



Convalescing Mandibular Anterior Crowding through Piezocision and the Micro-Osteoperforation Surgical Procedure—A Clinical Comparative Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
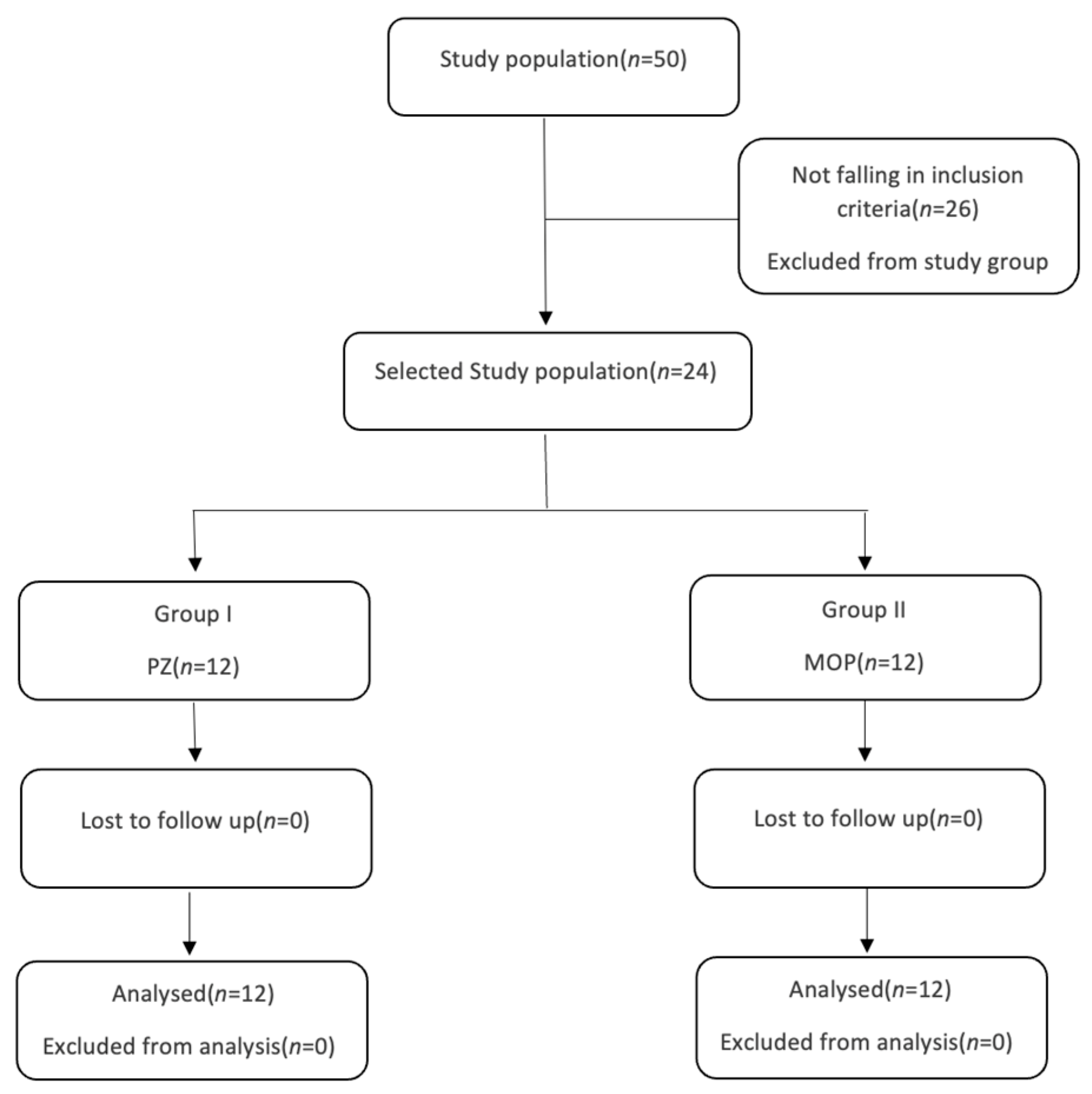
2.1. Study Design and Study Participants
2.2. Group Division
2.3. Periodontic Procedures
2.3.1. Piezocision Procedure (PZ)
2.3.2. Micro-Osteoperforation Procedure (MOP)
2.4. Orthodontic Procedure
- T0—at the initiation of orthodontic treatment.
- Tx—at the termination of the decrowding stage when LII was less than 1 mm.
- x denotes the month in which final decrowding was achieved.
2.5. Statistical Methods
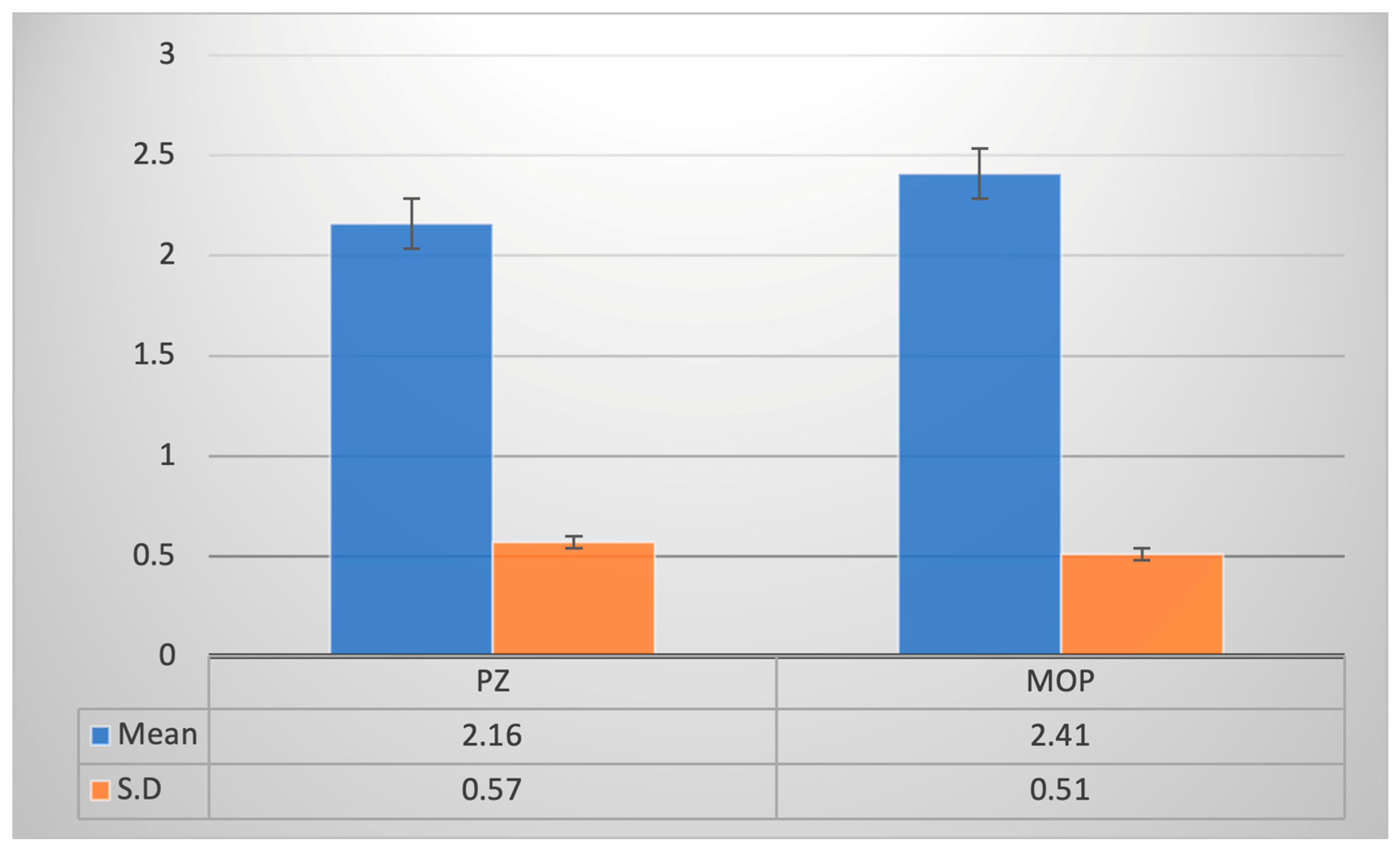
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dyer, G.S.; Harris, E.F.; Vaden, J.L. Age effects on orthodontic treatment: Adolescents contrasted with adults. Am. J. Orthod. Dentofac. Orthop. 1991, 100, 523–530. [Google Scholar] [CrossRef]
- Chaturvedi, S.; Khaled Addas, M.; Al Humaidi, A.S.A.; Al Qahtani, A.M.; Al Qahtani, M.D. A Novel Approach to Determine the Prevalence of Type of Soft Palate Using Digital Intraoral Impression. Int. J. Dent. 2017, 2017, 3268064. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, S.; Haralur, S.B.; Addas, M.K.; Alfarsi, M.A. CBCT analysis of schneiderian membrane thickness and its relationship with gingival biotype and arch form. Niger. J. Clin. Pract. 2019, 22, 1448–1456. [Google Scholar] [CrossRef]
- Nair, U.P.; Shivamurthy, R.; Nagate, R.R.; Chaturvedi, S.; Al-Qahtani, S.M.; Magbol, M.A.; Gokhale, S.T.; Tikare, S.; Chaturvedi, M. Effect of Injectable Platelet-Rich Fibrin with a Nano-Hydroxyapatite Bone Graft on the Treatment of a Grade II Furcation Defect. Bioengineering 2022, 9, 602. [Google Scholar] [CrossRef]
- Tayer, B.H.; Burek, M.J. A survey of adults’ attitudes toward orthodontic therapy. Am. J. Orthod. 1981, 79, 305–315. [Google Scholar] [CrossRef]
- Alshammari, A.K.; Siddiqui, A.A.; Al Shammary, N.H.; Malik, Y.R.; Alam, M.K. Assessment of Perception and Barriers toward Orthodontic Treatment Needs in the Saudi Arabian Adult Population. Healthcare 2022, 10, 2488. [Google Scholar] [CrossRef]
- Hassan, A.H.; Amin, H.E.S. Association of orthodontic treatment needs and oral health-related quality of life in young adults. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Wishney, M. Potential risks of orthodontic therapy: A critical review and conceptual framework. Aust. Dent. J. 2017, 62, 86–96. [Google Scholar] [CrossRef] [PubMed]
- Alobaid, M.A.; Alshahrani, E.M.; Alshehri, E.M.; Shaiban, A.S.; Haralur, S.B.; Chaturvedi, S.; Addas, M.K. Radiographic assessment of root canal morphology of mandibular central incisors using new classification system: A cross-sectional study. Medicine 2022, 101, e30751. [Google Scholar] [CrossRef]
- Gupta, K.; Kumar, S.; Kukkamalla, M.A.; Taneja, V.; Syed, G.A.; Pullishery, F.; Zarbah, M.A.; Alqahtani, S.M.; Alobaoid, M.A.; Chaturvedi, S. Dental Management Considerations for Patients with Cardiovascular Disease—A Narrative Review. Rev. Cardiovasc. Med. 2022, 23, 261. [Google Scholar] [CrossRef]
- Li, Y.; Jacox, L.A.; Little, S.H.; Ko, C.-C. Orthodontic tooth movement: The biology and clinical implications. Kaohsiung J. Med. Sci. 2018, 34, 207–214. [Google Scholar] [CrossRef]
- Nagate, R.R.; Tikare, S.; Chaturvedi, S.; AlQahtani, N.A.; Kader, M.A.; Gokhale, S.T. A novel perspective for predicting gingival biotype via dentopapillary measurements on study models in the Saudi population: Cross-sectional study. Niger. J. Clin. Pract. 2019, 22, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Frost, H.M. The regional acceleratory phenomenon: A review. Henry Ford Hosp. Med. J. 1983, 31, 3–9. [Google Scholar] [PubMed]
- Wilcko, W.M.; Wilcko, T.; Bouquot, J.E.; Ferguson, D.J. Rapid orthodontics with alveolar reshaping: Two case reports of decrowding. Int. J. Periodontics Restor. Dent. 2001, 21, 9–19. [Google Scholar]
- Zawawi, K. Patients’ acceptance of corticotomy-assisted orthodontics. Patient Prefer. Adherence 2015, 9, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Pouliezou, I.; Xenou, A.; Vavetsi, K.; Mitsea, A.; Sifakakis, I. Adverse Effects of Surgically Accelerated Orthodontic Techniques: A Systematic Review. Children 2022, 9, 1835. [Google Scholar] [CrossRef] [PubMed]
- Gasparro, R.; Bucci, R.; De Rosa, F.; Sammartino, G.; Bucci, P.; D’Antò, V.; Marenzi, G. Effectiveness of surgical procedures in the acceleration of orthodontic tooth movement: Findings from systematic reviews and meta-analyses. Jpn. Dent. Sci. Rev. 2022, 58, 137–154. [Google Scholar] [CrossRef] [PubMed]
- Dibart, S.; Sebaoun, J.D.; Surmenian, J. Piezocision: A minimally invasive, periodontally accelerated orthodontic tooth movement procedure. Compend. Contin. Educ. Dent. 2009, 30, 342. [Google Scholar] [PubMed]
- Alikhani, M.; Alansari, S.; Sangsuwon, C.; Alikhani, M.; Chou, M.Y.; Alyami, B.; Nervina, J.M.; Teixeira, C.C. Micro-osteoperforations: Minimally invasive accelerated tooth movement. Semin. Orthod. 2015, 21, 162–169. [Google Scholar] [CrossRef]
- Shetty, S.K.; Vincent, S.; Y, M.K.; Madhur, V.K. Effects of Microosteoperforations on Rate of Orthodontic Tooth Movement. Sch. J. Dent. Sci. 2021, 8, 239–242. [Google Scholar] [CrossRef]
- Sanjideh, P.A.; Rossouw, P.E.; Campbell, P.M.; Opperman, L.A.; Buschang, P.H. Tooth movements in foxhounds after one or two alveolar corticotomies. Eur. J. Orthod. 2010, 32, 106–113. [Google Scholar] [CrossRef]
- Teixeira, C.C.; Khoo, E.; Tran, J.; Chartres, I.; Liu, Y.; Thant, L.M.; Khabensky, I.; Gart, L.; Cisneros, G.; Alikhani, M. Cytokine expression and accelerated tooth movement. J. Dent. Res. 2010, 89, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Keser, E.I.; Dibart, S. Piezocision-assisted Invisalign treatment. Compend. Contin. Educ. Dent. 2011, 32. [Google Scholar]
- Keser, E.I.; Dibart, S. Sequential piezocision: A novel approach to accelerated orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 879–889. [Google Scholar] [CrossRef] [PubMed]
- Keser, E.; Naini, F.B. Accelerated orthodontic tooth movement: Surgical techniques and the regional acceleratory phenomenon. Maxillofac. Plast. Reconstr. Surg. 2022, 44, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.A.; Chandhoke, T.; Kalajzic, Z.; Flynn, R.; Utreja, A.; Wadhwa, S.; Nanda, R.; Uribe, F. Effect of corticision and different force magnitudes on orthodontic tooth movement in a rat model. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Milano, F.; Dibart, S.; Montesani, L.; Guerra, L. Computer-Guided Surgery Using the Piezocision Technique. Int. J. Periodontics Restor. Dent. 2014, 34, 523–529. [Google Scholar] [CrossRef]
- Dibart, S.; Yee, C.; Surmenian, J.; Sebaoun, J.D.; Baloul, S.; Goguet-Surmenian, E.; Kantarci, A. Tissue response during Piezocision-assisted tooth movement: A histological study in rats. Eur. J. Orthod. 2014, 36, 457–464. [Google Scholar] [CrossRef]
- Murphy, C.; Kalajzic, Z.; Chandhoke, T.; Utreja, A.; Nanda, R.; Uribe, F. The effect of corticision on root resorption with heavy and light forces. Angle Orthod. 2016, 86, 17–23. [Google Scholar] [CrossRef]
- Aksakalli, S.; Calik, B.; Kara, B.; Ezirganli, S. Accelerated tooth movement with piezocision and its periodontaltransversal effects in patients with Class II malocclusion. Angle Orthod. 2016, 86, 59–65. [Google Scholar] [CrossRef]
- Charavet, C. Localized Piezoelectric Alveolar Decortication for Orthodontic Treatment in Adults: A Randomized Controlled Trial. J. Oral Maxillofac. Surg. 2019, 77, e56–e57. [Google Scholar] [CrossRef]
- Abbas, N.H.; Sabet, N.E.; Hassan, I.T. Evaluation of corticotomy-facilitated orthodontics and piezocision in rapid canine retraction. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 473–480. [Google Scholar] [CrossRef]
- Dibart, S.; Alasmari, A.; Zanni, O.; Salih, E. Effect of Corticotomies with Different Instruments on Cranial Bone Biology Using an Ex Vivo Calvarial Bone Organ Culture Model System. Int. J. Periodontics Restor. Dent. 2016, 36, s123–s136. [Google Scholar] [CrossRef]
- Uribe, F.; Padala, S.; Allareddy, V.; Nanda, R. Patients’, parents’, and orthodontists’ perceptions of the need for and costs of additional procedures to reduce treatment time. Am. J. Orthod. Dentofac. Orthop. 2014, 145, S65–S73. [Google Scholar] [CrossRef]
- Sugimori, T.; Yamaguchi, M.; Shimizu, M.; Kikuta, J.; Hikida, T.; Hikida, M.; Murakami, Y.; Suemitsu, M.; Kuyama, K.; Kasai, K. Micro-osteoperforations accelerate orthodontic tooth movement by stimulating periodontal ligament cell cycles. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 788–796. [Google Scholar] [CrossRef]
- Alkebsi, A.; Al-Maaitah, E.; Al-Shorman, H.; Abu Alhaija, E. Three-dimensional assessment of the effect of micro-osteoperforations on the rate of tooth movement during canine retraction in adults with Class II malocclusion: A randomized controlled clinical trial. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 771–785. [Google Scholar] [CrossRef]
- Chan, E.; Dalci, O.; Petocz, P.; Papadopoulou, A.K.; Darendeliler, M.A. Physical properties of root cementum: Part 26. Effects of micro-osteoperforations on orthodontic root resorption: A microcomputed tomography study. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Attri, S.; Mittal, R.; Batra, P.; Sonar, S.; Sharma, K.; Raghavan, S.; Rai, K.S. Comparison of rate of tooth movement and pain perception during accelerated tooth movement associated with conventional fixed appliances with micro-osteoperforations—A randomised controlled trial. J. Orthod. 2018, 45, 225–233. [Google Scholar] [CrossRef]
- Hou, H.Y.; Li, C.H.; Chen, M.C.; Lin, P.Y.; Liu, W.C.; Cathy Tsai, Y.W.; Huang, R.-Y. A novel 3D-printed computer-assisted piezocision guide for surgically facilitated orthodontics. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 584–591. [Google Scholar] [CrossRef] [PubMed]
- van Gemert, L.N.; Campbell, P.M.; Opperman, L.A.; Buschang, P.H. Localizing the osseous boundaries of micro-osteoperforations. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 779–790. [Google Scholar] [CrossRef] [PubMed]
- Sivarajan, S.; Doss, J.G.; Papageorgiou, S.N.; Cobourne, M.T.; Wey, M.C. Mini-implant supported canine retraction with micro-osteoperforation: A split-mouth randomized clinical trial. Angle Orthod. 2019, 89, 183–189. [Google Scholar] [CrossRef]
- Charavet, C.; Van Hede, D.; Anania, S.; Maes, N.; Lambert, F. Multilevel biological responses following piezocision to accelerate orthodontic tooth movement: A study in rats. J. World Fed. Orthod. 2019, 8, 100–106. [Google Scholar] [CrossRef]
- Khlef, H.N.; Hajeer, M.Y.; Ajaj, M.A.; Heshmeh, O.; Youssef, N.; Mahaini, L. The effectiveness of traditional corticotomy vs flapless corticotomy in miniscrew-supported en-masse retraction of maxillary anterior teeth in patients with Class II Division 1 malocclusion: A single-centered, randomized controlled clinical trial. Am. J. Orthod. Dentofac. Orthop. 2020, 158, e111–e120. [Google Scholar] [CrossRef]
- Hannequin, R.; Ouadi, E.; Racy, E.; Moreau, N. Clinical follow-up of corticotomy-accelerated Invisalign orthodontic treatment with Dental Monitoring. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 878–888. [Google Scholar] [CrossRef]
- Hatrom, A.A.; Howait, M.S.; Zawawi, K.H.; Al-Turki, G.A.; Alansari, R.A.; Almehayawi, N.F.; Alammari, S.H.; Mohammed, R.A.; Hassan, A.H. Pulp volume changes after piezocision-assisted tooth movement: A randomized clinical trial. BMC Oral Health 2021, 21, 1–8. [Google Scholar] [CrossRef]
- Alvarez, M.A.; Mejia, A.; Alzate, D.; Rey, D.; Ioshida, M.; Aristizabal, J.F.; Rios, H.F.; Bellaiza-Cantillo, W.; Tirado, M.; Ruellas, A.; et al. Buccal bone defects and transversal tooth movement of mandibular lateral segments in patients after orthodontic treatment with and without piezocision: A case-control retrospective study. Am. J. Orthod. Dentofac. Orthop. 2021, 159, e233–e243. [Google Scholar] [CrossRef]
- Kernitsky, J.R.; Ohira, T.; Shosho, D.; Lim, J.; Bamashmous, A.; Dibart, S. Corticotomy depth and regional acceleratory phenomenon intensity: A preliminary study. Angle Orthod. 2021, 91, 206–212. [Google Scholar] [CrossRef]
- Charavet, C.; Van Hede, D.; Anania, S.; Maes, N.; Albert, A.; Lambert, F. One-stage versus two-stage piezocision-assisted orthodontic tooth movement: A preclinical study based on Nano-CT and RT-PCR analyses. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e663–e669. [Google Scholar] [CrossRef] [PubMed]
- Battista, M.; Di Kernitsky, J.; Exarchos, E.; Ohira, T.; Dibart, S. Quantification and comparison of the regional acceleratory phenomenon in bone following piezosurgery or bur osteotomy: A pilot study in rats. Clin. Exp. Dent. Res. 2023, 9, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Kotrikova, B.; Wirtz, R.; Krempien, R.; Blank, J.; Eggers, G.; Samiotis, A.; Mühling, J. Piezosurgery—A new safe technique in cranial osteoplasty? Int. J. Oral Maxillofac. Surg. 2006, 35, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Robiony, M.; Polini, F.; Costa, F.; Vercellotti, T.; Politi, M. Piezoelectric bone cutting in multipiece maxillary osteotomies. J. Oral Maxillofac. Surg. 2004, 62, 759–761. [Google Scholar] [CrossRef]
- Gibreal, O.; Hajeer, M.Y.; Brad, B. Efficacy of piezocision-based flapless corticotomy in the orthodontic correction of severely crowded lower anterior teeth: A randomized controlled trial. Eur. J. Orthod. 2019, 41, 188–195. [Google Scholar] [CrossRef]
- Charavet, C.; Lecloux, G.; Bruwier, A.; Rompen, E.; Maes, N.; Limme, M.; Lambert, F. Localized Piezoelectric Alveolar Decortication for Orthodontic Treatment in Adults. J. Dent. Res. 2016, 95, 1003–1009. [Google Scholar] [CrossRef]
- Yavuz, M.C.; Sunar, O.; Buyuk, S.K.; Kantarcı, A. Comparison of piezocision and discision methods in orthodontic treatment. Prog. Orthod. 2018, 19, 44. [Google Scholar] [CrossRef]
- Uribe, F.; Davoody, L.; Mehr, R.; Jayaratne, Y.S.N.; Almas, K.; Sobue, T.; Allareddy, V.; Nanda, R. Efficiency of piezotome-corticision assisted orthodontics in alleviating mandibular anterior crowding—A randomized clinical trial. Eur. J. Orthod. 2017, 39, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Shahrin, A.A.; Ghani, S.H.A.; Norman, N.H. Effect of micro-osteoperforations on external apical root resorption: A randomized controlled trial. Korean J. Orthod. 2021, 51, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Bansal, M.; Sharma, R.; Kumar, D.; Gupta, A. Effects of mini-implant facilitated micro-osteoperforations in alleviating mandibular anterior crowding: A randomized controlled clinical trial. J. Orthod. Sci. 2019, 8, 19. [Google Scholar] [CrossRef] [PubMed]
- Alqadasi, B.; Xia, H.Y.; Alhammadi, M.S.; Hasan, H.; Aldhorae, K.; Halboub, E. Three-dimensional assessment of accelerating orthodontic tooth movement—Micro-osteoperforations vs piezocision: A randomized, parallel-group and split-mouth controlled clinical trial. Orthod. Craniofac. Res. 2021, 24, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Ojima, K.; Kau, C.H. A perspective in accelerated orthodontics with aligner treatment. Semin. Orthod. 2017, 23, 76–82. [Google Scholar] [CrossRef]
- Kiatwarawut, K.; Rokaya, D.; Sirisoontorn, I. Antimicrobial Activity of Various Disinfectants to Clean Thermoplastic Polymeric Appliances in Orthodontics. Polymers 2022, 14, 2256. [Google Scholar] [CrossRef] [PubMed]
- Pérez Idarraga, A.; Yeste Ojeda, F.; Virto Ruiz, L.; Lacasa Litner, M.; Cacho Casado, A.; Martin, C. Randomized clinical trial on the effect of intermittent vibrational force application during orthodontic treatment with aligners on RANKL and OPG concentrations in crevicular fluid. Bioeng. Transl. Med. 2023, 8, e10491. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, S.; Pandian, S.; Aravind Kumar, S. Effect of bisphosphonates on orthodontic tooth movement—An update. J. Clin. Diagn. Res. 2015, 9, ZE01–ZE05. [Google Scholar] [CrossRef] [PubMed]
- Marya, A.; Karobari, M.I.; Shah, P.K.; Rokaya, D. Use of Natural Oral Care Products in Orthodontics. In Pharmacological Studies in Natural Oral Care; Wiley: Hoboken, NJ, USA, 2023; pp. 125–147. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year of Study | Author(s) of Publication | Test Subject | Sample Size | Presence of CG | Study Type | Procedure Being Assessed |
|---|---|---|---|---|---|---|
| 2010 | Sanjideh et al. [21] | A | Five | × | SM | COT |
| 2010 | Teixeira et al. [22] | A | Forty-Eight | √ | - | Soft tissue flap and osteoperforations |
| 2011 | Keser and Dibart [23] | H | One | × | - | PZ |
| 2013 | Keser and Dibart [24] | H | One | × | - | PZ |
| 2013 | Alikhani et al. [25] | H | Twenty | √ | CO | MOP |
| 2014 | Murphy et al. [26] | A | Forty-Four | √ | - | Corticision |
| 2014 | Milano et al. [27] | H | One | × | - | PZ |
| 2014 | Dibart et al. [28] | A | Ninety-Four | √ | - | PZ |
| 2016 | Murphy et al. [29] | A | Forty-Four | √ | - | Corticision |
| 2016 | Aksakalli et al. [30] | H | Ten | × | SM | PZ |
| 2016 | Charavet et al. [31] | H | Twenty-Four | √ | CO | PZ |
| 2016 | Abbas et al. [32] | H | Twenty | × | SM | COT, PZ |
| 2016 | Dibart et al. [33] | A | Two Hundred Seventy-Six | √ | - | piezoelectric knife, bur, handheld screw device |
| 2017 | Uribe et al. [34] | H | Twenty-Nine | √ | CO | Piezotome corticisions |
| 2018 | Sugimori et al. [35] | A | Fifty | √ | O | MOP |
| 2018 | Alkebsi et al. [36] | H | Thirty-Two | √ | CO | MOP |
| 2018 | Chan et al. [37] | H | Twenty | √ | CO | MOP |
| 2018 | Attri et al. [38] | H | Sixty | √ | CO | MOP |
| 2019 | Hou et al. [39] | H | One | × | - | PZ |
| 2019 | Strippoli et al. [25] | H | Twenty-Four | √ | CO | PZ |
| 2019 | Van Gemert [40] | A | Thirteen | × | SM | MOP |
| 2019 | Sivarajan et al. [41] | H | Thirty | × | SM | MOP |
| 2019 | Charavet et al. [42] | A | Sixty | √ | O | PZ |
| 2020 | Hatrom et al. [39] | H | Twenty-Six | √ | CO | PZ |
| 2020 | Khlef et al. [43] | H | Forty | × | - | COT, PZ |
| 2020 | Hannequin et al. [44] | H | One | × | - | COT, PZ |
| 2021 | Hatrom et al. [45] | H | Twenty-Three | √ | CO | PZ |
| 2021 | Alvarez et al. [46] | H | Thirty-Six | √ | CO | PZ |
| 2021 | Kernitsky et al. [47] | A | Eighteen | √ | - | piezoelectric decortications |
| 2021 | Sharon et al. [25] | H | Thirty | √ | CO | MOP |
| 2022 | Charavet C et al. [48] | A | Sixty | × | - | PZ |
| 2023 | Battista et al. [49] | A | Twenty-Two | √ | - | piezoelectric knife/rotary bur |
| Sample No. | T0 | Tx | T0 − Tx | Time (Interval) Taken for Decrowding (T) in Months | Rate of Decrowding (T0 − Tx/T) |
|---|---|---|---|---|---|
| PZ1 | 10.7 | 0.5 | 10.2 | 3 | 3.4 |
| PZ2 | 11.1 | 0.8 | 10.3 | 3 | 3.43 |
| PZ3 | 9.7 | 0.5 | 9.2 | 2 | 4.6 |
| PZ4 | 8.6 | 0.4 | 8.2 | 2 | 4.1 |
| PZ5 | 10.2 | 0.3 | 9.9 | 2 | 4.95 |
| PZ6 | 9 | 0.6 | 8.4 | 2 | 4.2 |
| PZ7 | 10.7 | 0.3 | 10.4 | 2 | 5.2 |
| PZ8 | 11.6 | 0.2 | 11.4 | 3 | 3.8 |
| PZ9 | 5.6 | 0.4 | 5.2 | 1 | 5.2 |
| PZ10 | 9.2 | 0 | 9.2 | 2 | 4.6 |
| PZ11 | 9.8 | 0.2 | 9.6 | 2 | 4.8 |
| PZ12 | 8.8 | 0 | 8.8 | 2 | 4.4 |
| MOP1 | 9.2 | 0.9 | 8.3 | 2 | 4.15 |
| MOP2 | 7.2 | 0.4 | 6.8 | 2 | 3.4 |
| MOP3 | 7.6 | 0.4 | 7.2 | 2 | 3.6 |
| MOP4 | 10.5 | 0.3 | 10.2 | 3 | 3.4 |
| MOP5 | 8.8 | 0.4 | 8.4 | 2 | 4.2 |
| MOP6 | 9.8 | 0.2 | 9.6 | 2 | 4.8 |
| MOP7 | 10.4 | 0.2 | 10.2 | 3 | 3.4 |
| MOP8 | 11.4 | 0 | 11.4 | 3 | 3.8 |
| MOP9 | 8.5 | 0.3 | 8.2 | 2 | 4.1 |
| MOP10 | 9.6 | 0 | 9.6 | 3 | 3.2 |
| MOP11 | 11.1 | 0.3 | 10.8 | 3 | 3.6 |
| MOP12 | 8.6 | 0.2 | 8.4 | 2 | 4.2 |
| t-Test for Equality of Means | ||||
|---|---|---|---|---|
| t | df | Sig. (Two-Tailed) | ||
| Time Taken | Equal variances assumed | −1.119 | 22 | 0.275 |
| t-Test for Equality of Means | ||||
|---|---|---|---|---|
| t | df | Sig. (Two-Tailed) | ||
| Rate | Equal variances assumed | 2.518 | 22 | 0.020 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rao, R.N.; Oommen, K.E.; Nagate, R.R.; Al-Qarni, M.A.; Ahmed, A.R.; Tikare, S.; Gokhale, S.T.; AlBariqi, A.A.; Elagib, M.F.A.; Chaturvedi, S. Convalescing Mandibular Anterior Crowding through Piezocision and the Micro-Osteoperforation Surgical Procedure—A Clinical Comparative Study. J. Pers. Med. 2024, 14, 173. https://doi.org/10.3390/jpm14020173
Rao RN, Oommen KE, Nagate RR, Al-Qarni MA, Ahmed AR, Tikare S, Gokhale ST, AlBariqi AA, Elagib MFA, Chaturvedi S. Convalescing Mandibular Anterior Crowding through Piezocision and the Micro-Osteoperforation Surgical Procedure—A Clinical Comparative Study. Journal of Personalized Medicine. 2024; 14(2):173. https://doi.org/10.3390/jpm14020173
Chicago/Turabian StyleRao, Raghunath Nagasundara, Karuna Elza Oommen, Raghavendra Reddy Nagate, Mohammed A. Al-Qarni, Abdul Razzaq Ahmed, Shreyas Tikare, Shankar T. Gokhale, Ahmed A. AlBariqi, Mohamed Fadul A. Elagib, and Saurabh Chaturvedi. 2024. "Convalescing Mandibular Anterior Crowding through Piezocision and the Micro-Osteoperforation Surgical Procedure—A Clinical Comparative Study" Journal of Personalized Medicine 14, no. 2: 173. https://doi.org/10.3390/jpm14020173