br. J. Health Psychol. 2015, 20, 549–562. [Google Scholar] [CrossRef]
- McDermott, M.S.; Oliver, M.; Simnadis, T.; Beck, E.J.; Coltman, T.; Iverson, D.; Caputi, P.; Sharma, R. The Theory of Planned Behaviour and dietary patterns: A systematic review and meta-analysis. Prev. Med. 2015, 81, 150–156. [Google Scholar] [CrossRef] [Green Version]
- Jacob, C.M.; Hardy-Johnson, P.L.; Inskip, H.M.; Morris, T.; Parsons, C.; Barrett, M.; Hanson, M.; Woods-Townsend, K.; Baird, J. A systematic review and meta-analysis of school-based interventions with health education to reduce body mass index in adolescents aged 10 to 19 years. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Mann, M.J.; Lohrmann, D.K. Addressing challenges to the reliable, large-scale implementation of effective school health education. Health Promot. Pract. 2019, 20, 834–844. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Sessions | Contents | Activities |
|---|---|---|
| 1st | Introduction of the program—Purpose of the program— Determine way of working—Initial evaluation | Students grouped—I learn about my body—What is BMI (Body Mass Index)?—What are metabolism and calories?—Students calculate their BMI—Communicate with significant others |
| 2nd | What is a healthy diet—Macronutrients—Table with nutrient information—Food pyramid | Knowledge test of healthy diet—Create a food pyramid poster with a collage of images of foods—Learn to read food labels—Create a message about nutritive food |
| 3rd | Lead causes of unhealthy diet—Consequences of poor diet—Eating disorders and their causes | Knowledge test of unhealthy foods—Analyze campaigns promoting the ideal body type—Create a message reflecting this session and communicate it to others. |
| 4th | Obesity—Data from Hellenic Medical Society of Obesity—Physical and mental health effects of obesity—Childhood obesity data—The psychology of obesity | Demystification of the ideal body—Teamwork: “To what extent do we judge ourselves and others by our/their appearance” |
| 5th | Diet—Restrictions on a diet—How mass media promotes unhealthy food products as healthy choices—Hidden messages—The effectiveness of a diet is related to psychology—The Forbidden Fruit Theory—How to monitor our eating habits | Personal assessment questionnaire—Interviewing a family member who makes effort to lose weight with no results—Keep a food diary—Create a message of the session |
| 6th | Regular exercise and its importance—Research data of PA benefits in physical and psychological health—List of calories burned in 1 h of exercise | Knowledge test of the health benefits of exercise—Self-assessment questionnaire: “Why do I not exercise?”—Keep a PA diary—“Creating the curve of monthly PA” |
| 7th | Changing our diet and PA habits—Reflection on our healthy and unhealthy behaviors—Assessment of eating behavior | Teamwork: “Create a balanced diet plan”—Complete a personal diet and PA diary—Step-by-step guidance for the goal-setting technique (Exercise behavior)—Create and communicate the message of the session |
| 8th | Models of behavior change—Controlling our emotions—Introducing control strategies | Strategies for developing emotional intelligence—Regulate our emotions—Positive self-talk—Awareness—Role-playing—Controlling thoughts—Relaxation techniques—Modifying outcome expectations |
| 9th | Setting goals for a healthy diet and regular exercise—Introduce goal-setting theory—What type of goals should I set?—Individual and team practice with the goal-setting skills for fitness issues | Step-by-step goal-setting technique (healthy diet behavior)—Overcoming obstacles to health (healthy dietary and exercise behavior)—Create the message of the session and communicate it to significant others |
| 10th | Publication of the program to other students, teachers, parents, and others—Learn how to transfer knowledge to significant others | Organize a lecture by health experts (psychologists, nutritionists, and fitness trainers) and obtain information about health issues—Organize a celebration with a buffet of healthy foods using all of the information gathered—Exhibition of the material of the program (posters, photos, images, and messages)—Presentation |
| Pre-Intervention | Post-Intervention | |||||
|---|---|---|---|---|---|---|
| Variables | α | M | SD | α | M | SD |
| Attitudes toward healthy eating | 0.80 | 6.06 | 0.90 | 0.81 | 6.14 | 0.94 |
| Intention toward healthy eating | 0.77 | 6.22 | 0.98 | 0.90 | 6.17 | 1.16 |
| Subjective norm | 0.81 | 5.85 | 1.22 | 0.87 | 5.98 | 1.22 |
| PBC | 0.44 | 6.18 | 0.94 | 0.64 | 6.21 | 0.98 |
| Attitudes toward the program * | 0.82 | 5.74 | 1.02 | 0.56 | 5.90 | 1.48 |
| Knowledge about healthy eating *** | 0.74 | 41.55 | 9.21 | 0.79 | 45.31 | 11.26 |
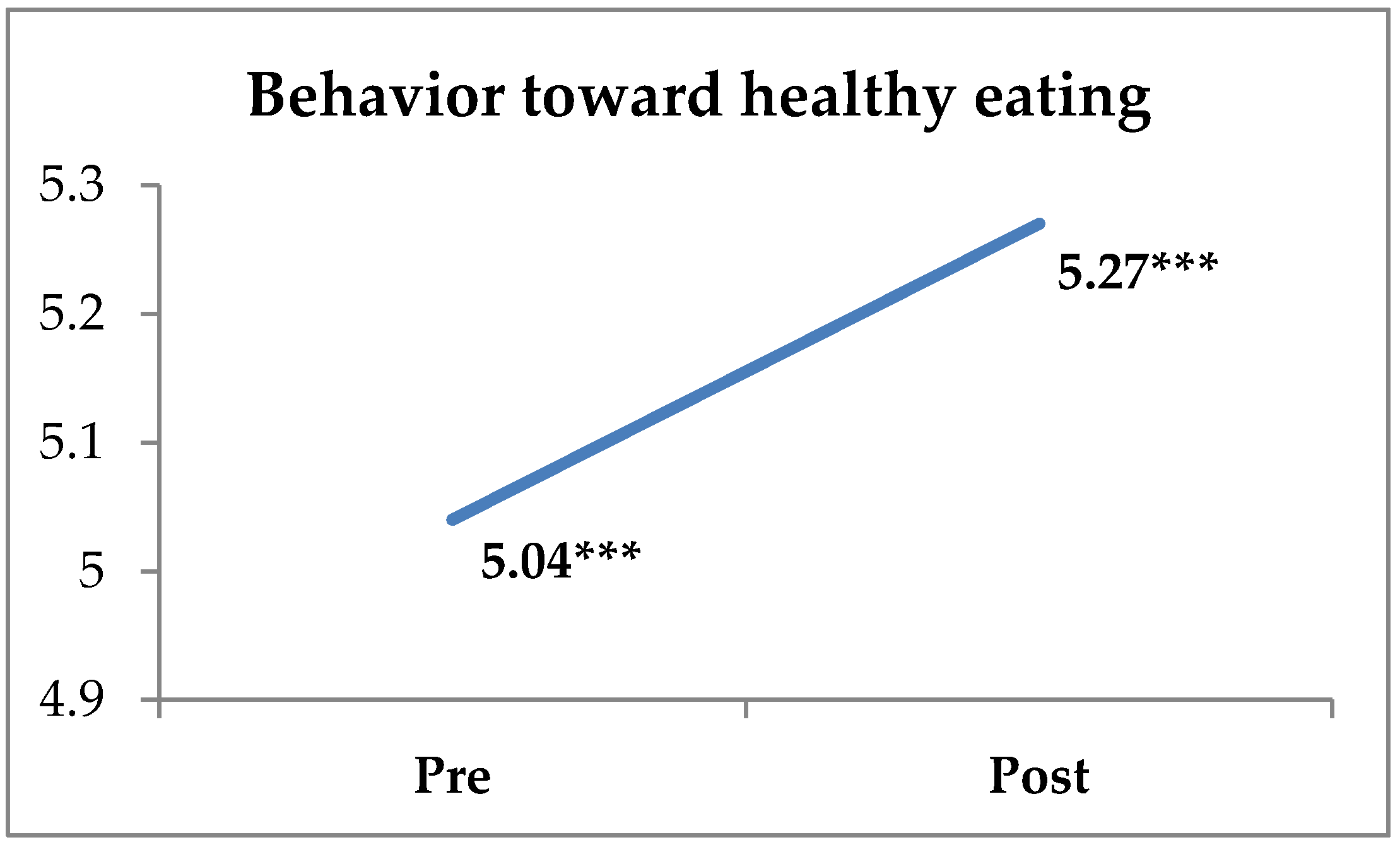
| Behavior about healthy eating ** | 0.81 | 5.04 | 1.30 | 0.88 | 5.27 | 1.40 |
| Exercise behavior | - | 4.59 | 1.17 | - | 4.57 | 1.27 |
| Satisfaction with the program | - | - | - | 0.84 | 5.83 | 0.99 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angeli, M.; Hassandra, M.; Krommidas, C.; Kolovelonis, A.; Bouglas, V.; Theodorakis, Y. Implementation and Evaluation of a School-Based Educational Program Targeting Healthy Diet and Exercise (DIEX) for Greek High School Students. Sports 2022, 10, 196. https://doi.org/10.3390/sports10120196
Angeli M, Hassandra M, Krommidas C, Kolovelonis A, Bouglas V, Theodorakis Y. Implementation and Evaluation of a School-Based Educational Program Targeting Healthy Diet and Exercise (DIEX) for Greek High School Students. Sports. 2022; 10(12):196. https://doi.org/10.3390/sports10120196
Chicago/Turabian StyleAngeli, Maria, Mary Hassandra, Charalampos Krommidas, Athanasios Kolovelonis, Vassilios Bouglas, and Yannis Theodorakis. 2022. "Implementation and Evaluation of a School-Based Educational Program Targeting Healthy Diet and Exercise (DIEX) for Greek High School Students" Sports 10, no. 12: 196. https://doi.org/10.3390/sports10120196